clinical efficacy and cognitive and neuropsychological effects of levetiracetam in epilepsy: an...
TRANSCRIPT

Epilepsy & Behavior 16 (2009) 468–474
Contents lists available at ScienceDirect
Epilepsy & Behavior
journal homepage: www.elsevier .com/locate /yebeh
Clinical efficacy and cognitive and neuropsychological effects of levetiracetamin epilepsy: An open-label multicenter study
Tony Wu a, Chih-Chuan Chen b, Ta-Cheng Chen c, Yuan-Fu Tseng d, Chen-Bang Chiang e, Chin-Chuan Hung f,Horng-Huei Liou b,g,*
a Department of Neurology, Chang-Gung Memorial University, Linkou, Taiwanb Department of Neurology, National Taiwan University Hospital, Taipei, Taiwanc Department of Neurology, Changhua Christian Hospital, Changhua, Taiwand Department of Neurology, Tzu-Chi General Hospital, Taipei, Taiwane Graduate Institute of Clinical Pharmacy, College of Medicine, National Taiwan University, Taiwanf Department of Pharmacy, College of Pharmacy, China Medical University, Taiwang Department of Pharmacology, College of Medicine, National Taiwan University, Taiwan
a r t i c l e i n f o a b s t r a c t
Article history:Received 20 May 2009Revised 6 August 2009Accepted 26 August 2009Available online 26 September 2009
Keywords:LevetiracetamCognitive functionNeuropsychological functionQuality of life
1525-5050/$ - see front matter � 2009 Published bydoi:10.1016/j.yebeh.2009.08.026
* Corresponding author. Address: Department of NCollege of Medicine, National Taiwan University, RooRoad, Taipei 100, Taiwan. Fax: +886 2 23915297.
E-mail address: [email protected] (H.-H. Liou).
The aim of this prospective, multicenter, open-label study was to investigate the efficacy of levetiracetam(LEV) and determine its effects on cognitive and neuropsychological function. Sixty-nine patients wereevaluated for effects of LEV on seizure control, cognitive (Mini-Mental State Examination [MMSE]) andneuropsychological (Symptom Checklist-90 Revised [SCL-90-R]) functions, and quality of life (Qualityof Life in Epilepsy—10 [QOLIE-10]) assessments at 3 and 12 months of follow-up. Thirty-nine percentof patients achieved seizure freedom, and 68% had a P50% seizure frequency reduction after 1 year ofLEV (1235.5 ± 392.7 mg/day). There were also significant improvements in mean MMSE score and inthe recall and language items of MMSE. There were modest improvements in interpersonal sensitivityand paranoid ideation scales of the SCL-90-R, and improvements in cognition and medication effect itemsof the QOLIE-10. The results demonstrate that LEV not only effectively reduces seizure frequency, but alsopossibly contributes to improvements in neuropsychological functions such as recall, language, interper-sonal sensitivity, and paranoid ideation.
� 2009 Published by Elsevier Inc.
1. Introduction
Levetiracetam [(S)-a-ethyl-2-oxo-1-pyrrolidine acetamide,Keppra, LEV] is a novel antiepileptic drug that is now widely usedas add-on therapy or monotherapy for partial and generalized to-nic–clonic seizures [1–5]. Three pivotal multicenter, double-blind,placebo-controlled trials of treatment of partial seizures have dem-onstrated its clinical efficacy and favorable safety profile [6–8].When used as add-on therapy, it can be as effective as or moreeffective than older antiepileptic drugs (AEDs) in controlling par-tial-onset seizures with or without generalization and in improv-ing neuropsychological and cognitive function outcomes [9]. Itmay also be equal in effectiveness to controlled-release carbamaz-epine when used as monotherapy for the initial treatment of pa-tients with partial or generalized tonic–clonic seizures [3].Depending on the dosage used and type of epilepsy treated, re-
Elsevier Inc.
eurology and Pharmacology,m 1141, No. 1, Sec. 1, Jan-Ai
sponder rates (patients with P50% reduction in seizure frequency)during LEV treatment are reported to be as high as 72% [2–4].
The mechanism of action of LEV differs from those of otherAEDs in that it binds specifically to a protein (synaptic vesicle pro-tein 2A) thought to regulate the synaptic vesicle exocytosis neces-sary for neurotransmitter release [3,5,6]. The pharmacokineticprofile of LEV also differs from those of other AEDs because it isnot metabolized by P450 enzymes in the liver, does not alter themetabolism of other AEDs, and is eliminated largely unchangedby the kidneys [10]. It has no known significant ethnic differencesin pharmacokinetics, and comparisons between Asian and Cauca-sian subjects reveal similar efficacy and tolerability profiles [11–14]. LEV treatment has been shown to have a positive effect onquality of life [15–17]. Although its adverse effects, like somno-lence/asthenia, dizziness, and coordination difficulties, are similarto those of other AEDs, some reports also record behavioral side ef-fects, such as irritability, agitation, and aggressive behavior, whichare similar to those reported for piracetam, the parent drug of LEV[17–20]. Negative short- and long-term side effects of LEV onmood, quality of life, and alertness are also reported [16,18].

T. Wu et al. / Epilepsy & Behavior 16 (2009) 468–474 469
This open-label, multicenter study investigated the clinical andpatient-perceived efficacy of LEV as an adjunct and as mono-therapy, as well as its effects on cognitive and neuropsychologicalfunction and quality of life. The goal was to clarify the role of LEV innormal clinical practice by recording its routine uses and overallefficacy in a heterogeneous patient cohort in which LEV mono-therapy or adjunctive therapy was individually tailored for specificpatient conditions and preferences.
2. Methods
2.1. Study design
A prospective, multicenter, open-label observational study wasconducted in four institutions in Taiwan from July 12, 2006 toDecember 25, 2007. The Ethical Practices Committees of NationalTaiwan University, Chang-Gung Memorial University, ChanghuaChristian Hospital, and Tzu-Chi General Hospital approved thestudy protocols, which adhered to prescribed guidelines and wereperformed according to the ethical standards of the 1964 Declara-tion of Helsinki. All of the participants provided written informedconsent.
To obtain a patient population similar to that found in clinicalpractice in Taiwan, each study physician was instructed to includethe first 15–20 patients who would normally be treated with LEVas monotherapy or add-on therapy. Each patient selected was seenat a baseline visit and at the end of 3 and 12 months of LEV treat-ment for objective and subjective assessments. The study com-prised a 3-month retrospective baseline phase, followed by a 4-week titration phase and then a 12-month maintenance phase.Demographic information and details of medical, epilepsy, andAED history were obtained for each patient at baseline. Seizureoccurrences were recorded at baseline and during and on comple-tion of treatment. Safety was assessed as frequency and severity ofadverse events, through patient perceptions and clinicalobservations.
Patients aged >16 years diagnosed with epilepsy characterizedby generalized tonic–clonic seizures or partial-onset seizures withor without secondary generalization were eligible. Patients musthave had at least two primary generalized seizures in the previous3 months or at least four partial seizures in the previous year withat least one during the previous 3 months. The dose of antiepilepticmedication must have been stable for 4 weeks prior to entry andremained stable throughout the study. Exclusion criteria were pre-vious exposure to LEV, presence or history of allergy to any LEVcomponents, progressive neurological disease, and any conditionthat might interfere with satisfactory performance on the subjec-tive and objective assessment protocols.
2.2. Criteria for evaluation: efficacy and safety
Primary efficacy variables included: seizure frequency, definedas the mean number of partial and generalized seizures per3 months over the 12-month treatment period (both titrationand maintenance phases); incidence of P50% and P75% reduc-tions in seizure frequency during the treatment period comparedwith baseline seizure frequency; and seizure freedom, defined asthe percentage of patients who experienced complete absence ofpartial or generalized tonic–clonic seizures during the last3 months of the treatment period. Seizure frequency was obtainedfrom self-reported seizure diaries in which patients noted the time,duration, and description of seizures. On each visit, the investigatorclassified the reported seizures according to the criteria of theCommission on Classification and Terminology of the InternationalLeague Against Epilepsy [21].
Information about adverse events was assessed at each visitusing a nonstructured interview and by clinical observations. Anadverse event was defined as any diagnosis or symptom that oc-curred during the study period, regardless of its relationship toLEV, and was rated as mild, moderate, or severe, and as possiblyor probably related to the LEV treatment. The scale used for ratingthe relationship of the adverse event to LEV was the WHO ToxicityGrading Scale for Determining the Severity of Adverse Events.
2.3. Cognitive and neuropsychological function
Cognitive function was assessed using the Mini-Mental StateExamination (MMSE) world version [22]. This widely used stan-dardized assessment consists of 11 items testing for orientation,memory, attention, language, and visuospatial function. Maximumscore is 30, and scores <24 are indicative of cognitive dysfunction.MMSE is as reliable and valid as other cognitive function scales,such as the Cognitive Abilities Screening Instrument (CASI).
Psychopathological function was assessed with the SymptomChecklist 90—Revised (SCL-90-R) questionnaire [23]. On thisextensively validated, self-reported checklist, respondents areasked to rate (on a 5-point Likert scale) how distressed they havefelt during the past 7 days using a list of 90 symptoms. Scoresare then generated for nine symptom scales: Depression, Somati-zation, Obsessive–Compulsive tendency, Interpersonal Sensitivity,Anxiety, Hostility, Phobic Anxiety and Psychoticism; an overallGlobal Severity Index (GSI) score reflects the number and severityof all items together. Reliability of the individual scales rangedfrom 0.77 for Psychoticism to 0.90 for Depression, and test–retestreliabilities ranged from 0.78 to 0.90, depending on the subscaleexamined and the time interval between tests [23,24].
2.4. Health-related quality of life
Health-related quality of life was assessed using the Quality ofLife in Epilepsy—10 Inventory (QOLIE-10) [25], a 10-item question-naire examining epilepsy-related quality-of-life variables, such asSeizure Worry, Overall Quality of Life, Emotional Well-Being, En-ergy/Fatigue, Cognitive Functioning, Medication Effect (physicaland mental effects of medication, two items), and Social Function(three items: work, driving, and social function). The QOLIE-10components and total scores were derived from the QOLIE-31 orig-inally developed by Cramer et al. [25]. Responses provided sub-scores and a total score, with higher scores indicating betterfunction.
2.5. Patient perceptions of LEV therapy
To assess perceptions of LEV therapy, the patients were inter-viewed using five questions on their perception of overall tolerabil-ity, overall efficacy, and speed of onset of action, comparison of LEVtherapy with previous AED therapy, improvements in daily activ-ity, and global satisfaction. Results were tabulated as the propor-tion of patients giving each response (see Table 7 for possibleresponses). The patients were tested at the end of the 12-monthtreatment period. A global satisfaction score (using a Visual Ana-logue Scale, 0–10) was determined at that time by both the patientand the physician.
2.6. Statistical methods
Continuous variables were represented as means ± SD for nor-mally distributed data and as means and ranges for nonnormallydistributed data. Categorical variables were represented as fre-quency and percentage. Mixed models were used to evaluatechanges over time, taking repeated measurements into consider-
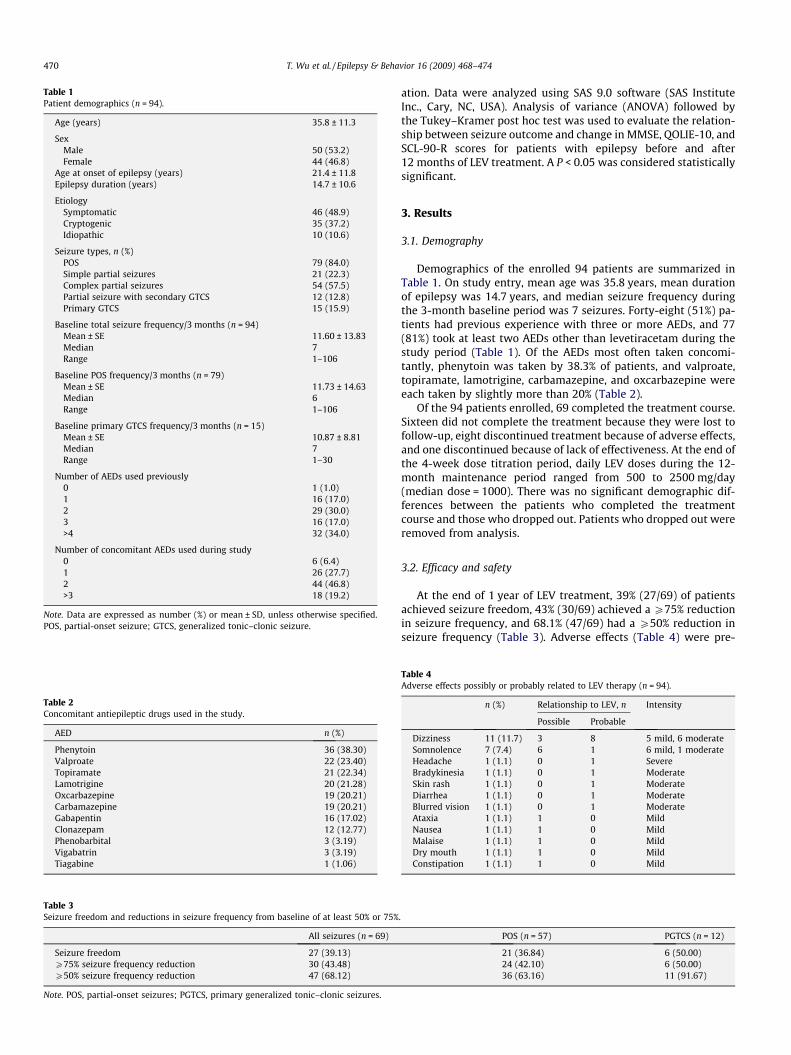
Table 1Patient demographics (n = 94).
Age (years) 35.8 ± 11.3
SexMale 50 (53.2)Female 44 (46.8)
Age at onset of epilepsy (years) 21.4 ± 11.8Epilepsy duration (years) 14.7 ± 10.6
EtiologySymptomatic 46 (48.9)Cryptogenic 35 (37.2)Idiopathic 10 (10.6)
Seizure types, n (%)POS 79 (84.0)Simple partial seizures 21 (22.3)Complex partial seizures 54 (57.5)Partial seizure with secondary GTCS 12 (12.8)Primary GTCS 15 (15.9)
Baseline total seizure frequency/3 months (n = 94)Mean ± SE 11.60 ± 13.83Median 7Range 1–106
Baseline POS frequency/3 months (n = 79)Mean ± SE 11.73 ± 14.63Median 6Range 1–106
Baseline primary GTCS frequency/3 months (n = 15)Mean ± SE 10.87 ± 8.81Median 7Range 1–30
Number of AEDs used previously0 1 (1.0)1 16 (17.0)2 29 (30.0)3 16 (17.0)>4 32 (34.0)
Number of concomitant AEDs used during study0 6 (6.4)1 26 (27.7)2 44 (46.8)>3 18 (19.2)
Note. Data are expressed as number (%) or mean ± SD, unless otherwise specified.POS, partial-onset seizure; GTCS, generalized tonic–clonic seizure.
Table 2Concomitant antiepileptic drugs used in the study.
AED n (%)
Phenytoin 36 (38.30)Valproate 22 (23.40)Topiramate 21 (22.34)Lamotrigine 20 (21.28)Oxcarbazepine 19 (20.21)Carbamazepine 19 (20.21)Gabapentin 16 (17.02)Clonazepam 12 (12.77)Phenobarbital 3 (3.19)Vigabatrin 3 (3.19)Tiagabine 1 (1.06)
Table 3Seizure freedom and reductions in seizure frequency from baseline of at least 50% or 75%
All seizures (n = 69)
Seizure freedom 27 (39.13)P75% seizure frequency reduction 30 (43.48)P50% seizure frequency reduction 47 (68.12)
Note. POS, partial-onset seizures; PGTCS, primary generalized tonic–clonic seizures.
470 T. Wu et al. / Epilepsy & Behavior 16 (2009) 468–474
ation. Data were analyzed using SAS 9.0 software (SAS InstituteInc., Cary, NC, USA). Analysis of variance (ANOVA) followed bythe Tukey–Kramer post hoc test was used to evaluate the relation-ship between seizure outcome and change in MMSE, QOLIE-10, andSCL-90-R scores for patients with epilepsy before and after12 months of LEV treatment. A P < 0.05 was considered statisticallysignificant.
3. Results
3.1. Demography
Demographics of the enrolled 94 patients are summarized inTable 1. On study entry, mean age was 35.8 years, mean durationof epilepsy was 14.7 years, and median seizure frequency duringthe 3-month baseline period was 7 seizures. Forty-eight (51%) pa-tients had previous experience with three or more AEDs, and 77(81%) took at least two AEDs other than levetiracetam during thestudy period (Table 1). Of the AEDs most often taken concomi-tantly, phenytoin was taken by 38.3% of patients, and valproate,topiramate, lamotrigine, carbamazepine, and oxcarbazepine wereeach taken by slightly more than 20% (Table 2).
Of the 94 patients enrolled, 69 completed the treatment course.Sixteen did not complete the treatment because they were lost tofollow-up, eight discontinued treatment because of adverse effects,and one discontinued because of lack of effectiveness. At the end ofthe 4-week dose titration period, daily LEV doses during the 12-month maintenance period ranged from 500 to 2500 mg/day(median dose = 1000). There was no significant demographic dif-ferences between the patients who completed the treatmentcourse and those who dropped out. Patients who dropped out wereremoved from analysis.
3.2. Efficacy and safety
At the end of 1 year of LEV treatment, 39% (27/69) of patientsachieved seizure freedom, 43% (30/69) achieved a P75% reductionin seizure frequency, and 68.1% (47/69) had a P50% reduction inseizure frequency (Table 3). Adverse effects (Table 4) were pre-
.
POS (n = 57) PGTCS (n = 12)
21 (36.84) 6 (50.00)24 (42.10) 6 (50.00)36 (63.16) 11 (91.67)
Table 4Adverse effects possibly or probably related to LEV therapy (n = 94).
n (%) Relationship to LEV, n Intensity
Possible Probable
Dizziness 11 (11.7) 3 8 5 mild, 6 moderateSomnolence 7 (7.4) 6 1 6 mild, 1 moderateHeadache 1 (1.1) 0 1 SevereBradykinesia 1 (1.1) 0 1 ModerateSkin rash 1 (1.1) 0 1 ModerateDiarrhea 1 (1.1) 0 1 ModerateBlurred vision 1 (1.1) 0 1 ModerateAtaxia 1 (1.1) 1 0 MildNausea 1 (1.1) 1 0 MildMalaise 1 (1.1) 1 0 MildDry mouth 1 (1.1) 1 0 MildConstipation 1 (1.1) 1 0 Mild

Table 5Repeated measurements of MMSE score analyzed by the mixed model (n = 69).
Baseline 3 months 12 months P
Orientation 9.43 ± 1.53 9.54 ± 1.33 9.68 ± 1.37 0.11Registration 2.96 ± 0.36 2.93 ± 0.40 2.94 ± 0.38 0.22Attention and calculation 4.38 ± 1.36 4.55 ± 1.25 4.59 ± 1.06 0.19Recall (short-term memory) 2.36 ± 1.01 2.70 ± 0.69 2.75 ± 0.67 0.0006a
Language 7.48 ± 1.11 7.80 ± 0.63 7.83 ± 0.73 <0.0001a
Construction 0.96 ± 0.21 0.97 ± 0.17 0.99 ± 0.12 0.37Total score 27.67 ± 4.35 28.51 ± 3.66 28.78 ± 3.68 <0.0001a
Note. Data are expressed as mean ± SD.a P < 0.05.
Table 6Repeated measurements of SCL-90-R analyzed by the mixed model (n = 46).
Baseline 3 months 12 months P
Somatization 0.86 ± 0.56 0.87 ± 0.57 0.83 ± 0.59 0.64Obsessive–Compulsive 1.30 ± 0.71 1.26 ± 0.70 1.17 ± 0.64 0.18Interpersonal Sensitivity 0.75 ± 0.68 0.81 ± 0.66 0.65 ± 0.58 0.022a
Depression 1.09 ± 0.85 1.00 ± 0.72 0.92 ± 0.66 0.095Anxiety 0.86 ± 0.68 0.79 ± 0.66 0.72 ± 0.60 0.14Hostility 0.80 ± 0.63 0.73 ± 0.59 0.69 ± 0.52 0.35Phobic Anxiety 0.72 ± 0.84 0.68 ± 0.72 0.57 ± 0.66 0.16Paranoid Ideation 0.61 ± 0.53 0.74 ± 0.56 0.57 ± 0.48 0.024a
Psychoticism 0.64 ± 0.50 0.63 ± 0.47 0.55 ± 0.49 0.31Global Severity Index 0.77 ± 0.65 0.81 ± 0.71 0.77 ± 0.66 0.77
Note. Data are expressed as means ± SD.a P < 0.05.
T. Wu et al. / Epilepsy & Behavior 16 (2009) 468–474 471
dominantly mild to moderate in severity and caused prematurewithdrawal in only eight cases (dizziness 2; somnolence 2; and 1each for headache, skin rash, diarrhea, and bradykinesia). Dizzinessand somnolence were the only treatment-related adverse effectsreported in >5% of patients (Table 4). There were no serious ad-verse effects such as hospitalization, life-threatening events, signif-icant disability/incapacity, and death.
3.3. Cognitive and neuropsychological function
The mean MMSE score at baseline was 27.57, which indicatedno cognitive dysfunction and increased to 28.78 at the end of12 months of LEV therapy (P < 0.0001) (Table 5). Only two of theseven individual test items showed highly significant improve-ment: Recall (short-term memory) and Language (P < 0.0006 andP < 0.0001, respectively).
Forty-six patients completed the SCL-90-R questionnaire beforeand after 12 months of LEV treatment. The mean Global SeverityIndex for the SCL-90-R at baseline was 0.77 ± 0.65, which did notsignificantly change after the 12-month treatment period. None-theless, there were modestly significant improvements by theend of the treatment period for two of the nine symptom scales:Interpersonal Sensitivity (P = 0.0217) and Paranoid Ideation(P = 0.0239) (Table 6).
Table 7Repeated measurements of QOLIE-10 analyzed by the mixed model (n = 69).
Baseline
Energy 48.70 ± 21.55Emotional Well-Being 52.75 ± 23.00Overall QOL 55.07 ± 19.92Daily Activity/Social Function 59.30 ± 20.24Seizure Worry 56.52 ± 36.30Cognition 44.20 ± 32.69Medication Effect 50.36 ± 34.56
Total score 52.42 ± 13.35
Note. Data are expressed as means ± SD.a P < 0.05.
3.4. Health-related quality of life and patient perceptions
The mean total score for quality of life on the QOLIE-10 in-creased from 52.42 ± 13.35 at baseline to 55.83 ± 13.57 at theend of the study, an increase of borderline statistical significance(P = 0.0344). Similarly, there were modestly significant improve-ments in two subscores, Cognition (P = 0.0150) and Medication Ef-fect (P = 0.0023). However, the Daily Activity/Social Functionsubscore was significantly worse (P = 0.0004) at the end than atthe beginning of treatment (Table 7).
As subjectively reported by the patients themselves (Table 8),overall tolerability and effectiveness were generally perceived as‘‘good,” and most reported a moderately rapid onset of action(within 1 month). Compared with previous therapy, LEV therapywas generally perceived as being ‘‘somewhat better” (42.03%) or‘‘just as good” (39.13%). Most patients reported LEV therapy to be‘‘somewhat better” (46.38%) in terms of improvement in dailyactivity. The Global Satisfaction scores were 7.39 (patients) and7.41 (physicians).
3.5. Seizure outcome and MMSE, QOLIE-10, and SCL-90-R
Table 9 outlines the relationship between seizure outcome andchange in MMSE, QOLIE-10, and SCL-90-R scores for patients withepilepsy before and after 12 months of LEV treatment. Patientswith a greater than 50% seizure reduction rate after LEV treatmenthad significantly improved QOLIE-10 scores on Seizure Worry,Overall Quality of Life, and Total Quality of Life. Seizure outcomehad no effect on MMSE and SCL-90-R scores.
4. Discussion
4.1. Clinical efficacy and safety of LEV
The efficacy and safety profile of LEV in this study is consistentwith those reported in the literature [2–4,6–8]. A larger percentageof patients achieved seizure freedom (39% vs 16%) and seizure fre-quency reduction P50% (68% vs 50%) after the 12 months of treat-
3 months 12 months P
51.30 ± 21.82 54.78 ± 22.66 0.1155.88 ± 21.46 59.13 ± 22.61 0.1360.14 ± 22.00 57.25 ± 20.16 0.2050.48 ± 16.66 51.33 ± 17.89 0.0004a
58.46 ± 32.55 53.62 ± 32.46 0.4952.54 ± 32.69 53.26 ± 32.34 0.015a
64.49 ± 29.98 61.41 ± 29.61 0.0023a
56.15 ± 14.55 55.83 ± 13.57 0.034a

Table 8Perceived effectiveness and tolerability of LEV therapy (n = 69).
Index n (%)
Overall tolerabilityVery good 15 (21.74)Good 36 (52.17)Moderate 17 (24.64)Poor 1 (1.45)
Overall effectivenessVery good 12 (17.39)Good 29 (42.03)Moderate 28 (40.58)
Onset of actionVery rapid (1 day) 4 (5.80)Rapid (1 week) 31 (44.93)Moderate (within 1 month) 34 (49.28)
Current therapy versus previous therapyMuch better 11 (15.94)Somewhat better 29 (42.03)Just as good 27 (39.13)Moderate 1 (1.45)Somewhat worse 1(1.45)
Improvement in daily activityMuch better 9 (13.04)Somewhat better 32 (46.38)Just as good 26 (37.68)Somewhat worse 2 (2.90)
Global satisfaction (physician) 7.41 ± 1.21Global satisfaction (patient) 7.39 ± 1.48
Note. Data are expressed as numbers (%) or means ± SD.
472 T. Wu et al. / Epilepsy & Behavior 16 (2009) 468–474
ment in this study than in the SKATE trial, an earlier large, open-la-bel study [26]. However, the SKATE trial included only those with
Table 9Changes in MMSE, QOLIE-10, and SCL-90-R scores for patients with epilepsy before and a
P50% seizure frequency reduction(n = 47)
0–50% se(n = 12)
MMSETotal score 1.04 ± 2.52 0.08 ±Orientation 0.04 ± 0.09 0.08 ±Registration �0.02 ± 0.15 �0.08 ±Attention and calculation 0.20 ± 1.34 �0.08 ±Recall (short-termmemory)
0.47 ± 1.14 0.17 ±
Language 0.36 ± 0.89 0.17 ±Construction 0.00 ± 0.37 �0.08 ±
QOLIE-10Total score 10.00 ± 2.53 4.50 ±Energy 2.13 ± 3.61 13.33 ±Emotional Well-Being 3.40 ± 3.51 3.33 ±Overall QOL 9.58 ± 3.19 0.00 ±Daily activity/SocialFunction
11.70 ± 4.20 1.39 ±
Seizure Worry 12.60 ± 4.12 �2.83 ±Cognition 7.98 ± 4.24 8.33 ±Medication Effect 14.63 ± 5.26 9.38 ±
SCL-90-R (n = 28) (n = 10)Somatization �0.21 ± 0.08 �0.06 ±Obsessive–Compulsive �0.14 ± 0.07 �0.16 ±Interpersonal Sensitivity �0.06 ± 0.10 �0.21 ±Depression �0.18 ± 0.08 �0.48 ±Anxiety �0.19 ± 0.07 �0.14 ±Hostility �0.01 ± 0.13 �0.57 ±Phobic Anxiety �0.16 ± 0.09 �0.02 ±Paranoid Ideation 0.02 ± 0.10 0.15 ±Psychoticism �0.09 ± 0.06 0.07 ±Global Severity Index �0.15 ± 0.10 0.13 ±
Note. Data are expressed as means ± SD.a P < 0.05.
partial seizures, whereas this study was designed to be similar tonormal clinical practice and included patients newly diagnosedwith epilepsy and idiopathic generalized tonic–clonic seizures,which are easier to treat [3]. Nevertheless, the limitation of usingself-reported seizure frequency may overestimate efficacy, as pa-tients may have had seizures of which they were unaware.
Most adverse events are mild or moderate, and confined mainlyto the central nervous system, that is, somnolence, fatigue, dizzi-ness, and headache. There were eight cases of LEV withdrawal,which constitutes 8.5% of the 94 intent-to-treat patient populationand is within the 7–19% range reported in the literature [3,27,28].
4.2. Cognitive and psychopathological function
The results indicated improved cognition after LEV treatment,consistent with previous reports [13,18,19,28]. There was highlysignificant improvement in two subscores, Recall and Language,which are areas impaired in treated persons with epilepsy com-pared with healthy controls [16]. Piazzini et al. [29] reported sim-ilar specific improvements in memory and verbal fluency after LEVuse in epilepsy. LEV is derived from piracetam, a drug that has beenreported to improve learning, memory, and attention [30]. Our re-sults revealed no association between improvements in MMSE andbetter seizure control (Table 9), suggesting that LEV per se may im-prove cognitive function. Even so, MMSE is a crude test with greatvariability; thus the increase in MMSE score might not be clinicallysignificant. It is possible that a greater increase may be observed,but this is limited by the ceiling effect. Without a healthy controlgroup in our study, it is not possible to know whether greaterimprovements may be seen without LEV. Although the presentstudy showed that MMSE scores were increased by LEV, furtherstudy of the ability of LEV to improve cognitive function is needed.
fter 12 months of LEV treatment.
izure frequency reduction Increased seizure frequency(n = 10)
P
0.56 1.17 ± 0.57 0.420.31 0.39 ± 0.26 0.340.08 �0.11 ± 0.09 0.460.23 0.33 ± 0.24 0.640.21 0.33 ± 0.21 0.69
0.16 0.22 ± 0.13 0.660.08 �0.11 ± 0.08 0.45
3.09 �1.22 ± 3.48 0.04a
7.91 �4.44 ± 5.25 0.1611.50 �6.67 ± 6.05 0.406.88 �11.11 ± 6.14 0.007a
5.88 4.17 ± 5.69 0.37
9.70 �20.50 ± 8.15 0.001a
7.11 5.56 ± 5.91 0.9411.83 6.25 ± 6.08 0.66
(n = 8)0.16 0.05 ± 0.14 0.240.20 �0.18 ± 0.17 0.960.20 �0.04 ± 0.13 0.710.27 �0.07 ± 0.17 0.230.28 �0.13 ± 0.07 0.910.36 0.00 ± 0.12 0.110.16 �0.20 ± 0.22 0.740.27 0.06 ± 0.11 0.850.27 0.06 ± 0.11 0.520.25 0.04 ± 0.08 0.33

T. Wu et al. / Epilepsy & Behavior 16 (2009) 468–474 473
The instrument used to assess psychological changes, the SCL-90-R, revealed no significant change in the Global score and mod-est improvements in two of the nine subscores, Paranoid Ideationand Interpersonal Sensitivity, at the end of the 12-month treat-ment period. Compared with the healthy population, patients withepilepsy in Taiwan have poorer quality of life with respect to thephysical, psychological, and social domains [31]. They have diffi-culty developing personal relationships and are less likely to be ac-cepted or respected by others [31]. This may be due tomisconceptions and negative attitudes held by people in Asia.Our QOLIE-10 results revealed a significant improvement in mentaleffects on AEDs. SCL-R-90 scores indicated that Paranoid Ideationand Interpersonal Sensitivity improved with LEV, implying that pa-tients with epilepsy were less insecure after LEV treatment. Ciesiel-ski et al. [32] also reported a marked improvement in InterpersonalSensitivity in in patients with refractory partial epilepsy treatedwith LEV. One limitation of our study is that the SCL-90-R wasnot designed to determine increases in aggressive and challengingbehavior as reported in four other studies [19,20,33,34]. Those sideeffects have been well documented and remain an obstacle in clin-ical practice. However, it must be noted that two of these studiesenrolled people with epilepsy with intellectual disabilities, a pop-ulation different from the routine clinical population studied here.
4.3. Health-related quality of life and patient perceptions
In the current study quality of life improved modestly, and pa-tients had a generally positive subjective perception of the effec-tiveness and tolerability of LEV therapy. In addition,improvement of seizure control is important in reducing seizureworry and improving overall quality of life after LEV treatment.However, there is one unexplained contradiction between the QO-LIE-10 test results and the patients’ personal perceptions. QOLIE-10 Daily Activity/Social Function subscores significantly worsenedwith LEV treatment, but 96% of the patients themselves rated theirdaily activity during LEV treatment as ‘‘just as good as” or ‘‘betterthan before.” However, because this is an open-label study, themore positive subjective rating may be due to a placebo effect. Interms of the progressive worsening of social function seen in theQOLIE results, negative behavioral changes are not specifically ac-counted for in the present study. Reports on add-on LEV therapy inpatients with epilepsy indicate a relatively high incidence of irrita-bility, agitation, anger, and aggressive behavior ranging from 8.1 to15% regardless of magnitude or frequency of dosage [19,20,33].Studies on the behavior of patients following LEV remain insuffi-cient and additional studies are needed.
The patient-perceived effectiveness of LEV in terms of onset,tolerability, and overall effectiveness is consistently reported tobe ‘‘somewhat better” than or at least ‘‘just as good” as that affor-ded by previous AEDs. This is still consistent with the clinical effi-cacy outcomes of previous studies [7].
5. Conclusions
This study demonstrates that adjunctive therapy or mono-therapy with LEV in patients with epilepsy not only effectively re-duces seizure frequency while maintaining a favorable safetyprofile, but also possibly improves cognitive and neuropsychologi-cal functions such as recall, language, interpersonal sensitivity, andparanoid ideation. Patient perceptions of LEV therapy are consis-tent with clinical findings, and treatment-associated adverse ef-fects are either minimal or most frequently mild in severity. LEVmay, however, contribute to negative outcomes with respect to so-cial function. Additional research is required to investigate its neg-
ative behavioral effects (e.g., aggression and irritability) followingshort- and long-term therapy.
Conflict of interest statement
None of the authors was funded by UCB. The authors state noconflict of interest.
Acknowledgment
The study was sponsored by UCB (Taiwan) Ltd.
References
[1] Chaisewikul R, Privitera MD, Hutton JL, Marson AG. Levetiracetam add-on fordrug-resistant localization related (partial) epilepsy. Cochrane DatabaseSystemic Rev 2001:CD001901.
[2] Berkovic SF, Knowlton RC, Leroy RF, Schiemann J, Falter U. Placebo-controlledstudy of levetiracetam in idiopathic generalized epilepsy. Neurology2007;69:1751–60.
[3] Brodie MJ, Perucca E, Ryvlin P, Ben Menachem E, Meencke HJ. Comparison oflevetiracetam and controlled-release carbamazepine in newly diagnosedepilepsy. Neurology 2007;68:402–8.
[4] Noachtar S, Andermann E, Meyvisch P, Andermann F, Gough WB, Schiemann-Delgado J. For the N166 Levetiracetam Study Group. Levetiracetam for thetreatment of idiopathic generalized epilepsy with myoclonic seizures.Neurology 2008;70:607–16.
[5] Surges R, Volynski KE, Walker MC. Is levetiracetam different from otherantiepileptic drugs? Levetiracetam and its cellular mechanism of actionrevisited. Ther Adv Neurol Disord 2008;1:13–24.
[6] Ben-Menachem E, Falter U. For the European Levetiracetam Study Group.Efficacy and tolerability of levetiracetam 3000d in patients with refractorypartial seizures: a multi-center double-blind, responder-selected studyevaluating monotherapy. Epilepsia 2000;41:1276–83.
[7] Cereghino JJ, Biton V, Abou-Khalil B, Dreifuss F, Gauer LJ, Leppik IE.Levetiracetam for partial seizures: results of a double-blind, randomizedclinical trial. Neurology 2000;55:236–42.
[8] Shorvon SD, Lowenthal A, Janz D, Bielen E, Loiseau P. For the EuropeanLevetiracetam Study Group. Multi-center double-blind, randomized, placebo-controlled trial of levetiracetam as add-on therapy in patients with refractorypartial seizures. Epilepsia 2000;41:1179–86.
[9] Meador KJ, Gevins A, Loring DW, et al. Neuro-psychological and neuro-physiologic effects of carbamazepine and levetiracetam. Neurology2007;69:2076–84.
[10] Pigeolet E, Jacqmin P, Sargentini-Maier ML, Stockis A. Populationpharmacokinetics of levetiracetam in Japanese and Western adults. ClinPharmacokinet 2007;46:503–12.
[11] Tsai JJ, Yen DJ, Hsih MS, et al. Efficacy and safety of levetiracetam (up to2000 mg/day) in Taiwanese patients with refractory partial seizures: a multi-center, randomized, double-blind placebo-controlled study. Epilepsia2006;47:77–81.
[12] Heo K, Lee BI, Yi SD, et al. Efficacy and safety of levetiracetam as adjunctivetreatment of refractory partial seizures in a multi-center open-label single-arm trial in Korean patients. Seizure 2007;16:4029.
[13] Wu XY, Hong Z, Wu X, et al. Multi-center double-blind, randomized, placebo-controlled trial of levetiracetam as add-on therapy in Chinese patients withrefractory partial-onset seizures. Epilepsia 2008;50:398–405.
[14] Zhao Q, Jiang J, Li X, Lu ZS, Hu P. Single-dose pharmacokinetics of levetiracetamin healthy Chinese male subjects. Br J Clin Pharmacol 2007;63:614–7.
[15] Zhou B, Zhang Q, Tian L, Xiao J, Stefan H, Zhou D. Effects of levetiracetam as anadd-on therapy on cognitive function and quality of life in patients withrefractory partial seizures. Epilepsy Behav 2008;12:305–10.
[16] Lutz MT, Helmstaedter C. EpiTrack: tracking cognitive side effects ofmedication on attention and executive functions in patients with epilepsy.Epilepsy Behav 2005;7:708–14.
[17] French J, Edrich P, Cramer JA. A systematic review of the safety profile oflevetiracetam: a new anti-epileptic drug. Epilepsy Res 2001;47:77–90.
[18] Cramer JA, Arrigo C, Van Hammee G, Gauer LJ, Cereghino JJ. For the N132 StudyGroup. Effect of levetiracetam on epilepsy-related quality of life. Epilepsia2000;41:868–74.
[19] White JR, Walczak TS, Leppik IE, et al. Discontinuation of levetiracetambecause of behavioral side effects: a case-control study. Neurology2003;61:1218–21.
[20] Hurtado B, Koepp MJ, Sander JW, Thompson PJ. The impact of levetiracetam onchallenging behavior. Epilepsy Behav 2006;8:588–92.
[21] Commission on Classification and Terminology of the International LeagueAgainst Epilepsy. Proposal for revised clinical and electroencephalographicclassification of epileptic seizures. Epilepsia 1981;22:489–501.
[22] Folstein MF, Folstein SE, Mchugh PR. ‘Mini Mental State’: a practical methodfor grading the cognitive state of patients for the clinician. J Psychiatr Res1975;12:189–98.

474 T. Wu et al. / Epilepsy & Behavior 16 (2009) 468–474
[23] Derogatis LR. Symptom Checklist-90-R (SCL-90-R): administration, scoringand procedures manual. 3rd ed. Minneapolis: National Computer Systems;1994.
[24] Green BL, Gleser GC, Stone WN. Seifert RF Relationships among diversemeasures of psychotherapy outcome. J Consult Clin Psychol1975;43:689–99.
[25] Cramer JA. Quality of life assessments in epilepsy. In: Spilker B, editor. Qualityof life and pharmacoeconomics in clinical trials. Philadelphia: Lippincott–Raven; 1996. p. 909–18.
[26] Steinhoff BJ, Somerville ER, Van Paesschen W, Ryvlin P, Schelstraete I. TheSKATE study: an open-label community-based study of levetiracetam as add-on therapy for adults with uncontrolled partial epilepsy. Epilepsy Res2007;76:6–14.
[27] Ferrendelli JA, French J, Leppik IE, et al. Use of levetiracetam in a population ofpatients aged 65 years and older: a subset analysis of the KEEPER trial.Epilepsy Behav 2003;4:702–9.
[28] Helmstaedter C, Witt JA. The effects of levetiracetam on cognition: a non-interventional surveillance study. Epilepsy Behav 2008;13:642–9.
[29] Piazzini A, Chifari R, Canevini MP, Turner K, Fontana SP, Canger R.Levetiracetam: an improvement of attention and of oral fluency in patientswith partial epilepsy. Epilepsy Res 2006;68:181–8.
[30] Genton P, Van Vleymen B. Piracetam and levetiracetam: close structuralsimilarities but different pharmacological and clinical profiles. Epileptic Disord2000;2:99–105.
[31] Liou HH, Chen RC, Chen CC, Chiu MJ, Chang YY, Wang JD. Health related qualityof life in adult patients with epilepsy compared with a general referencepopulation in Taiwan. Epilepsy Res 2005;64:151–9.
[32] Ciesielski AS, Samson S, Steinhoff B. Neuropsychological and psychiatricimpact of add-on titration of pregabalin versus levetiracetam: a comparativeshort-term study. Epilepsy Behav 2006;9:424–31.
[33] Dinkelacker V, Dietl T, Widman G, Lengler U, Elger CE. Aggressive behavior ofepilepsy patients in the course of levetiracetam add-on therapy: report of 33mild to severe cases. Epilepsy Behav 2003;4:537–47.
[34] Beavis J, Meek A, Felce D, Kerr M. A prospective multi-centre open label studyof the use of levetiracetam as add-on treatment of epilepsy and intellectualdisabilities. Seizure 2009;18:279–84.