brandwonden kinderen azo v3 · kinderen met brandwonden ... anaesthesiology intensive therapy...
TRANSCRIPT
KinderenmetbrandwondenAcuteopvangenintensivecaremanagement
JorisLemson
Intensivecarekinderen
(Potentiële)belangenverstrengeling Geen
Voorbijeenkomstmogelijkrelevanterelatiesmetbedrijven
•Geen
•Sponsoringofonderzoeksgeld•Honorariumofandere(financiële)vergoedingen•Aandeelhouder•Andererelatie
•Geen•Geen•Geen•Geen
DisclosurebelangenverstrengelingvoordesprekersvandeAZOscholingsavond
Ann surg 1947;126:1010-1045
Ann N Y Acad Sci 1968;150:874-894

InflammaGon
Sepsis Surgery
Myocardialdysfunc3onCapillaryleakageVasodila3onFeverAutonomicdysregula3on
youngerchildrenmoresuscepBve?EurJofCardio-thoracicSurg1997;12:862–868
PediatrCritCareMed2003;4:299–304CardiovascularResearch2007;73:26–36
CritCareMed2007;35:1599–1608
InflammationTraumaBurns

• Systemic inflammation (> 15%) • peak effect at aprox. 24 hours • high TBSA => long lasting inflammation • capillary leak
• edema (+ overzealous fluids => abdominal compartment syndrome)
• Circulating catecholamines • Loss of skin => loss of proteins and fluids • Loss of temperature control • Hyper-metabolic response • Colonisation en infections • Muscle weakness • . . . . .
Pathophysiology of severe burns
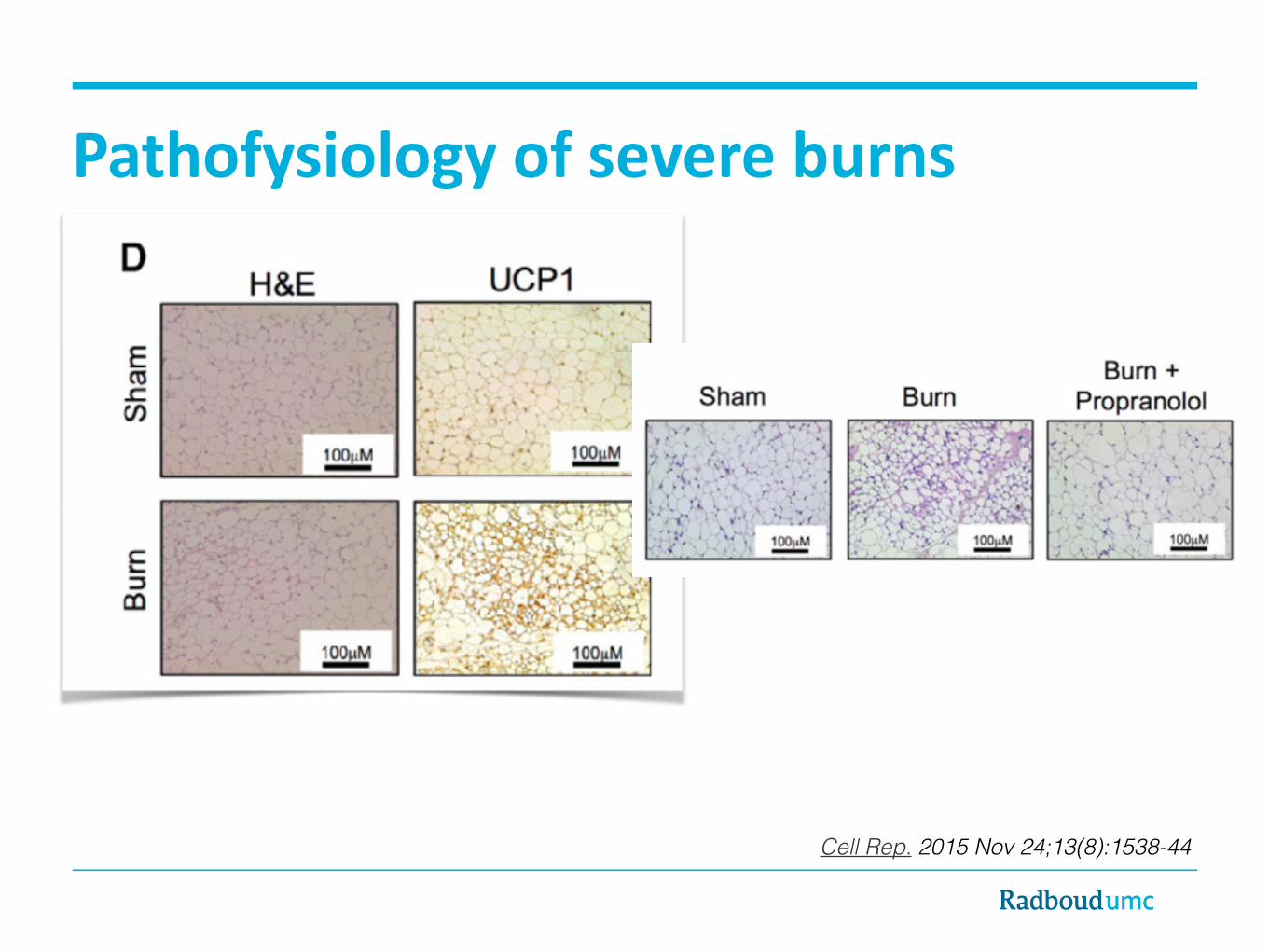
Pathofysiologyofsevereburns
Cell Rep. 2015 Nov 24;13(8):1538-44

• Consider mechanisme (blast, electrocution, inhalation trauma, etc)
• ABCDEFG • Cooling (be aware of hypothermia) • iv / io access • Pain and anxiety control (consider sedation+intubation) • Fluids • CO en cyanide intox, tetanus etc • Woundcare • Determine burn surface • . . . .
First treatment
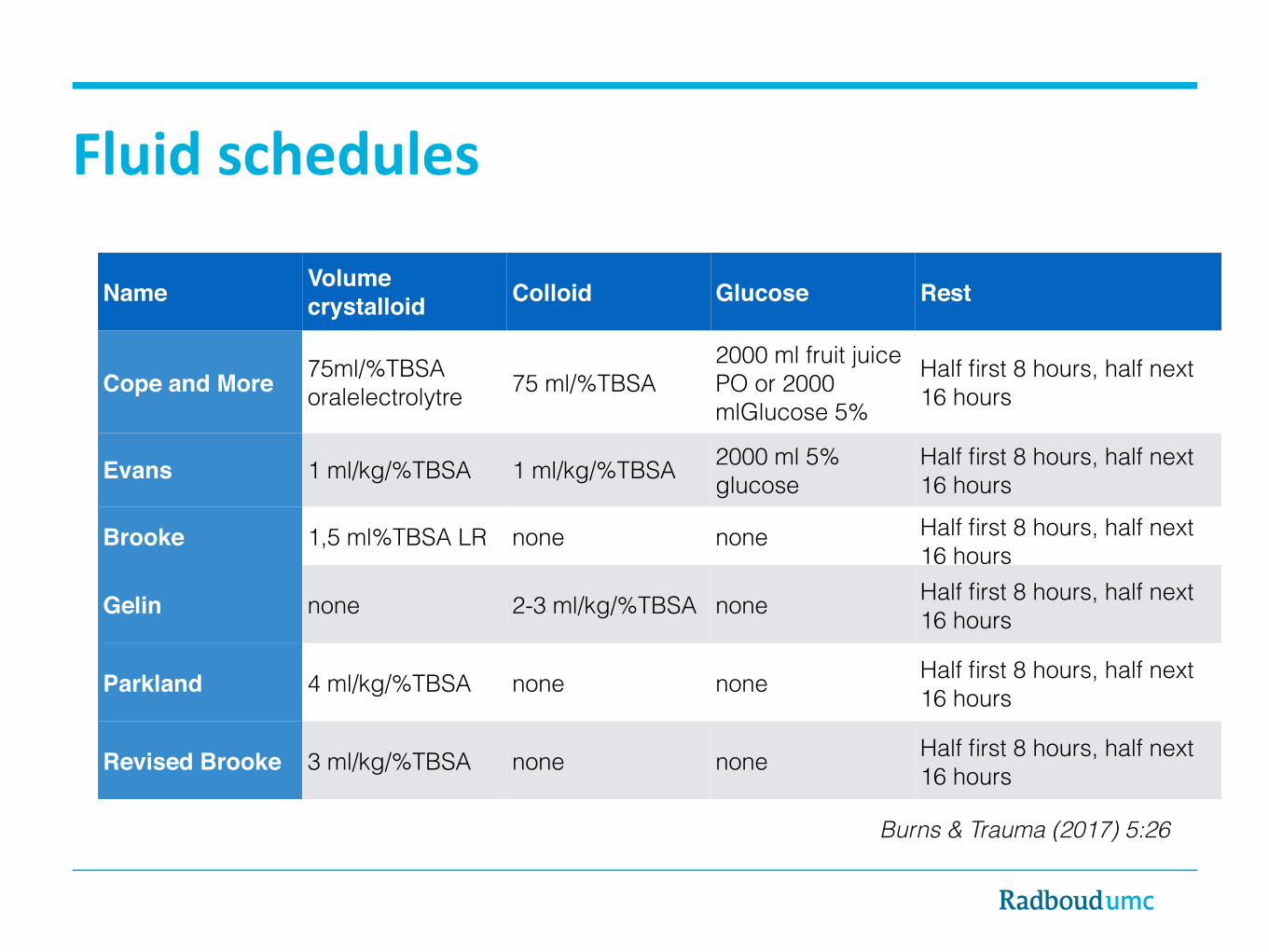
Name Volume crystalloid Colloid Glucose Rest
Cope and More 75ml/%TBSA oralelectrolytre 75 ml/%TBSA
2000 ml fruit juice PO or 2000 mlGlucose 5%
Half first 8 hours, half next 16 hours
Evans 1 ml/kg/%TBSA 1 ml/kg/%TBSA 2000 ml 5% glucose
Half first 8 hours, half next 16 hours
Brooke 1,5 ml%TBSA LR none none Half first 8 hours, half next 16 hours
Gelin none 2-3 ml/kg/%TBSA none Half first 8 hours, half next 16 hours
Parkland 4 ml/kg/%TBSA none none Half first 8 hours, half next 16 hours
Revised Brooke 3 ml/kg/%TBSA none none Half first 8 hours, half next 16 hours
Burns & Trauma (2017) 5:26
Fluidschedules

Fluidcreep
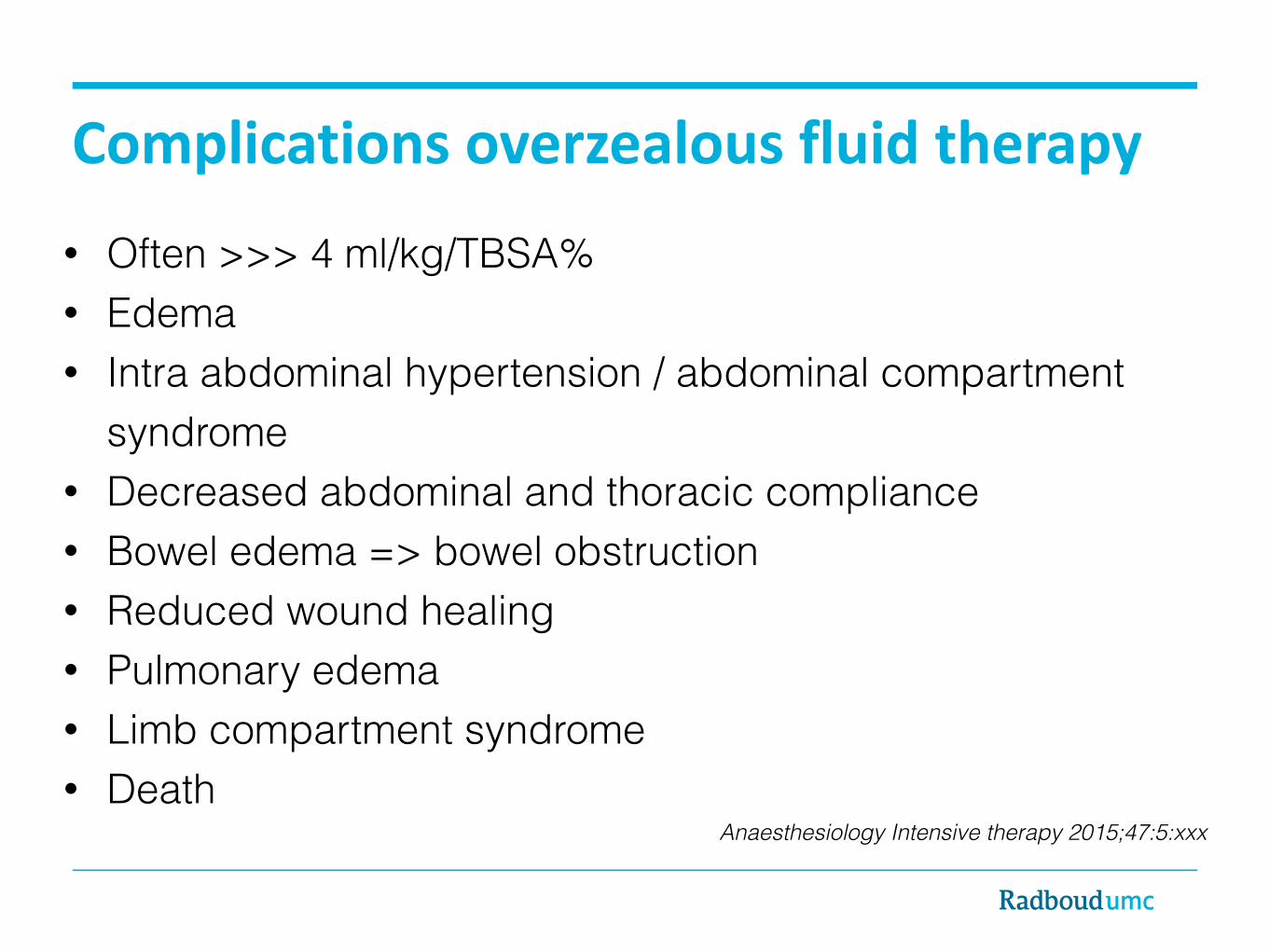
Anaesthesiology Intensive therapy 2015;47:5:xxx
Complicationsoverzealousfluidtherapy• Often >>> 4 ml/kg/TBSA% • Edema • Intra abdominal hypertension / abdominal compartment
syndrome • Decreased abdominal and thoracic compliance • Bowel edema => bowel obstruction • Reduced wound healing • Pulmonary edema • Limb compartment syndrome • Death
Cri3calCare2011,15:R118
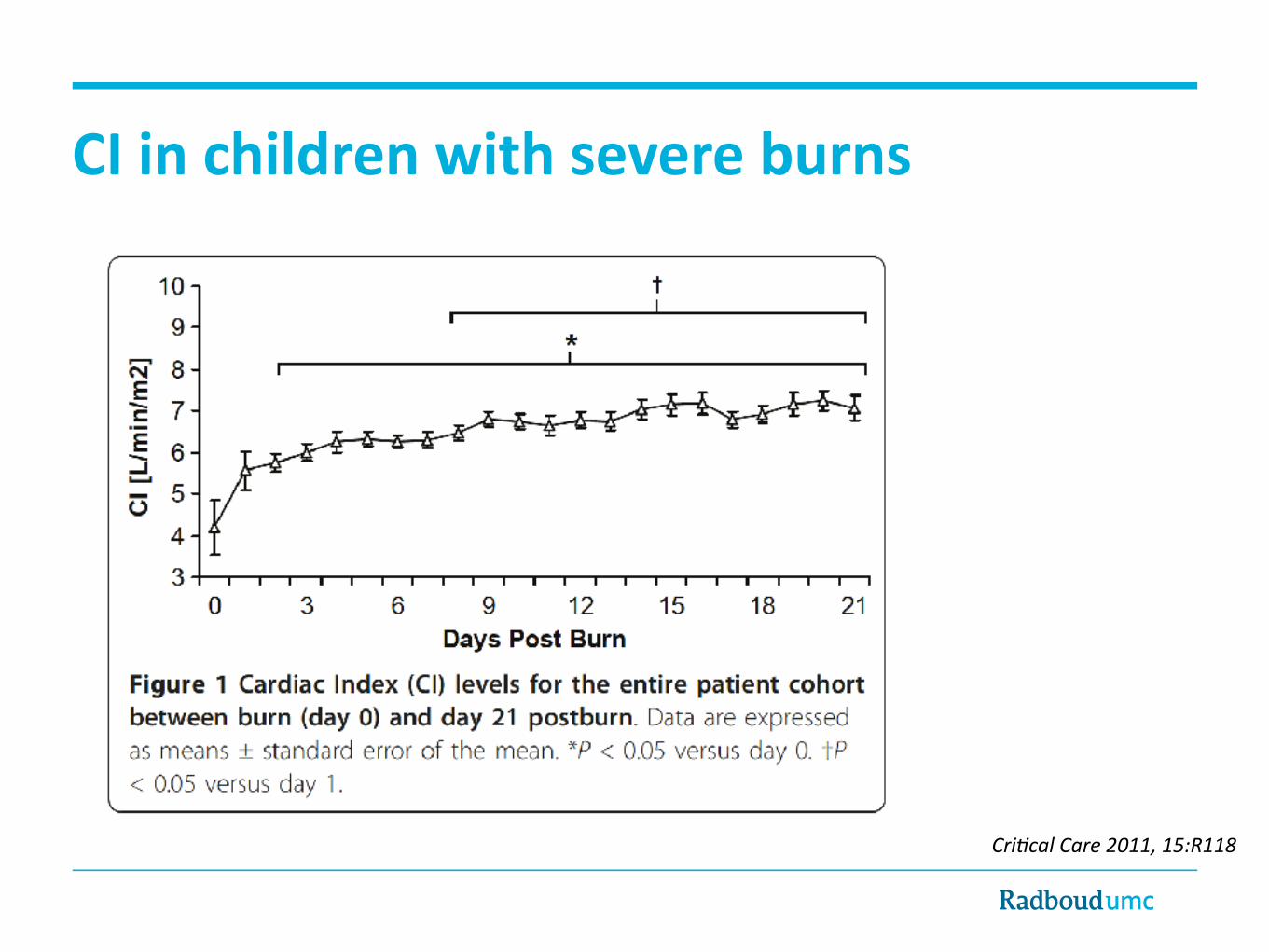
Cri3calCare2011,15:R118
CIinchildrenwithsevereburns

Cri3calCare2011,15:R118
EVLWIinchildrenwithsevereburns
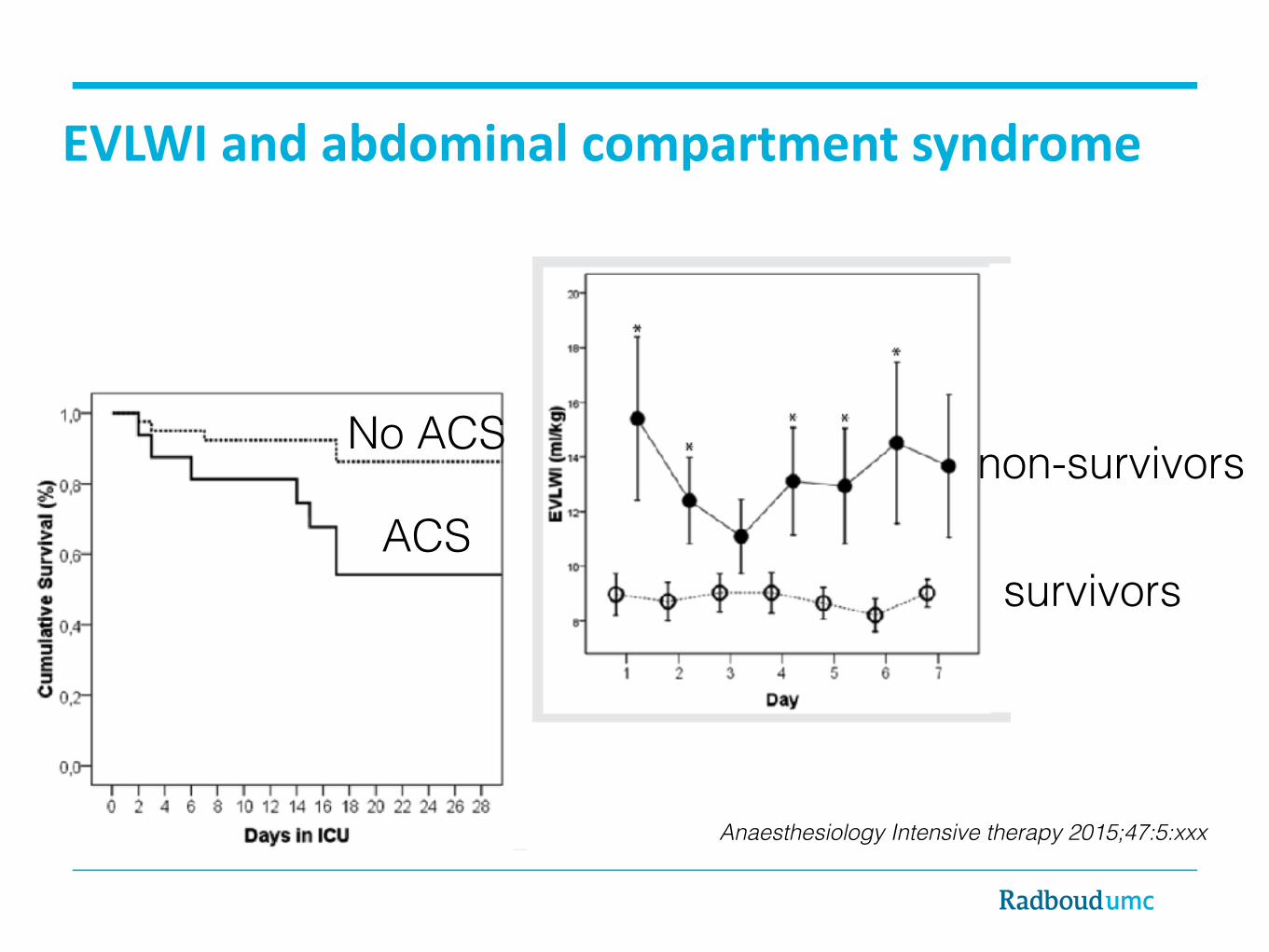
Anaesthesiology Intensive therapy 2015;47:5:xxx
ACS
No ACS
survivors
non-survivors
EVLWIandabdominalcompartmentsyndrome
Anaesthesiology Intensive therapy 2015;47:5:xxx
Monitoring• CVP, urinary output, blood pressure, HR
=> all unreliable
• Advanced monitoring (echo, PiCCO etc) => Efficiency unknown but useful info
• Recent knowledge => Try to maintain low CVP with adequate CO/MAP
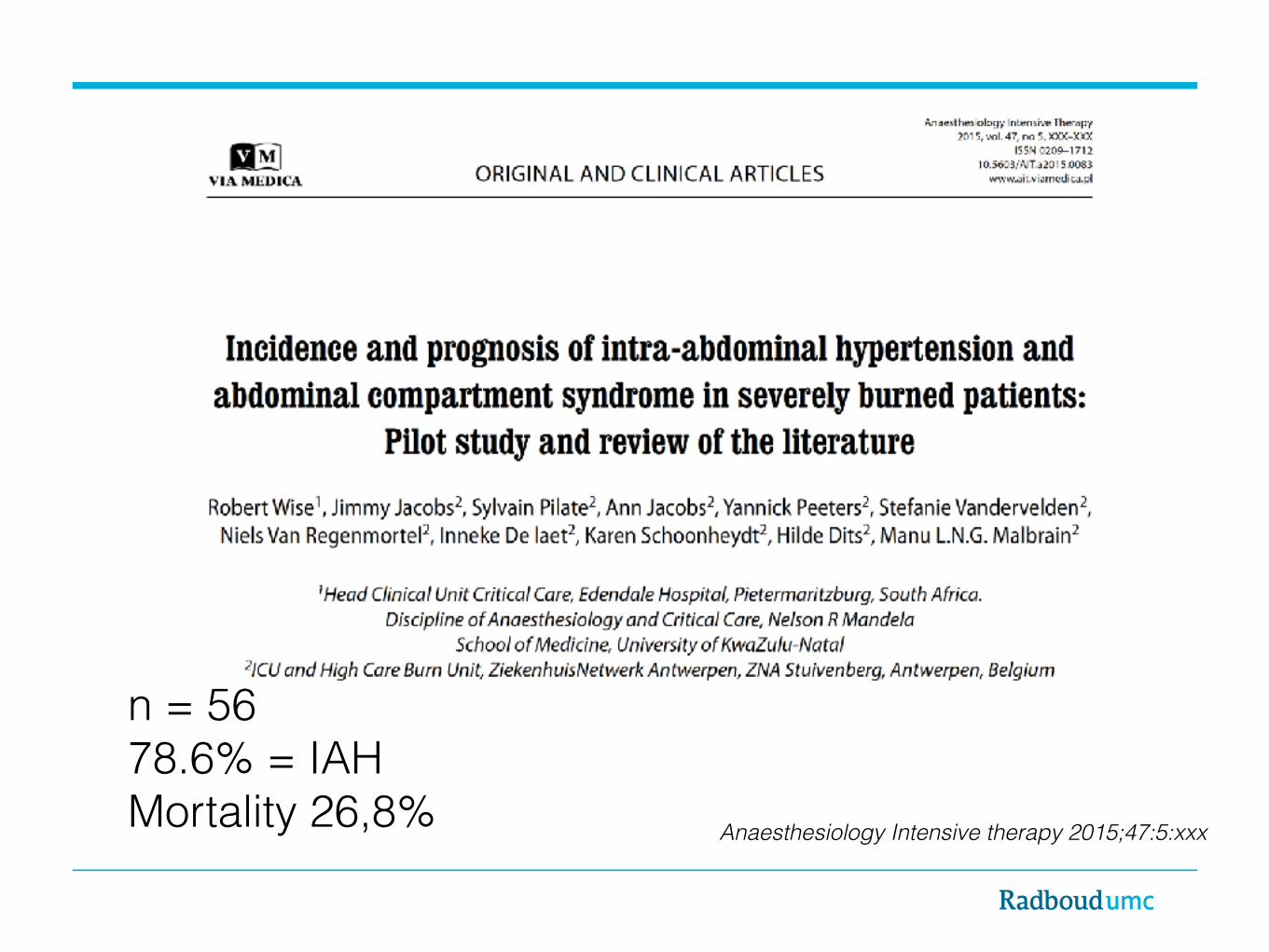
Anaesthesiology Intensive therapy 2015;47:5:xxx
n = 56 78.6% = IAH Mortality 26,8%
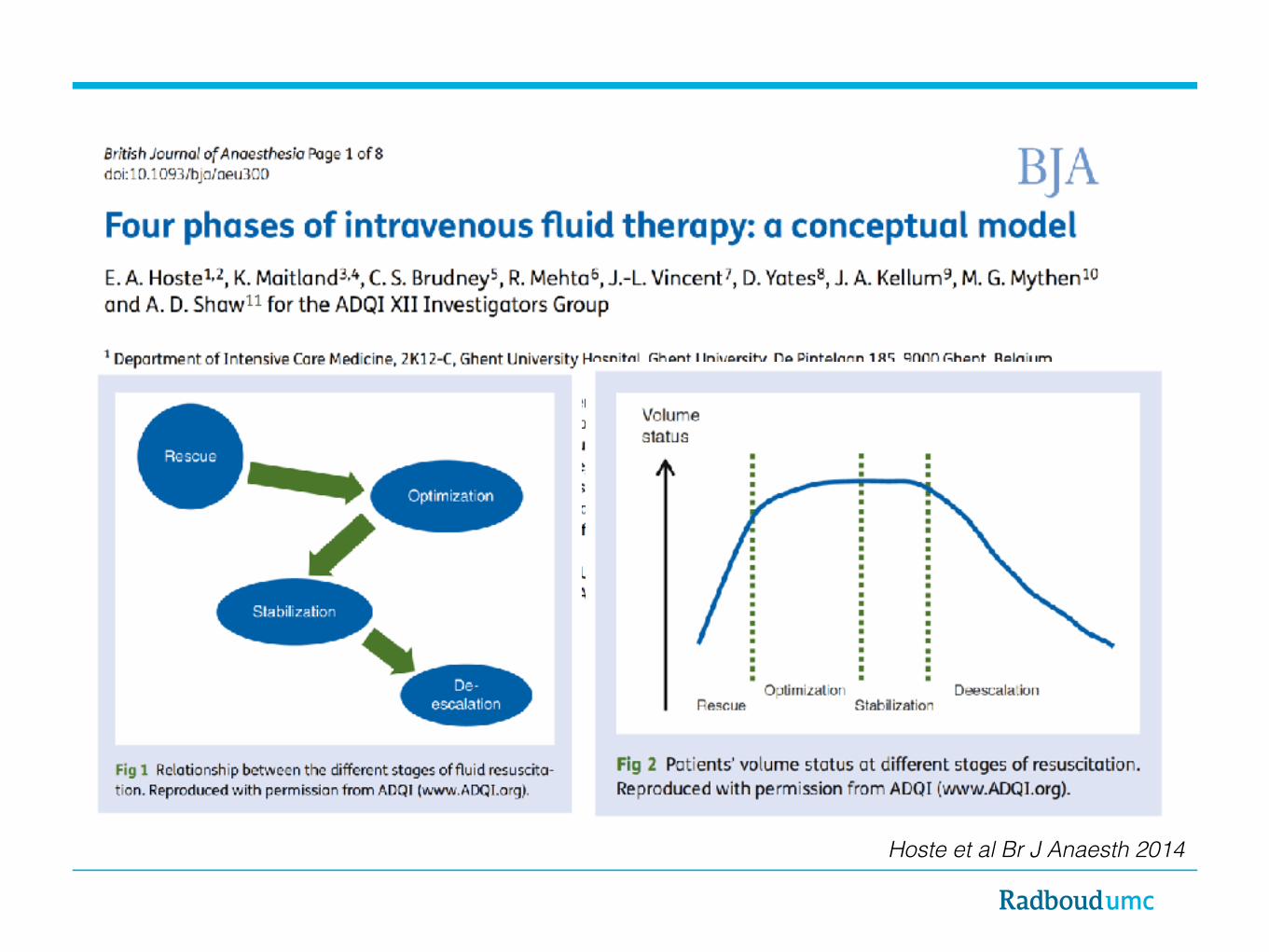
Hoste et al Br J Anaesth 2014
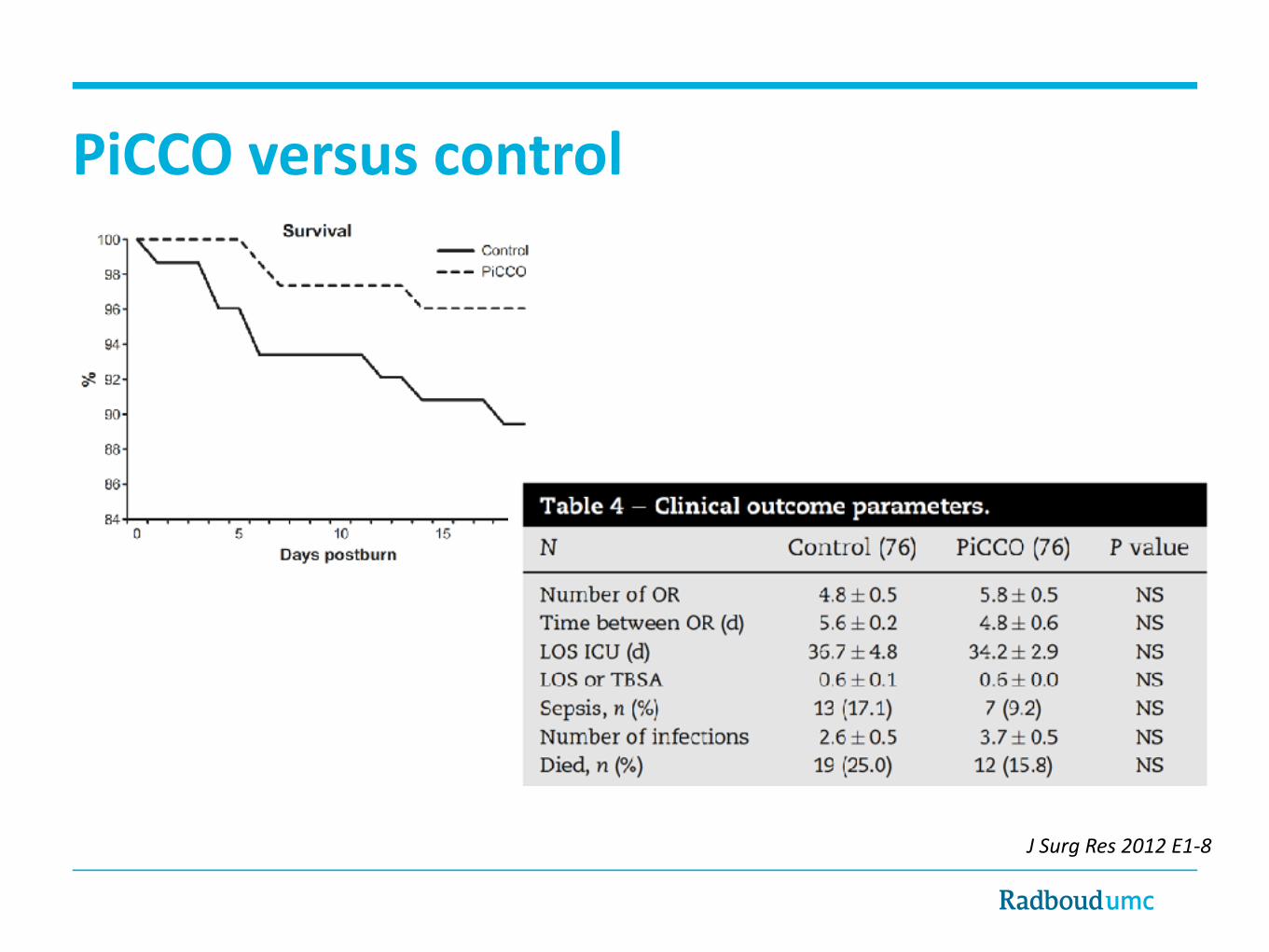
JSurgRes2012E1-8
• Children > 30% burns • Age 8 (SD 0,6) • 76 treated conventionally • 76 monitored with PiCCO • No RCT!
JSurgRes2012E1-8
PiCCOversuscontrol
Non-surgicalmanagement• Early aggressive fluid therapy when necessary • PICU management with careful fluid strategy
• No standard formula after emergency care • MAP, HR, urine production, CVP as usual • Advanced hemodynamic monitoring (PiCCO) • Monitor abdominal pressure • Monitor energy expenditure • Laboratory testing • Vasoactive drugs when necessary • Propranolol?????

Soussi et al. Ann. Intensive Care (2016) 6:87
• Lower HD variables have predictive value, fluids not • Target CO/MAP instead of ml/kg
World Journal of Emergency Surgery (2017) 12:11
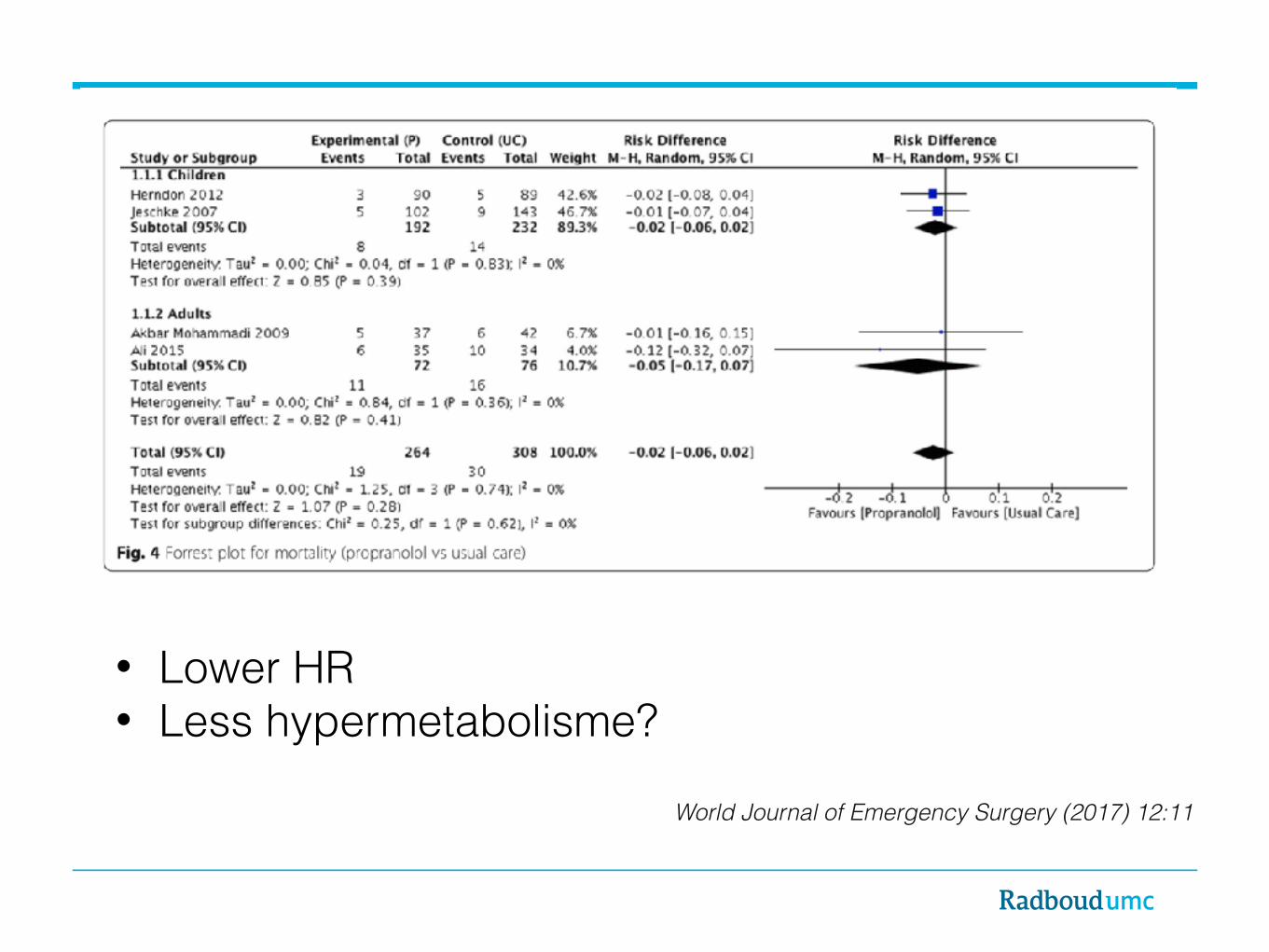
World Journal of Emergency Surgery (2017) 12:11
• Lower HR • Less hypermetabolisme?
Questions