흉관 관리 및 배액법. role of chest tube removal of fluid or air from pleural space...
TRANSCRIPT

흉관 관리 및 배액법

Role of chest tube
• Removal of fluid or air from pleural space– restoration of the negative pressure– full expansion of the lung– effective gas exchange
• Instillation of chemotherapeutic agent after removal of malignant effusion
Indications of chest tube insertion
• post-thoracotomy status
• hemothorax
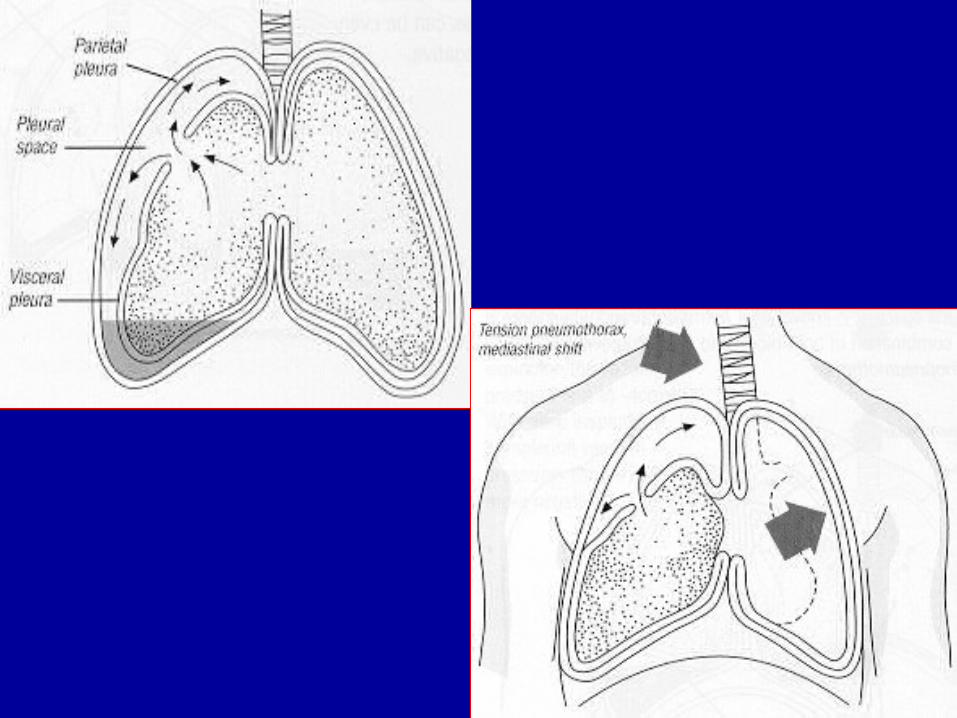
• pneumothorax
• empyema
• chylothorax
• emphysema disease
• prophylactic: ARDS, high PEEP
• others


Placement of chest tube• Post-thoracotomy status
– usually two site insertion(28Fr, 32Fr)• Pneumothorax
– usually 4th ICS on anterior axillary line– 흉강경 수술이 예상될 경우 7th ICS on mid- axillary line
• Pleural fluid – usually 5th, 6th ICS on mid axillary line ( 가능한 dependent position 에 위치 )– Loculation 이 된 경우라면 위치가 달라질 수도 있으며 . 방사선과에서 PCD (Pigtail Chest Drainage) 시행
• Chest tube size– Pneumothorax : 20-28Fr, Effusion : largest that can easily be drained
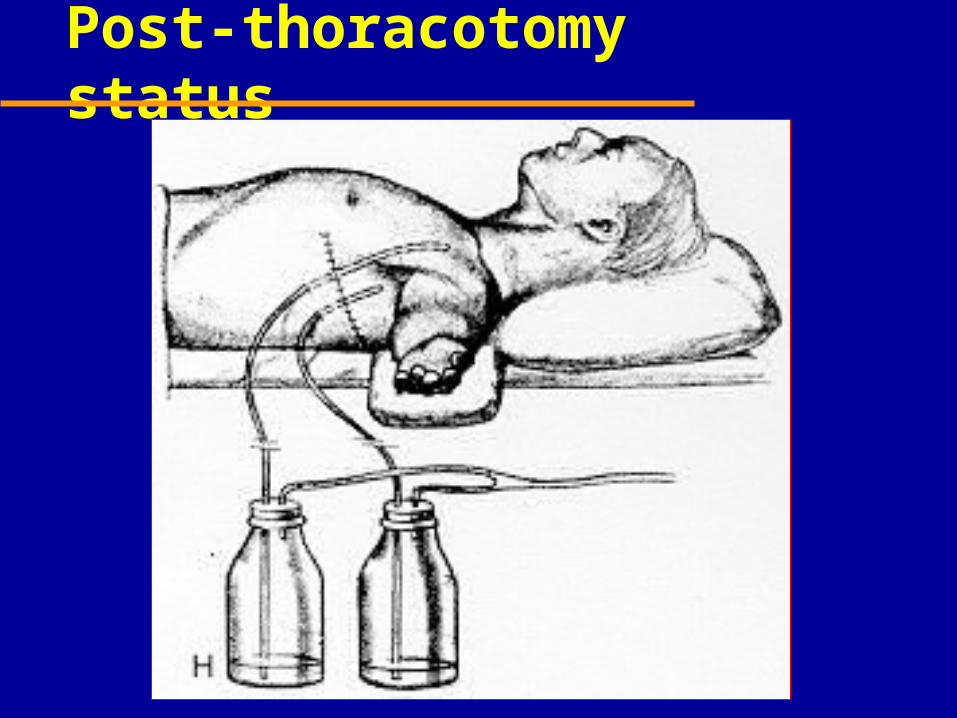
Post-thoracotomy status
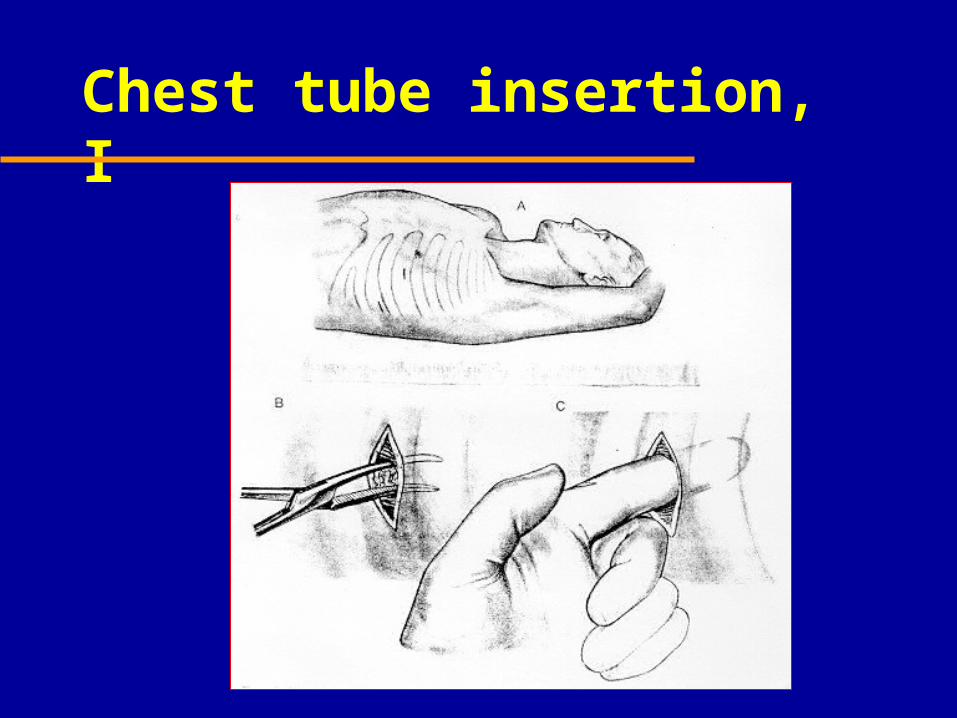
Chest tube insertion, I

Chest tube insertion, II
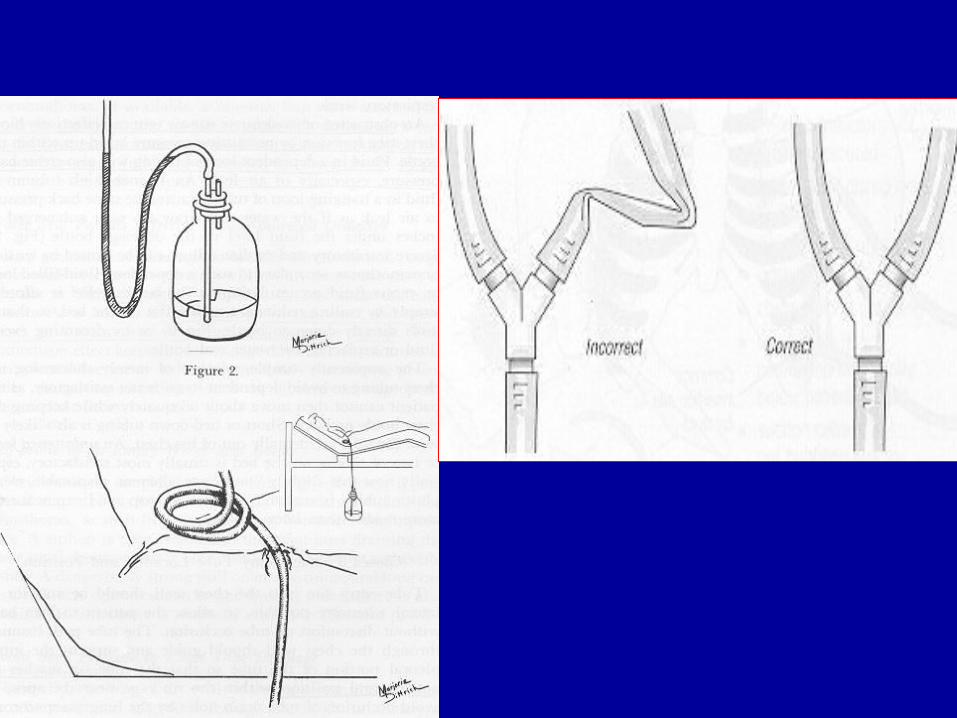
Underwater seal drainage system
A. one-bottle system
B. two-bottle system
C. three-bottle system
D. balanced drainage system
* Heimlich valve
outpatient management

Bottle systems

Commonly used bottles
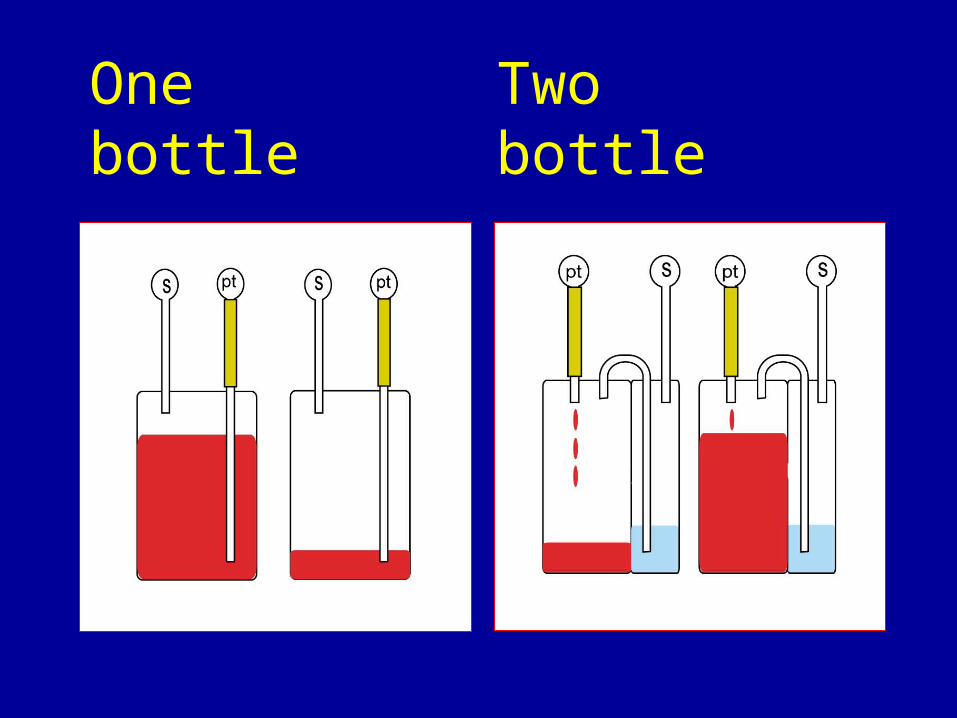
One bottle Two bottle

Suction
• To overcome the air leak• To expand the lung early only in air leak
• Optimal pressure -10 ~ -20 cm H2O
• Higher levels of suction should be avoided– lung damage, pulmonary edema
– avoid vigorous milking or squeezing
Observation of drainage system
• Fluctuations according to respiratory pattern absent - full expansion - blocked tubing • Fluids: volume, color, consistency Hemothorax > 200-300ml/hr• Air leak• Tube clamping should be avoided• Bottle position: 70-90cm below the thorax

Position & Drain

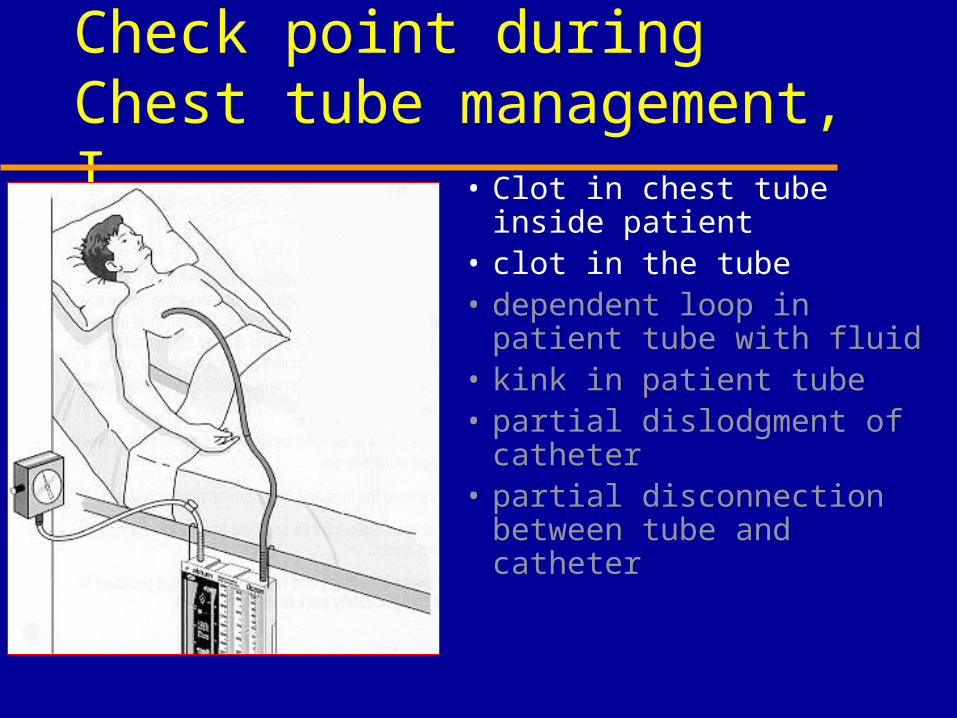
Check point during Chest tube management, I
• Clot in chest tube inside patient
• clot in the tube• dependent loop in patient
tube with fluid• kink in patient tube• partial dislodgment of
catheter• partial disconnection
between tube and catheter
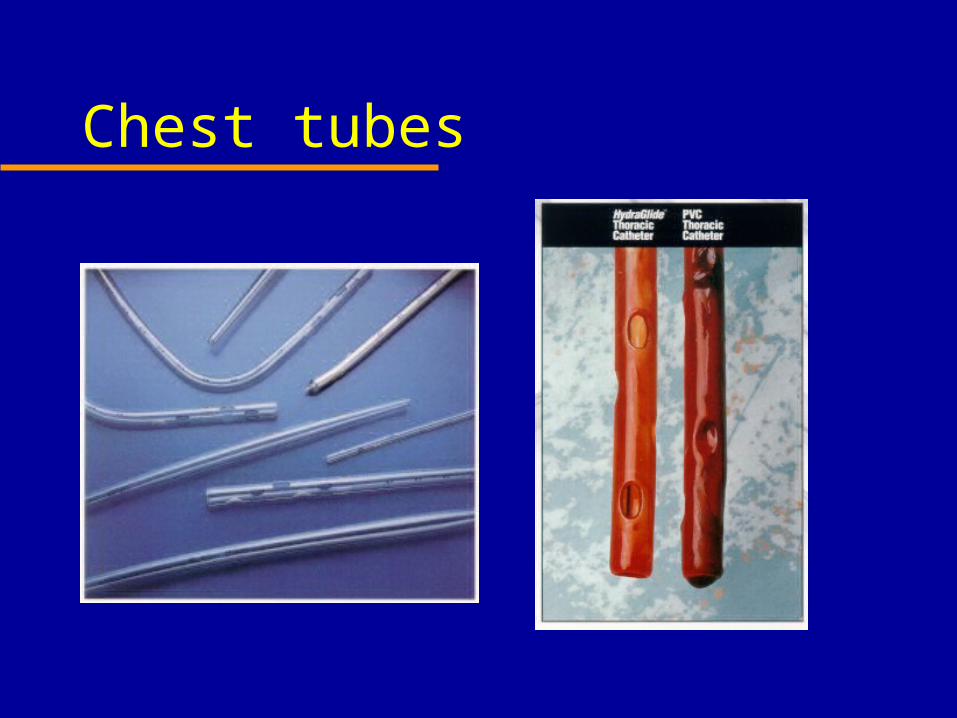
Chest tubes

Check point during Chest tube management, I
• Clot in chest tube inside patient
• clot in the tube• dependent loop in patient
tube with fluid• kink in patient tube• partial dislodgment of
catheter• partial disconnection
between tube and catheter

Check point during Chest tube management, I
• Clot in chest tube inside patient
• clot in the tube• dependent loop in patient
tube with fluid• kink in patient tube• partial dislodgment of
catheter• partial disconnection
between tube and catheter

Check point during Chest tube management, II
• Overfilled water seal• in line connectors not
properly secured• patient tube clamp in situ• chest drain in not upright• insufficient suction• suction is too vigorous• too high chest drain
position

Check point during Chest tube management, II
• Overfilled water seal• in line connectors not
properly secured• patient tube clamp in situ• chest drain in not upright• too high chest drain
position • insufficient suction• suction is too vigorous

Check point during Chest tube management, II
• Overfilled water seal• in line connectors not
properly secured• patient tube clamp in situ• chest drain in not upright• too high chest drain
position• insufficient suction• suction is too vigorous

Chest tube occlusion• Etiology
– blood clots or viscous pleural effusion– kinking of chest tube
• prevention– strip chest tube hourly– insert sufficient large tube– insert additional tube to help evacuate blood, if needed– eliminate kinking by proper positioning and exit
location of the tube - never place tube posterior to midaxillary line
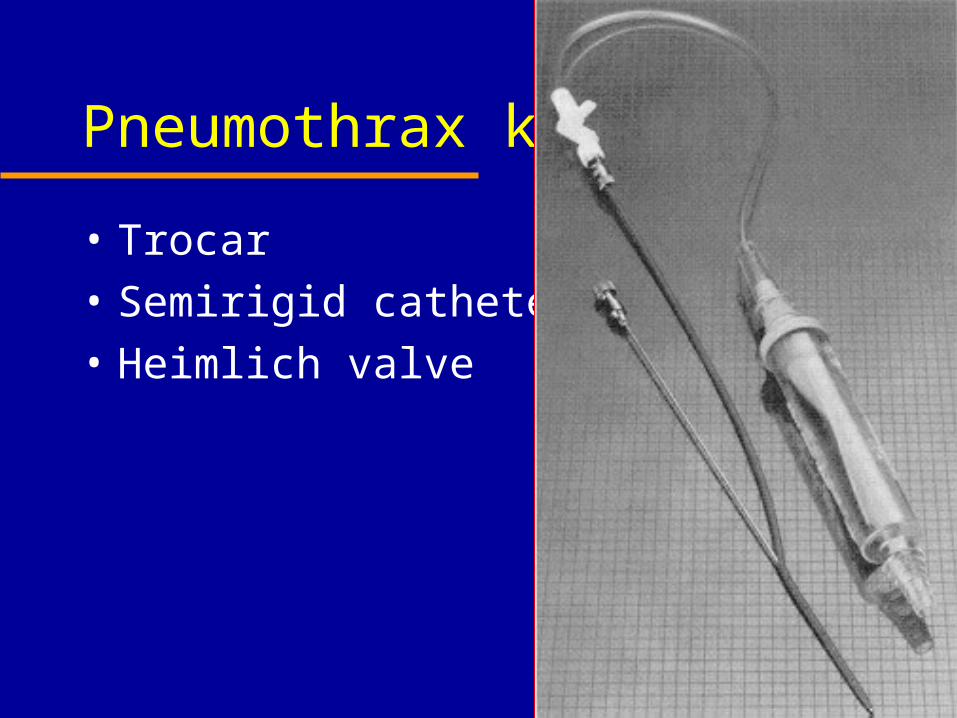
Pneumothrax kit
• Trocar
• Semirigid catheter
• Heimlich valve

Urgent transfusion
Removal of chest tube
• Indication– air and fluid are no longer present
in the pleural space– full re-expansion of the lung
• Clamp the tube for 12-24hrs
• “Inflate and hold ” technique
• Occlusive dressing
• Be confirmed by chest X-ray
Reminder again• Water seal• Keep the bottle below the patient• Transporting injured patient with Chest
bottle; do not clamp the tube• Right connection between bottle and chest
tube• Periodic check kinking of the tube• Avoid back pressure to chest tube drainage

Comment
Very useful and effective measure to evacuate intrathoracic air and/or fluid
Should be carefully observed because
the chest tube and bottle system is not always safe