30 años del tratamiento sistémico del cáncer de...
TRANSCRIPT

30 Años del Tratamiento Sistémico del Cáncer
de Cabeza y Cuello Localmente Avanzado
Avances y Retos Pendientes
Dra. Elvira del Barco
Hospital Clínico Universitario, Salamanca

30 Años del….
La paradoja
del tratamiento sistémico en CCLA
• Es un tumor frecuente
• Es un tumor quimiosensible (más que muchos otros)
• Usos: inducción, concomitante, adyuvancia
• Hay pocas cosas claramente establecidas
• Resultados no son buenos (supervivencia, toxicidad, calidad de vida)
• Las estrategias de integración siguen siendo objeto de debate
…….Sigue utilizándose (y mucho)
¿Existen otros caminos que permiten llegar al mismo lugar, dejando
las limitaciones que comúnmente tenemos, por otras que no hemos
experimentado ?
CAMBIAR PARADIGMAS
Dejar de hacer lo mismo de la misma manera

TREATMENT BY CHEMOTHERAPY (CYCLOPHOSPHAMIDE)
AND TELECOBALTOTHERAPY ASSOCIATION OF ADVANCED
LARYNGEAL AND PHARYNGO-LARYNGEAL CANCERS (44
CASES)].
CACHIN Y, PIET R, LALANNE JC, BRULE G.
Ann Otolaryngol Chir Cervicofac. 1963 Dec;80:959-70.
SYSTEMIC THERAPY WITH AMETHOPTERIN IN SQUAMOUS
CARCINOMA OF THE HEAD AND NECK.
PAPAC RJ, JACOBS EM, FOYE LV Jr, DONOHUE DM.
Cancer Chemother Rep. 1963 Oct;32:47-54.

Chemotherapy of advanced head and neck cancer with a combination of bleomycin,
vincristine, methotrexate and hydroxyuree or cis-dichloro-diamino-platinium. Analysis of local and
general parameters of prognosis (author's transl)
Pouillart P, Palangie T, Garcia-Giralt E, Jouve M, Bataini JP, Jaulerry M, Brugère J, Asselin B.
Bull Cancer. 1980;67(3):269-80. French.
Chemotherapy of advanced head and neck cancer with methotrexate, bleomycin, and
cis-diamminedichloroplatinum II in an effective outpatient schedule.
Vogl SE, Kaplan BH.
Cancer. 1979 Jul;44(1):26-31.
Induction chemotherapy in advanced
squamous head and neck carcinoma with high-dose cis-platinum and
bleomycin infusion.
Hong WK, Shapshay SM, Bhutani R, Craft ML, Ucmakli A, Yamaguchi
KT, Vaughan CW, Strong MS. Cancer. 1979
The role of cis-platinum in solid-tumor therapy
Einhorn LH, Williams SD.
N Engl J Med. 1979 Feb 8;300(6):289-91.

QUIMIOTERAPIA DE INDUCCIÓN
DÉCADA DE LOS 80-90........
Supervivencia No beneficios excepto 2 estudios GSTTC. Pacagnella, 1994 Sp 10 años: 16% vs 6% en irresecables GETTEC. Domengne, 2000 Mediana SV: 5.1 vs 3.3 . BENEFICIOS EN RESECABLES Y NO RESECABLES
Preservación de órgano (QTI RT vs CIRUGIART)
VALGS, 1991 Laringe RT SOLO A LOS QUE RESPONDEN Preservación L-5 años: 39%
EORTC. Lefebvre, 1996 Hipofaringe Preservación L-5 años: 35% Menos mts a distancia aunque igual SV
QTI CON CDDP-5FU SEGUIDO DE RT CONSIGUE PRESERVACIÓN CON LA MISMA SUPERVIVENCIA QUE CIRUGÍA
Bryan Adams
Everything i do, i do it for you
Scorpions
Wind of change
Roxette
Joyride
Michael Jackson
Black or white
Gloria Estefan
Coming out of the dark
Whitney Houston
All the man that i need
U2
The fly

AÑO 2000. El “efecto”

Meta-Analysis of Chemotherapyin Head & Neck Cancer
MACH-NC
AÑO 2000. El “efecto” del Metanálisis

Between 1965 and 1993, 63 trials (10.741 patients) of locoregional treat with
or without chemotherapy in oropharynx, oral cavity, larynx, or hypopharynx
• Adjuvant
• Noadjuvant
• Concomitant
AÑO 2000, Metanálisis Meta-Analysis of Chemotherapy
in Head & Neck Cancer
MACH-NC

Adyuvante
Neoadyuvante
Concomitante
con CDDP
NS
NS
< 0.0001
1 %
2 %
8 %
11%
Total < 0.0001 4 %
p-valor Beneficio Absoluto
a 5 años Nº pacien.
1854
5269
3727
10850
AÑO 2000, Metanálisis Frente a RT sola
Effect of chemotherapy on survival
Meta-Analysis of Chemotherapyin Head & Neck Cancer
MACH-NC

PF Otra QTI
Nº Estudios
15 16
QTI CON CDDP-5FU (PF)
Nº Pacientes
2487 2782
Diferencia
5% 0%
0,01 0,91
HR 0,88 (95% IC0: 79-0,97), p= 0,05
AÑO 2000, Metanálisis Meta-Analysis of Chemotherapy
in Head & Neck Cancer
MACH-NC

Concurrente QTRT RT 70 Gy
Cisplatino 100 mg/m2 Días 1, 22, 43
(n = 171)
RT sola 70 Gy (2.0 Gy/sem. x 5 días /sem. )
por 7 semanas (n =171)
Glotis y Supraglotis resecables (N = 547)
Objetivo principal:
Preservación
de laringe
Inducción PF Cisplatino 100 mg/m2 Día 1
5-FU 1000 mg/m2 PC Días 1-5 2 ciclos cada 3 semanas
(n = 173)
3º ciclo de PF seguido de RT sola
Laringectomia Seguido de RT
RC o RP
EE
Progresión
Exclusión: T1 y T4 (si invasión > 1 cm en base de lengua o invasión del cartílago
Forasterier, 2003
RT sola vs QUIMIORADIOTERAPIA vs INDUCCIÓN-RT
RTOG 91-11
Patients with intact larynx (primary endpoint): 2 years higher in the CCRT group : 88% vs. 75% in IC, p = 0.005 vs 70% in RT alone, p < 0.001 Increased mucosal toxicity No benefit in OS

Mortalidad de la quimioradioterapia
Muertes tempranas relacionadas con tratamiento
Muertes tardías relacionadas con tratamiento
45%
21%
9%
10%9%
6%
Causa de muerte Mediana de tiempo trascurrido
Progresión 1.5 (0.3–8.6)
Comorbilidades 1.9 (0.07–8.8)
Relación tratamiento 0.3 (0.03–3.4)
Segundos primarios 3.5 (1.5–10.1)
desconocidos 5.1 (1.1–9.5)
Argiris A, et al. Clin Cancer Res 2004;10:1956–1962http://clincancerres.aacrjournals.org/content/10/6/1956.long
Toxicidad tardía de la quimioradioterapia
Análisis de 203 pacientes sometidos a QRT de los estudios: RTOG 91-11, 97-03, 99-14
Paci
ente
s %
43%
13%
27%
12%10%
50
Cualquier tipo de toxicidad tardía
Disfunción faríngea
SNG >2 años tras RT
Disfunción laríngea
Muertes
Machtay M et al. JCO 2008
Our sample size of 230 patients makes this
one of the largest studies of late
toxicity in the CCRT era. retrospectivo
Toxicidad aguda de la quimioradioterapia
Acute adverse effects: Grade ≥3
p<0.05
ns
Patients (%)
p<0.01
Wendt TG, et al. J Clin Oncol 1998;16:1318–1324
0 10 20 30 40 50 60
Xerostomia
Nausea/emesis
Leukopenia
Dermatitis
Mucositis
RT alone (n=140)
CRT (n=130)

Morbilidad
Toxicidad aguda y tardía QT-RT
Deglución
Salivación
Fonación: mala función laringea
Estéticos
Resultados pobres: <40% vivos a los 5 años
Metástasis a distancia:
series de autopsias: > 60%
20% clínicas

Nueva proteína … EGFR
2006…..el mundo entero mirándola
Nueva molécula … cetuximab

Bonner J et al. N Engl J Med 2006;354:567–578

ANALISIS DE DATOS
INDIVIDUALES DE
1.772 PACIENTES
Esquema de tratamiento óptimo
……PF vs TPF
Beneficio en SG absoluta de 7,4 % a los 5 años para TaxPF
( 35,0 % frente a 42,4 %). HR: 0,79 ( 95 % [IC ] = 0,70-0,89 , P < 0,001
Esquema de tratamiento óptimo
……PF vs TaxoterePF (AÑOS 2007-2009)
Lancet Oncol. 2011 Feb;12(2):153-9. doi: 10.1016/S1470-2045(10)70279-5. Induction chemotherapy with cisplatin and fluorouracil
alone or in combination with docetaxel in locally advanced squamous-cell cancer of the head and neck: long-term results of the
TAX 324 randomised phase 3 trial. Lorch JH1, Goloubeva O, Haddad RI, Cullen K, Sarlis N, Tishler R, Tan M, Fasciano J, Sammartino
DE, Posner MR; TAX 324 Study Group.
Journal of Clinical Oncology, 2015 ASCO Annual Meeting (May 29 - June 2, 2015). Vol 33, No 15_suppl (May 20 Supplement), 2015
Enfermedad localmente avanzada. Estudios en los años 2010…
• Toxicidad aguda y a largo plazo de la RT
concomitante con cisplatino a altas dosis
• Intensificación con Quimio-Bio-Rt
• Quimioradioterapia vs Bioradioterapia
• Interés de la quimioterapia de inducción
• Integración y secuencia de los tratamientos

• La mediana de seguimiento: 10,8 años • RT sola es inferior a Inducción y RT concomitancia Induction chemotherapy v RT alone: hazard ratio [HR], 0.75; 95% CI, 0.59 to 0.95; P = .02 Concomitant chemotherapy v RT alone: HR, 0.78; 95% CI, 0.78 to 0.98; P = .03
• Inducción y concomitancia eficacia similar (Supervivencia libre de Laringectomia) • Supervivencia global: no diferencias
Muertes NO atribuidas al cáncer de laringe > con QRTR. QTRT: 30,8%. QTI: 20,8%. RT: 16,9%
Forasterier, 2013
RTOG 91-11
QRTR
QTInducción
RT

Intensificación QuimioRadioterapia
Stages III and IV* SCC of: • oropharynx • hypopharynx • larynx (n=720)
R
Accelerated RT Cisplatin 100 x2
Accelerated RT Cisplatin CETUXIMAB
Ongoing RTOG phase III trial (0522)
Ang KK, Zhang Q, Rosenthal DI, et al: Randomized phase III trial of concurrent accelerated
radiation plus cisplatin with or without cetuximab for stage III to IV head and neck carcinoma:
RTOG 0522. J Clin Oncol 32:2940-2950, 2014
Mesia R, Henke M, Fortin A, et al. Chemoradiotherapy with or without panitumumab in
patients with unresected, locally advanced squamous-cell carcinoma of the head and
neck (CONCERT-1): a randomised, controlled, openlabel phase 2 trial. Lancet Oncol
2015;16:208–20. [49]
Martins et al. (LA-CECC: RT+CDDP+-Erlotinib). Martins RG, Parvathaneni U, Bauman JE, et al. Cisplatin and radiotherapy with or without
erlotinib in locally advanced squamous cell carcinoma of the head and neck: a randomized phase II trial. J Clin Oncol 2013;31:1415-21
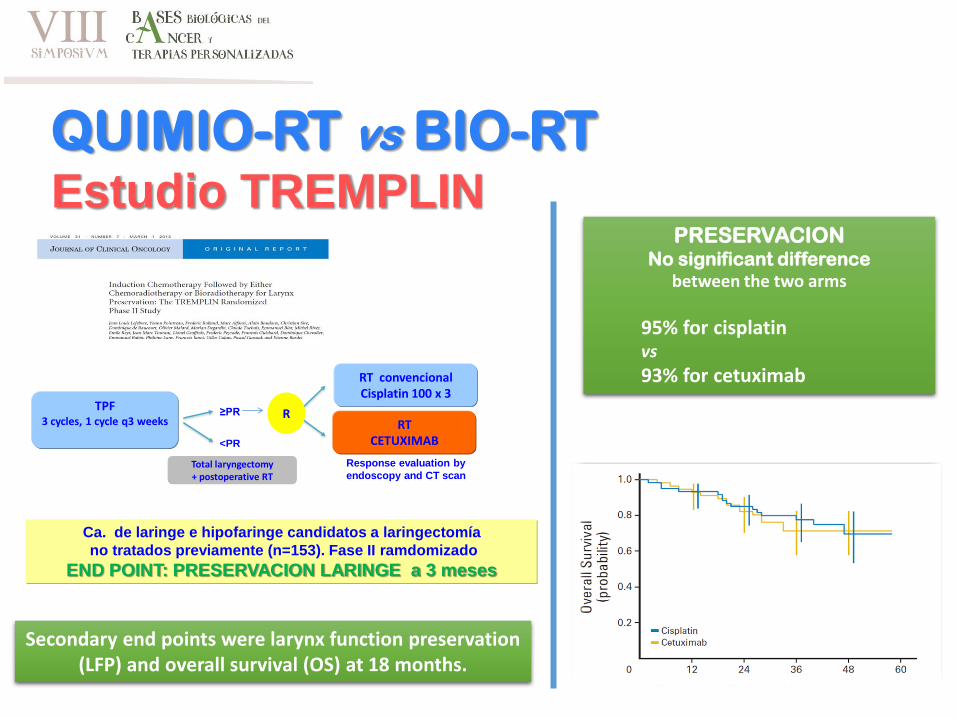
QUIMIO-RT vs BIO-RT Estudio TREMPLIN
Secondary end points were larynx function preservation (LFP) and overall survival (OS) at 18 months.
Total laryngectomy + postoperative RT
Response evaluation by
endoscopy and CT scan
R
<PR
≥PRTPF
3 cycles, 1 cycle q3 weeks
RT convencionalCisplatin 100 x 3
RT CETUXIMAB
Ca. de laringe e hipofaringe candidatos a laringectomía
no tratados previamente (n=153). Fase II ramdomizado
END POINT: PRESERVACION LARINGE a 3 meses
PRESERVACION No significant difference
between the two arms
95% for cisplatin vs
93% for cetuximab

TTCC – 2007.01
Primary end-point: not inferiority of
experimental arm (CTRT Arm B) in front
of standard arm (CRT Arm A) in term of
overall survival. Other objectives were:
Response Rate( RR), loco-regional
control (LRC) ,and toxicity.
530 pts
ECOG 0-1
QUIMIO-RT vs BIO-RT

Papel de la quimioterapia de inducción e
integración y secuencia de los tratamientos
Estadio
III/IV
Localmente
avanzado
RADIOTERAPIA
CONCOMITANTE
CON PLATINO o
BIOLÓGICOS
• Predice respuesta a la RT y selecciona pacientes
• Reduce la necesidad de Cx de rescate tras RT
• Manejo de los síntomas temprano y rápido (trismus, disfagia, dolor)
• Reduce intervenciones (traqueotomía urgente, PEG),
• Mejora el estado nutricional y el PS
• Es un tratamiento precoz de las metástasis a distancia
QT INDUCCIÓN
con TPF
¿ EFECTO SOBRE
la SUPERVIVENCIA?
RADIOTERAPIA
CONCOMITANTE
CON PLATINO o
BIOLÓGICOS

1. TTCC 2503. Annal Oncology, 2014
2. PARADIGM. Lancet Oncology, 2013
3. DeCIDE. J Clin Oncol, 2014
4. NCT01086826. ASCO, 2014. No Publicado
Papel de la quimioterapia de inducción e
integración y secuencia de los tratamientos

DeCIDE: A phase III randomized trial of docetaxel (D), cisplatin (P), 5-fluorouracil
(F) (TPF) induction chemotherapy (IC) in patients with N2/N3 locally advanced squamous cell carcinoma of the head and neck (SCCHN)
Ezra E. W. Cohen, Theodore Karrison, Masha Kocherginsky, Chao H Huang, Mark Agulnik, Bharat Bhushan Mittal, Furhan Yunus, SandeepSamant, Bruce Brockstein, Luis E. Raez, Ranee Mehra, Priya Kumar, Frank G. Ondrey, Tanguy Y. Seiwert, Victoria Meucci Villaflor, Daniel J. Haraf, Everett E. Vokes
N2/N3
TPF x 2 ciclos QTRTRT hiperfracionada +
DFHX
QTRTRT hiperfracionada +
DFHX
5 days of Docetaxel (25 mg/m2), FU (600 mg/m2), hydroxyurea (500mg BID), and RT (150 cGy BID) followed by a 9 day break
D (75 mg/m2), P (75 mg/m2), F (750 mg/m2 day 1-5)
400 pt
280 pt.
2004-2009
CohenEE, Karrison T, KocherginskyMet al. DeCIDE: A phase II randomized trial of docetaxel, cisplatin, 5FU induction chemotherapy in
patients with N2 N3 locally advanced squamous cell cancer of the head and neck. J Clin Oncol 2012;30(suppl 15):5500.
TPF (155 pacientes)Docetaxel 75 mg/m2 Día 1Cisplatino 75 mg/m2 Día 1
5-FU 750 mg/m2 PC, Días 1-5 Cada 3 semanas por 4 ciclos
PF (156 pacientes)Cisplatino 100 mg/m2 Día 1
5-FU 1000 mg/m2 PC, Días 1-5 Cada 3 semanas por 4 ciclos
Localmente avanzadoIrresecable (N = 439) QTRT (128 pacientes)
RT 66-70 GyCisplatino
100 mg/m2 Días 1, 22, 43
Sin Inducción
Cirugía de rescate si enfermedad residual antes o después de
RT
Estudio 2503 Grupo español de TTCC
OP: Tiempo al fracaso terapeutico * (Progresión, recurrencia, muerte, perdida por efectos adversos)
December 2002 and May 2007
The PARADIGM trial: Induction chemotherapy followed by concurrent chemoradiotherapy
(sequential chemoradiotherapy) versus concurrent chemoradiotherapy alone in locally advanced head and neck cancer (PARADIGM): a randomised phase 3 trial
Haddad R, O'Neill A, Rabinowits G, Tishler R, Khuri F, Adkins D, Clark J, Sarlis N, Lorch J, Beitler JJ, Limaye S, Riley S, Posner M.
Estadio III/IV TPF x 3 ciclos
D (75 mg/m2), P (100 mg/m2), F (1000mg/m2 day 1-4)330 pt. ESPERADOS 145 RECLUTADOS08/04-12/08
NR
CR
DOCETAXEL SEMANAL x4RT ACELERADA BOOST (1-5)
6 SEMANAS A1
CARBOPLATINO SEMANAL
RT (1-5) x7 SEMANAS. A2
CISPATINO SEMANA (1,4)RT ACELERADA BOOST (1-5)
6 SEMANAS. B
A
Lancet Oncol. 2013 Mar;14(3):257-64

Estudio TTCC 2503 Pacientes con mucha carga tumoral y bajo PS 3 brazos Alta toxicidad. Δ mortalidad precoz no relacionada con CCC
DeCIDE y Paradigm Esquemas de tratamiento no habitual RT y concomtancia Disminuyen metástasis Sin poder estadístico por bajo reclutamiento y cierre precoz SG en el brazo de control más alta de la esperada (78% vs 55% en el momento de diseño del estudio)
Papel de la quimioterapia de inducción e
integración y secuencia de los tratamientos
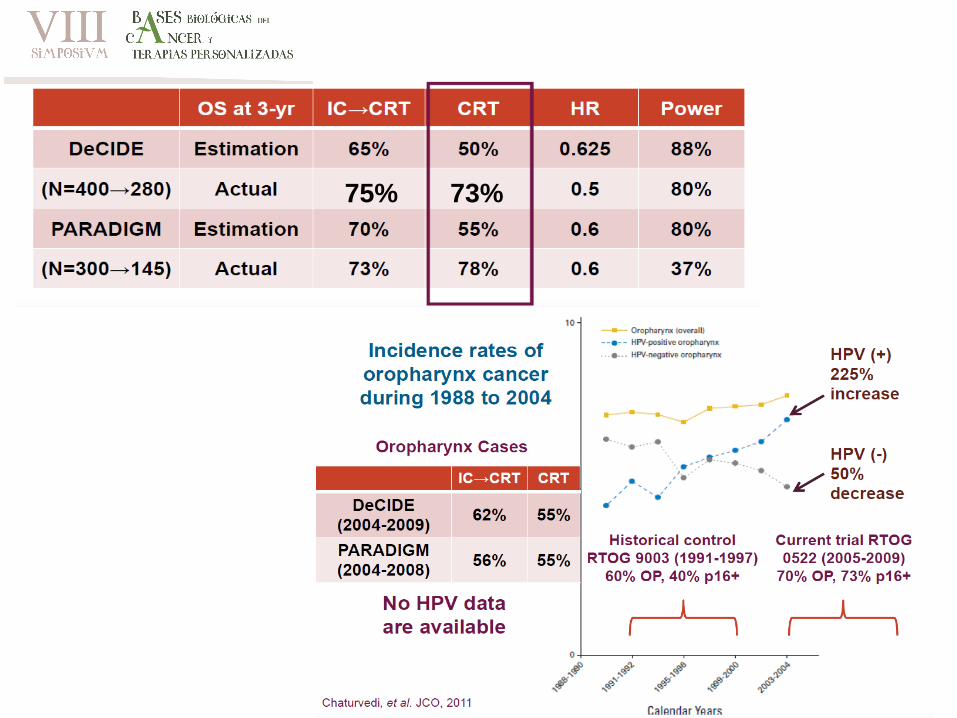
75% 73%

50-60%
50-60%
20-30%
H. Salamanca, 2008-2013: 24%, 87% ASOCIADOS A FUMADORES

HPV-Positive HNSCC
HPV-Negative HNSCC
Anatomic site[7-9]
Oropharynx (tonsil/base of
tongue, soft palate)
All sites/upper aerodigestive tract
Histology[10] Basaloid Keratinized
Age[9,11] Younger Older
Sex[12] 3:1 men (unclear why) 3:1 men (due to tobacco use)
Socioeconomic status
Tends to be high Tends to be low
Risk factors[9,11,13]
Sexual behavior Tobacco/alcohol
Incidence[11,12] Rising rapidly Declining
Survival[9,13] Improved Worse
2nd cancers[11] Uncommon Common (including lung cancer)
Comorbilidad
es
no si
7. Smith EM, et al. J Natl Cancer Inst. 2004;96:449-455. 8. Herrero R. J Natl Cancer Inst Monogr. 2003;31:47-51.
9. Fakhry C, et al. J Clin Oncol. 2006;24:2606-2611. 10. Poetsch M, et al. Head Neck. 2003;25:904-910.11. Chaturvedi AK, et al. J Clin
Oncol. 2008;26:612-619. 12. Cole L, et al. PLoS One. 2012;7:e32657. 13. Ritchie JM, et al. Int J Cancer. 2003;104:336-344. 14. Gillison
ML, et al. J Natl Cancer Inst. 2008;100:407-420. 17. D’Souza G, et al. J Acquir Immune Defic Syndr. 2013. [ePub ahead of print] 19.
D’Souza G, et al. N Engl J Med. 2007;356:1944-1956.
HPV +: Diferencias biológicas, clínicas y pronósticas
Treatment deintensification for HPV-asscociatedOropharyngeal Cancer
Cmelak A et al. 49th ASCO Meeting 2014
Best outcome for < T4, T1-N2b, < 10 Pack/years

TPF x 3
Localmente avanzado
irresecable (N =420)
QT-RT (PF x2)
RT- cetuximab
TPF x3
QT-RT (PF x2)
RT- cetuximab
C. Oral OroF. HipoF. No laringe
1, SG a 3 años entre Inducción vs No inducción
2, Toxicidad grado 3-4 entre QTRT vs RT-cetX
Cetuximab/RT versus concomitant CT/RT with or without induction TPF in locally
advanced H&N squamous cell carcinoma. Toxicidad y eficacia (NCT01086826)

In contrast to the TTCC 2503, DeCIDE and the PARADIGM studies, this study found a meaningful and
significant benefit in
PFS (29.7 vs. 18.5 m HR 0.73, p = 0.0155)
OS (53.7 vs. 30.3 m, HR 0.72, p = 0.025)
Cetuximab/RT versus concomitant CT/RT with or without induction TPF in locally
advanced H&N squamous cell carcinoma. Toxicidad y eficacia (NCT01086826)
SG a 3 años entre Inducción vs No inducción

Cetuximab/RT versus concomitant CT/RT with or without induction TPF in locally
advanced H&N squamous cell carcinoma. Toxicidad y eficacia (NCT01086826)
SG a 3 años entre Inducción vs No inducción
• Tipo de pacientes parecido al estudio español
• Menos pérdidas y menos toxicidad que el Español
• Número escaso de pacientes para 4 brazos
• Factor de confusión brazos con Cetuximab + RT
• Efecto diferente en función a la localizacion (negativo en orofaringe)
No cambia la práctica clínica habitual
No cambia el estándar
In contrast to the TTCC 2503, DeCIDE and the PARADIGM studies, this study found a meaningful and
significant benefit in
PFS (29.7 vs. 18.5 m HR 0.73, p = 0.0155)
OS (53.7 vs. 30.3 m, HR 0.72, p = 0.025)

• Desintensificación del tratamiento en HPV +
• Nuevas terapias: inmunoterapia
• Integrar los conocimiento de la biología molecular
Surgery
1846
Radiation Therapy
1901
Chemotherapy
1960
Targeted Therapy
2006
Immuno-Oncology
2016….
Selección molecular
2015
HPV
2010
Avances y
Retos Pendientes
El objetivo:
1. Mejorar el tratamiento de pacientes de mal
pronóstico
2. Largos supervivientes, con PFS > 85%, con
mínima toxicidad
…The emphasis on toxicity as well as efficacy is prescient,
because it is estimated that by 2030 there will be more than
20,000 head and neck cancer survivors each year in the United
States alone …
Rosenthal DI, Harari PM, Giralt J, et al: Impact of p16 status on the results of the phase III cetuximab (cet)/radiotherapy (RT). J Clin Oncol 32, 2014
(suppl; abstr 6001)
Zain A. Husain, VOLUME 34 • NUMBER 5 • FEBRUARY 10, 2016. Cisplatin Versus Cetuximab With Radiotherapy in Locally Advanced Squamous Cell
Carcinoma of the Head and Neck
Avances y
Retos Pendientes

Trial Inclusion criteria Treatment Outcomes
Cmelak et al, phase 2 Stage III, IVA/B, HPV-16 ISHþ
/p16þ OPSCC
IC with 3 cycles of cisplatin/paclitaxel/cetuximab.
Complete clinical responders received 54
Gy with weekly cetuximab
2-y PFS
2 year OS
RTOG 1016, phase 3
(clinicaltrials.gov Identifier:
NCT01302834)
Stage III, IVA/B, p16þ OPSCC Cisplatin 100 mg/m2 on days 1 and 22 with
70 Gy accelerated IMRT (6 wk) vs
weekly cetuximab with 70 Gy
accelerated IMRT (6 wk)
2-Year PFS
2-Year OS
ECOG 3311, phase 2
(clinicaltrials.gov Identifier:
NCT01898494)
Stage III, IVA/B, p16þ OPSCC Initial TORS with neck dissection and risk
stratification determines adjuvant treatment.
Low risk: Observation
Intermediate risk: randomized to RT alone, 50 Gy vs 60 Gy
High risk: Weekly cisplatin/66 Gy RT
2-Year PFS
2-Year OS
Quarterback Trial, phase 3
(clinicaltrials.gov Identifier:
NCT01706939)
Stage III, IVA/B, p16þ OPSCC,
unknown primary tumor,
nasopharynx
IC with 3 cycles of TPF and responders
(CR or PR) randomized 2:1 to RT 56
Gy with weekly carboplatin vs RT 70 Gy with carboplatin
3-Year PFS
3-Year LRC
5-Year OS
ADEPT, phase 3 adjuvant
trial (clinicaltrials.gov
Identifier: NCT01687413)
p16þ OPSCC with
postoperative pathological
T1-4aNþ with ECS
IMRT 60 Gy vs IMRT 60 Gy with weekly cisplatin
2-Year DFS
2-Year LRC
5-Year DM rate
TROG 12.01, phase 3
(clinicaltrials.gov Identifier:
NCT01855451)
Stage III, IVA/B, p16þ OPSCC,
(excluding T1-2N1 and T4N3, >10
py smokers with N2b or N2c)
RT 70 Gy with weekly cetuximab vs RT 70
Gy with weekly 40 mg/m2 cisplatin Compare treatment
adverse effects using
MDASI-HN
De-ESCALaTE, phase 3
(clinicaltrials.gov Identifier:
NCT01874171)
Stage III, IVA/B, p16þ OPSCC
(T3N0-T4N0, T1N1- T4N3)
RT 70 Gy with weekly cetuximab vs RT 70
Gy with cisplatin 100 mg/m2 on days 1,
22, and 43
Compare treatment
adverse
effects
De-escalation Trials in HPV-Positive OPSCC
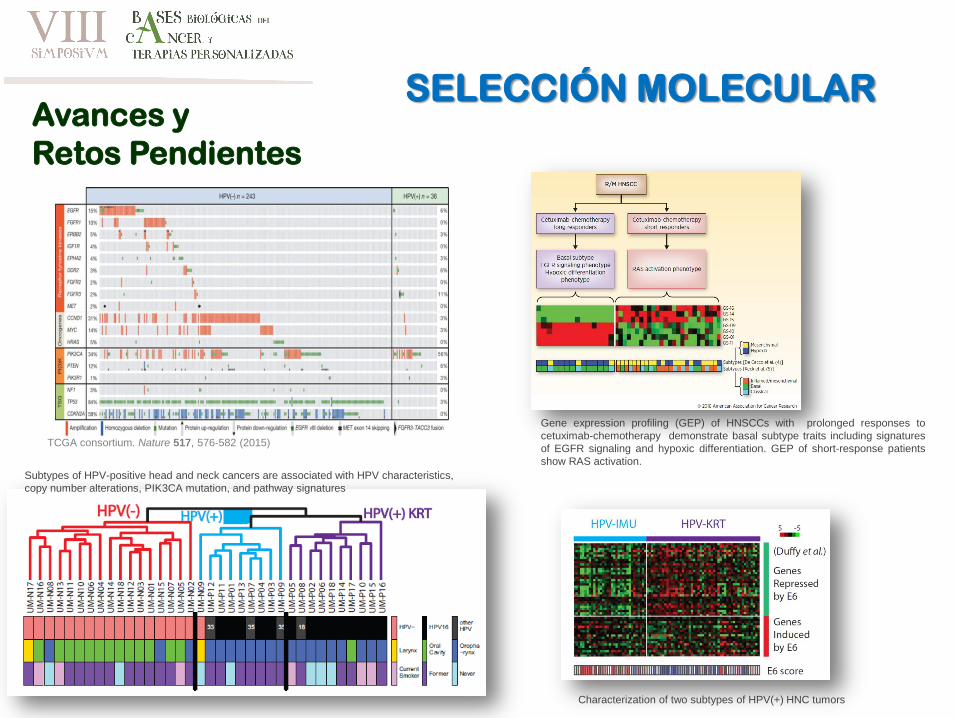
TCGA consortium. Nature 517, 576-582 (2015)
Gene expression profiling (GEP) of HNSCCs with prolonged responses to
cetuximab-chemotherapy demonstrate basal subtype traits including signatures
of EGFR signaling and hypoxic differentiation. GEP of short-response patients
show RAS activation.
Subtypes of HPV-positive head and neck cancers are associated with HPV characteristics,
copy number alterations, PIK3CA mutation, and pathway signatures
Characterization of two subtypes of HPV(+) HNC tumors
SELECCIÓN MOLECULAR Avances y
Retos Pendientes

Avances y
Retos Pendientes
Inmunoterapia
