case presentation:-
DESCRIPTION
بسم الله الرحمن الرحيم وزارة الدفاع رئاسة الأركان المشتركة الادارة العامة للخدمات الطبية قسم العناية المكثفة. Case Presentation:-. Prepared by : Dr.Altayeb M.Altayeb Abdalaziz ICU – Resident Supervised by : Dr.Kamal Osman Mergani Consultant Intensivist. - PowerPoint PPT PresentationTRANSCRIPT

الرحيم الرحمن الله بسمالدفاع وزارة
المشتركة األركان رئاسةالطبية للخدمات العامة االدارة
المكثفة العناية قسم

Prepared by :
Dr.Altayeb M.Altayeb Abdalaziz ICU – Resident
Supervised by :
Dr.Kamal Osman Mergani Consultant Intensivist
Mss. S.A.A.M is a 75 yrs old female who is known to be Hypertensive for 5 yrs on regular treatment, not known to be diabetic, referred to our department as a case of severe sepsis due to hospital acquired pneumonia.
She was admitted on 10th.0ct.2012 & her examination on admission was as follow:
Vital Signs
GCS: 15/15, B.P: 110/60 , PR: 120/min , RR:22/min, Temp.:38C
CNS: Unremarkable. CVS: Unremarkable
Respiratory System : Fine crepes bilaterally
Abdominal & Renal system : Unremarkable
What To Do NEXT ?
1. Patient Received (1)L of Normal Saline.
2. Blood sent for Investigations(CBC,RFTS).
3. Patient started antibiotics(Meropenem1gTDS)
4. Observation of Vital signs & urine output hourly.
General: Unwell , BP:130/80 , PR: 100/min , RR:20/min, Temp. 37.6 C , U.O.P : Adequate at (0.5-1)ml/kg/hr
Chest: Fine Crepes bilaterally
CNS, CVS, Abdomen —> Unremarkable
Quartz
MazenK
9
2
3
1
4
65
1112
7
8
10
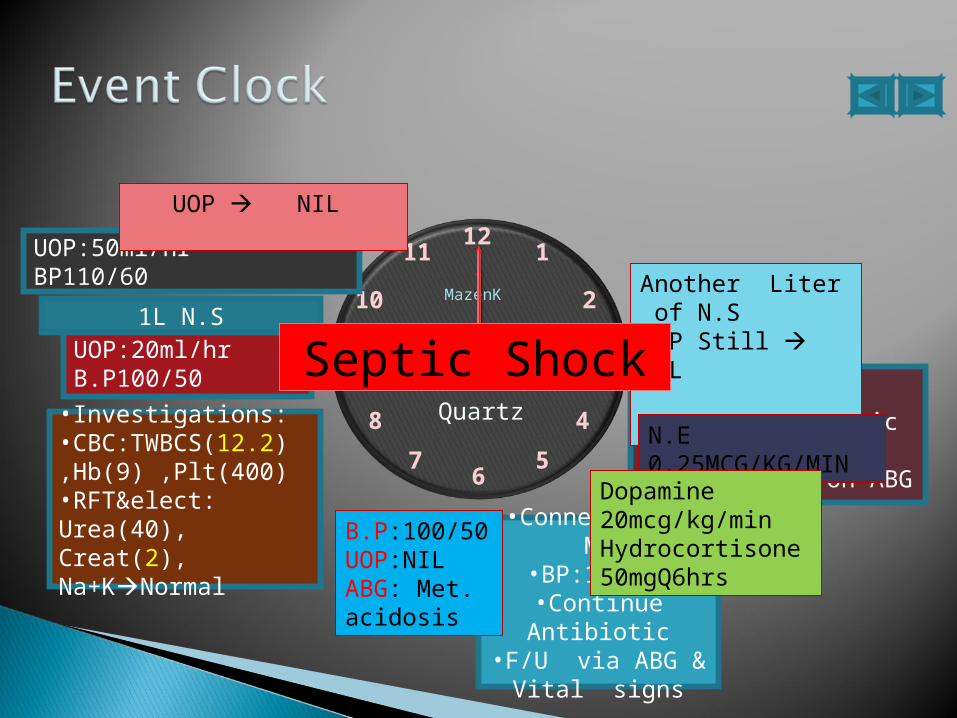
AT : 16:15Confused.Tachypnic + type II Resp.Failure on ABG
•Connected To MV•BP:110/60•Continue Antibiotic
•F/U via ABG & Vital signs
•Investigations: •CBC:TWBCS(12.2) ,Hb(9) ,Plt(400)•RFT&elect: Urea(40), Creat(2), Na+KNormal
UOP:20ml/hrB.P100/50
1L N.S
UOP:50ml/hrBP110/60
UOP NIL
Another Liter of N.SUOP Still NIL B.P:100/50(55)
N.E 0.25MCG/KG/MIN
Dopamine 20mcg/kg/minHydrocortisone 50mgQ6hrs
B.P:100/50UOP:NILABG: Met. acidosis
Septic Shock
What to Do Next ?
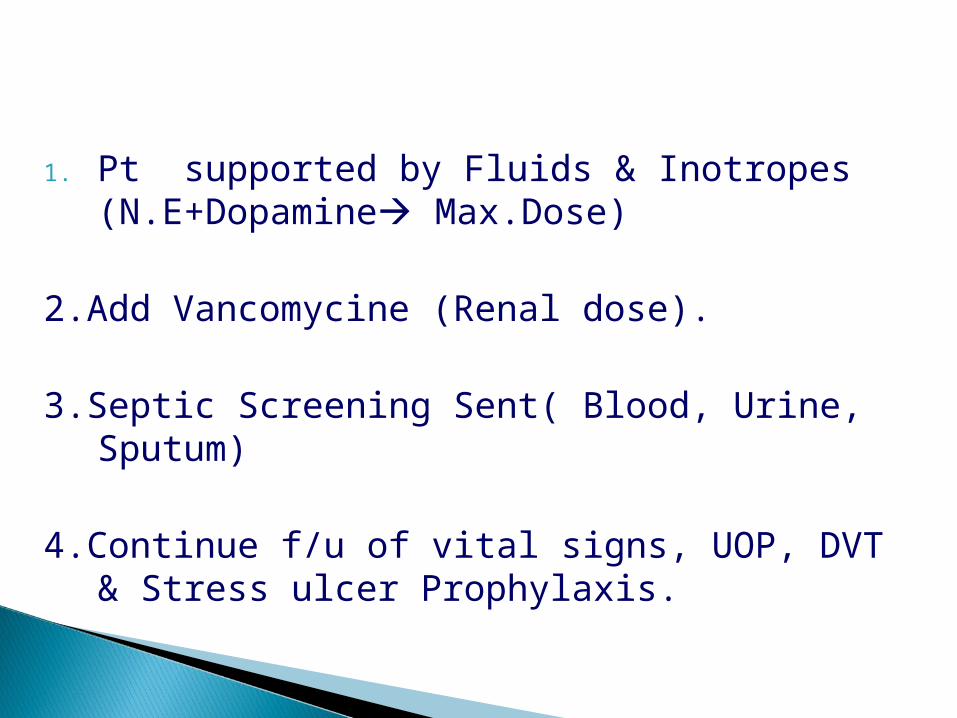
1. Pt supported by Fluids & Inotropes (N.E+Dopamine Max.Dose)
2.Add Vancomycine (Renal dose).
3.Septic Screening Sent( Blood, Urine, Sputum)
4.Continue f/u of vital signs, UOP, DVT & Stress ulcer Prophylaxis.
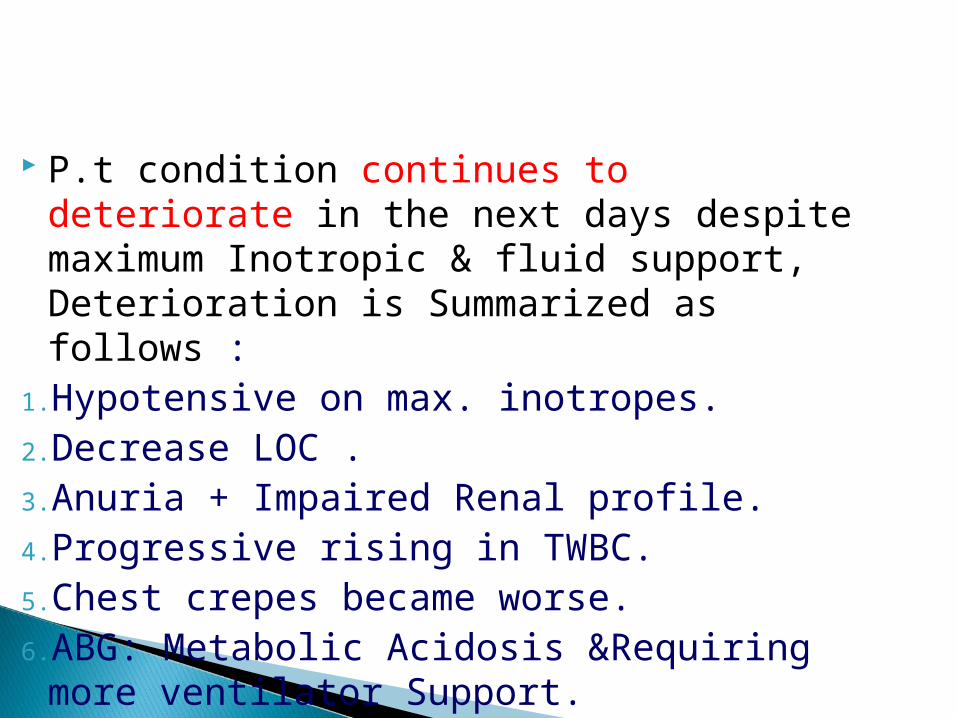
P.t condition continues to deteriorate in the next days despite maximum Inotropic & fluid support, Deterioration is Summarized as follows :
1.Hypotensive on max. inotropes.2.Decrease LOC .3.Anuria + Impaired Renal profile.4.Progressive rising in TWBC.5.Chest crepes became worse.6.ABG: Metabolic Acidosis &Requiring more
ventilator Support.
A few observation and much reasoningleads to error, many observations andlittle reasoning to truth Alexis Carrel (1873-1944)
Ketoconazole is added at 15th.10.012
Patient condition continues to deteriorate clinically and investigation wise as follows:
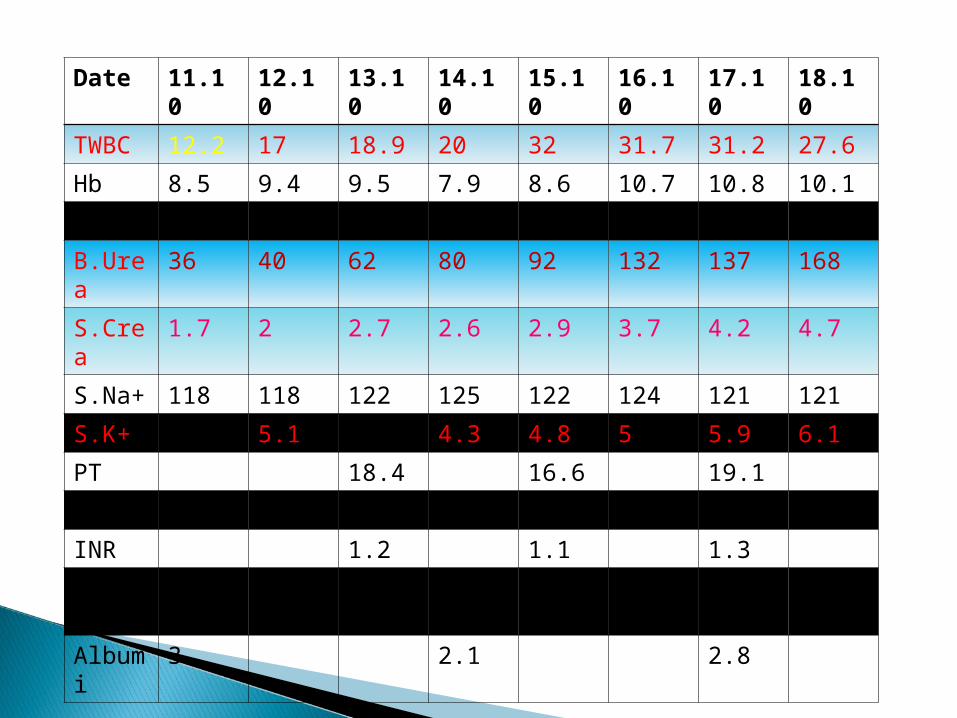
Date 11.10
12.10
13.10
14.10
15.10
16.10
17.10
18.10
TWBC 12.2 17 18.9 20 32 31.7 31.2 27.6
Hb 8.5 9.4 9.5 7.9 8.6 10.7 10.8 10.1
PLt 341 448 393 270 245 227 178 149
B.Urea
36 40 62 80 92 132 137 168
S.Crea
1.7 2 2.7 2.6 2.9 3.7 4.2 4.7
S.Na+
118 118 122 125 122 124 121 121
S.K+ 3.8 5.1 4.9 4.3 4.8 5 5.9 6.1
PT 18.4 16.6 19.1
PTT 44.6 37 68
INR 1.2 1.1 1.3
T.Prot 6.5 5.5 6.5
Albumi
3 2.1 2.8

11.10
12.10
13.10
14.10
15.10
16.10
17.10
18.10
PH 7.15 7.27 7.21 7.17 7.08 7.05 7.02 6.90
PCO2 46.7 32.7 37.3 36.8 38 45 48 61
PO2 93 242 84 182 94 80 59 130
HCO3 16.8 15.3 15.1 13.7 11.4 12.8 12.6 12
SaO2 94% 99% 93% 99% 93% 89% 76% 96%
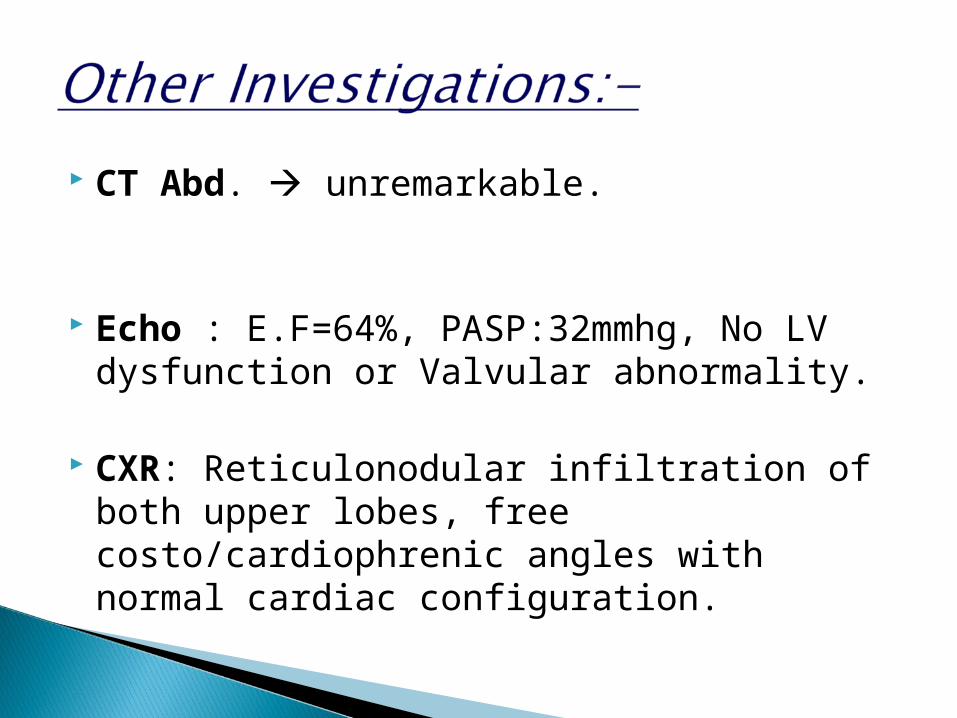
CT Abd. unremarkable.
Echo : E.F=64%, PASP:32mmhg, No LV dysfunction or Valvular abnormality.
CXR: Reticulonodular infiltration of both upper lobes, free costo/cardiophrenic angles with normal cardiac configuration.
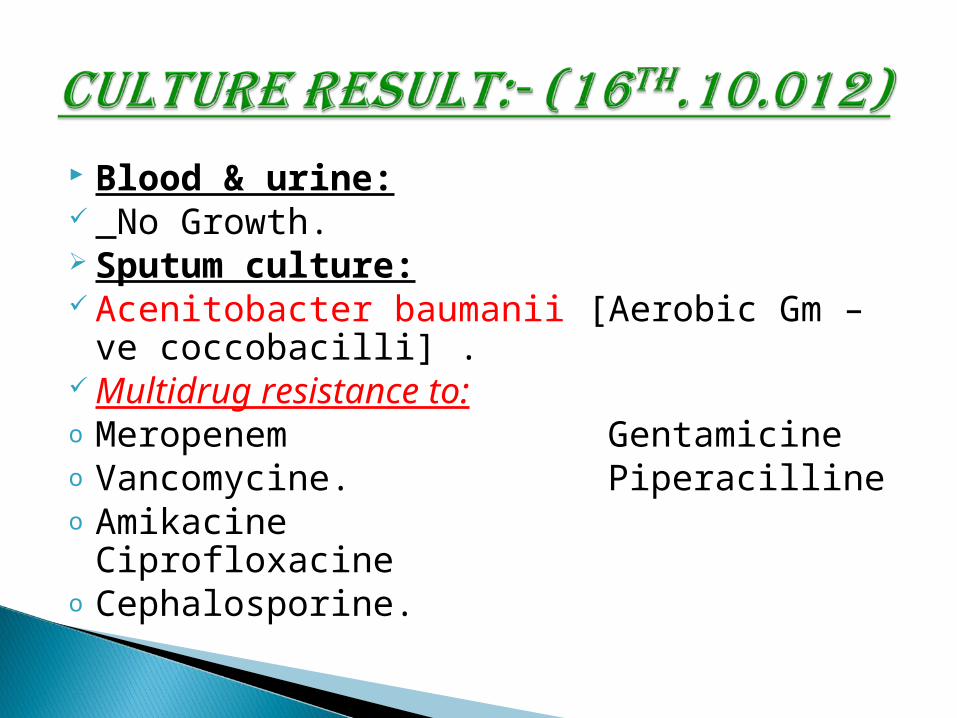
Blood & urine: No Growth. Sputum culture: Acenitobacter baumanii [Aerobic Gm –ve
coccobacilli] . Multidrug resistance to:o Meropenem Gentamicineo Vancomycine. Piperacilline o Amikacine Ciprofloxacineo Cephalosporine.


1. Stop All antibiotics.
2. Put patient in a contact isolation
3. Continue with the other supportive therapy.
4. Search for : (Colistine OR Tigicycline).
=Unfortunately BOTH are not available in Sudan =
0n 18th.Oct.O12 patient arrested at 7:00PM , didn’t respond to CPR and death declared at 7:30pm

Faculty of medicine U of G in Autumn ( wadmadani )SUDAN
“We are born to see, but haveto train ourselves to observe”
Gram negative Coccobacillus . Strictly Aerobic, Non motile. Water and soil.
Associated with antibiotic resistance.
Not part of normal human flora
Infections and outbreaks ◦ Intensive care unit and healthcare settings ◦ Compromised immune systems and risk◦ Colonized and infected patients as point
sources
Since Operation Iraqi Freedom began in 2003, more than 700 US soldiers have been infected or colonized with Acinetobacter baumannii. A significant number of additional cases have been found in the Canadian and British armed forces, and among wounded Iraqi civilians.
hospitalization significant co-
morbidity mechanical
ventilation cardio respiratory
failure previous infection antimicrobial therapy CVP lines urinary catheters
Acinetobacter infections are uncommon and occur almost exclusively in hospitalized patients
• “A doctor is a person
• who kills your ills • with pills, & then • kills you with his • bills”• Anonymous

"It is nice to have money and the things that money can buy, but it's important to make sure you haven't lost the things money can't buy."
George Lorimer1867-1937, Editor of "Saturday Evening Post"
Infection or colonization with Acinetobacter is usually diagnosed by clinical culture of blood, sputum, urine, wound, sterile body fluid, etc. Microbiologic cultures can be processed by standard methods on routine media.

Oxidase negative (opposite to Neisseria spp. or Moraxella spp.)
Haemolytic Indole negative.
Catalase positive.
Nonmotile Strictly aerobic
Gram negative coccobacillus
Highly antibiotic resistant
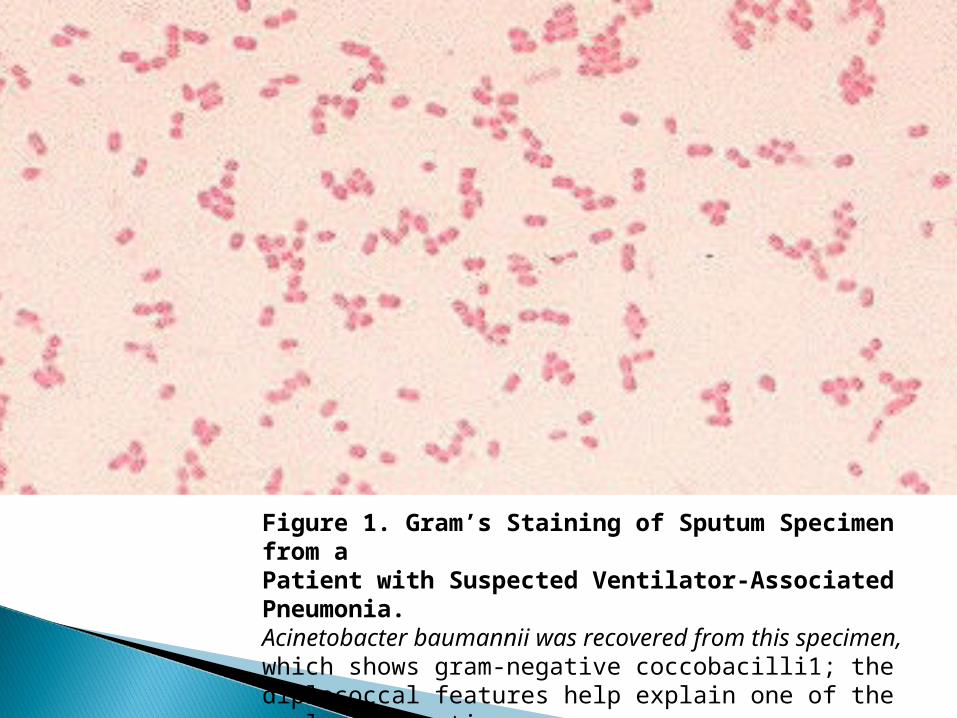
Figure 1. Gram’s Staining of Sputum Specimen from aPatient with Suspected Ventilator-Associated Pneumonia.Acinetobacter baumannii was recovered from this specimen,which shows gram-negative coccobacilli1; thediplococcal features help explain one of the early designationsof acinetobacter as neisseria.
Villegas M, Hartstein A. Infect Control Hosp Epidemiol. 2003;24:284-295
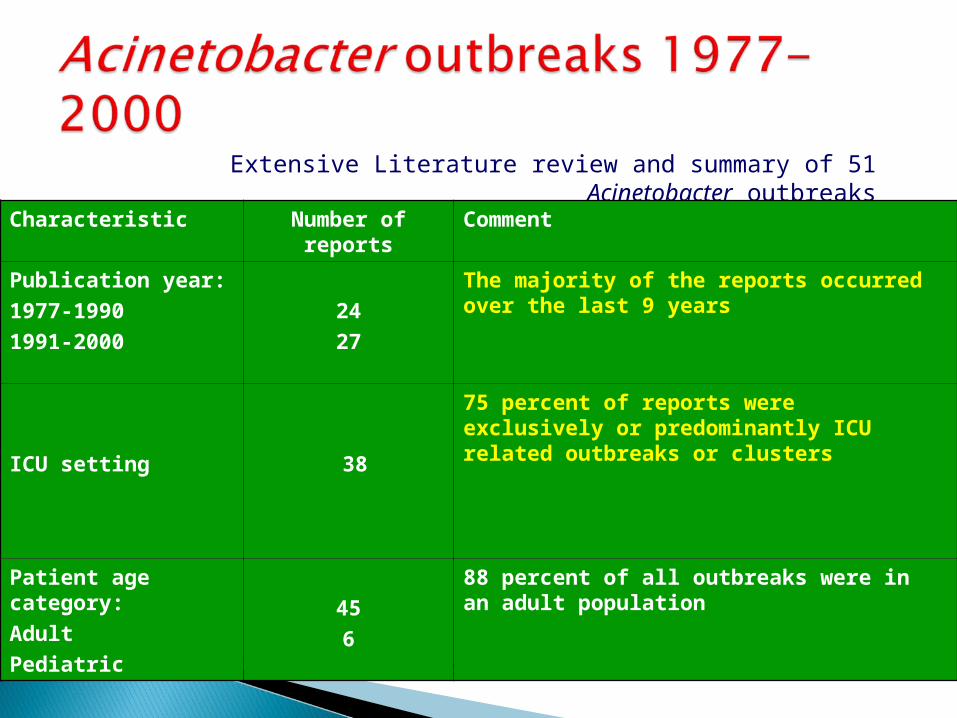
Extensive Literature review and summary of 51 Acinetobacter outbreaks
Characteristic Number of reports Comment
Publication year:
1977-1990
1991-2000
24
27
The majority of the reports occurred over the last 9 years
ICU setting 38
75 percent of reports were exclusively or predominantly ICU related outbreaks or clusters
Patient age category:
Adult
Pediatric
45
6
88 percent of all outbreaks were in an adult population
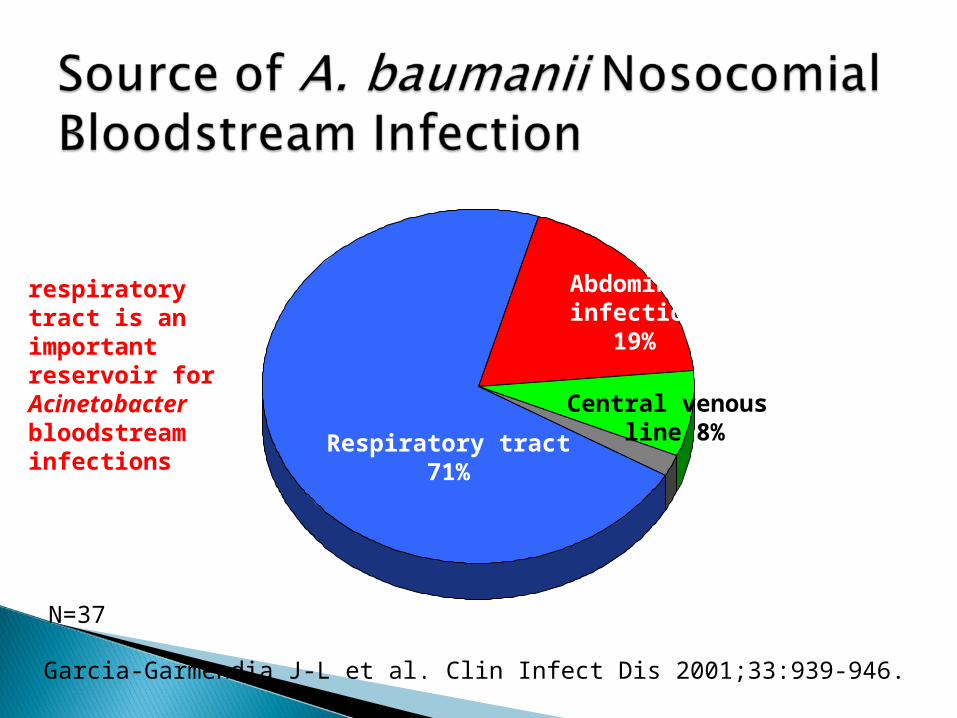
Respiratory tract71%
Central venous line 8%
Abdominal infection
19%
N=37
Garcia-Garmendia J-L et al. Clin Infect Dis 2001;33:939-946.
respiratory tract is an important reservoir for Acinetobacter bloodstream infections
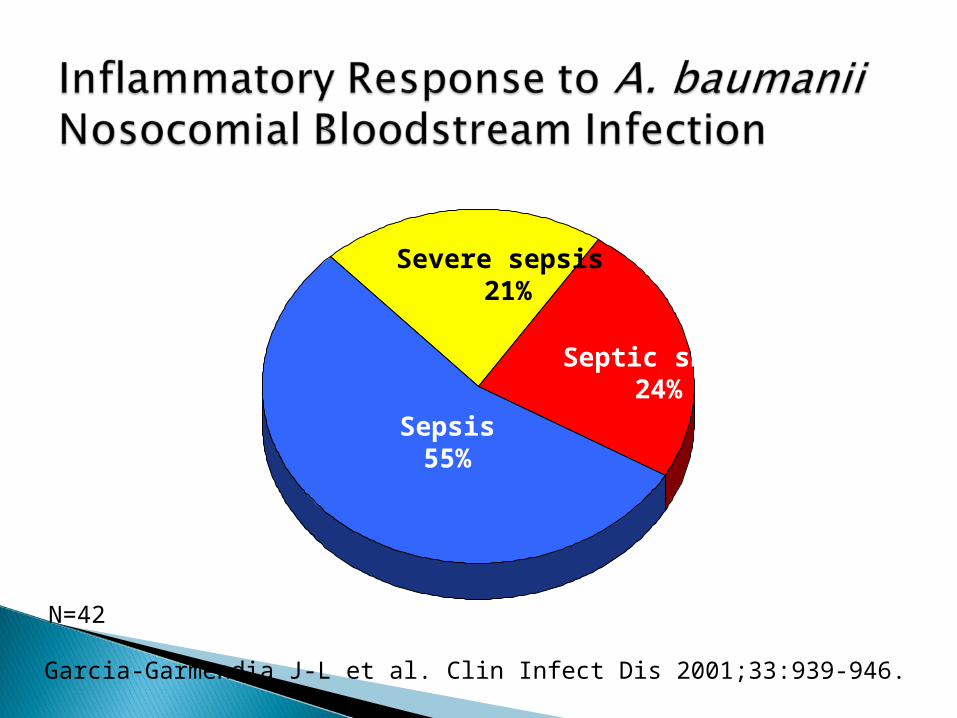
Sepsis55%
Severe sepsis 21%
Septic shock24%
N=42
Garcia-Garmendia J-L et al. Clin Infect Dis 2001;33:939-946.

One of the biggest issues with treating Acinetobacter baumannii is that the bacterium is naturally resistant to a number of antibiotics, making it challenging to find a drug regimen which will effectively attack it in an infected patien
Quantitative and/or qualitative changes in outer membrane porins.
Altered penicillin-binding proteins.
Aminoglycosides-modifying enzymes. Broad-spectrum β-lactamases .
Efflux pumps .
Carbapenems (Imipenem and Meropenem) are the mainstay of treatment for antimicrobial-resistant gram-negative infections, though Carbapenems-resistant Acinetobacter is increasingly reported.
Resistance to the Carbapenems class of antibiotics makes multidrug-resistant Acinetobacter infections difficult, if not impossible, to treat.

Multidrug-resistant A. baumannii is a common problem in many hospitals in the US and Europe. First line treatment is with a Carbapenems antibiotic such as imipenem, but carbapenem resistance is increasingly common. Other treatment options include Colistin, tigecycline and Aminoglycosides.
Colistin and Polymyxin B have been used to treat highly resistant Acinetobacter infections. The choice of appropriate therapy is further complicated by the toxicity of colistin which is mainly renal. Acinetobacter isolates resistant to colistin and Polymyxin B have also been reported.
History◦ Used extensively worldwide in topical otic and
ophthalmic solutions for decades◦ Intravenous Colistin was initially used in Japan and in
Europe during the 1950s, and in the United States in the form of colistimethate sodium in 1959
◦ The intravenous formulations of colistin and
polymyxin B were gradually abandoned in most parts of the world in the early 1980s because of the reported high incidence of nephrotoxicity
◦ Colistin was mainly restricted during the past 2 decades for the treatment of lung infections due to multidrug-resistant (MDR), gram-negative bacteria in patients with cystic fibrosis
Numerous recent clinical studies have confirmed that colistin is an efficient antimicrobial agent against nosocomial infections, including bacteremia, ventilator-associated pneumonia, urinary tract infection, and meningitis due to MDR GNB, such as P. aeruginosa, A.baumannii, and K. pneumonia, with an acceptable safety profile. Whereas colistin is mainly administered i.v. incritically ill patients, it can be safely be administered by inhalation in patients with pneumonia/VAP or intrathecally in patients with meningitis due to MDR GNB.
Mechanism of action:◦Target:
Bacterial cell membrane( Bactericidal). Colistin binding with the bacterial membrane
occurs through electrostatic interactions between the cationic polypeptide (colistin) and
anionic lipopolysaccharide (LPS) molecules in the outer membrane of the gram-negative bacteria leads to a derangement of the cell membrane
The result of this is an increase in the permeability of the cell envelope, leakage of cell contents, and, subsequently, cell death.

Important pharmacokinetic parameters:
◦ Colistin sulfate and colistimethate sodium are not absorbed by the gastrointestinal tract with oral administration
◦ Primary route of excretion is through glomerular filtration
◦ Experimental studies have shown that colistin is tightly bound to membrane lipids of tissues,
including liver, lung, kidney, brain, heart, and muscles
◦ Concentration of colistin in the CSF is 25% of the serum concentration
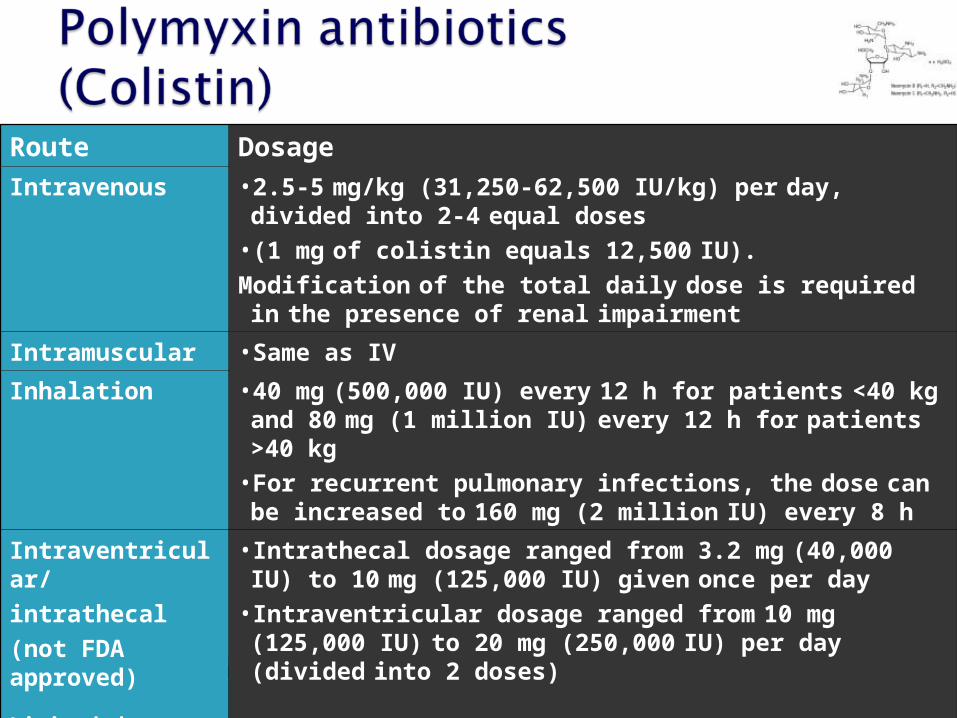
Route Dosage
Intravenous • 2.5-5 mg/kg (31,250-62,500 IU/kg) per day, divided into 2-4
equal doses
• (1 mg of colistin equals 12,500 IU).
Modification of the total daily dose is required in the presence of renal impairment
Intramuscular •Same as IV
Inhalation • 40 mg (500,000 IU) every 12 h for patients <40 kg and 80 mg (1 million IU) every 12 h for patients >40 kg
• For recurrent pulmonary infections, the dose can be increased to 160 mg (2 million IU) every 8 h
Intraventricular/
intrathecal
(not FDA approved)
Limited data based on case reports
• Intrathecal dosage ranged from 3.2 mg (40,000 IU) to 10 mg (125,000 IU) given once per day
• Intraventricular dosage ranged from 10 mg (125,000 IU) to 20 mg (250,000 IU) per day (divided into 2 doses)
Loading dose should be given as an IV infusion over 2 hours.
Maintenance dose should be given as IV infusion can be given over 30 minutes.
First maintenance dose should be given 24 hours after loading dose.
IM administration is not recommended.Half-life is 3-4 hours in patients with normal
renal function, and up to 2-3 days inpatients with renal impairment.

Nephrotoxicity•The majority of nephrotoxic events are reversible•1970’s- incidence of nephrotoxicity was 20.2%•More recent studies- incidence of nephrotoxicity ranged from 8%-18%.•Lower incidence of Nephrotoxicity at present:
–Greater supportive treatment to critically ill patients–Close monitoring of renal function–Avoidance of co-administered nephrotoxic agents–Older formulations of Colistin contained a greater proportion of colistin sulfate (greater nephrotoxicity)


Acinetobacter rarely causes serious infection in otherwise healthy people and therefore poses minimal threat to healthcare workers or patients’ family members.
Pregnant healthcare workers are not at increased risk from this organism and can therefore care for patients infected or colonized with the organism.
Hand hygiene◦Use of alcohol-based hand sanitizers
Contact precautions ◦Gowns/gloves◦Sterilization and hand wash
Environmental decontamination
Prudent use of antibiotics
Early Recognition & Control of the source.
Sterilization of the equipments ( MV, Circuits… etc).
The organism is highly susceptible to antiseptic & disinfectants.
Hand wash ( Generally the hardest measure to implement) .
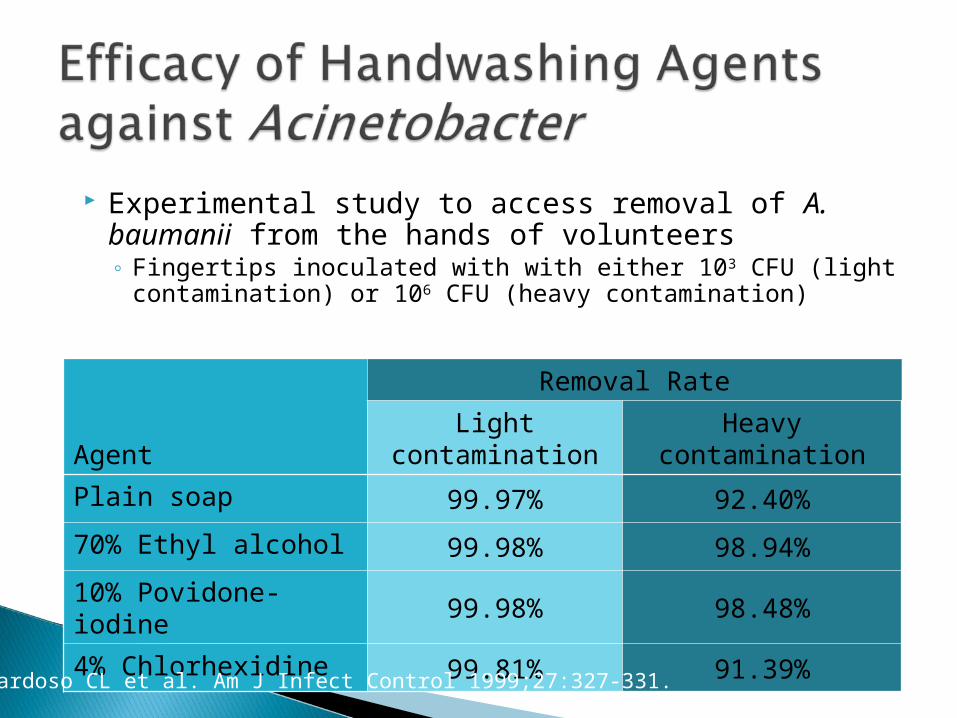
Experimental study to access removal of A. baumanii from the hands of volunteers◦ Fingertips inoculated with with either 103 CFU (light
contamination) or 106 CFU (heavy contamination)
Agent
Removal Rate
Light contamination Heavy contamination
Plain soap 99.97% 92.40%
70% Ethyl alcohol 99.98% 98.94%
10% Povidone-iodine 99.98% 98.48%
4% Chlorhexidine 99.81% 91.39%
Cardoso CL et al. Am J Infect Control 1999;27:327-331.

Although commonly found on the skin of healthy humans, Acinetobacter plays the role of an opportunistic pathogen in the critically ill patient
High level of antibiotic resistance makes it well suited as a pathogen in areas with high use of antibiotics (e.g., ICU setting)
Control requires good hand hygiene, barrier precautions & environmental decontamination◦ Alcohol-based products containing chlorhexidine
should be considered the hand hygiene agents of choice
