排尿障礙治療中心 版權所有 stress urinary incontinence hann-chorng kuo department of...
TRANSCRIPT
排尿障礙治療中心 版權所有
Stress Urinary Incontinence
Hann-Chorng Kuo
Department of Urology
Buddhist Tzu Chi General Hospital
排尿障礙治療中心 版權所有
Incontinence
• Definition
Failure of voluntary control of urination causing loss of urine per urethra
排尿障礙治療中心 版權所有
Types of Incontinence by symptomatology
• Continuous or total incontinence
• Urge incontinence
• Stress incontinence
• Overflow incontinence
• Transient incontinence
• Giggle incontinence
排尿障礙治療中心 版權所有
Types of Incontinence by Pathophysiology
• Bladder related incontinence
Detrusor overactivity
Detrusor underactivity & low compliance
• Urethral related incontinence
Intrinsic sphincteric deficiency
Hypermobility of bladder neck & urethra
• Mixed type of incontinence
排尿障礙治療中心 版權所有
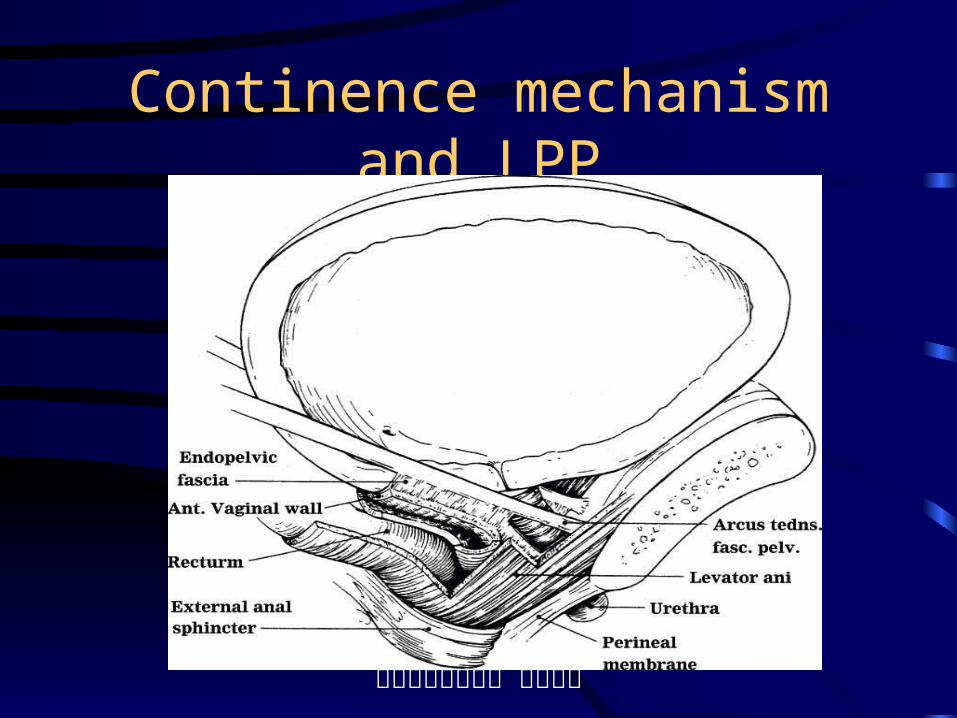
Continence mechanism
• Stable bladder
• High position of bladder neck
• Good urethral coaptation
• Competent bladder neck
• Positive pressure transmission ratio
• Reflex contraction of periurethral muscles
排尿障礙治療中心 版權所有
Extrinsic Continence Mechanism
• Pubourethral & pubovesical ligaments
• Pubocervical fascia
• Attachments to archus tendineus fascia pelvic
• Vaginal endopelvic fascia
• Attachments to levator ani
• Uterosacral ligaments
排尿障礙治療中心 版權所有
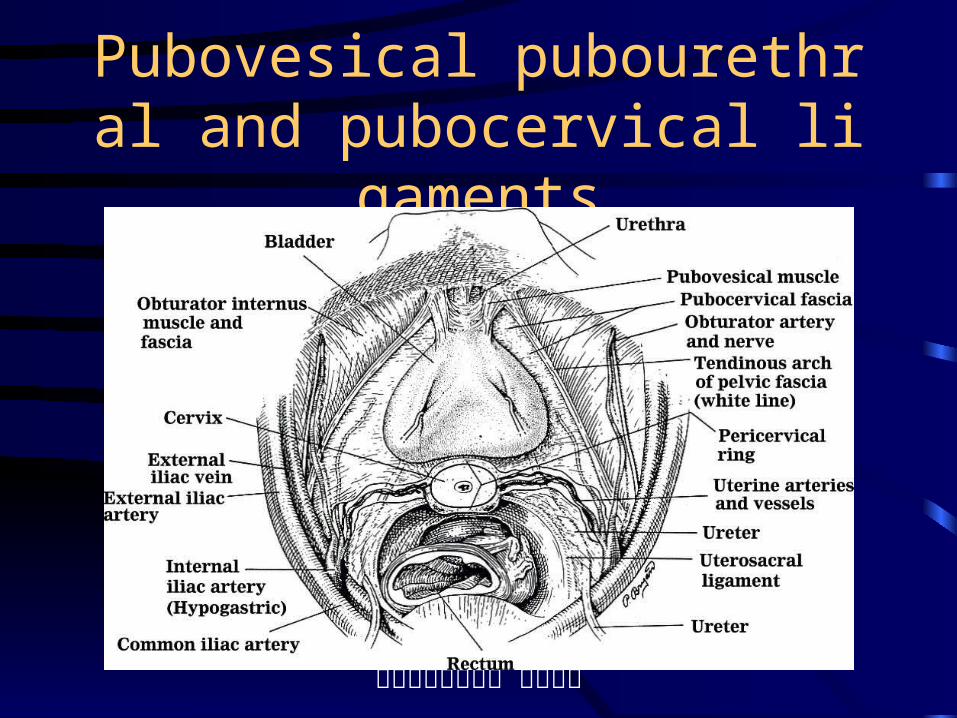
Pubovesical pubourethral and pubocervical ligaments
排尿障礙治療中心 版權所有
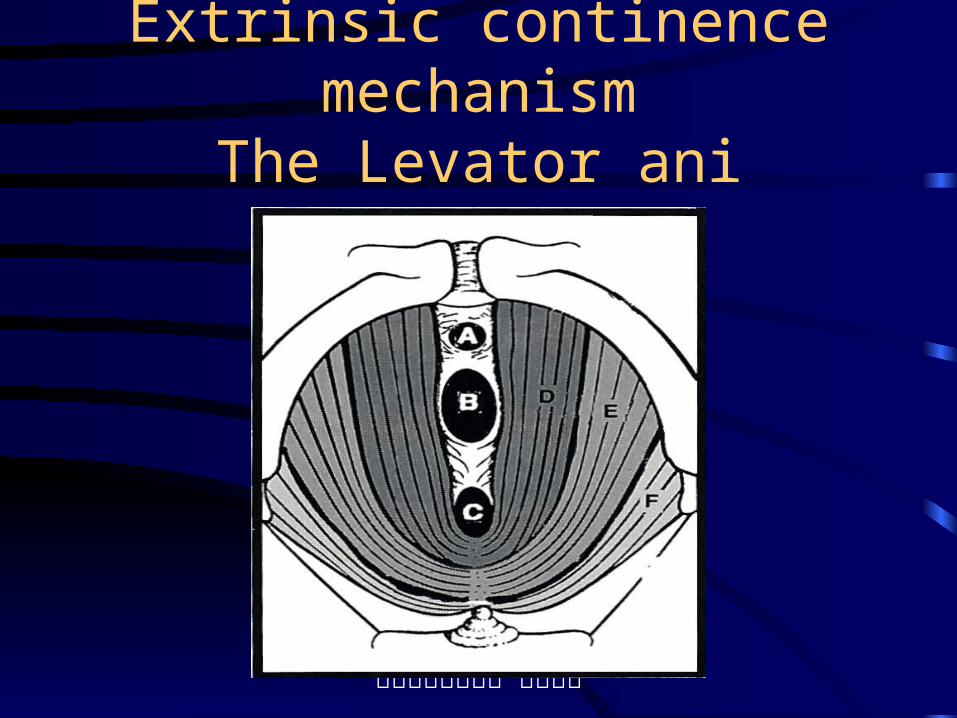
Extrinsic continence mechanismThe Levator ani muscles
排尿障礙治療中心 版權所有
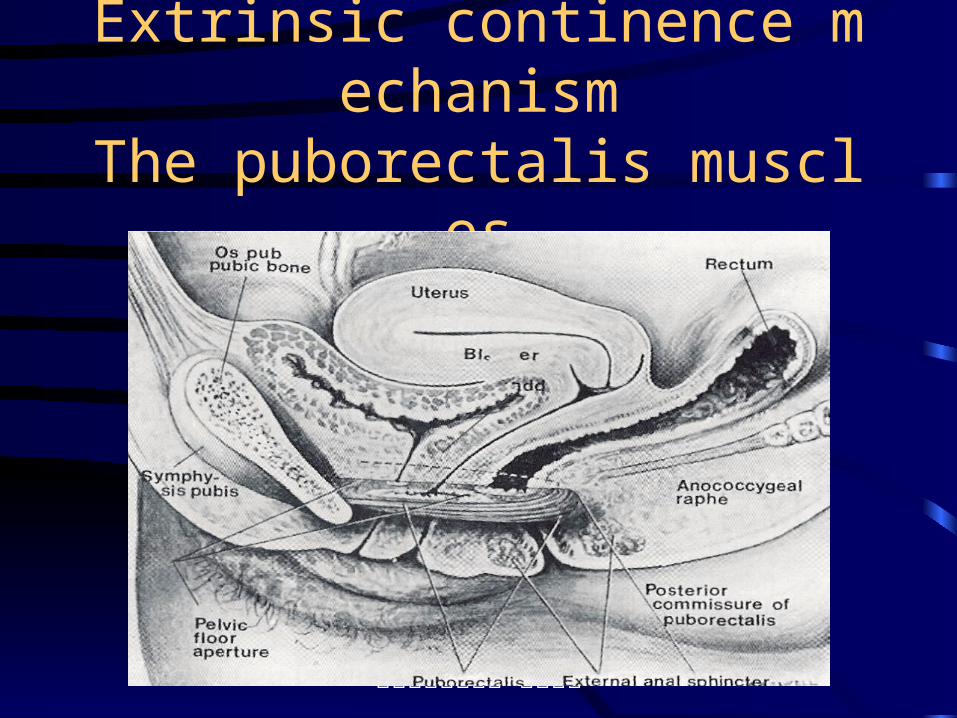
Extrinsic continence mechanismThe puborectalis muscles
排尿障礙治療中心 版權所有
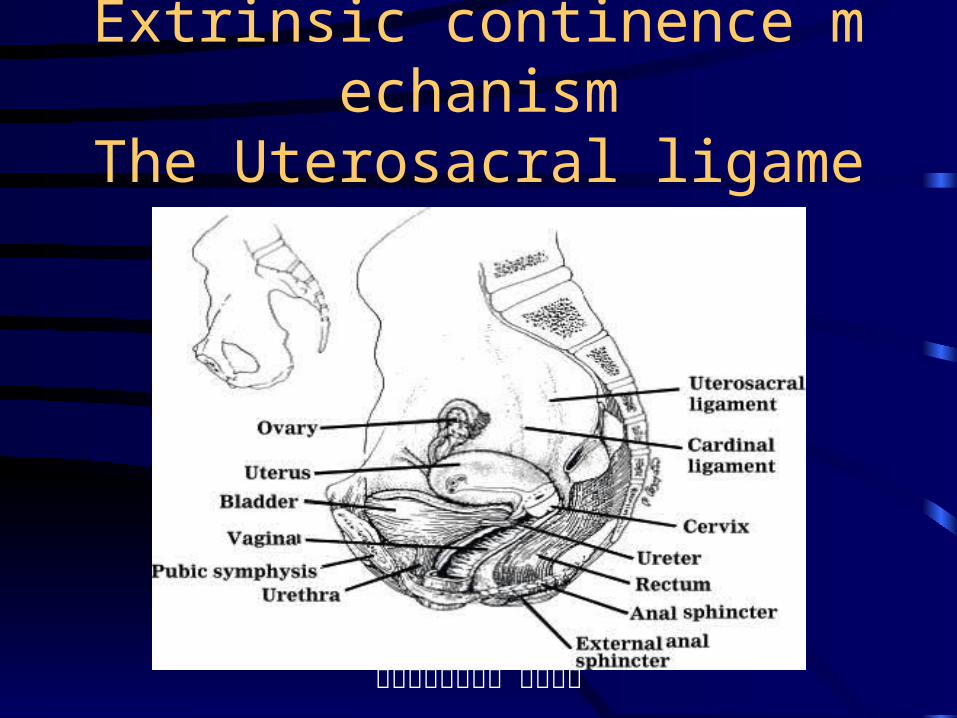
Extrinsic continence mechanismThe Uterosacral ligaments
排尿障礙治療中心 版權所有
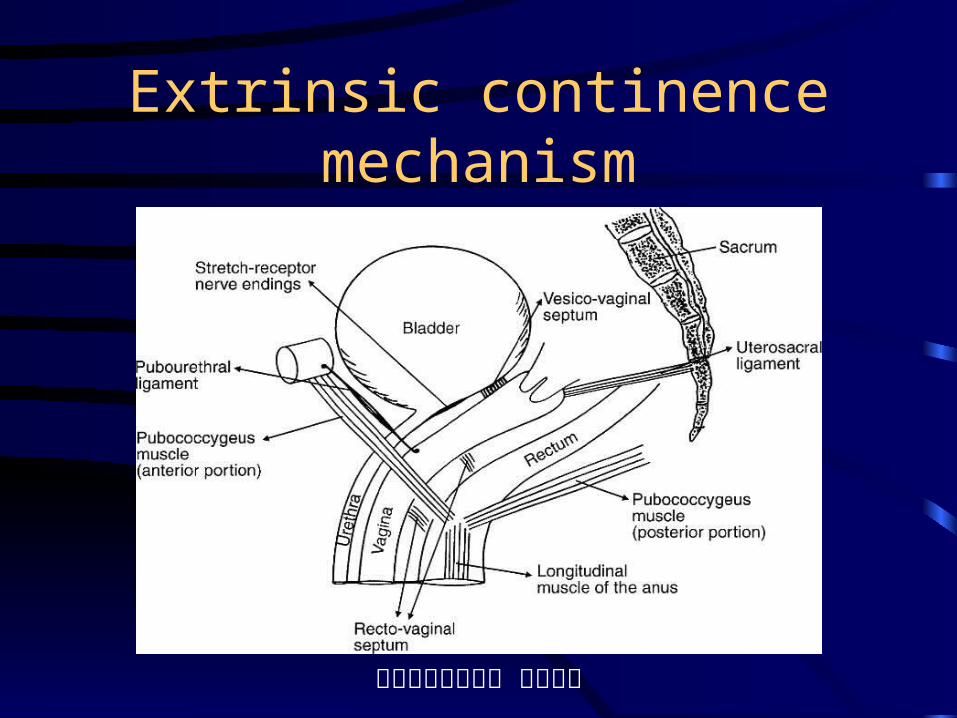
Extrinsic continence mechanism
排尿障礙治療中心 版權所有
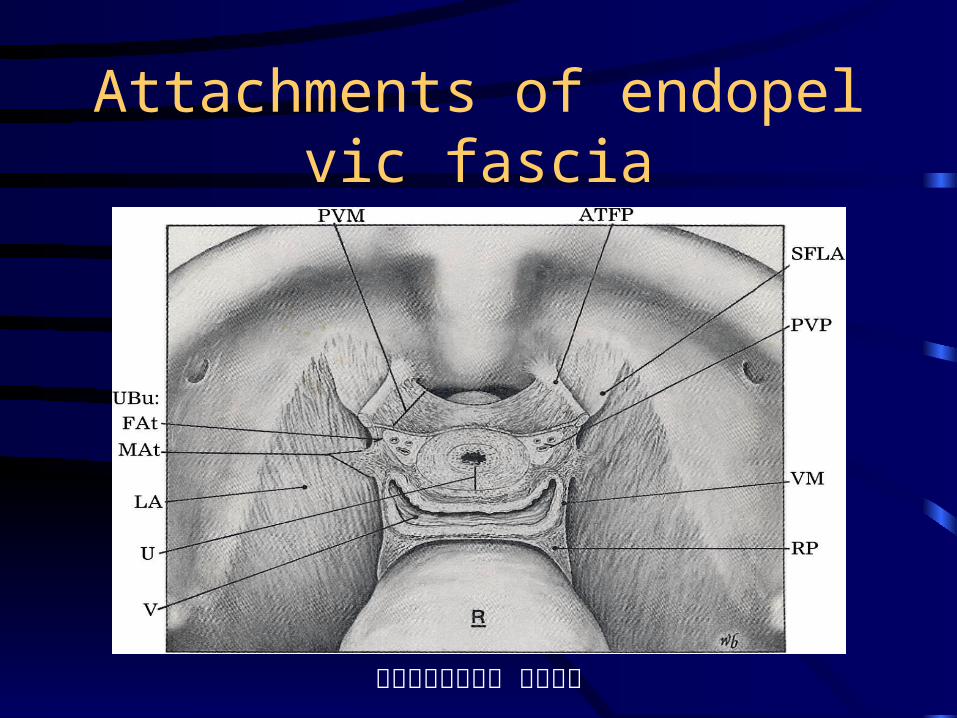
Attachments of endopelvic fascia
排尿障礙治療中心 版權所有
Defects in Exterinsic continence mechanism• Hypermobility of Bladder neck and urethra
• Loss of hammock effect during increased abdominal pressure
• Low pressure transmission ration to urethra
• Causing cystocele or stress incontinence
• Coexisting prolapse
排尿障礙治療中心 版權所有
Causes of defects in Extrinsic continence mechanisms• Multiple childbirth
• Hysterectomy
• Menopause
• Surgical trauma
• Peripheral neuropathy (Pudendal nerve)
• Ageing process
• Chronic debilitative diseases
排尿障礙治療中心 版權所有
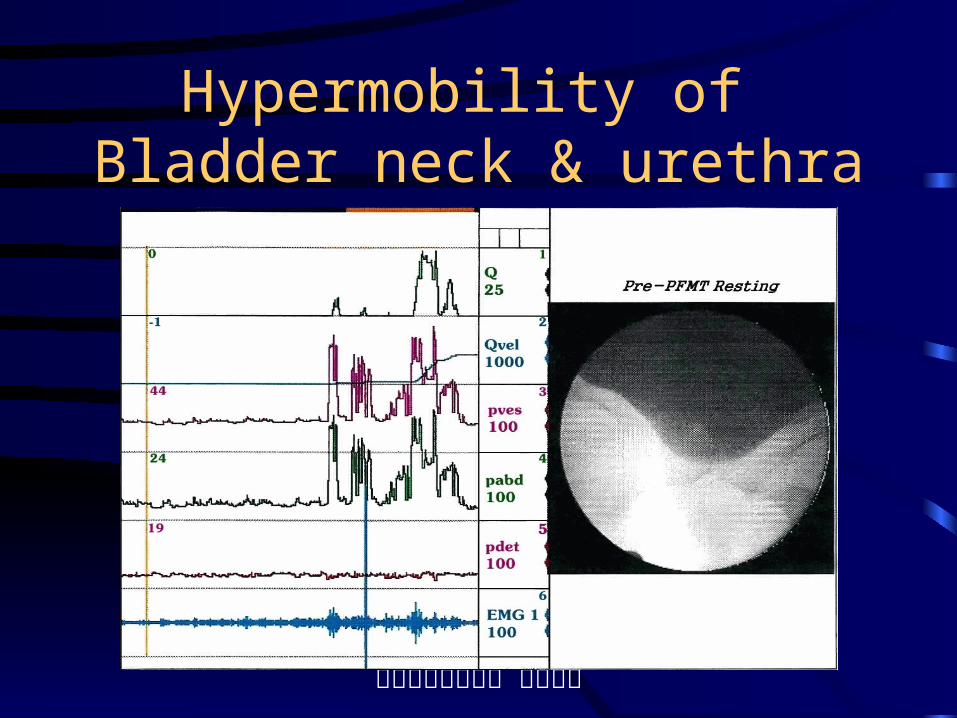
Hypermobility of Bladder neck & urethra
排尿障礙治療中心 版權所有
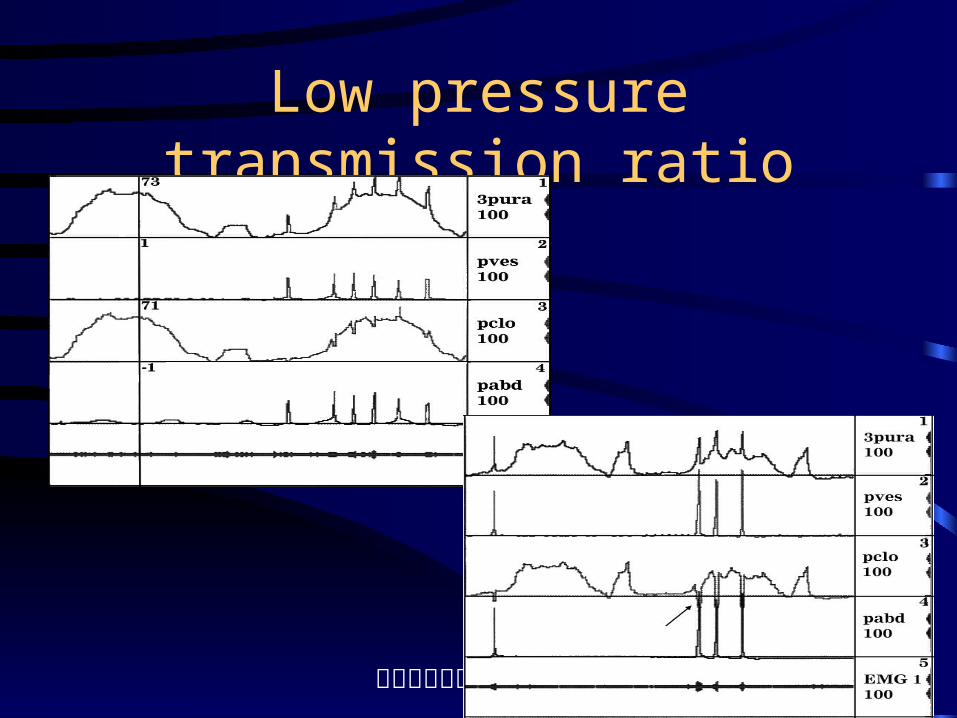
Low pressure transmission ratio
排尿障礙治療中心 版權所有
Cystocele formation in defects of extrinsic continence mechanism
排尿障礙治療中心 版權所有
Intrinsic Continence Mechanism
• Urethral mucosa
• Submucosal vasculature
• Connective tissue
• Urethral smooth muscles
• Urethral striated muscles
排尿障礙治療中心 版權所有
Urethral muscles
• Urethral smooth muscle
Thick inner longitudinal & outer circular m.
Pudendal anesthesia cannot block • Urethral striated muscle
Surround smooth muscle coat
about 20-64% of urethral length
mainly of slow twitch fibers
muscle blocker blocks 40% of muscle tone
排尿障礙治療中心 版權所有
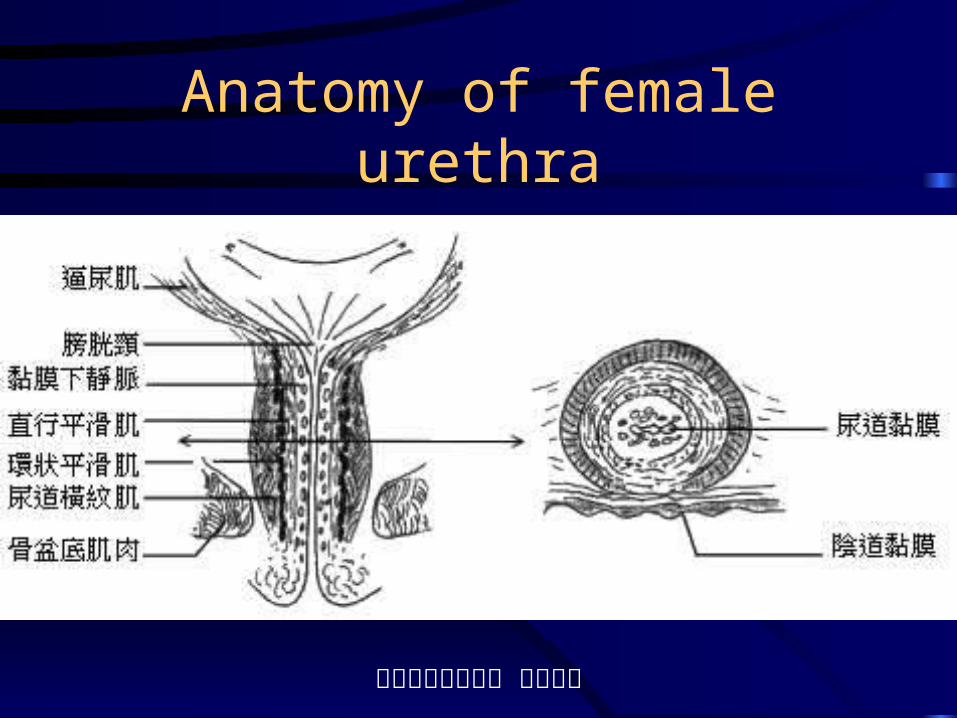
Anatomy of female urethra
排尿障礙治療中心 版權所有
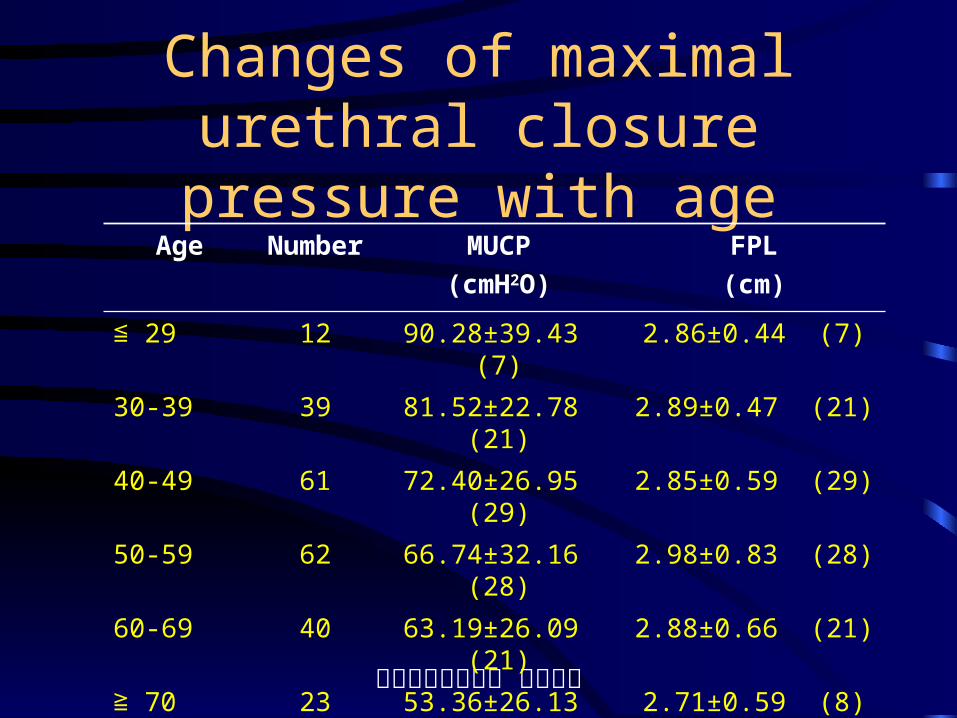
Changes of maximal urethral closure pressure with age
Age Number MUCP
(cmH2O)
FPL
(cm)
≦ 29 12 90.28±39.43 (7) 2.86±0.44 (7)
30-39 39 81.52±22.78 (21) 2.89±0.47 (21)
40-49 61 72.40±26.95 (29) 2.85±0.59 (29)
50-59 62 66.74±32.16 (28) 2.98±0.83 (28)
60-69 40 63.19±26.09 (21) 2.88±0.66 (21)
≧ 70 23 53.36±26.13 (8) 2.71±0.59 (8)
Regression analysis P=0.0010 P=0.8279
Total 237 70.75±29.80 (114) 2.89±0.65 (114)
排尿障礙治療中心 版權所有
Anatomical classification of SUI
• Type I: hypermobility of bladder neck without loss of urethrovesical angle
• Type II: hypermobility of bladder neck with inferior and external rotation of VUJ
• Type III: intrinsic sphincteric deficiency with none or minimal hypermobility
• Mixed type II & III SUI
排尿障礙治療中心 版權所有
Classification of SUI by Leak-point pressures
• Type 1 SUI : Abdominal leak-point pressure >120cm water with hypermobility
• Type 2 SUI : ALPP >90 cm water with urethral hypermobility
• Mixed type 2 & 3 SUI : 60 <ALPP< 90 with hypermobility
• Type 3 SUI : ALPP < 60 cm water without hypermobility
排尿障礙治療中心 版權所有
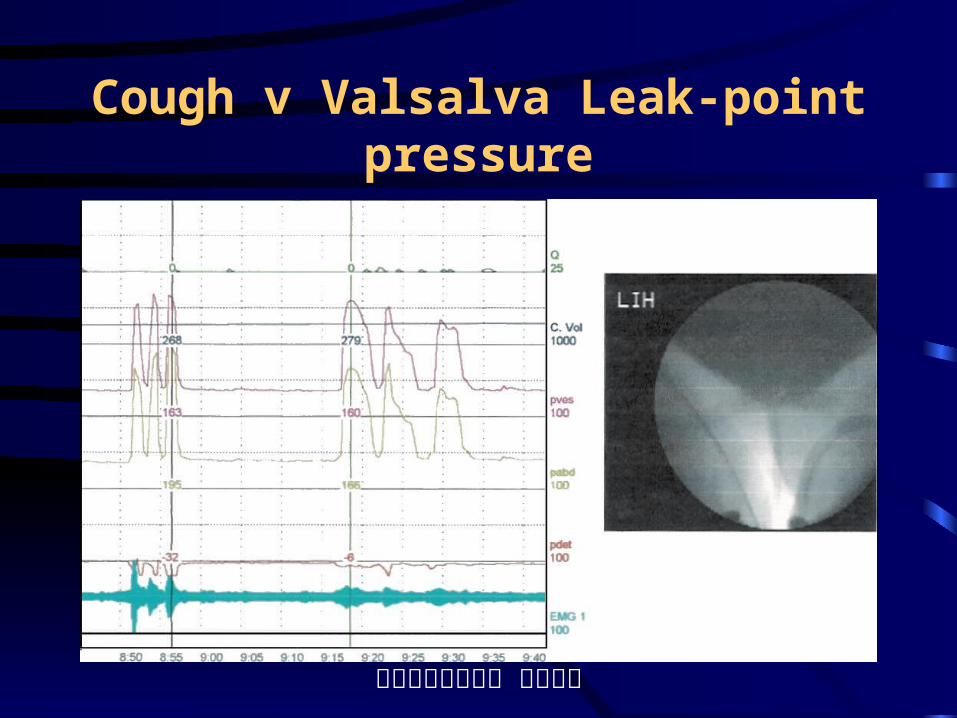
Cough vs Valsalva LPP
• Cough induced reflexic contraction of levator ani and enhance urethral closure by vaginal endopelvic fascia, against urethral resistance and extrinsic continence mechanism
• Valsalva maneuver causing bearing down of pelvic floor muscles, against intra-urethral resistance
• CLPP > VLPP in most cases with SUI
排尿障礙治療中心 版權所有
Continence mechanism and LPP
排尿障礙治療中心 版權所有
Grades of Stress incontinence
• Rare: occur less than 1/month, small amount, no pad protection
• Minimal: occur only with severe straining, small amount, no pad protection
• Moderate: occur with mild straining, pad protection is needed
• Severe: occur with changing position or total incontinence
排尿障礙治療中心 版權所有
Diagnosis of stress incontinence
• Symptomatology: grades of SUI, types of urinary incontinence
• Physical signs: demonstration of incontinence or fistula, associated with cystocele or uterine prolapse
• Endosonography of bladder & urethral• Urodynamic study• Leak point pressure measurement
排尿障礙治療中心 版權所有
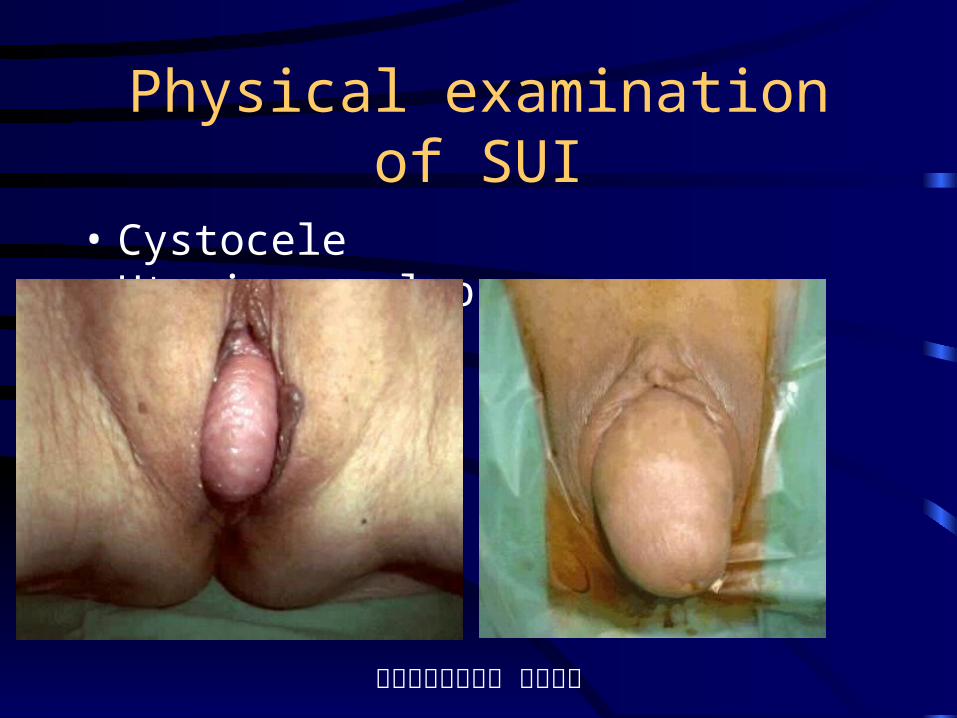
Physical examination of SUI
• Cystocele Uterine prolapse

排尿障礙治療中心 版權所有
Ectopic ureteral orifice & urinary incontinence

排尿障礙治療中心 版權所有
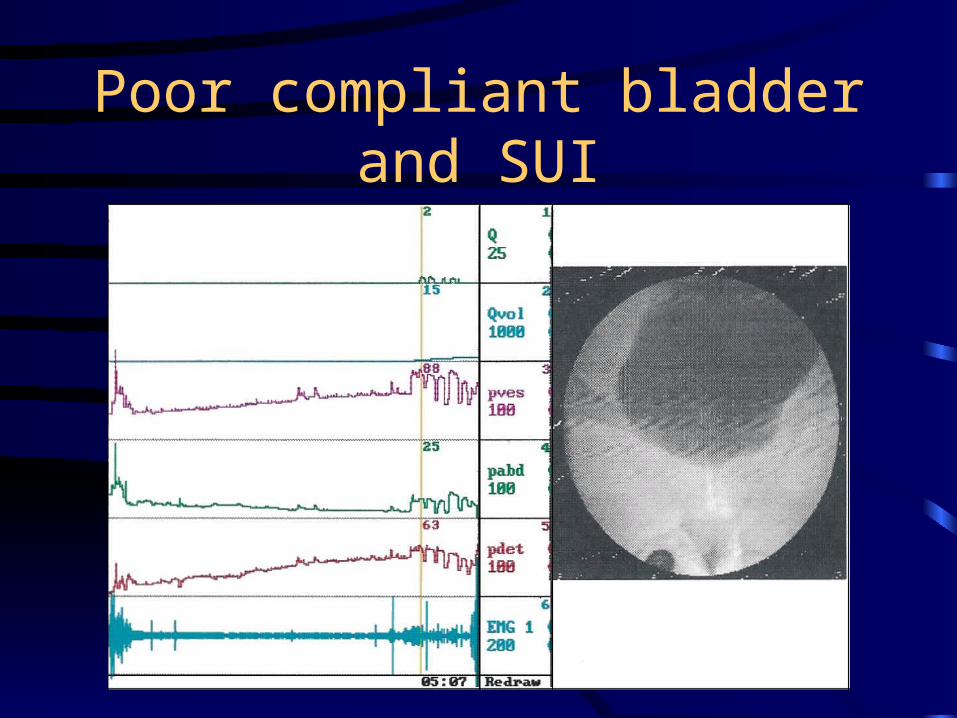
Urodynamic study for SUI
• Routine cystometry cannot confirm SUI, but can diagnose detrusor overactivity and low compliant bladder
• Leak point pressure is a better diagnostic tool to stage stress incontinence
• Maximal urethral closure pressure has a low but significant correlation with ISD
排尿障礙治療中心 版權所有
Poor compliant bladder and SUI
排尿障礙治療中心 版權所有
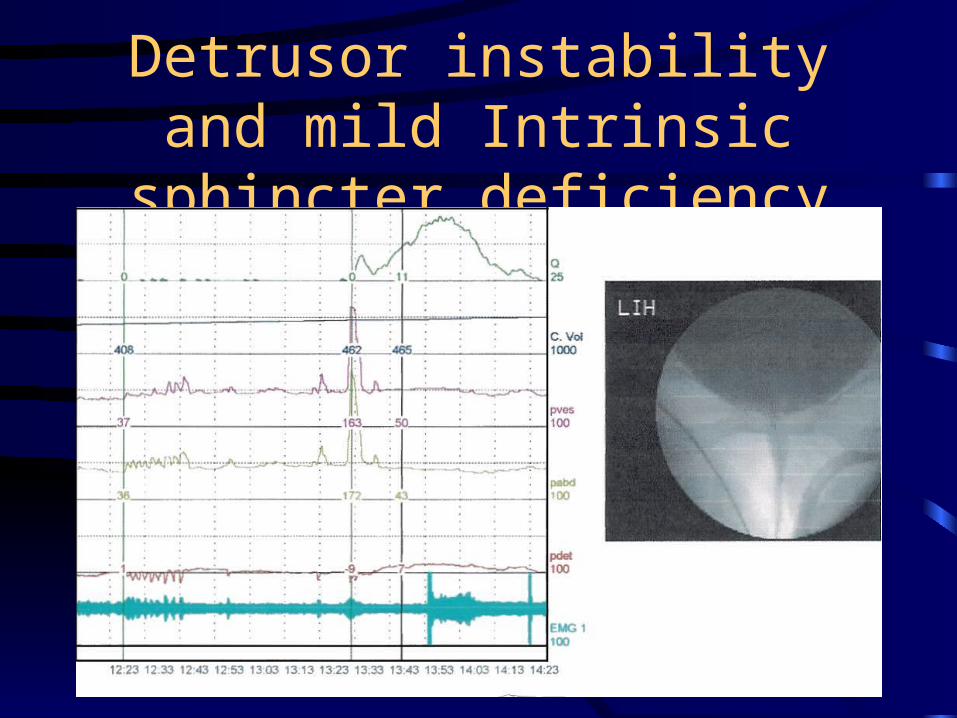
Detrusor instability and mild Intrinsic sphincter deficiency
排尿障礙治療中心 版權所有
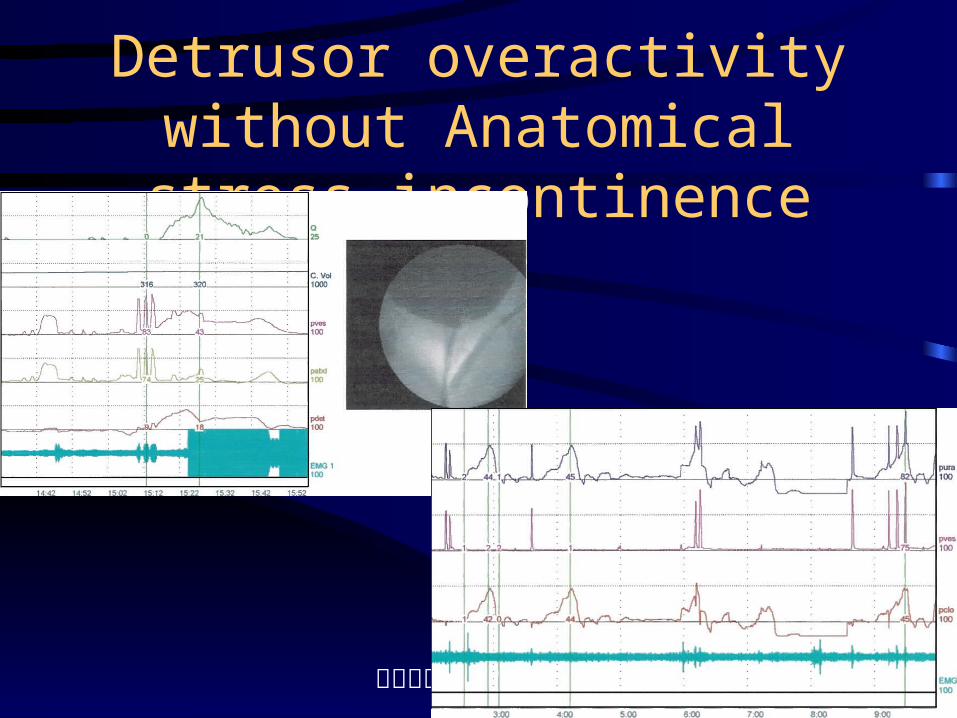
Videourodynamics in SUI
• Videourodynamic study can determine leak point pressures and the bladder neck hypermobility during stress
• Leakage of urine is clearly demonstrated and the accurate leak point pressure can be measured
• Concomitant pressure flow study to avoid misdiagnosis of bladder outlet obstruction
排尿障礙治療中心 版權所有
Detrusor overactivity without Anatomical stress incontinence
排尿障礙治療中心 版權所有
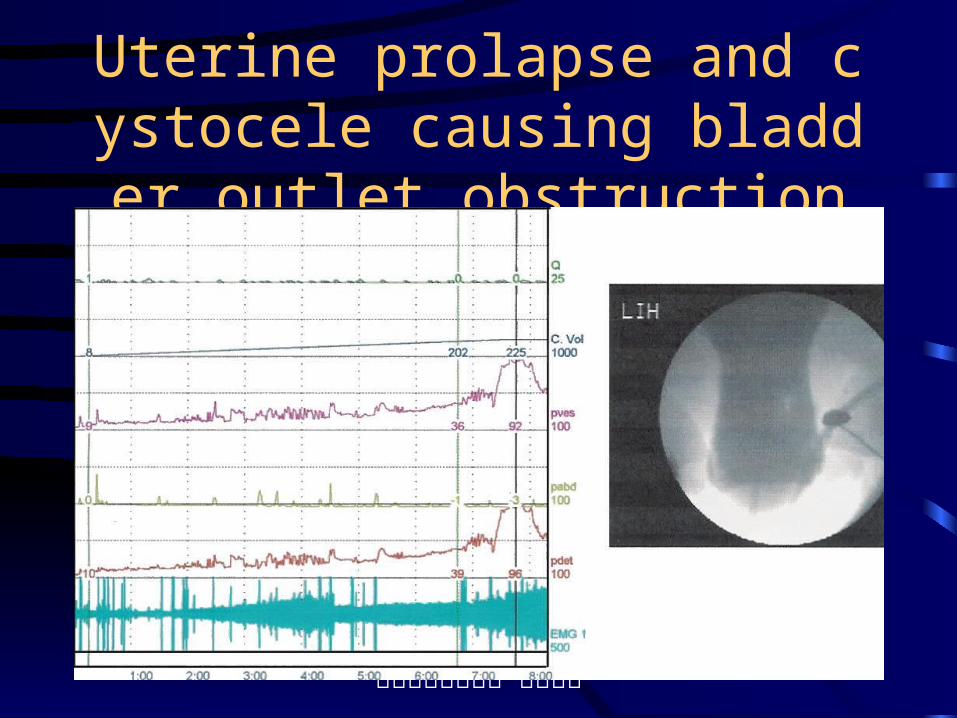
Uterine prolapse and cystocele causing bladder outlet obstruction
排尿障礙治療中心 版權所有
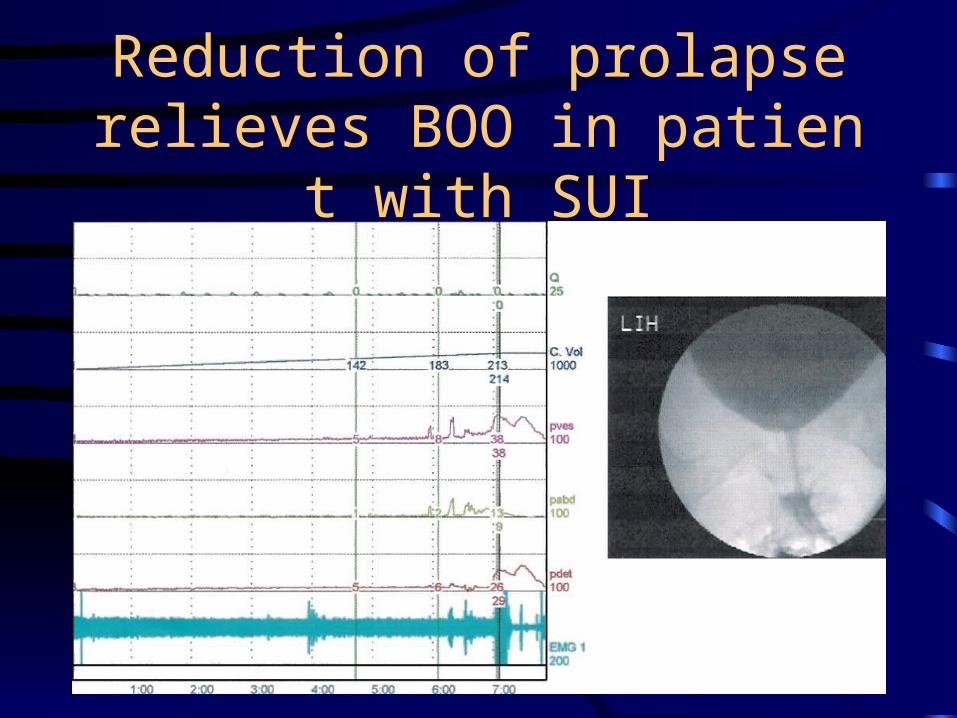
Reduction of prolapse relieves BOO in patient with SUI
排尿障礙治療中心 版權所有
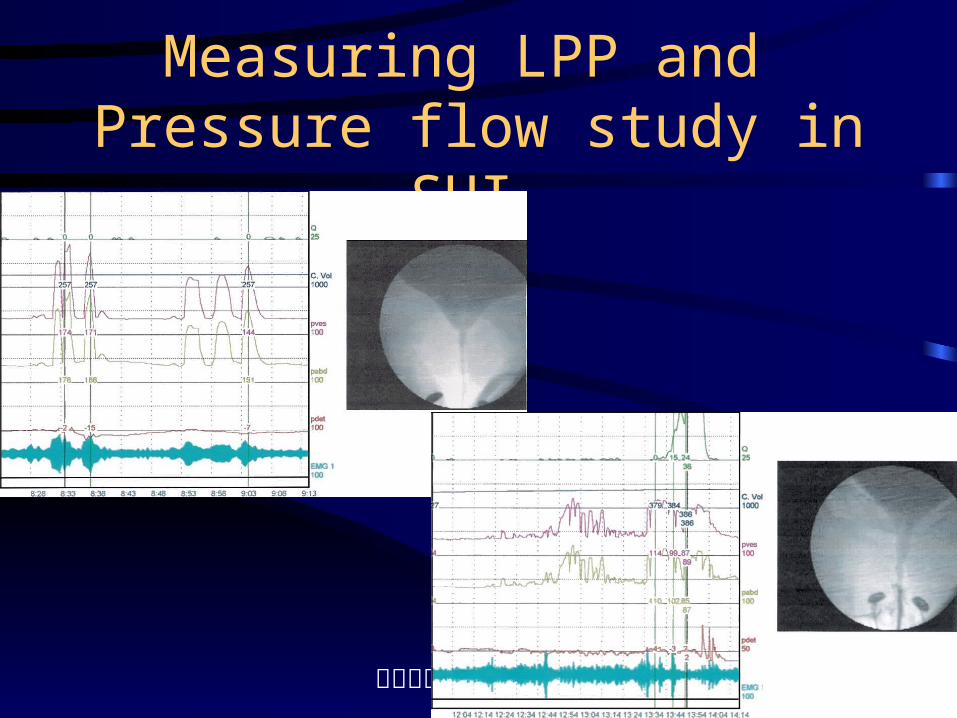
Measuring LPP and Pressure flow study in SUI
排尿障礙治療中心 版權所有
Leak point pressure in SUI
• Cough LPP and Valsalva LPP should be measured concomitantly
• VLPP measures intrinsic urethral resistance
• CLPP measures resistance from intrinsic and extrinsic continence mechanisms
• Measure the pressure at exactly the point that urine loss
排尿障礙治療中心 版權所有
Cough v Valsalva Leak-point pressure
排尿障礙治療中心 版權所有
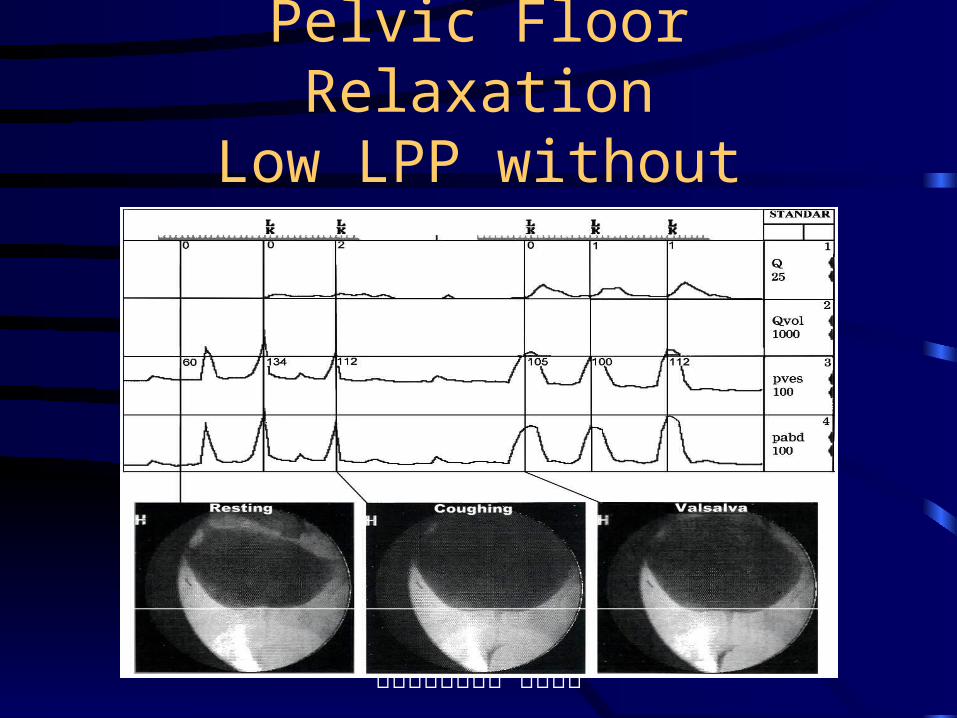
Pelvic Floor RelaxationLow LPP without Hypermobility
排尿障礙治療中心 版權所有
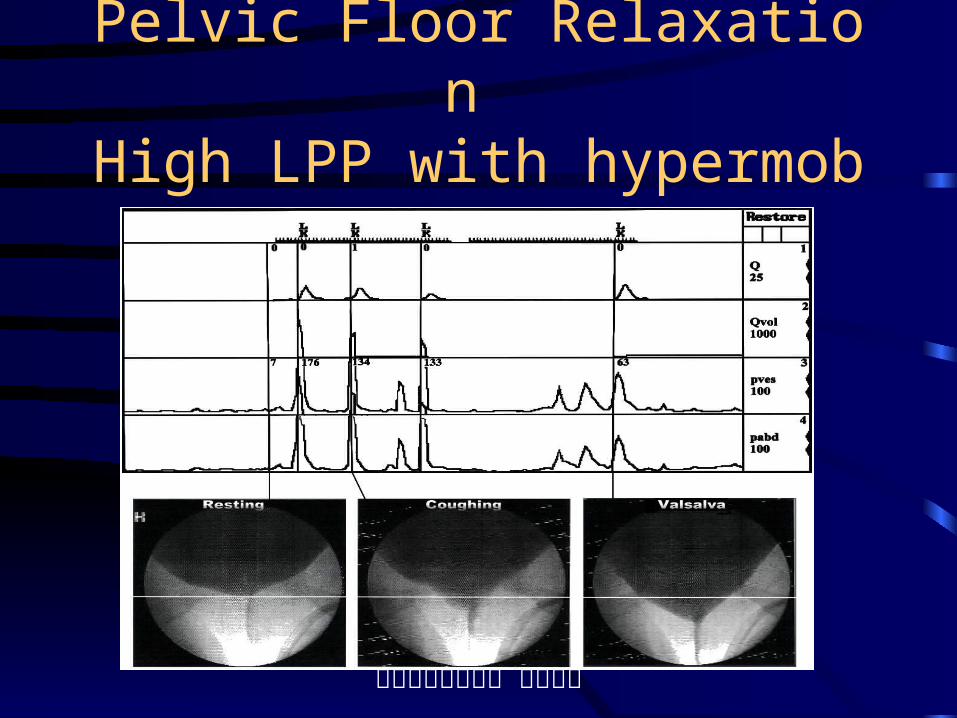
Pelvic Floor Relaxation High LPP with hypermobility
排尿障礙治療中心 版權所有
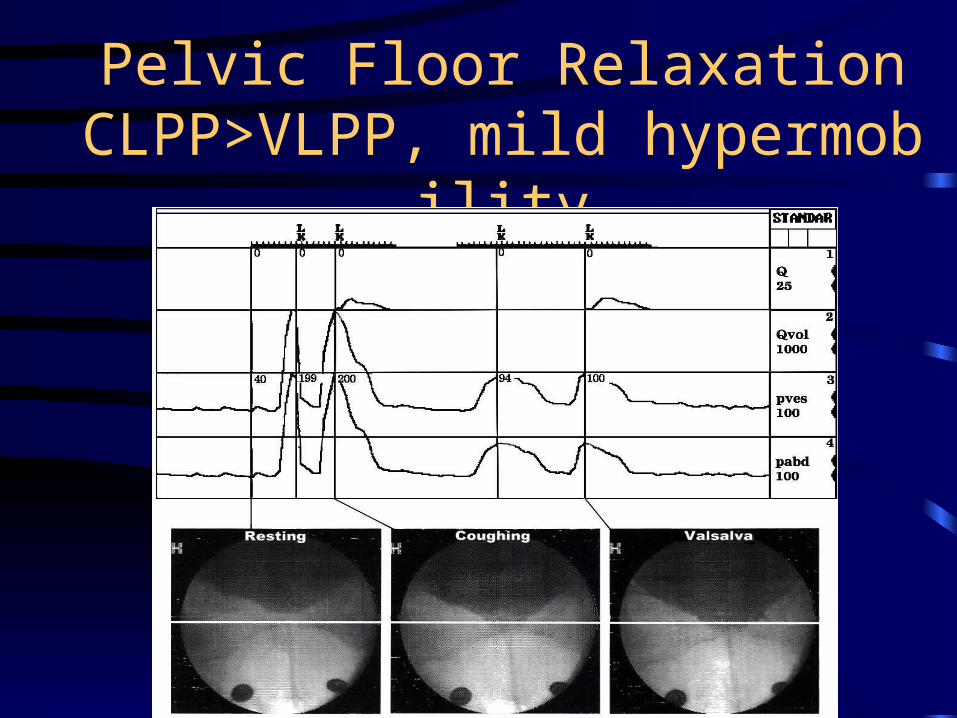
Pelvic Floor RelaxationCLPP>VLPP, mild hypermobility
排尿障礙治療中心 版權所有
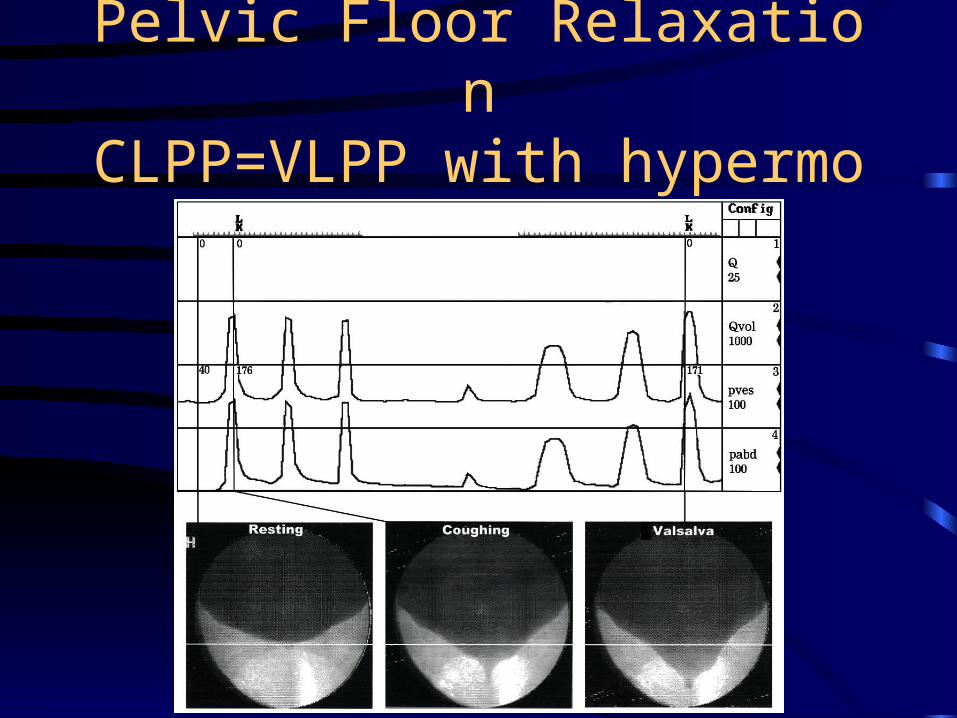
Pelvic Floor RelaxationCLPP=VLPP with hypermobility
排尿障礙治療中心 版權所有
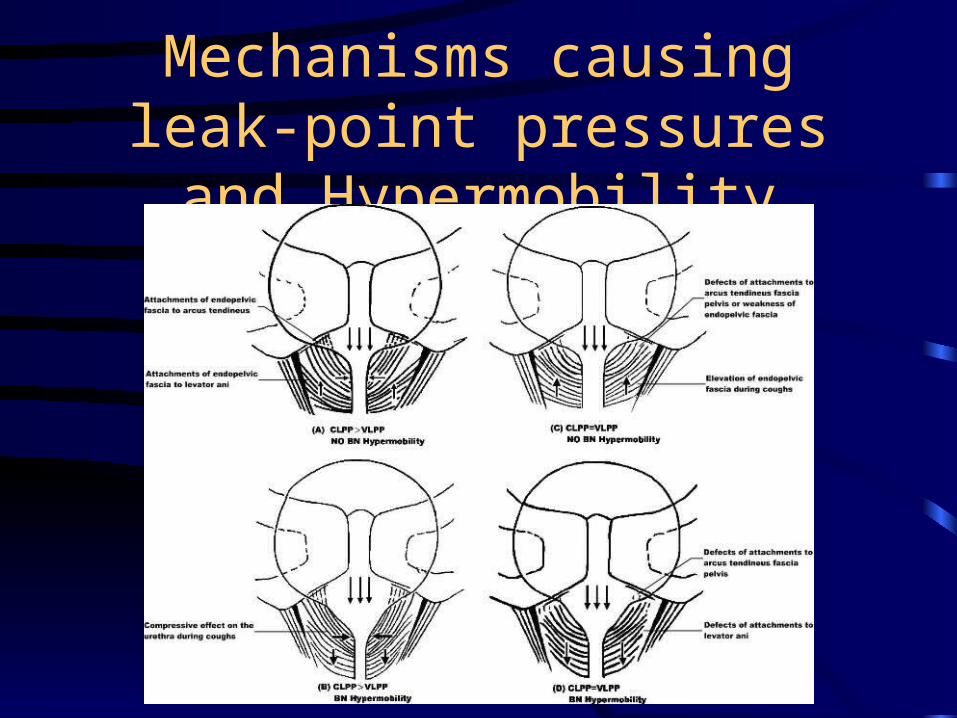
Mechanisms causing leak-point pressures and Hypermobility
排尿障礙治療中心 版權所有
Urethral pressure profilometry in Diagnosis of SUI
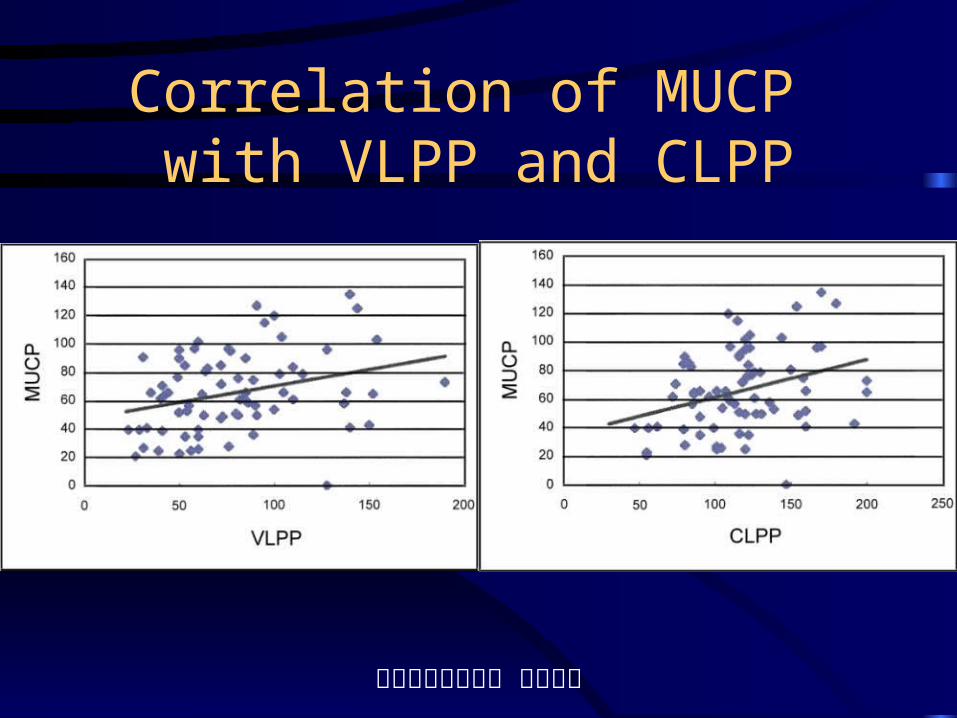
• Perfusion UPP or microtip catheter UPP• A lower MUCP was measured by microtip
catheter• A lower MUCP is associated with a lower
Valsalva LPP (p=0.011) and cough LPP (p= 0.005)
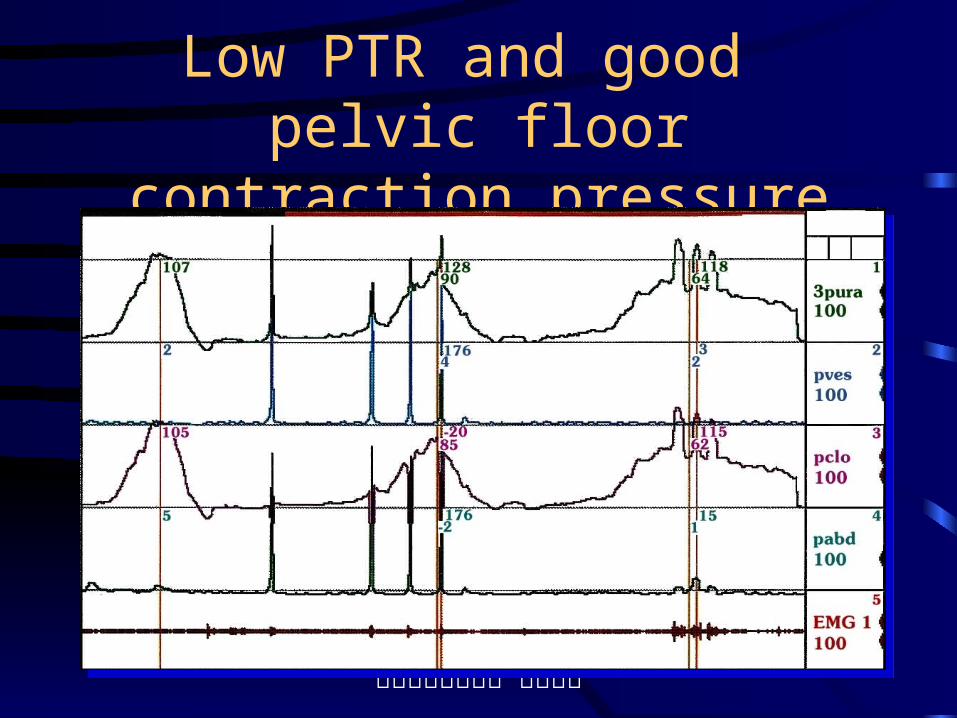
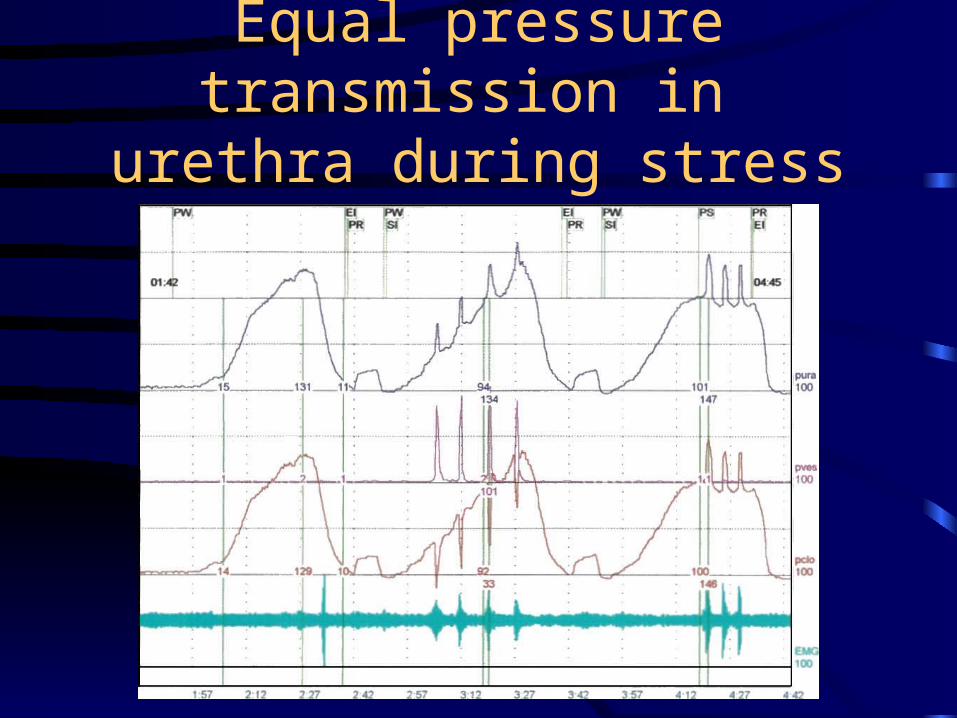
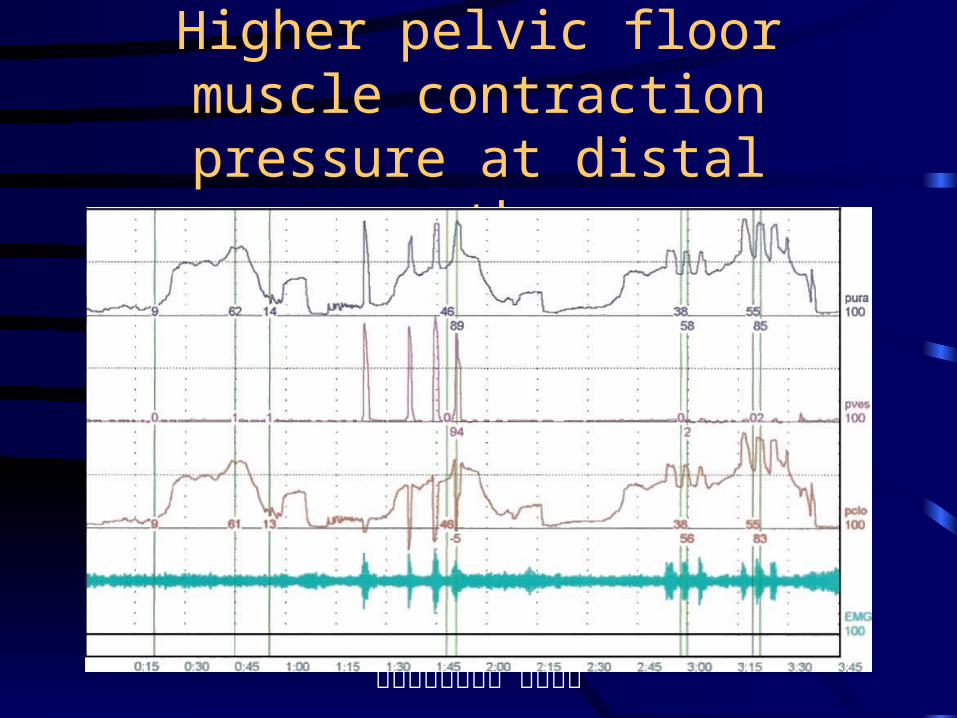
• Dynamic UPP to measure pelvic floor muscle contractility and effect on urethra
排尿障礙治療中心 版權所有
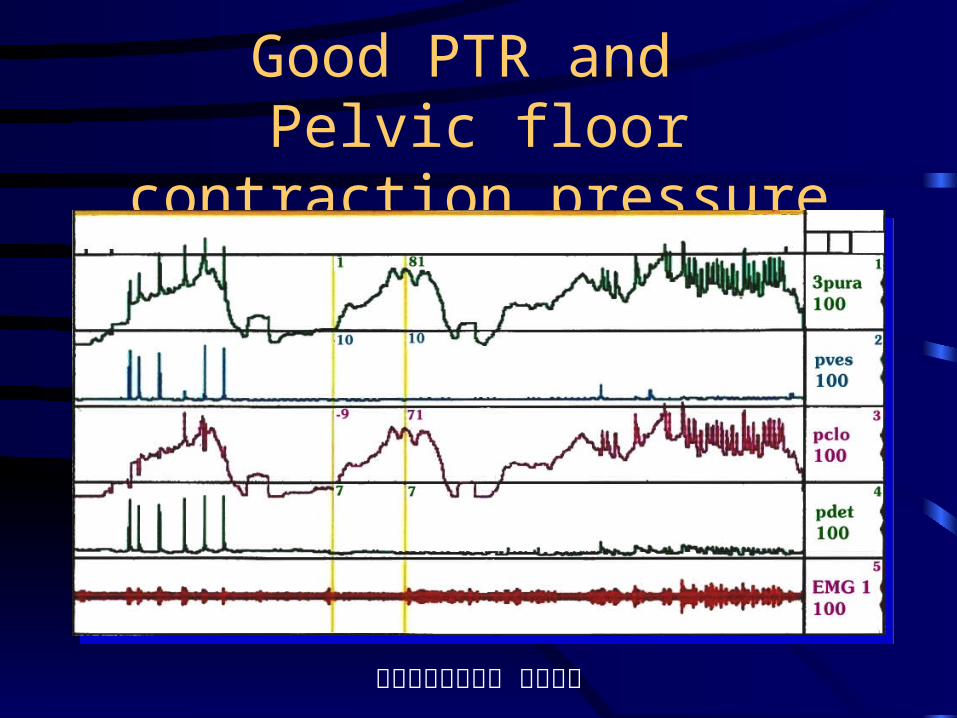
Good PTR and Pelvic floor contraction pressure
排尿障礙治療中心 版權所有
Low PTR and good pelvic floor contraction pressure
排尿障礙治療中心 版權所有
Equal pressure transmission in urethra during stress UPP
排尿障礙治療中心 版權所有
Higher pelvic floor muscle contraction pressure at distal urethra
排尿障礙治療中心 版權所有
Correlation of MUCP with VLPP and CLPP
排尿障礙治療中心 版權所有
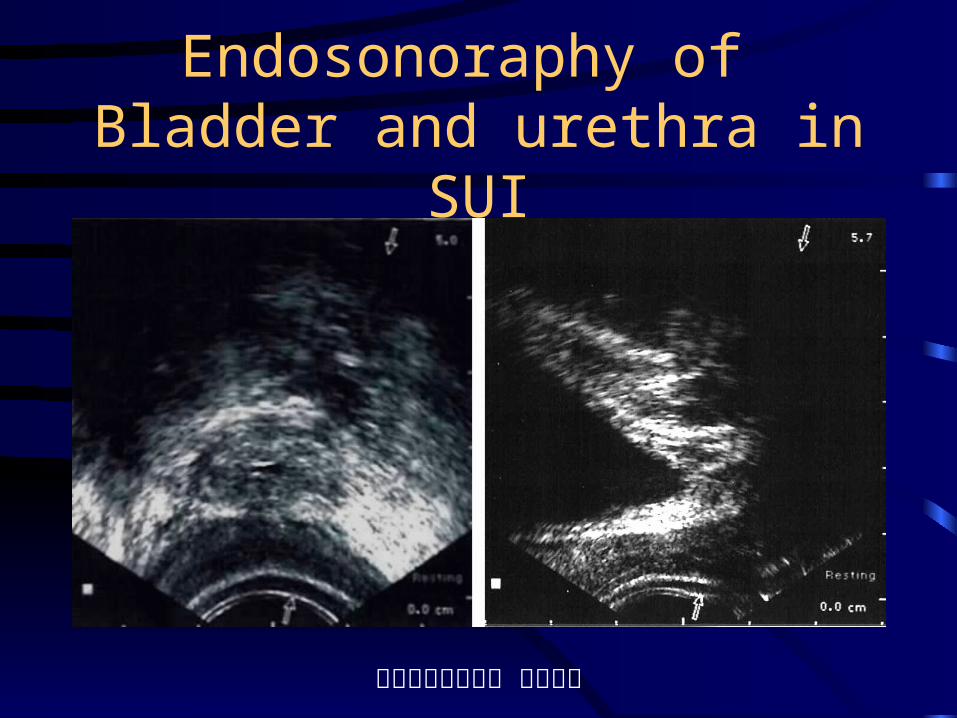
Endosonoraphy of Bladder and urethra in SUI

排尿障礙治療中心 版權所有
Measurement of Urethral striated muscle component
排尿障礙治療中心 版權所有
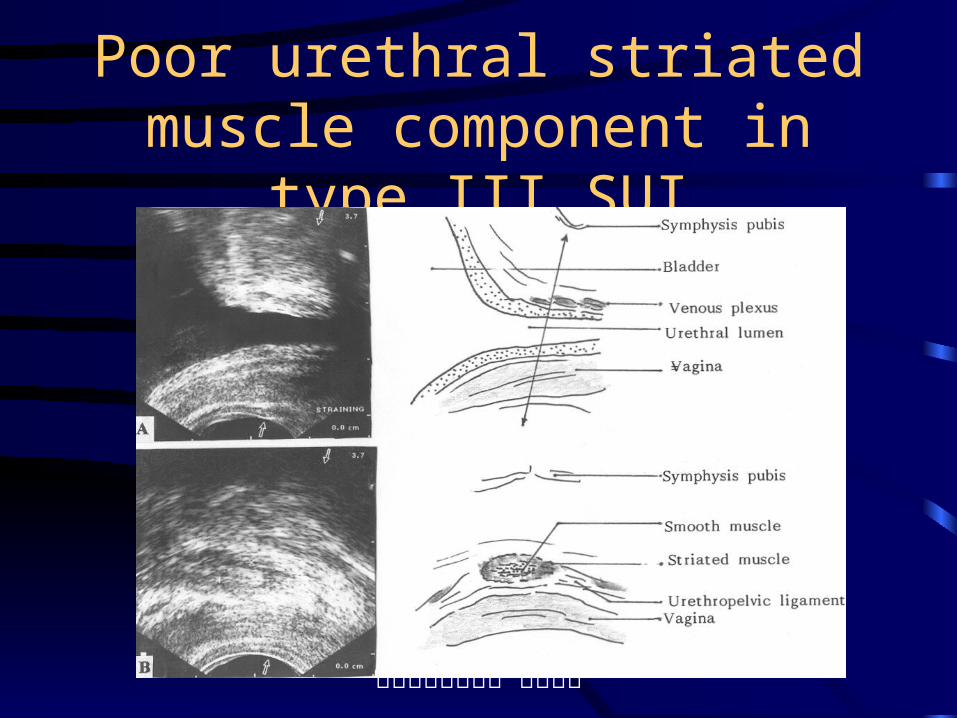
Poor urethral striated muscle component in type III SUI
排尿障礙治療中心 版權所有
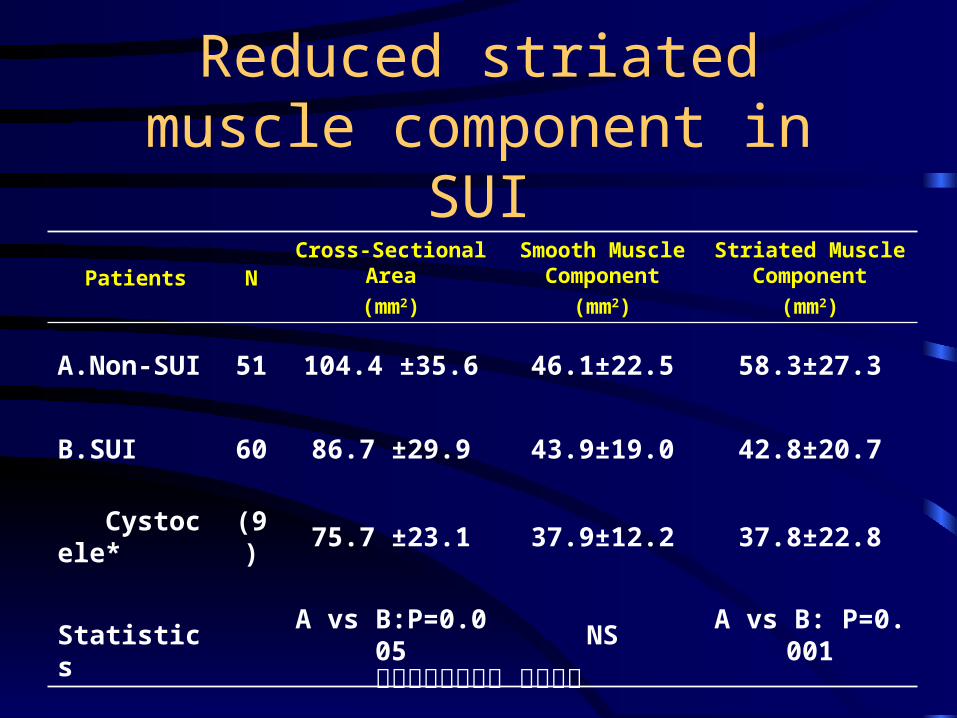
Reduced striated muscle component in SUI
Patients NCross-Sectional Area
(mm2)
Smooth Muscle Component
(mm2)
Striated Muscle Component
(mm2)
A.Non-SUI 51 104.4 ±35.6 46.1±22.5 58.3±27.3
B.SUI 60 86.7 ±29.9 43.9±19.0 42.8±20.7
Cystocele* (9) 75.7 ±23.1 37.9±12.2 37.8±22.8
Statistics A vs B:P=0.005 NS A vs B: P=0.001
排尿障礙治療中心 版權所有
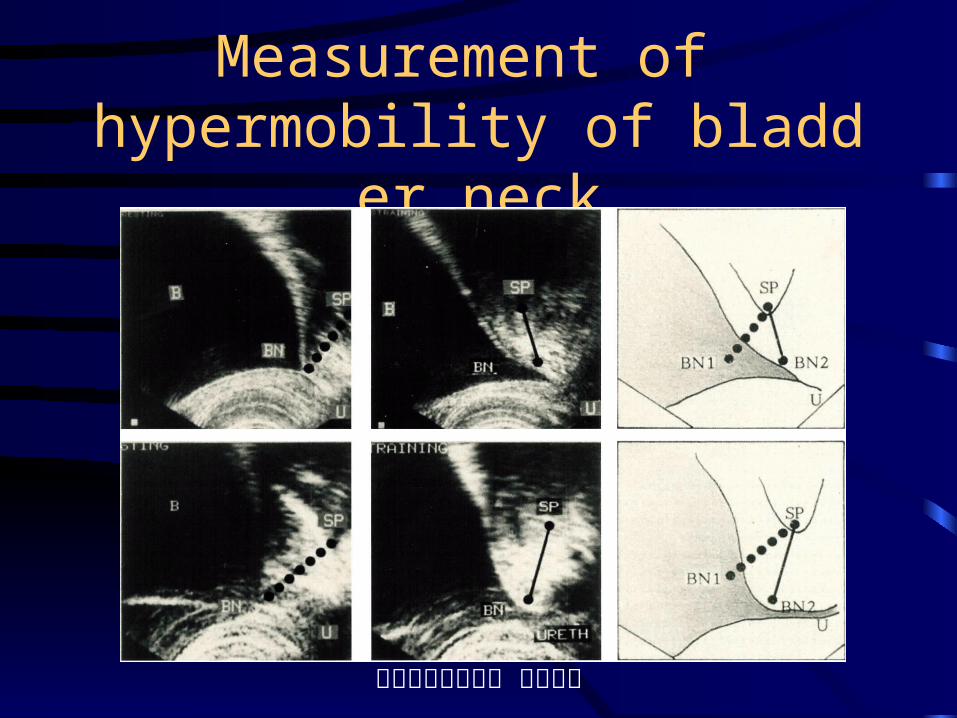
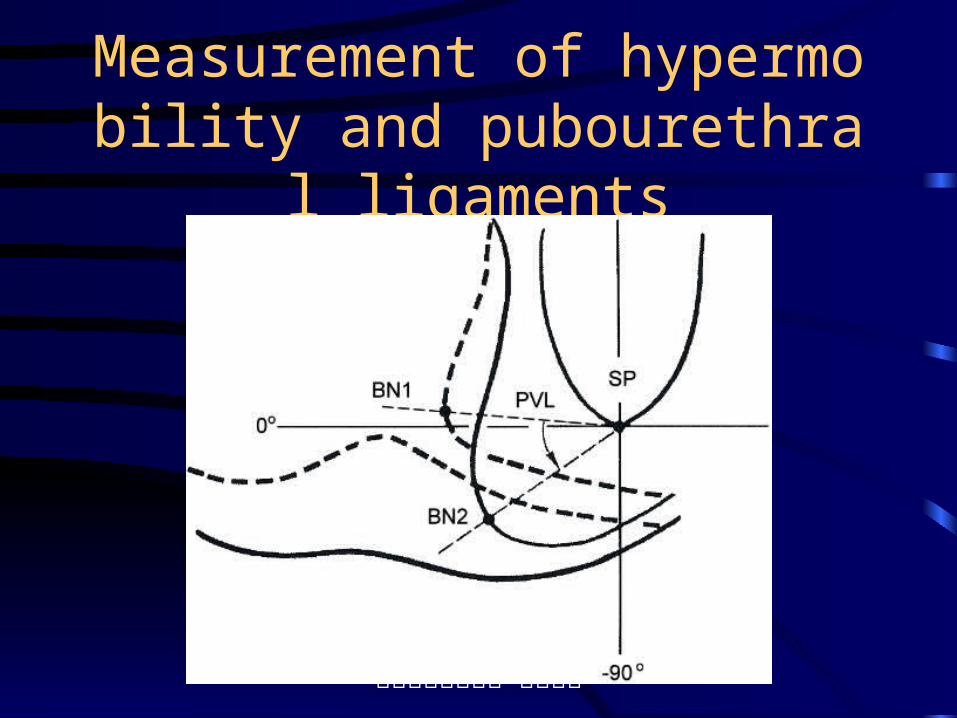
Measurement of hypermobility of bladder neck
排尿障礙治療中心 版權所有
Measurement of hypermobility and pubourethral ligaments
排尿障礙治療中心 版權所有
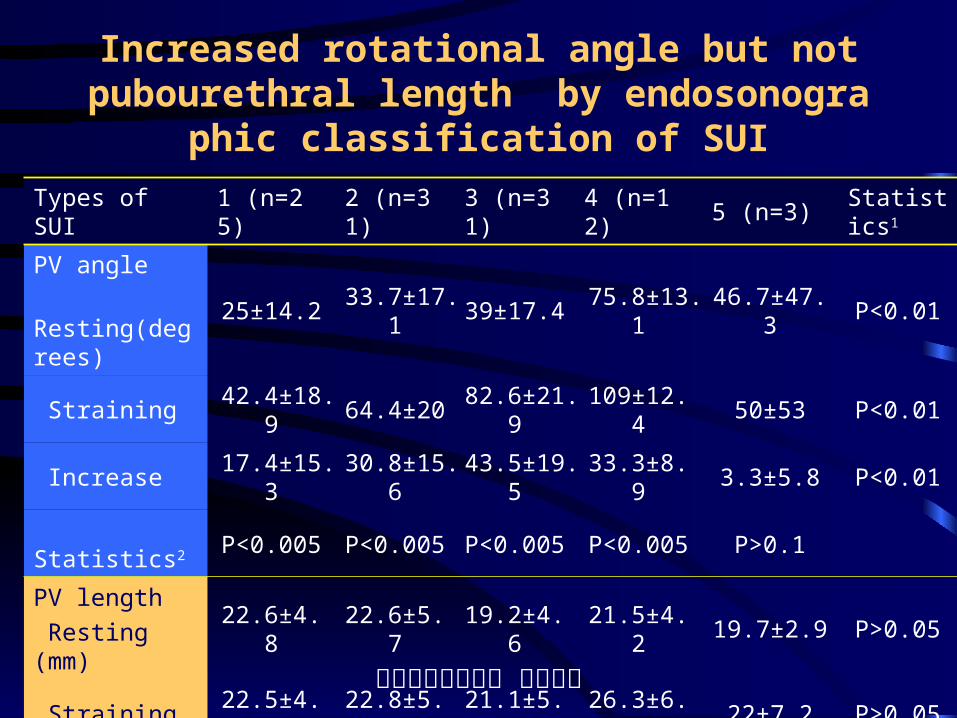
Increased rotational angle but not pubourethral length by endosonographic classification of SUI
Types of SUI 1 (n=25) 2 (n=31) 3 (n=31) 4 (n=12) 5 (n=3) Statistics1
PV angle
Resting(degrees)
25±14.2 33.7±17.1 39±17.4 75.8±13.1 46.7±47.3 P<0.01
Straining 42.4±18.9 64.4±20 82.6±21.9 109±12.4 50±53 P<0.01
Increase 17.4±15.3 30.8±15.6 43.5±19.5 33.3±8.9 3.3±5.8 P<0.01
Statistics2 P<0.005 P<0.005 P<0.005 P<0.005 P>0.1
PV length
Resting (mm)22.6±4.8 22.6±5.7 19.2±4.6 21.5±4.2 19.7±2.9 P>0.05
Straining 22.5±4.5 22.8±5.7 21.1±5.1 26.3±6.8 22±7.2 P>0.05
Increase 0.1±1.59 0.2±3.04 1.9±3.72 4.8±4.94 2.3±4.51
Statistics2 P>0.4 P>0.3 P>0.005 P>0.005 P>0.2
排尿障礙治療中心 版權所有
Diagnosis of Stress Incontinence
• Determine the underlying pathophysiology causing incontinence
• Therapeutic modality depends on grades of SUI
• Correct the exact defects in continence mechanisms
• Search for coexisting mixed incontinence and vaginal prolapse