adapting healthcare messages for pregnant indigenous australian women
TRANSCRIPT
Adapting Healthcare Messages For Pregnant Indigenous Australian
Women
By Reece George
Traditional greeting
• Matu Man, traditionally from the Pilbra region of Western Australia.
• http://bit.ly/1Q5AMHI• Photos from ‘country’.
Beyondie
New homestead
Muster
Desert Pea
Waterhole
Bastard eggs
Ghost gums
The creek
‘Bungarra’

Jumping 45 years.
• http://www.mobilemamaalliance.org/
• Support Millennium Development Goals 4 and 5, which address maternal and child health.
Jumping 45 years.
• http://www.mobilemamaalliance.org/
• Support Millennium Development Goals 4 and 5, which address maternal and child health.
• Directly assists programs in Bangladesh, South Africa, India and Nigeria
Mobile messages
• Mobile health messages are portable, accessible and discreet and can be saved or shared. They can provide information, dispel myths, highlight warning signs and connect pregnant women and new moms with local health services.
• MAMA’s adaptable messages are based on WHO and UNICEF guidelines and have been developed in close collaboration with a group of global health experts who make up MAMA’s Health Content Advisory Council.

MAMA Mobile messages
• Mobile health messages are portable, accessible and discreet and can be saved or shared. They can provide information, dispel myths, highlight warning signs and connect pregnant women and new moms with local health services.
• MAMA’s adaptable messages are based on WHO and UNICEF guidelines and have been developed in close collaboration with a group of global health experts who make up MAMA’s Health Content Advisory Council.

MAMA Core SMS
• The core messages are arranged by "age and stage" in two sets. The pregnancy/baby messages cover weeks 5 to 42 of pregnancy, and the first year of the baby's life. The child messages cover ages 1-3.
• This project only focusing on pregnancy messages. Scope for further research.
• Examples
MAMA Core SMS
• The core messages are arranged by "age and stage" in two sets. The pregnancy/baby messages cover weeks 5 to 42 of pregnancy, and the first year of the baby's life. The child messages cover ages 1-3.
• This project only focusing on pregnancy messages. Scope for further research.
• Examples

MAMA Core SMS
• The core messages are arranged by "age and stage" in two sets. The pregnancy/baby messages cover weeks 5 to 42 of pregnancy, and the first year of the baby's life. The child messages cover ages 1-3.
• This project only focusing on pregnancy messages. Scope for further research.
• Examples
Real world application
• https://www.youtube.com/watch?v=nwxVRzCuxZ4
MAMA BangladeshResearch
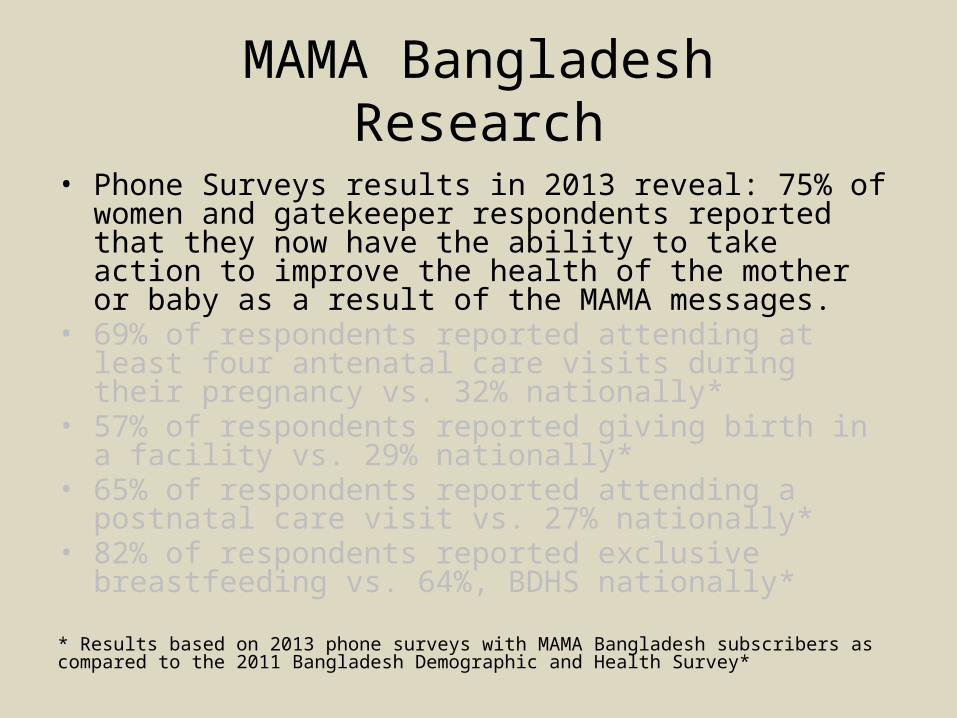
• Phone Surveys results in 2013 reveal: 75% of women and gatekeeper respondents reported that they now have the ability to take action to improve the health of the mother or baby as a result of the MAMA messages.
• 69% of respondents reported attending at least four antenatal care visits during their pregnancy vs. 32% nationally*
• 57% of respondents reported giving birth in a facility vs. 29% nationally*
• 65% of respondents reported attending a postnatal care visit vs. 27% nationally*
• 82% of respondents reported exclusive breastfeeding vs. 64%, BDHS nationally*
* Results based on 2013 phone surveys with MAMA Bangladesh subscribers as compared to the 2011 Bangladesh Demographic and Health Survey*
MAMA BangladeshResearch
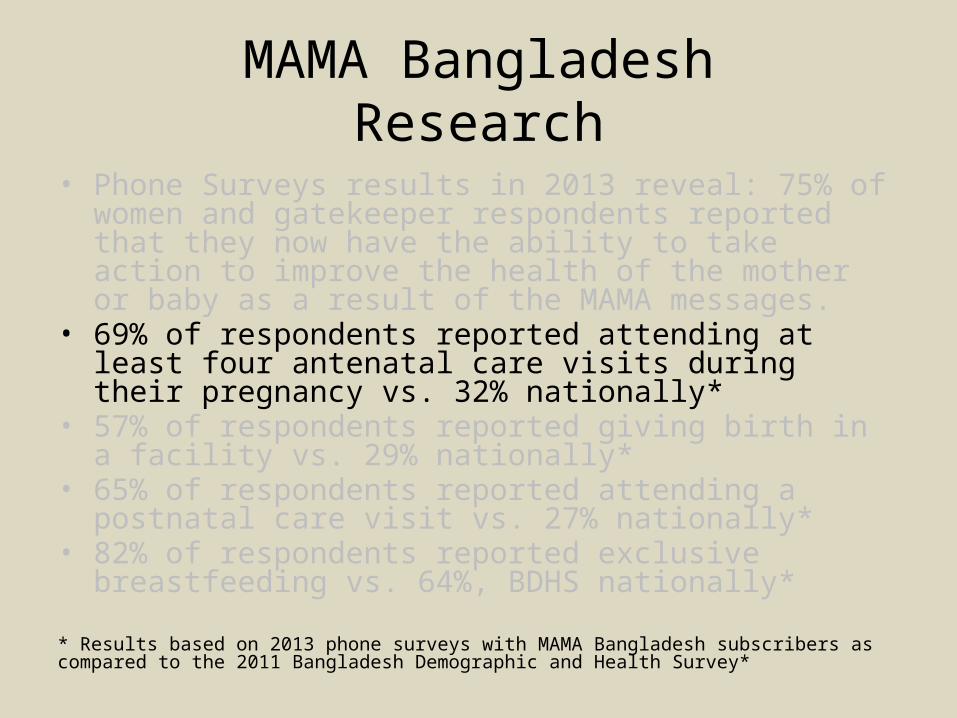
• Phone Surveys results in 2013 reveal: 75% of women and gatekeeper respondents reported that they now have the ability to take action to improve the health of the mother or baby as a result of the MAMA messages.
• 69% of respondents reported attending at least four antenatal care visits during their pregnancy vs. 32% nationally*
• 57% of respondents reported giving birth in a facility vs. 29% nationally*
• 65% of respondents reported attending a postnatal care visit vs. 27% nationally*
• 82% of respondents reported exclusive breastfeeding vs. 64%, BDHS nationally*
* Results based on 2013 phone surveys with MAMA Bangladesh subscribers as compared to the 2011 Bangladesh Demographic and Health Survey*

MAMA BangladeshResearch
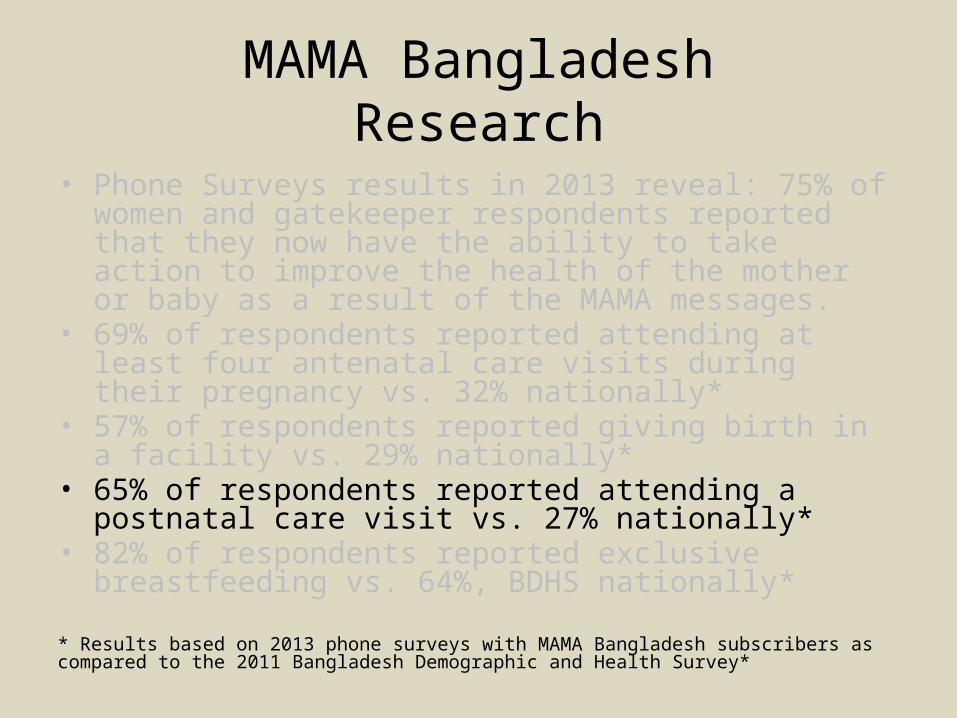
• Phone Surveys results in 2013 reveal: 75% of women and gatekeeper respondents reported that they now have the ability to take action to improve the health of the mother or baby as a result of the MAMA messages.
• 69% of respondents reported attending at least four antenatal care visits during their pregnancy vs. 32% nationally*
• 57% of respondents reported giving birth in a facility vs. 29% nationally*
• 65% of respondents reported attending a postnatal care visit vs. 27% nationally*
• 82% of respondents reported exclusive breastfeeding vs. 64%, BDHS nationally*
* Results based on 2013 phone surveys with MAMA Bangladesh subscribers as compared to the 2011 Bangladesh Demographic and Health Survey*
MAMA BangladeshResearch
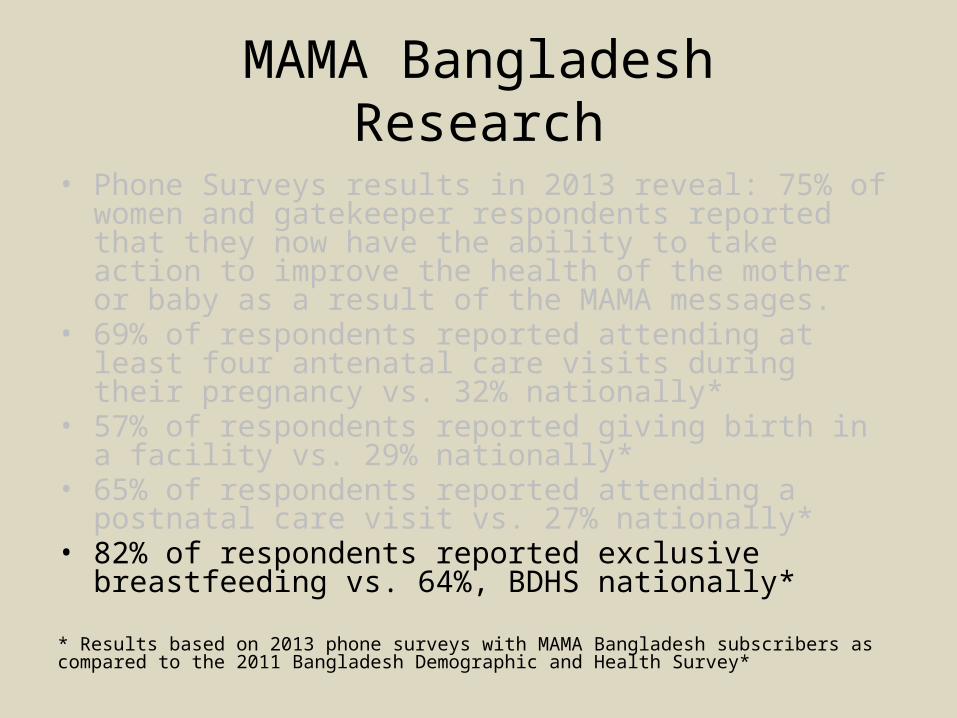
• Phone Surveys results in 2013 reveal: 75% of women and gatekeeper respondents reported that they now have the ability to take action to improve the health of the mother or baby as a result of the MAMA messages.
• 69% of respondents reported attending at least four antenatal care visits during their pregnancy vs. 32% nationally*
• 57% of respondents reported giving birth in a facility vs. 29% nationally*
• 65% of respondents reported attending a postnatal care visit vs. 27% nationally*
• 82% of respondents reported exclusive breastfeeding vs. 64%, BDHS nationally*
* Results based on 2013 phone surveys with MAMA Bangladesh subscribers as compared to the 2011 Bangladesh Demographic and Health Survey*
MAMA BangladeshResearch
• Phone Surveys results in 2013 reveal: 75% of women and gatekeeper respondents reported that they now have the ability to take action to improve the health of the mother or baby as a result of the MAMA messages.
• 69% of respondents reported attending at least four antenatal care visits during their pregnancy vs. 32% nationally*
• 57% of respondents reported giving birth in a facility vs. 29% nationally*
• 65% of respondents reported attending a postnatal care visit vs. 27% nationally*
• 82% of respondents reported exclusive breastfeeding vs. 64%, BDHS nationally*
* Results based on 2013 phone surveys with MAMA Bangladesh subscribers as compared to the 2011 Bangladesh Demographic and Health Survey*
MAMA South Africa Research
Most participants in a 2013 focus group discussion felt the MAMA messages gave them new information about how to care for their baby, and specifically mentioned:
• When to introduce solid foods• How to monitor developmental milestones• When to vaccinate• That they should never to leave the child
unattended on a bed or couch

Why Indigenous Australian women?
• The cost of healthcare for Indigenous Australians compared to non-Indigenous Australians is not only more expensive but also the maternal health outcomes are significantly worse.
• In Australia, Indigenous health expenditure was estimated to be $4.55 billion in 2010–11, 3.7% of the total Australian health expenditure (Australian Institute of Health and Welfare [AIHW], 2013).
• There is a higher prevalence of smoking during pregnancy, hypertensive disorders, teenage pregnancy and gestational diabetes (Prime Minister's Science, Engineering and Innovation Council 2008).
Why Indigenous Australian women?
• The cost of healthcare for Indigenous Australians compared to non-Indigenous Australians is not only more expensive but also the maternal health outcomes are significantly worse.
• In Australia, Indigenous health expenditure was estimated to be $4.55 billion in 2010–11, 3.7% of the total Australian health expenditure (Australian Institute of Health and Welfare [AIHW], 2013).
• There is a higher prevalence of smoking during pregnancy, hypertensive disorders, teenage pregnancy and gestational diabetes (Prime Minister's Science, Engineering and Innovation Council 2008).
Why Indigenous Australian women?
• The cost of healthcare for Indigenous Australians compared to non-Indigenous Australians is not only more expensive but also the maternal health outcomes are significantly worse.
• In Australia, Indigenous health expenditure was estimated to be $4.55 billion in 2010–11, 3.7% of the total Australian health expenditure (Australian Institute of Health and Welfare [AIHW], 2013).
• There is a higher prevalence of smoking during pregnancy, hypertensive disorders, teenage pregnancy and gestational diabetes (Prime Minister's Science, Engineering and Innovation Council 2008).
State of Indigenous Maternal Health
• The maternal mortality ratio for Indigenous Australian women between 2003-2005 was 21.5 deaths per 100,000, for non-Indigenous Australian women the ratio was 7.9 per 100,000 Sullivan, Hall and King (2008). This is known to be underestimated (Kildea, 2008 in Bar-Zeev et al., 2014).
• Perinatal death rate is twice as high for Indigenous Australian infants (17.3 per 1000 births) compared to non-Indigenous Australian infants (9.7 per 1000 births), as is preterm birth (13.3% v. 8.0%) and low birth weight (12.4% v. 5.9%) (Li, Zeki, Hilder, & Sullivan, 2012, in Bar-Zeev et al., 2014).
State of Indigenous Maternal Health
• The maternal mortality ratio for Indigenous Australian women between 2003-2005 was 21.5 deaths per 100,000, for non-Indigenous Australian women the ratio was 7.9 per 100,000 Sullivan, Hall and King (2008). This is known to be underestimated (Kildea, 2008 in Bar-Zeev et al., 2014).
• Perinatal death rate is twice as high for Indigenous Australian infants (17.3 per 1000 births) compared to non-Indigenous Australian infants (9.7 per 1000 births), as is preterm birth (13.3% v. 8.0%) and low birth weight (12.4% v. 5.9%) (Li, Zeki, Hilder, & Sullivan, 2012, in Bar-Zeev et al., 2014).
Cultural Issues• Thomas’s (2004) book, Reading Doctor’s Writing
was an attempt to understand, rather than ignore the entanglement of healthcare research and the brutality of colonialism in Australia. Thomas reports… ‘The control of the sexuality of Indigenous people, especially Indigenous women (but rarely their sexual partners if they were white men), was the central element of policy and power’ (2004, p. 21). As a result of healthcare research, this central policy theme was responsible some of the cruelest excesses of colonialism.
Cultural IssuesLinda Tuhiwia-Smith, an Indigenous researcher and member of the Maori community, provides this sobering perspective: • Stories about research and particularly researchers (the human carriers of
research) were intertwined with stories about all other forms of colonisation and injustice. There were cautionary tales where the surface story was not as important as the underlying examples of cultural protocol broken, values negated, small tests failed and key people ignored. The greater danger, however, was in the creeping policies that intruded into every aspect of our lives, legitimated by research, informed more often by ideology. The power of the research was not in the visits made by researchers to our communities, nor by their fieldwork and the rude questions they often asked . . . ‘We are the most researched people in the world’ is a comment I have heard frequently from several Indigenous communities. The truth of such a comment is unimportant, what does need to be taken seriously is the sense of weight and unspoken cynicism about research that the message conveys (1999, p. 3).
Cultural Issues
• Matthews (2011) report on more recent events, describing the insidious nature of “culturally insensitive research designs and methodologies that fail to match the needs, customs, and standards of Aboriginal communities” (p. 2). They refer to the “ample examples of contemporary research that has inappropriately required Aboriginal people to discuss sensitive topics that violate culturally determined gender roles or community structures of authority” (2011, p. 2).

Women’s/Men’s Business
• A serious need for methodology design to proceed with caution, with respect to cultural requirements.
• ‘Men’s business’ involves hunting, conflicts, the land, male anatomy and male ceremonial business (Maher, 1999, p. 232). ‘Women’s business’ is defined by Reid (1979) as... 'experience and knowledge of menstruation, pregnancy, childbirth and contraception' (cited in Barclay, Andre and Glover 1989, p. 122).
Women’s/Men’s Business
• A serious need for methodology design to proceed with caution, with respect to cultural requirements.
• ‘Men’s business’ involves hunting, conflicts, the land, male anatomy and male ceremonial business (Maher, 1999, p. 232). ‘Women’s business’ is defined by Reid (1979) as... 'experience and knowledge of menstruation, pregnancy, childbirth and contraception' (cited in Barclay, Andre and Glover 1989, p. 122).
Women’s Business• Traditionally, Aboriginal women gave birth in the place
where they were born, ‘on country’ with other women by their side. Young women learn about borning and the Grandmothers Law from the older women during their first labour. Birthing is ‘women’s business’ and intricately related to ‘Aboriginal Law’ and the ‘Dreamtime’. The dreamtime explains creation and many of the rules and symbols are expressed in the myths and stories that are passed from generation to generation. The process of borning is a process where the spirit of the land and the people come together, and the place where a person is born establishes their relationship to the land (Kildea, Wardaguga & Dawumal, 2004, The Centre, para. 2).

Women’s/Men’s Business within a Healthcare Context
• Breaches of these traditional divisions (e.g. female nurse washing elderly initiated male Aboriginal, a female nurse teaching an Aboriginal man self-catheterisation or a male doctor undertaking a vaginal inspection) is likely to cause great distress and ‘shame’. Shame is a complex concept that is difficult to translate into non-Aboriginal English (Maher, 1999, p. 232).
• Domestic violence, grog (alcohol) use and smoking are real big problems... but we (non-Aboriginal midwives) can't be the one trying to talk to them (pregnant women) about this... it needs to be health workers, the old ladies (Elders) doing all the talking… I feel like it always comes across like your shaming (embarrassing, humiliating) them if you bring it up... like pointing fingers... (Bar-Zeev et al., 2014, p. 293).
Women’s/Men’s Business within a Healthcare Context
• Breaches of these traditional divisions (e.g. female nurse washing elderly initiated male Aboriginal, a female nurse teaching an Aboriginal man self-catheterisation or a male doctor undertaking a vaginal inspection) is likely to cause great distress and ‘shame’. Shame is a complex concept that is difficult to translate into non-Aboriginal English (Maher, 1999, p. 232).
• Domestic violence, grog (alcohol) use and smoking are real big problems... but we (non-Aboriginal midwives) can't be the one trying to talk to them (pregnant women) about this... it needs to be health workers, the old ladies (Elders) doing all the talking… I feel like it always comes across like your shaming (embarrassing, humiliating) them if you bring it up... like pointing fingers... (Bar-Zeev et al., 2014, p. 293).

Responsibility of Senior Indigenous Australian Women
• Maternal healthcare is the traditional responsibility of senior women. Senior female family members such as grandmothers and aunts assume important social roles to pregnant women. Older women are greatly respected and are often considered to have the special knowledge and experience to attend to women during pregnancy, childbirth and the postpartum period (Callaghan, 2001).
A Methodology• This methodology was only possible following recommendations
from MAMA, consultations with senior Indigenous Australian women, consultations with healthcare professionals, and peer reviews from The University ethics committee and the Aboriginal Health and Medical Research Council (AH&MRC).
• The projects theoretical foundation originated within the discipline of Human Computer Interaction (HCI), specifically, within the discipline of Captology, which includes the study of Persuasive Technology.
• From persuasive technology, MAMA, in the development of the original messages, chose BJ Fogg’s model of behavior change.
• It was possible to extend and modify its usage for continued application to the current study. The process is detailed in Fogg’s paper, Creating Persuasive Technologies: An Eight-Step Design Process (2009).

A Methodology• This methodology was only possible following recommendations
from MAMA, consultations with senior Indigenous Australian women, consultations with healthcare professionals, and peer reviews from The University of Newcastle ethics committee and the Aboriginal Health and Medical Research Council (AH&MRC).
• The projects theoretical foundation originated within the discipline of Human Computer Interaction (HCI), specifically, within the discipline of Captology, which includes the study of Persuasive Technology.
• From persuasive technology, MAMA, in the development of the original messages, chose BJ Fogg’s model of behavior change.
• It was possible to extend and modify its usage for continued application to the current study. The process is detailed in Fogg’s paper, Creating Persuasive Technologies: An Eight-Step Design Process (2009).
A Methodology• This methodology was only possible following recommendations
from MAMA, consultations with senior Indigenous Australian women, consultations with healthcare professionals, and peer reviews from The University of Newcastle ethics committee and the Aboriginal Health and Medical Research Council (AH&MRC).
• The projects theoretical foundation originated within the discipline of Human Computer Interaction (HCI), specifically, within the discipline of Captology, which includes the study of Persuasive Technology.
• From persuasive technology, MAMA, in the development of the original messages, chose BJ Fogg’s model of behavior change.
• It was possible to extend and modify its usage for continued application to the current study. The process is detailed in Fogg’s paper, Creating Persuasive Technologies: An Eight-Step Design Process (2009).
A Methodology• This methodology was only possible following recommendations
from MAMA, consultations with senior Indigenous Australian women, consultations with healthcare professionals, and peer reviews from The University of Newcastle ethics committee and the Aboriginal Health and Medical Research Council (AH&MRC).
• The projects theoretical foundation originated within the discipline of Human Computer Interaction (HCI), specifically, within the discipline of Captology, which includes the study of Persuasive Technology.
• From persuasive technology, MAMA, in the development of the original messages, chose BJ Fogg’s model of behavior change.
• It was possible to extend and modify its usage for continued application to the current study. The process is detailed in Fogg’s paper, Creating Persuasive Technologies: An Eight-Step Design Process (2009).
Persuasive TechnologyPersuasive technology is defined in the Proceedings in First International Conference on Persuasive Technology,(2006) as: • Persuasive technology is the general class of technology that has
the explicit purpose of changing human attitudes and behaviors. Persuasive technologies apply principles of social psychology in influencing people; principles of credibility, trust, reciprocity, authority and the like. … The scope of technologies that hold persuasive potential is broader than ICT alone, and includes persuasive product design and architectural design, yet the interactive nature of computers uniquely enables user-sensitive and user-adaptive responding, allowing persuasive messages to be tailored to the specific user in question, presented at the right place and at the right time, thereby heightening their likely persuasive impact (Ijsselsteijn 2006, p. v).
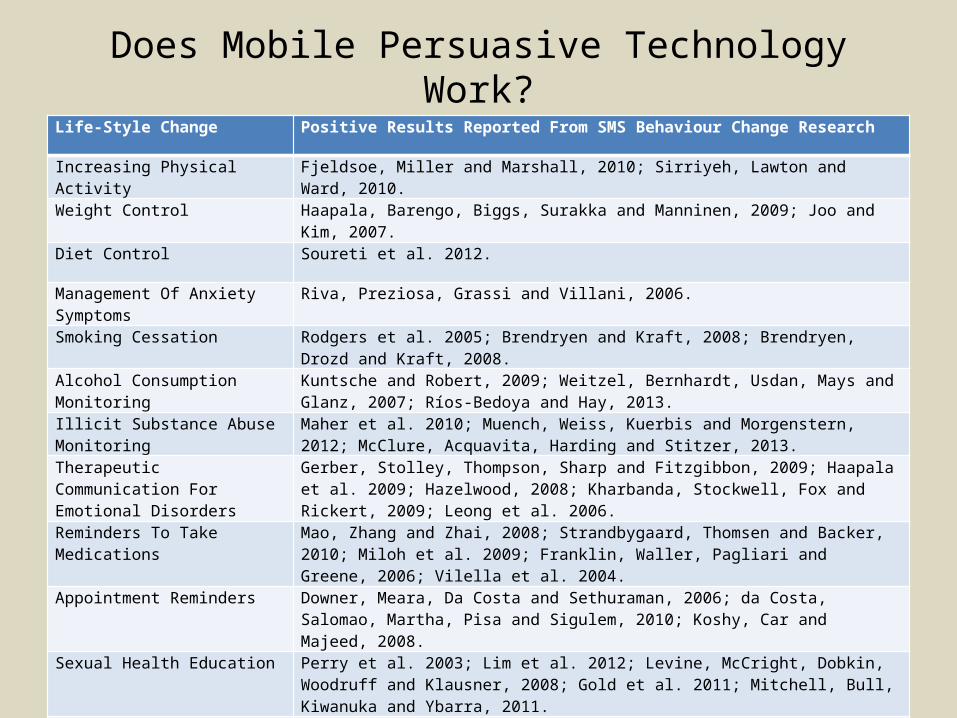
Does Mobile Persuasive Technology Work?Life-Style Change Positive Results Reported From SMS Behaviour Change Research
Increasing Physical Activity Fjeldsoe, Miller and Marshall, 2010; Sirriyeh, Lawton and Ward, 2010.
Weight Control Haapala, Barengo, Biggs, Surakka and Manninen, 2009; Joo and Kim, 2007.
Diet Control Soureti et al. 2012.
Management Of Anxiety Symptoms Riva, Preziosa, Grassi and Villani, 2006.
Smoking Cessation Rodgers et al. 2005; Brendryen and Kraft, 2008; Brendryen, Drozd and Kraft, 2008.
Alcohol Consumption Monitoring Kuntsche and Robert, 2009; Weitzel, Bernhardt, Usdan, Mays and Glanz, 2007; Ríos-Bedoya and Hay, 2013.
Illicit Substance Abuse Monitoring Maher et al. 2010; Muench, Weiss, Kuerbis and Morgenstern, 2012; McClure, Acquavita, Harding and Stitzer, 2013.
Therapeutic Communication For Emotional Disorders
Gerber, Stolley, Thompson, Sharp and Fitzgibbon, 2009; Haapala et al. 2009; Hazelwood, 2008; Kharbanda, Stockwell, Fox and Rickert, 2009; Leong et al. 2006.
Reminders To Take Medications Mao, Zhang and Zhai, 2008; Strandbygaard, Thomsen and Backer, 2010; Miloh et al. 2009; Franklin, Waller, Pagliari and Greene, 2006; Vilella et al. 2004.
Appointment Reminders Downer, Meara, Da Costa and Sethuraman, 2006; da Costa, Salomao, Martha, Pisa and Sigulem, 2010; Koshy, Car and Majeed, 2008.
Sexual Health Education Perry et al. 2003; Lim et al. 2012; Levine, McCright, Dobkin, Woodruff and Klausner, 2008; Gold et al. 2011; Mitchell, Bull, Kiwanuka and Ybarra, 2011.
Contraception Adherence Castano, Bynum, Andres, Lara and Westhoff, 2012; Hou, Hurwitz, Kavanagh, Fortin and Goldberg, 2010.
Family Violence Management Howard, Friend, Parker and Streker, 2010.
Fogg’s (2009) Eight steps in early-stage persuasive design Model.
1. Choose a simple behavior to target2. Choose a receptive audience3. Find what is preventing the target behavior4. Choose an appropriate channel5. Find relevant examples of persuasion technology6. Imitate successful examples7. Test and iterate quickly8. Expand on success
Fogg (2009) intended flexibility in the process, with each step representing a milestone, rather than a rigid step-by-step process. Adapting the sequence to the circumstances, according to Fogg, ‘… is a valid part of the design process’ (Fogg 2009, p. 2).
Fogg’s (2009) Eight steps in early-stage persuasive design Model.
1. Choose a simple behavior to target2. Choose a receptive audience3. Find what is preventing the target behavior4. Choose an appropriate channel5. Find relevant examples of persuasion technology6. Imitate successful examples7. Test and iterate quickly8. Expand on success
Fogg (2009) intended flexibility in the process, with each step representing a milestone, rather than a rigid step-by-step process. Adapting the sequence to the circumstances, according to Fogg, ‘… is a valid part of the design process’ (Fogg 2009, p. 2).
Adapting Messages To the Australian Healthcare System
The first team will be made up of healthcare professionals with experience working in Indigenous healthcare, two from midwifery and two from obstetrics.
The healthcare team:
• Check that the content is correct for Indigenous Australian women.
• Adapt messages to reflect the conditions of pregnant Indigenous Australian women.
• Add new messages that address local health concerns for Indigenous Australian women. (MAMA 2014d)
Adapting Messages To the Australian Healthcare System
The first team will be made up of healthcare professionals with experience working in Indigenous healthcare, two from midwifery and two from obstetrics.
The healthcare team:
• Check that the content is correct for Indigenous Australian women.
• Adapt messages to reflect the conditions of pregnant Indigenous Australian women.
• Add new messages that address local health concerns for Indigenous Australian women. (MAMA 2014d)

Adapting Messages To the Australian Healthcare System
The first team will be made up of healthcare professionals with experience working in Indigenous healthcare, two from midwifery and two from obstetrics.
The healthcare team:
• Check that the content is correct for Indigenous Australian women.
• Adapt messages to reflect the conditions of pregnant Indigenous Australian women.
• Add new messages that address local health concerns for Indigenous Australian women. (MAMA 2014d)
Adapting Messages To Pregnant Indigenous Australian Women
The second team will be made up of senior Indigenous Australian women. Members of this team are required to be Grandmothers, Auntie’s or Mothers, the traditional owners of ‘women’s business’.
The culture team:
• Review of healthcare language: to reword the messages into the traditional style they would use if speaking personally to a younger pregnant woman.
• Review healthcare terms: for example, in some cultures, the term ‘health worker’ or ‘health clinic’ is used, but in other cultures this may not convey the correct meaning.
• Check foods and produce: references to food items must be familiar to younger Indigenous Australian women.
• Review local customs and practices: in many cultures, for example, it is common for women to eat certain foods or non-foods during pregnancy; senior women will need to reveal local practices and beliefs and adapt the messages accordingly (MAMA 2013b).

Adapting Messages To Pregnant Indigenous Australian Women
The second team will be made up of senior Indigenous Australian women. Members of this team are required to be Grandmothers, Auntie’s or Mothers, the traditional owners of ‘women’s business’.
The culture team:
• Review of healthcare language: to reword the messages into the traditional style they would use if speaking personally to a younger pregnant woman.
• Review healthcare terms: for example, in some cultures, the term ‘health worker’ or ‘health clinic’ is used, but in other cultures this may not convey the correct meaning.
• Check foods and produce: references to food items must be familiar to younger Indigenous Australian women.
• Review local customs and practices: in many cultures, for example, it is common for women to eat certain foods or non-foods during pregnancy; senior women will need to reveal local practices and beliefs and adapt the messages accordingly (MAMA 2013b).
Adapting Messages To Pregnant Indigenous Australian Women
The second team will be made up of senior Indigenous Australian women. Members of this team are required to be Grandmothers, Auntie’s or Mothers, the traditional owners of ‘women’s business’.
The culture team:
• Review of healthcare language: to reword the messages into the traditional style they would use if speaking personally to a younger pregnant woman.
• Review healthcare terms: for example, in some cultures, the term ‘health worker’ or ‘health clinic’ is used, but in other cultures this may not convey the correct meaning.
• Check foods and produce: references to food items must be familiar to younger Indigenous Australian women.
• Review local customs and practices: in many cultures, for example, it is common for women to eat certain foods or non-foods during pregnancy; senior women will need to reveal local practices and beliefs and adapt the messages accordingly (MAMA 2013b).

Adapting Messages To Pregnant Indigenous Australian Women
The second team will be made up of senior Indigenous Australian women. Members of this team are required to be Grandmothers, Auntie’s or Mothers, the traditional owners of ‘women’s business’.
The culture team:
• Review of healthcare language: to reword the messages into the traditional style they would use if speaking personally to a younger pregnant woman.
• Review healthcare terms: for example, in some cultures, the term ‘health worker’ or ‘health clinic’ is used, but in other cultures this may not convey the correct meaning.
• Check foods and produce: references to food items must be familiar to younger Indigenous Australian women.
• Review local customs and practices: in many cultures, for example, it is common for women to eat certain foods or non-foods during pregnancy; senior women will need to reveal local practices and beliefs and adapt the messages accordingly (MAMA 2013b).
Testing Messages
• Messages will be tested on pregnant Indigenous Australian women aged 16-30, as to whether they like the wording and ‘tone’ of the messages. They will be asked to pick from a set of three, the message they like the best.
• It allows the observation of how the women reacts to the messages.
• Again, women are not required to speak about women’s business.
Testing Messages
• Messages will be tested on pregnant Indigenous Australian women aged 16-30, as to whether they like the wording and ‘tone’ of the messages. They will be asked to pick from a set of three, the message they like the best.
• It allows the observation of how the women reacts to the messages.
• Again, women are not required to speak about women’s business.
Testing Messages
• Messages will be tested on pregnant Indigenous Australian women aged 16-30, as to whether they like the wording and ‘tone’ of the messages. They will be asked to pick from a set of three, the message they like the best.
• It allows the observation of how the women reacts to the messages.
• Again, women are not required to speak about women’s business.
Further Research• It is at the completion of this project that the SMS are ready
for use in clinical trials. Yet, even at this stage, positive behavior change is not guaranteed, the messages have merely been developed to a point where they have the maximum possibility of success.
• Field studies, such as those used in HCI are recommended for testing technology systems designed for health behavior change, even short studies that contain a significant qualitative component uncover bugs in the system that can go undetected, even in lab-based usability testing (Rogers et al. 2007).
• Only after the system has matured, Random Controlled Trials (RCTs) become necessary to demonstrate that the new technology is effective.
Further Research• It is at the completion of this project that the SMS are ready
for use in clinical trials. Yet, even at this stage, positive behavior change is not guaranteed, the messages have merely been developed to a point where they have the maximum possibility of success.
• Field studies, such as those used in HCI are recommended for testing technology systems designed for health behavior change, even short studies that contain a significant qualitative component uncover bugs in the system that can go undetected, even in lab-based usability testing (Rogers et al. 2007).
• Only after the system has matured, Random Controlled Trials (RCTs) become necessary to demonstrate that the new technology is effective.
Further Research• It is at the completion of this project that the SMS are ready
for use in clinical trials. Yet, even at this stage, positive behavior change is not guaranteed, the messages have merely been developed to a point where they have the maximum possibility of success.
• Field studies, such as those used in HCI are recommended for testing technology systems designed for health behavior change, even short studies that contain a significant qualitative component uncover bugs in the system that can go undetected, even in lab-based usability testing (Rogers et al. 2007).
• Only after the system has matured, Random Controlled Trials (RCTs) become necessary to demonstrate that the new technology is effective.
Thanks
Adapting Healthcare Messages For Pregnant Indigenous Australian
Women
By Reece George
Question Time
• If I don’t have time to answer your question, please feel free to email me at:
• This presentation is available for download at:
http://reecegeorge.com