4 ธันวาคม พ.ศ. 2551 - · pdf...
TRANSCRIPT

CPC 4 ธนัวาคม พ.ศ. 2551
อายรุแพทย์ รศ.พญ. นิจศรี ชาญณรงค์ผูป่้วยชายไทยคู ่ อาย ุ 45 ปี อาชพีขายน ้าเตา้หู-้ปาทอ่งโก๋ภมูลิ าเนาและทีอ่ยูปั่จจบุนั ต.หว้ยตามอญ อ.ภสูงิห ์ จ.อตุรดถิต์1st admission ประวตัไิดจ้ากผูป่้วย และเวชระเบยีน เชือ่ถอืได ้CC: ขาสองขา้งออ่นแรง 1 เดอืน PTAPI: 5 เดอืน PTA รูส้กึหนา ๆ บวมๆ บรเิวณตัง้แตข่อ้เทา้ถงึปลายนิว้เทา้
ขวา บางครัง้รูส้กึเหมอืนมอีะไรมาแทงฝ่าเทา้เวลาเหยยีบพืน้ ไมม่อีาการแขนขาออ่นแรง ขบัถา่ยปกต ิ ไปรับการรักษาทีค่ลนิกิใกลบ้า้น แพทย์วนิจิฉัยวา่เป็นเกา๊ต ์ใหย้าขบัปัสสาวะ และ allopurinol มารับประทาน อาการไมด่ขี ึน้ ความรูส้กึหนา ๆ และเจ็บทีบ่รเิวณฝ่าเทา้เป็นเทา่ ๆ เดมิ มีคนทักวา่ผวิสคีล ้าขึน้ สงัเกตวา่เป็นมากบรเิวณทีถ่กูแสงแดด3 ½ เดอืน PTA เริม่รูส้กึใสร่องเทา้แลว้เทา้ขวาหลดุงา่ย อาการหนาๆ บวม ๆ ยงัคงอยูเ่ทา่ ๆ เดมิ ปัสสาวะอจุจาระปกตดิี2 ½ เดอืน PTA เริม่มอีาการปลายนิว้เทา้ซา้ยมชีา ฝ่าเทา้ทัง้สองขา้งเหมอืนมอีะไรมาแทงเวลาเหยยีบพืน้ 1 เดอืน PTA เทา้ซา้ยใสร่องเทา้แลว้หลดุ เดนิลากเทา้ไมไ่ด ้ ตอ้งยกเทา้ขึน้สงู ขา้งขวาเป็นมากกวา่ขา้งซา้ย ชามากบรเิวณปลายนิว้เทา้ทัง้สองขา้ง ไมม่แีขนออ่นแรง ปัสสาวะอจุจาระปกตดิ ี

5 mo. Sensory3.5 mo. Motor
2.5 mo. Sensory1 mo. Motor

น ้าหนักลดลง (80 73 กก.) ในชว่ง 5 เดอืน มีคนทักวา่ผวิคล ้าขึน้ ไมป่วดหลัง ไมม่ไีข ้ ขบัถา่ยปกต ิ ไมม่อีบุัตเิหตกุระทบกระเทอืนทีห่ลัง
PH: ความดนัโลหติสงู เคยกนิยาแลว้ความดันปกต ิ แพทยใ์หห้ยดุยา
Hyperuricemia 1-2 yr. ได ้ Allopurinol (300) 1x1
ปฏเิสธใชย้าชดุ ยาหมอ้ ยาลกูกลอน
ปฏเิสธแพย้า
ปฏเิสธดืม่สรุา,สบูบหุรี่
ปฏเิสธอาการผืน่แพแ้สง แผลในปาก ปวดขอ้
FH: ปฏเิสธประวัตโิรคทางระบบประสาทในครอบครัว

Physical Examination:Vital signs: BT 37 º C , PR 100 /min, BP 159/95 mmHg,
RR 20 /minGA: A Thai middle aged male, good consciousnessSkin and appendages: No rash, hyperpigmented skin at
sun-exposure areas (as pictures)
HEENT: Not pale conjunctivae , no icteric sclerae, no cervical and axillary lymphadenopathy.
Pulmonary system: Equal breath sound, no adventitious sound
CVS: Regular rhythm, normal S1S2, no murmur, PMI at 5th ICS MCL
Abdomen: Normal contour; soft, not tender; normoactive bowel sound; liver 1 cm. below RCM with span 12 cm., blunt edge, rubbery consistency; spleen just palpated
Extremities: Mild pitting edema at dorsum of feet



Neurological Examination:
Good consciousness, cooperative
Cranial nerve: Pupils 3 mm. with reaction to light; no exudates or hemorrhages; other CNs were normal
Motor Upper extremities No fasciculation, no atrophy Tone: Normal
Power: grade V all Reflex: 2+ all
Lower extremitiesNo fasciculation, no atrophy Tone: mild hypotoniaPower:
EHL, Tibialis anterior (Rt./Lt.): I/II
Finger flexors (Rt./Lt): I/II
Ankle extensor (Rt./Lt.): I/III
Ankle flexor (Rt./Lt.): I/II
Ankle inversion (Rt./Lt.): II/III
Ankle eversion (Rt./Lt.): II/III
Reflex: 0+ all
Babinski’s sign: Plantar responseClonus: Negative

SensoryUpper extremities
Pinprick sensation: Normal
Proprioception: Normal
Lower extremities
Pinprick sensation: Decreased all toes
Proprioception: Loss of joint position sensation of both feet;
Romberg: positive
Hyperesthesia of both plantar sides
ANSAnal sphincter tone: Normal
Anal reflex: Normal
CerebellumFTN: normal, no dysdiadocokynesia, no trunkal ataxia
Tandem gait: can’t be evaluated
No meningeal sign

2+2+
2+
2+
2+
2+
00
00
Motor : weaknesshypotoniaPinprick
Proprioception / Hyperesthesia

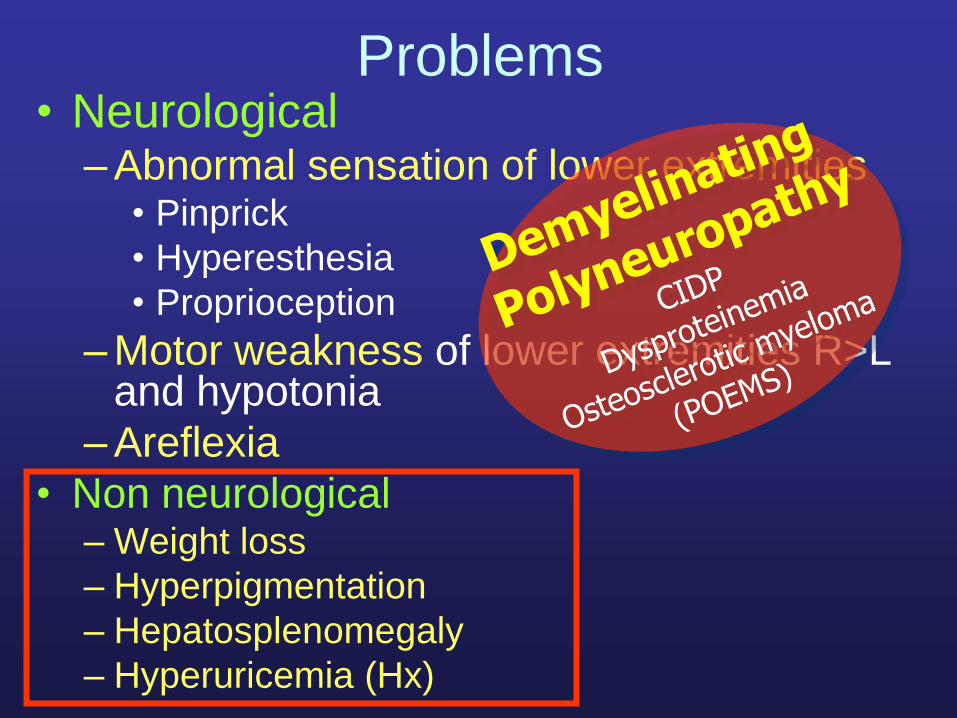
Problems• Neurological
– Abnormal sensation of lower extremities• Pinprick
• Hyperesthesia
• Proprioception
– Motor weakness of lower extremities R>L and hypotonia
– Areflexia
• Non neurological– Weight loss
– Hyperpigmentation
– Hepatosplenomegaly
– Hyperuricemia (Hx)

The Nervous system• CNS
– Brain
– Spinal cord
• PNS
– Nerve
• Nerve root (Cauda equina)
• LS Plexus
• Peripheral nerve
– Mononeuropathy
– Multiple mononeuropathy
– Polyneuropathy
– NMJ, Muscle
ANS spared
Non root distribution
Discrepancy of motor,
sensory
Infiltrative ?Immune ?
Asymmetry

Hx and PE
Multifocal neuropathy
Mononeuropathy
Peripheral neuropathy
EMG
Axonal
Demyelination
Approach to Peripheral Nerve Disease


Axonopathy Demyelination
Motor Distal Proxima/ Distal
Sensory (pinprick)
Distal, Gloves and stockings
Not well demarcated
Proprioception Intact Impaired
Reflexes Decreased distal
Decreased generalized
Autonomic May involve Rarely
Length dependent
Axonopathy VS Demyelination


Impression:
Bilateral sural sensory, bilateral tibial, peroneal motor responses were absent.
Right median, ulnar motor responses showed prolonged distal latencies; slow
conduction velocities; prolonged F wave latencies.
The above studies are consistent with severe demyelinating polyneuropathies; lower extremities more affected than upper.

Hx and PE
Multifocal neuropathy
Mononeuropathy
Peripheral neuropathy
EMG
Axonal
Demyelination
Approach to Peripheral Nerve Disease
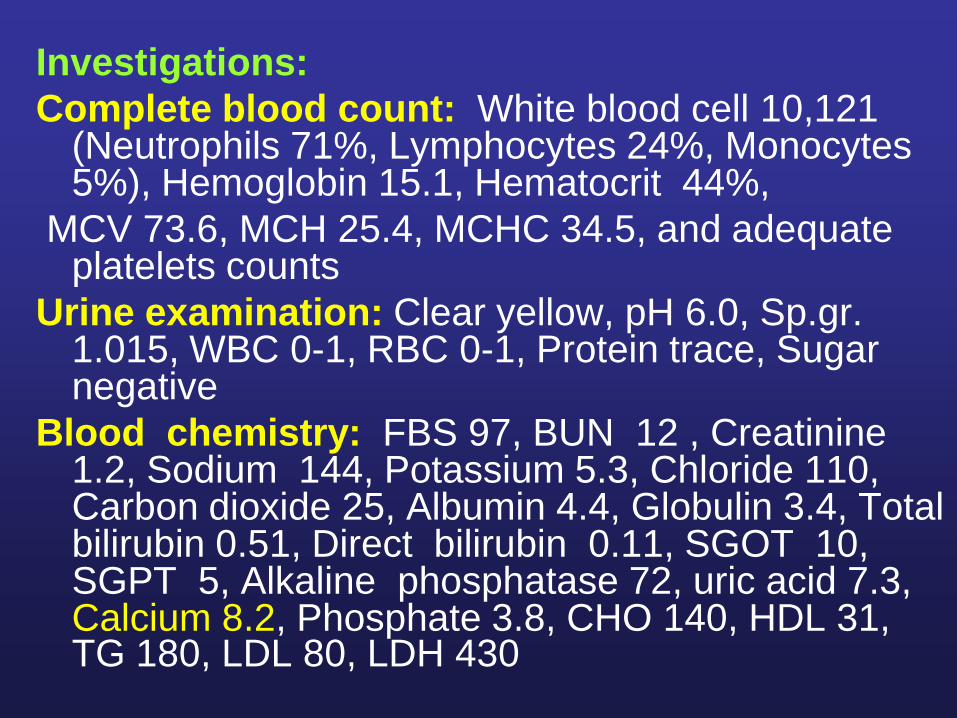
Investigations:
Complete blood count: White blood cell 10,121 (Neutrophils 71%, Lymphocytes 24%, Monocytes 5%), Hemoglobin 15.1, Hematocrit 44%,
MCV 73.6, MCH 25.4, MCHC 34.5, and adequate platelets counts
Urine examination: Clear yellow, pH 6.0, Sp.gr. 1.015, WBC 0-1, RBC 0-1, Protein trace, Sugar negative
Blood chemistry: FBS 97, BUN 12 , Creatinine 1.2, Sodium 144, Potassium 5.3, Chloride 110, Carbon dioxide 25, Albumin 4.4, Globulin 3.4, Total bilirubin 0.51, Direct bilirubin 0.11, SGOT 10, SGPT 5, Alkaline phosphatase 72, uric acid 7.3, Calcium 8.2, Phosphate 3.8, CHO 140, HDL 31, TG 180, LDL 80, LDH 430

Thyroid function test:
FT3 3.48 pg/ml (2.39-6.79)
FT4 0.90 mg/dl (0.58-1.64)
TSH 4.36 uIU/ml. (0.34-5.6)
CEA (Carcinoembreonic Antigen): 0.57 ng/ml (<4)
Vitamin B12 level: 300 pg/mL (243-894)
Anti-HIV: Negative
ESR: 11 mm/hr. (<20)
Serum VDRL: Non-reactive
HBsAg: Negative
Anti-HBc : Positive
Anti-HBs: Positive (55.9 mIU/mL)
Anti-HCV: NegativeANA: Negative
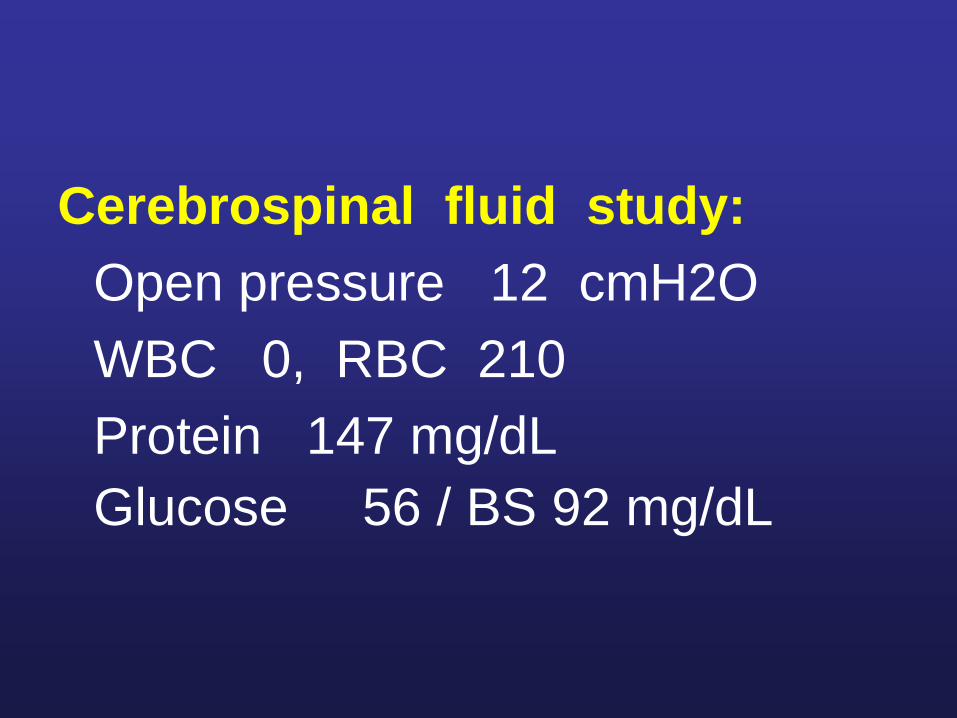
Cerebrospinal fluid study:
Open pressure 12 cmH2O
WBC 0, RBC 210
Protein 147 mg/dL
Glucose 56 / BS 92 mg/dL

CIDP
Lewis -Sumner
CIDP in systemic diseases
CIDP-DM
Sensory variant
SIDP
CIDP with CNS demyelination
CIDP-MGUS
MMN
DADS IgM/antiMAG
POEMS
CANOMAD(Chronic inflammatory
demyelinating polyneurpathy)

Typical CIDP
Motor : symmetrical proximal and distal limb weaknessSensory : symmetrical loss of proprioceptionand distal loss pinprick sensation
Autonomic : spared
Chronic progressive > 8 weeks or relapsing remitting
Clinical presentation

Typical CIDP
Investigations
High CSF protein in 80-95%
Electrodiagnosis demyelinating polyneuropathy
Nerve biopsy is rarely needed
R/O CIDP mimics
Treatments
good response to immunomodulating therapies
Problems• Neurological
– Abnormal sensation of lower extremities• Pinprick
• Hyperesthesia
• Proprioception
– Motor weakness of lower extremities R>L and hypotonia
– Areflexia
• Non neurological– Weight loss
– Hyperpigmentation
– Hepatosplenomegaly
– Hyperuricemia (Hx)

Abnormality Neuropathy
Ulcerations Hereditary sensory and autonomic neuropathies, diabeticHypopigmentation Sarcoid, leprousHyperpigmentation POEMS, adrenomyeloneuropathy, cobalamin deficient
eosinophilia-myalgia syndromePurpura Cryoglobulinemic neuropathy (vasculitis)Livido reticularis Cryoglobulinemic neuropathy (vasculitis)Ichthyosis Refsum diseaseAngiokeratomas Fabry diseaseVesicles and bullae Variegate porphyriaAlopecia Hypothyroid, systemic lupus erythematosus, thalliumCurly hair Giant axonal neuropathyMees’ lines Arsenic and thallium toxicityWhite nails POEMS*Clubbing POEMS*, paraneoplastic (lung cancer), neuropathy with
pulmonary disease, Neuropathy with cirrhosis, neuropathy with inflammatory bowel disease
Skin, Hair, and Nail Changes Associated with Peripheral Neuropathies
Hyperpigmentation POEMS
adrenomyeloneuropathy
cobalamin deficient
eosinophilia-myalgia syndrome

Paraproteinemic Disorders associated with Neuropathy
•Multiple myeloma•Waldenstrom macroglobulinemia•POEMS (Osteosclerotic myeloma)•Amyloidosis•Cryoglobulinemia•Lymphoma (Castleman’s disease)
Ultrasound upper abdomen:
Mild-to-moderate hepatomegaly with mild increased echogenicity of liver parenchyma, no space-taking lesions, and no intrahepatic and common bile duct dilatation; no gall stone; moderate splenomegaly with mild increased echogenicity; no ascites; and no lymphadenopathy
Echocardiography:
All valvular structures appeared normal.
All cardiac chambers were not dilated. Good LV systolic function (LVEF 80% by Teich) without RWMA. RV normal contraction.
Doppler and color flow study showed normal.
Neither intracardiac thrombus nor pericardial effusion was detected.

P olyneuropathy
O rganomegaly (liver, spleen, lymph nodes,
cardiomyopathy)
E ndocrinopathy (diabetes mellitus, hypothyroidism,
gynecomastia, impotence, amenorrhea, elevated FSH)
M onoclonal gammopathy (M-spike)
S kin changes (hypertrichosis, hyperpigmentation, diffuse
skin thickening, hemangiomas, white nail beds)
Other features: wt loss, clubbing of fingers, peripheral edema, ascites, papilledema polycythemia, leukocytosis, thrombocytosis
POEMS Syndrome (Crow-Fukase Syndrome, Osteosclerotic myeloma)

Resembles CIDP with proximal and distal Weakness
Hypo-or areflexia
Large-fiber sensory loss (proprioception and vibration > pain and temperature)
Autonomic fibers spared
Cranial nerves spared (except for occasional papilledema)
Chronic, slowly progressive courses
Electrophysiologic features may be predominatly axonal or demyelinating
Clinical Features of the Neuropathy of Osteosclerotic Myeloma

Criteria for Diagnosis POEMS





Bone lesions in POEMS
• Osteosclerotic only 54-94%
• Mixed sclerotic and lytic 31-59%
• Lytic only 0-13%
• Solitary lesion 41-45%
• 2 or 3 lesions 23%
• >3 lesions 32%


Clinical diagnosis
• POEMS syndrome

Criteria for Diagnosis POEMS


• Serum protein immune electrophoresis:
Monoclonal gammopathy IgG ,lambda type
light chain
• Serum free light chain-kappa 59.3 mg/L
(3.30-19.40)
• Serum free light chain-lambda 55.5 mg/L
(5.71-26.30)• IgG 1990 mg/dL (700-1900)
• IgM 224 mg/dL (40-230)
• IgA 307 mg/dL (70-400)
• B2 Microglobulin 2461.2 ug/L (670-1310)

• Bone marrow aspiration: Hypocellular
marrow, plasma cell 8%







• Bone marrow biopsy
– Plasma cell neoplasm, mature plasma cells,
diffuse involvement.

Thank You…