acoustics for hospitals: fgi guidelines, hcahps, and...
TRANSCRIPT

Acoustics forHospitals: FGI
Guidelines, HCAHPS,and LEED
Jeff BoldtKJWW Engineering

PresenterJeff Boldt, PE, LEED® AP, HBDPKJWW Engineering (~500 staff)
Principal – Director of Engineering• Voting Member ASHRAE SSPC-90.1
– Chair - 90.1 Healthcare Working Group (WG),Hydronic WG, Elevator WG, Duct Leakage WG
• Member ASHRAE 189.1• Author AEDG Small & Large Healthcare• 2 Years Post-Graduate Acoustical Engineering
– Herriot-Watt University Edinburgh, Scotland– Member FGI Acoustics Working Group

FGI 2010

When Guidelinesare Required
Joint CommissionBeginning in January 2011, the JointCommission requires compliance with the2010 Guidelines in its accreditation manuals.
The Joint Commission does not mandateuse of the Guidelines if another state ornational standard is being applied to aproject.

When Guidelines areRequired
• States that Adopt:– January, 2012 list– Georgia, Iowa, Louisiana,
Massachusetts, New Jersey, New York,Pennsylvania, Virginia, Washington,Wisconsin (ventilation only)

Who Adopts Now

FGI Requirements
• At least 14 pages contain acousticalrequirements.
• Virtually no facilities comply with allof the 2010 requirements!

FGI Requirements
Acoustical Categories• Site Exterior Noise• Speech Privacy• Room Sound Absorption• Room Noise Levels• Isolation Between Rooms• Vibration• Misc. (Helipads, Noise Control, NICU)

2010 FGI in General
“The planning and design of new healthcare facilities and the retrofitting ofexisting health care facilities shall conformto these Guidelines and all applicablecodes and regulations with respect toexterior environmental sound and interiorsound within all occupied buildingspaces.” (1.2-6.1.1)
Site Exterior Noise
“Building facade sound isolationperformance shall depend on the siteclassification and shall be as required toprovide acceptable interior sound levels.”(1.2-6.1.2.3) (1.2-4.1.1 proposed for 2014)

Site Exterior Noise
Noise NOT produced by the facilityA = minimalB = moderateC = significantD = extreme
Façade design depends on category

Site Exterior Noise

Hard in Loud Areas
• Standard double-pane glass = STC-32• Thick laminated glass = STC-39• Limits the allowable glazed areas• For B, C or D,
determine exteriornoise usingANSI/ASA S12.9 testfor at least one week.

Exterior Survey

Your Exterior Noise
• Based on exterior noise category• Recommends maximum property line
noise levels produced by the facility(Not mandatory)
• Local codes may be more strict– (e.g. Illinois is much stricter)

You Can Comply!

Speech Privacy
“Spaces shall bedesigned to meetspeech privacy goalsusing one of the fourspeech privacy ratingmethods as shown inTable 1.2-4.”
(1.2-6.1.6.1) (1.2-4.1.6.1)

Speech Privacy
* Some changes proposed for 2014
Sound Absorption
“All normally occupied health care facilityspaces shall incorporate acoustic finishesto achieve design room average soundabsorption coefficients equal to or greaterthan in Table 1.2-1.”(1.2-6.1.3) (1.2-4.1.3)

Sound Absorption
• Gypsum Board = 0.07• Vinyl Flooring = 0.03


Room Noise Levels
“Room noise levels shall fall within thesound level ranges shown for the chosenrating system in Table 1.2-2.”(1.2-6.1.4) (1.2-4.1.4.1)
• Noise levels determined for the unoccupiedroom (w/o operating medical equipment).
Designing within a 10 dBA range is hard!• I believe this requires sound masking.• Proposed to be only maximums for 2014.

Room Noise LevelsRoom Type NC/RC(N)/RNC dBAPatient Rooms 30 - 40 35 - 45Multiple Occupant Patient Care Areas 35 - 45 40 - 50NICU 25 - 35 30 - 40Operating Rooms* 35 - 45 40 - 50Corridors and Public Spaces 35 - 45 40 - 50Testing/Research Lab, Minimal Speech* 45 - 55 50 - 60Research Lab, Extensive Speech* 40 - 50 45 - 55Group Teaching Lab 35 - 45 40 - 50Doctor's Offices, Exam Rooms 30 - 40 35 - 45Conference Rooms 25 - 35 30 - 40Teleconferencing Rooms ≤ 25 ≤ 30Auditoriums, Large Lecture Rooms 25 - 30 30 - 35* in appendix
Room Noise Levels
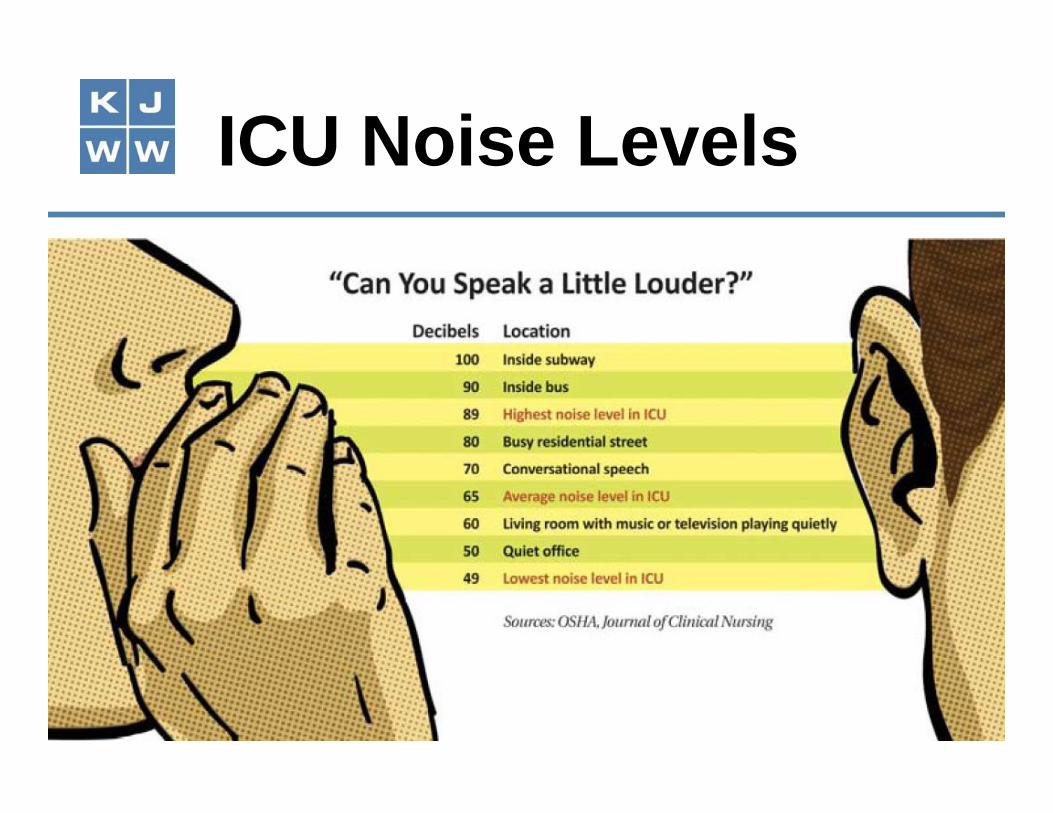
ICU Noise Levels
Predicting Noise Levels
OR TestingRecommends40-50 dBA<55 dBA
Too loud, IMO
Auditorium Testing

Isolation Between Rooms
“The composite sound transmission class(STCC) rating of demising wall assembliesshall not be less than the ratings indicatedin Table 1.2-3.”(1.2-6.1.5.2) (1.2-4.1.5.2)Table includes floors.

Isolation Between Rooms

STCc 35 STCc 45Patient room tocorridor and examroom to corridor• 4-inch stud cavity• 1 layer of 5/8-inch
gypsum each side• 2-inch glass fiber batting• Construction gaps and
electrical boxes sealed
Patient room topatient room
• Additional layer of5/8-inch gypsumto one side ofassembly.
• Viscoelasticadhesive betweenlayers.

STCc 50 STCc 60Patient room topublic spaceNICU to patientroom or corridor
• Staggered studconstruction oncommon 6-inchplate.
Patient room toservice area
• Staggered-studconstruction onseparate 4-inchplates.

Vibration
“Vibration levels in the building shall notexceed applicable guidelines and limitsoutlined in this section.”(1.2-6.1.7.2) (1.2-4.1.7.2)
“Vibration should not exceed levels inANSI S2.71.”(A1.2-6.1.7) (A1.2-4.1.7)

Equipment Vibration
“All fixed building equipment that rotatesor vibrates shall be considered forvibration isolation.”(1.2-6.1.7.2) (1.2-4.1.7.2)
“The types of isolators and isolator staticdeflections shall be as recommended inASHRAE Handbook -HVAC Applications.”(1.2-6.1.7.2(1)) (1.2-4.1.7.2(1))
Footfall Vibration
“The structural floor shall be designed toavoid footfall vibration levels that exceedthe peak vibration velocities inTable 1.2-5.”(1.2-6.1.7.2 (2)) (1.2-4.1.7.2 (2))(Evaluated per AISC Design Guide 11)
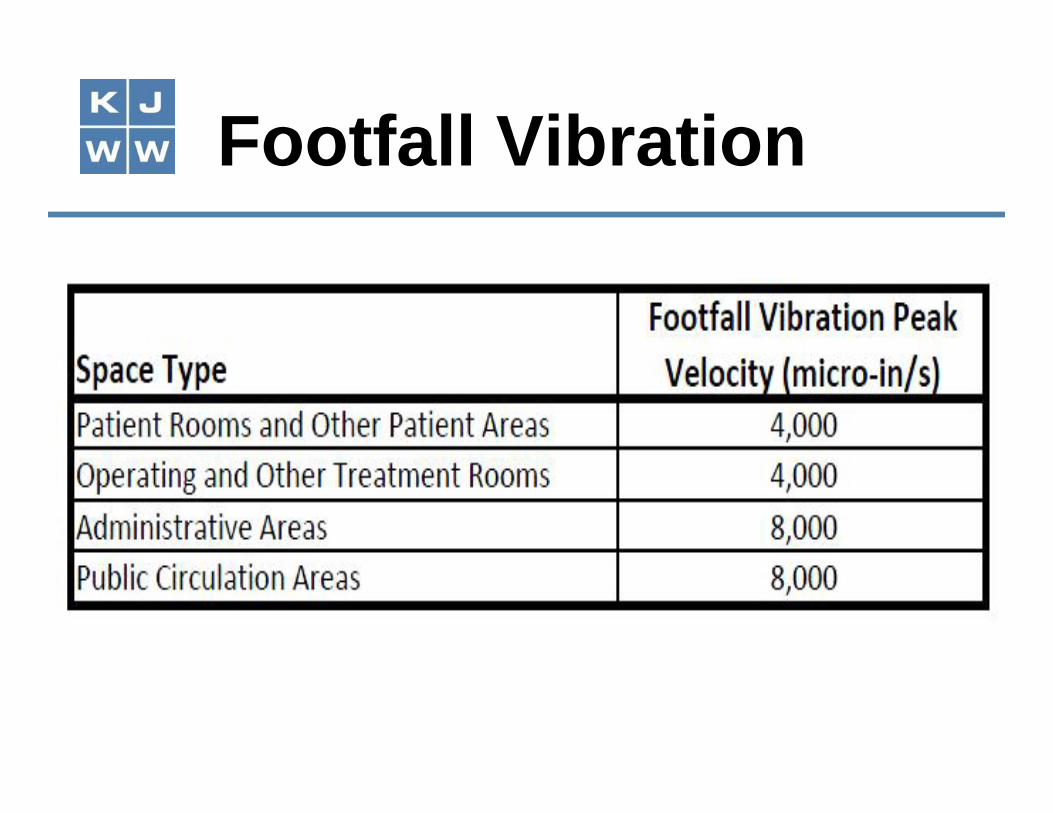
Footfall Vibration

Vibration
• Not trivial to comply.• Steel with concrete
slab is predictable.(Heavier constructionthan normal)
• CIP concrete is morelikely to comply.(Prediction duringdesign is difficult.)

Helipads
• “Facilities with helipads shallincorporate noise mitigation strategiesto meet the acoustic requirements.”
• “Special consideration”required when:• 700 feet or less to patient areas• Pad on top of building• Over two night flights per week

Noise Control
“Recreation rooms, exercise rooms,equipment rooms, and similar spaceswhere impact noises may be generatedshall not be located directly over patientbed areas or delivery and operatingsuites, unless special provisions aremade to minimize such noise.”(2.1-7.2.2.12)

NICU

NICU
“Infant rooms (including airborne infectionisolation rooms), staff work areas, familyareas, and staff lounge and sleepingareas - and the spaces opening ontothem - shall be designed to produceminimal background noise and to containand absorb much of the transient noisethat arises within them.”(2.2-2.10.9.3)
NICU - Proposed
“Infant rooms (including airborne infectionisolation rooms), staff work areas, familyareas, and staff lounge and sleepingareas - and the spaces opening ontothem - shall be designed to comply withroom noise criteria in Table 1.2-2.”*(2.2-2.10.9.3)
* Quietest area

NICU
“The combination of continuousbackground sound and operational soundin infant bed rooms and adult sleep areasshall not exceed an hourly Leq of 45 dBAand an hourly L10 of 50 dBA. The Lmax(transient sounds) shall not exceed 65dBA in these rooms/ areas.” *(2.2-2.10.9.3 (1))
* Proposed to be deleted in 2014.

NICU
“Ceilings shall have a noise reductioncoefficient (NRC) of 0.95 for 80 percent ofthe entire surface area or an average NRCof 0.85 for the entire ceiling, includingreflective and acoustically absorptivesurfaces.”(2.2-2.10.9.1 (2))

NICU
“Ceilings in infantrooms and adultsleep areas shallhave a ceilingattenuation class(CAC) of 29 orhigher.”(2.2-2.10.9.1 (2))

NICU Noise
Fire alarms in the infant area should berestricted to flashing lights without anaudible signal. The audible alarm level inother occupied areas must be adjustable.

NICU Noise
Telephones audiblefrom the infant areashould have adjustableannouncing signals.

NICU Lighting
• “Provisions shall be made for indirectlighting and high-intensity lighting.”(2.2-2.10.9.2)
• “Electric light sources shall have colorrendering index of no less than 80, afull-spectrum color index of no less than55, and a gamut area of no less than 65and no greater than 100.”(2.2-2.10.9.2)

NICU Lighting
“No direct ambient lighting shall bepermitted in the infant care space, andany direct ambient lighting used outsidethe infant area shall be located or framedto avoid a direct line of sight from anyinfant to the fixture.”(2.2-2.10.9.2)

LEED for Healthcare
Up to 2 LEED-HC Points• No prerequisites• 1 point: Sound isolation & privacy per FGI-
2010; room noise levels per FGI-2010• 1 more point: Do items above; acoustical
finishes (calculate or measure); site exteriornoise (comply with SV Guidelines and FGI-2010 envelope requirements)

HCAHPS• Hospital Consumer Assessment of
Healthcare Provider & Systems• Quarterly standardized assessment, by
adult inpatients, of their perception oftotal quality of care.

HCAHPS
• Compare Hospitals – TodayYour scores will drive patients to or away fromyour facility.

Your Best Hospital…

HCAHPS
• 8 criteria (effectively 6)“Patients who reported that the area aroundtheir room was "Always" quiet at night.”

Patient Survey Results

HCAHPS
• Healthcare exit survey cites acoustics& noise as #1 complaint.
• Studies:– Akansel, N (2008)– Gurses & Carayon, (2009)
• Medical machines, equipment, alarms,paging, etc., tops on list. Medicalequipment matters.

HCAHPS
I am not a reimbursement expert, but herecomes the math …

HCAHPS MathInpatient $3,000/day bill (CA average)
• HCAHPS 80% quietness vs. 50% quietnessscore
• 1% of reimbursement based on performance(rising to 2% in 2017)
• 70% outcomes / 30% HCAHPS• 80% vs. 50% = 30% improvement• 1 of 6 objective scores (also affects 2 others)• $3,000*1%*30%*30%/6 = $164 per patient
room per year ($328/room-year in 2017)

Why Improve Acoustics?
• HCAHPS reimbursement– Worth about $1,000 per patient room
• More patients via HACHPS survey– What’s the value?
• More patients via better patientsatisfaction

Solve FGI & HCAHPS
• Hire an acoustical consultant– Pick one who understands HVAC and
equipment
• Get an audit

Advance Planning
• Design facility modifications• Staff training• Repeat audit
– Demonstrate improvements for JCAHO oryour AHJ
This is Not a DIY
• Survey requires expertise and expensiveequipment
• Recommendations need expertise• Follow-up survey needs expertise

Maybe Later a DIY
• If you have a smart staffer shadow thesurveyor, follow-ups can become DIY ifit is worth the instrument cost, and yourequire the surveyor to train yourshadow.

What is best ROI?• Education for staff may be the cheapest way
to improve HCAHPS scores• Have the consultant present an acoustics
seminar so your staff understands.• Invite the nurses!
Test Equipment

Sound Meters
50 dB 40 dB 35 dB 30dB 20dB-integrates$50 $120 $200 $4,000 ~$10,000

Summary
• Action now can avoid headaches later.• Acoustical improvements can bring in
more patients now.• Prepare for surveys based on FGI 2010
or 2014.• A few firms can provide your acoustical
needs and integrate them with HVACsystems and medical equipmentselections.

Questions for you• How many facilities have had acoustical surveys?• How important are HCAHPS scores to you?• Do you plan to wait for a requirement for FGI-2010
compliance, or to comply soon to improve yourperformance and customer satisfaction?
• How much emphasis do you place on the ability ofpatients to sleep?
• Are most of your noise complaints HVAC, medicalequipment, paging, or staff activities?
Have questions?Contact:Jeff BoldtKJWW Engineering(608) [email protected]