3281 hyponatremia practicetool
TRANSCRIPT
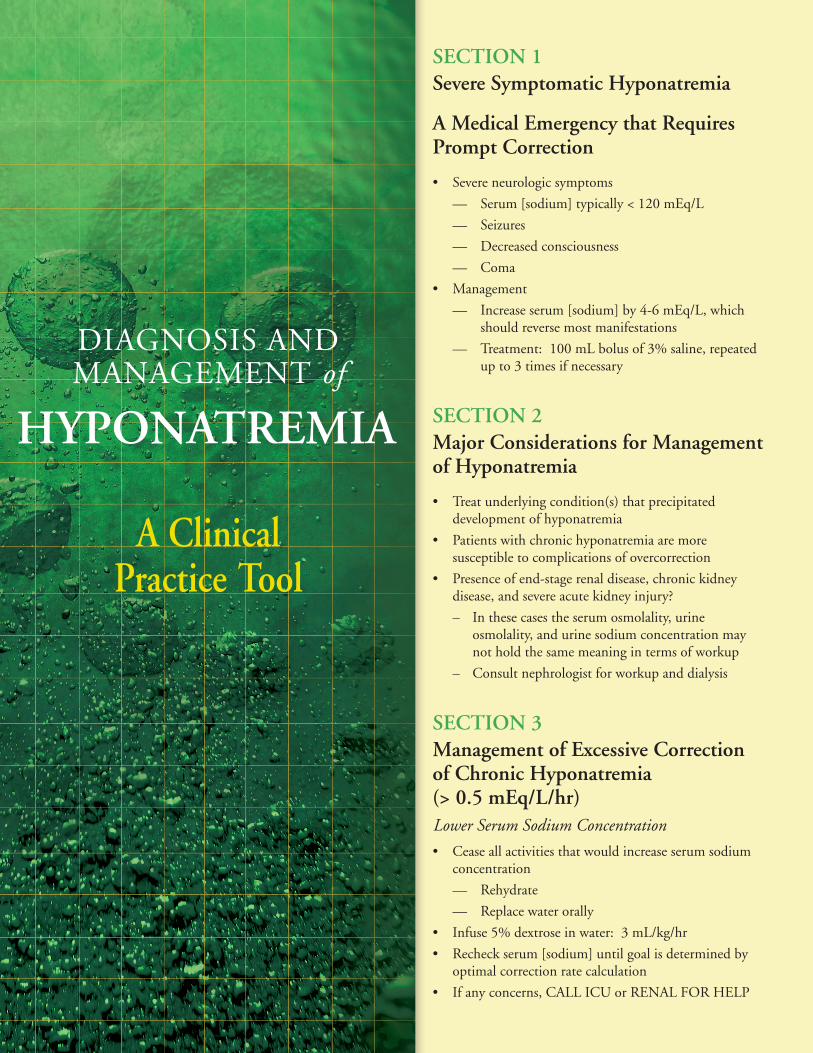
DIAGNOSIS AND MANAGEMENT of
A clinical Practice tool
HYPonAtReMiA
Section 1Severe Symptomatic Hyponatremia
A Medical emergency that Requires Prompt correction
• Severe neurologic symptoms
— Serum [sodium] typically < 120 mEq/L
— Seizures
— Decreased consciousness
— Coma
• Management
— Increase serum [sodium] by 4-6 mEq/L, which should reverse most manifestations
— Treatment: 100 mL bolus of 3% saline, repeated up to 3 times if necessary
Section 2Major considerations for Management of Hyponatremia
• Treat underlying condition(s) that precipitated development of hyponatremia
• Patients with chronic hyponatremia are more susceptible to complications of overcorrection
• Presence of end-stage renal disease, chronic kidney disease, and severe acute kidney injury?
– In these cases the serum osmolality, urine osmolality, and urine sodium concentration may not hold the same meaning in terms of workup
– Consult nephrologist for workup and dialysis
Section 3Management of excessive correction of chronic Hyponatremia (> 0.5 meq/L/hr)Lower Serum Sodium Concentration
• Cease all activities that would increase serum sodium concentration
— Rehydrate
— Replace water orally
• Infuse 5% dextrose in water: 3 mL/kg/hr
• Recheck serum [sodium] until goal is determined by optimal correction rate calculation
• If any concerns, CALL ICU or RENAL FOR HELP
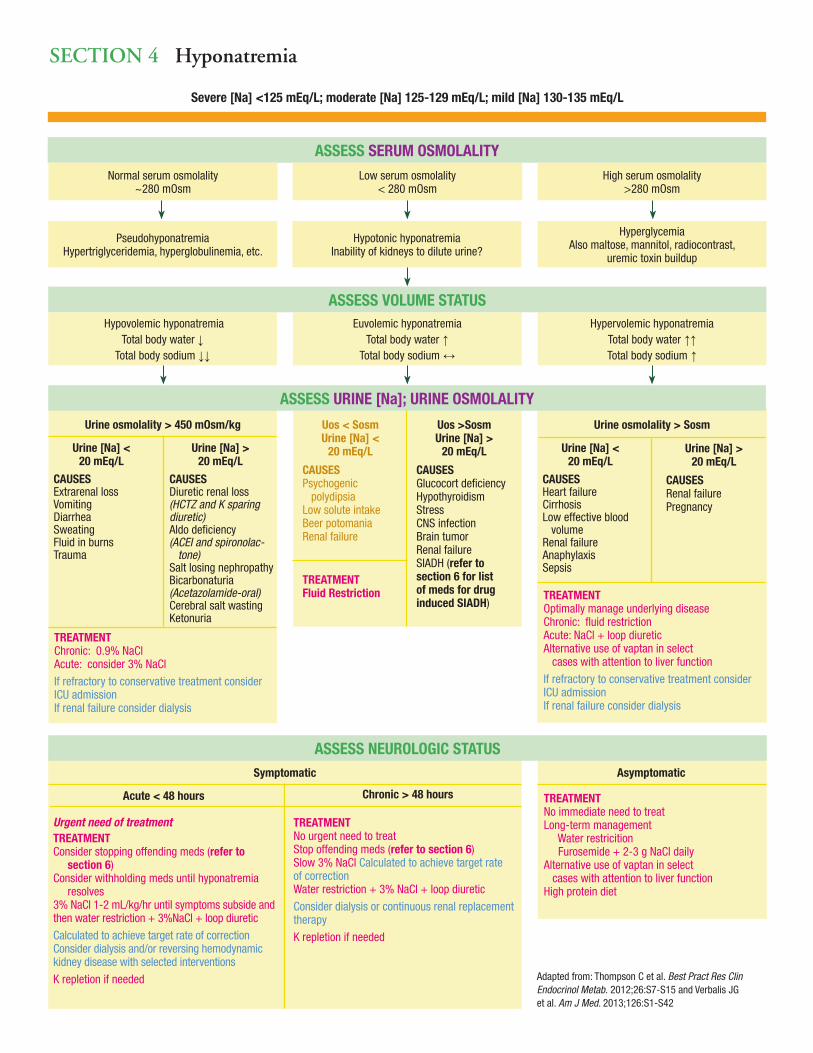
Section 4 Hyponatremia
Severe [Na] <125 mEq/L; moderate [Na] 125-129 mEq/L; mild [Na] 130-135 mEq/L
ASSESS SERUM OSMOLALITYNormal serum osmolality
~280 mOsmLow serum osmolality
< 280 mOsmHigh serum osmolality
>280 mOsm
PseudohyponatremiaHypertriglyceridemia, hyperglobulinemia, etc.
Hypotonic hyponatremiaInability of kidneys to dilute urine?
HyperglycemiaAlso maltose, mannitol, radiocontrast,
uremic toxin buildup
Hypovolemic hyponatremiaTotal body water ↓
Total body sodium ↓↓
Euvolemic hyponatremiaTotal body water ↑
Total body sodium ↔
Hypervolemic hyponatremiaTotal body water ↑↑Total body sodium ↑
Urine osmolality > 450 mOsm/kg
Urine [Na] < 20 mEq/L
CAUSESExtrarenal lossVomitingDiarrheaSweatingFluid in burns Trauma
Urine [Na] > 20 mEq/L
CAUSESDiuretic renal loss(HCTZ and K sparing diuretic)Aldo deficiency(ACEI and spironolac- tone)Salt losing nephropathyBicarbonaturia(Acetazolamide-oral)Cerebral salt wastingKetonuria
Uos >SosmUrine [Na] >
20 mEq/L
CAUSESGlucocort deficiencyHypothyroidismStressCNS infectionBrain tumorRenal failureSIADH (refer to section 6 for list of meds for drug induced SIADH)
Uos < SosmUrine [Na] <
20 mEq/L
CAUSESPsychogenic polydipsiaLow solute intakeBeer potomaniaRenal failure
Urine osmolality > Sosm
Urine [Na] < 20 mEq/L
CAUSESHeart failureCirrhosisLow effective blood volumeRenal failureAnaphylaxis Sepsis
Urine [Na] > 20 mEq/L
CAUSESRenal failurePregnancy
TREATMENTOptimally manage underlying diseaseChronic: fluid restrictionAcute: NaCl + loop diureticAlternative use of vaptan in select cases with attention to liver function
If refractory to conservative treatment consider ICU admissionIf renal failure consider dialysis
Symptomatic
Acute < 48 hours Chronic > 48 hours
Urgent need of treatmentTREATMENTConsider stopping offending meds (refer to section 6)Consider withholding meds until hyponatremia resolves3% NaCl 1-2 mL/kg/hr until symptoms subside and then water restriction + 3%NaCl + loop diuretic
Calculated to achieve target rate of correction Consider dialysis and/or reversing hemodynamic kidney disease with selected interventions
K repletion if needed
TREATMENTNo urgent need to treatStop offending meds (refer to section 6)Slow 3% NaCl Calculated to achieve target rate of correctionWater restriction + 3% NaCl + loop diuretic
Consider dialysis or continuous renal replacement therapy
K repletion if needed
Asymptomatic
TREATMENTNo immediate need to treatLong-term management Water restricition Furosemide + 2-3 g NaCl dailyAlternative use of vaptan in select cases with attention to liver function High protein diet
ASSESS VOLUME STATUS
ASSESS URINE [Na]; URINE OSMOLALITY
ASSESS NEUROLOGIC STATUS
Adapted from: Thompson C et al. Best Pract Res Clin Endocrinol Metab. 2012;26:S7-S15 and Verbalis JG et al. Am J Med. 2013;126:S1-S42
TREATMENTChronic: 0.9% NaClAcute: consider 3% NaCl
If refractory to conservative treatment consider ICU admissionIf renal failure consider dialysis
TREATMENT Fluid Restriction
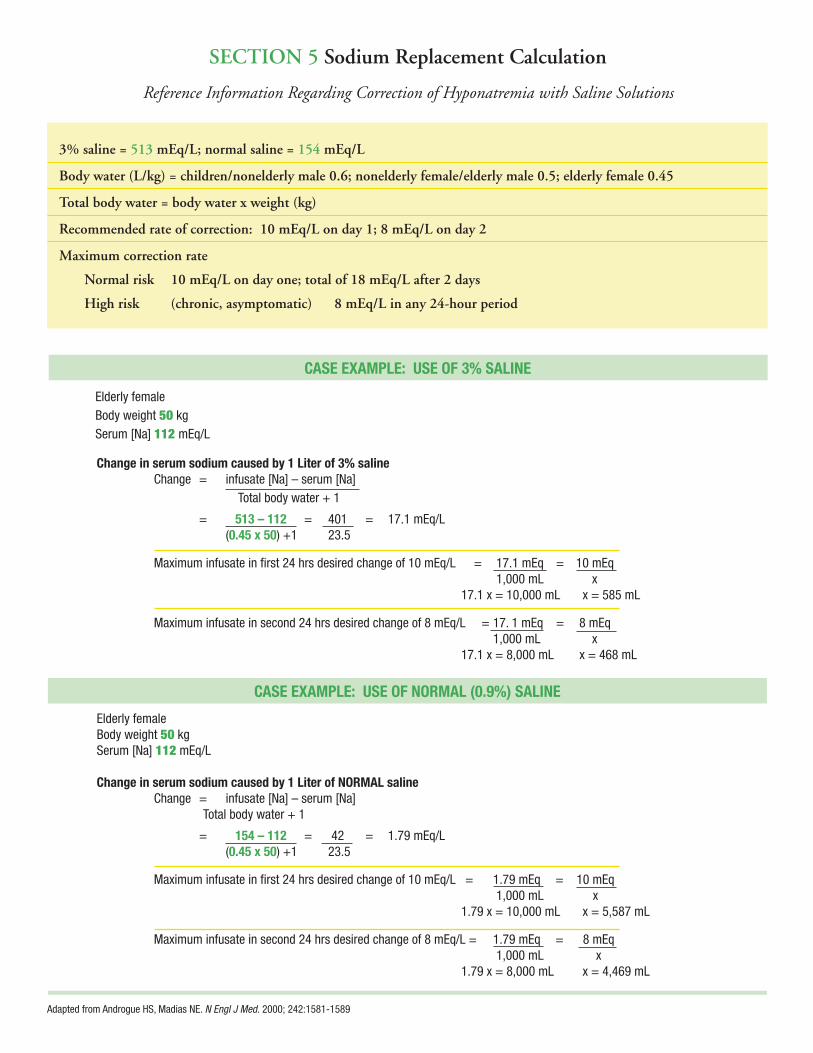
Section 5 Sodium Replacement calculation
Reference Information Regarding Correction of Hyponatremia with Saline Solutions
3% saline = 513 meq/L; normal saline = 154 meq/L
Body water (L/kg) = children/nonelderly male 0.6; nonelderly female/elderly male 0.5; elderly female 0.45
total body water = body water x weight (kg)
Recommended rate of correction: 10 meq/L on day 1; 8 meq/L on day 2
Maximum correction rate
normal risk 10 meq/L on day one; total of 18 meq/L after 2 days
High risk (chronic, asymptomatic) 8 meq/L in any 24-hour period
CASE EXAMPLE: USE OF 3% SALINE
Elderly female Body weight 50 kg Serum [Na] 112 mEq/L
Change in serum sodium caused by 1 Liter of 3% saline Change = infusate [Na] – serum [Na] Total body water + 1
= 513 – 112 = 401 = 17.1 mEq/L (0.45 x 50) +1 23.5
Maximum infusate in first 24 hrs desired change of 10 mEq/L = 17.1 mEq = 10 mEq 1,000 mL x 17.1 x = 10,000 mL x = 585 mL
Maximum infusate in second 24 hrs desired change of 8 mEq/L = 17. 1 mEq = 8 mEq 1,000 mL x 17.1 x = 8,000 mL x = 468 mL
Elderly female Body weight 50 kg Serum [Na] 112 mEq/L
Change in serum sodium caused by 1 Liter of NORMAL saline Change = infusate [Na] – serum [Na] Total body water + 1
= 154 – 112 = 42 = 1.79 mEq/L (0.45 x 50) +1 23.5
Maximum infusate in first 24 hrs desired change of 10 mEq/L = 1.79 mEq = 10 mEq 1,000 mL x 1.79 x = 10,000 mL x = 5,587 mL
Maximum infusate in second 24 hrs desired change of 8 mEq/L = 1.79 mEq = 8 mEq 1,000 mL x 1.79 x = 8,000 mL x = 4,469 mL
CASE EXAMPLE: USE OF NORMAL (0.9%) SALINE
Adapted from Androgue HS, Madias NE. N Engl J Med. 2000; 242:1581-1589

Diuretics• Indapamide• Thiazides• Furosemide • Aldosterone inhibitors
AVP Analogues• Desmopressin• Oxytocin
Antiepileptics• Carbamazepine• Oxcarbazepine• Sodium valproate• Lamotrigine• Levetiracetam
Antidepressants• Selective serotonin uptake inhibitors• Monoamine oxidase inhibitors• Tricyclics
Antipsychotics• Carbamazepine• Clozapine • Thioridazine• Trifl uoperazine• Haloperidol
Antiarrhythmic drugs• Amiodarone• Lorcainide • Propafenone
Anti-infectives• Azithromycin• Lopinavir• Miconazole• Rifabutin
Antiparkinson agents• Amantadine• Levodopa• Pramipexole• Trihexyphenidyl
Antineoplastics• Vinca alkaloids – Carboplatin – Cisplatin • Alkylating agents – Cyclophosphamide – Melphalan – Methotrexate – Ifosfamide
ACE inhibitors• Enalapril• Captopril
Pain medications• Opiates• Tramadol• COX-2 inhibitors• NSAIDS
Proton pump inhibitors• Omeprazole• Pantoprazole
Hypnotics• Temazepam
Hypoglycemic agents• Sulfonylureas
Street drugs• MDMA (ecstasy)• Nicotine
Section 6 Drugs that induce SiADH
Adapted from Liamis G et al. Am J Kidney Dis. 2008;52:144-153
This activity is supported by an educational grant from Otsuka America Pharmaceutical, Inc.
This tool guide is meant to be used in conjunction with proper supervision from appropriate clinical services.
The opinions expressed herein are those of the authors and do not necessarily represent the views of Albert Einstein College of Medicine, Montefi ore Medical Center, Rockpointe or Otsuka, USA. Please review complete prescribing information of specifi c drugs or combination of drugs, including indications, contraindications, warnings, and adverse effects before administering pharmacologic therapy to patients.
This reference tool is a companion to “HYPONATREMIA: Detection and Management in the Hospital Setting” a CME-certifi ed program jointly provided by Albert Einstein College of Medicine of Yeshiva University and Montefi ore Medical Center’s Center for Continuing Medical Education and Rockpointe.
© 2014 Rockpointe