diagnostic relevance of overexpressions of pkc- θand...
TRANSCRIPT

Abstract. Background: We investigated the clinicopatho-logical and immunohistochemical characteristics, geneticaberrations and prognostic factors in 28 patients withextragastrointestinal stromal tumors (EGISTs) from six centersin South Korea. Patients and Methods: Immunohistochemistrywas performed for c-KIT (CD117), PKC-θ (protein kinase Ctheta), DOG-1 (discovered on GIST-1), CD34, alpha-smoothmuscle actin (α-SMA), vimentin, desmin and S-100 protein.Genetic analyses for the KIT gene (exon 9, 11, 13 and 17) andthe platelet- derived growth factor receptor alpha (PDGFRA)gene (exons 12 and 18) were performed by direct sequencing ofPCR products. The relationships of various clinicopathologicalcharacteristics and outcomes were also examined. Results: Ofthe tumor samples, 78.6% (22/28) were located in the intra-abdominal cavity including the omentum and mesentery, and
10.7% (3/28) were located in the retroperitoneum. All patientswere older than 39 years. The median size of the tumors was10 cm for the maximum diameter. When first detected, 57.1% ofEGISTs were large in size, measuring more than 10 cm.Tumors that were larger than 10 cm were found morefrequently among tumors with more than 10 mitoses per 50high-power fields (HPFs) and this finding was statisticallysignificant (p<0.05). Based on immunohistochemical results,the EGISTs were positive for c-KIT in 96.4% (27/28) ofsamples, PKC-θ in 82.1% (23/28), DOG-1 in 85.7% (24/28),PDGFRA in 82.1% (23/28), CD34 in 67.9% (19/28), vimentinin 100% (28/28), α-SMA in 28.6% (8/28), S-100 protein in39.3% (11/28) and desmin in 28.6% (8/28). c-KIT, DOG-1 andPKC-θ immunostains were sensitive and specific, but thePDGFRA stain was not specific for EGISTs. c-KIT expressionwas correlated with DOG-1 expression (p<0.05). One c-KIT-negative EGIST was also negative for DOG-1, but positive forPDGFRA and PKC-θ immunostains. Out of all EGISTs, 57.1%had tumor necrosis and most of these were more than 10 cmin size, and had obvious nuclear atypia and high mitotic counts(>10/50 HPFs). Overall survival (OS) was correlated withtumor size >10 cm, tumor necrosis, obvious nuclear atypia,mitotic counts >10/50 HPFs and epithelioid or mixed cell type(p<0.05). Eleven EGISTs (44.0%) had mutations in the KITgene and 6 (24.0%) had mutations in the PDGFRA gene, the
923
Correspondence to: Dong-Hoon Kim, MD, Ph.D., Department ofPathology, Kangbuk Samsung Hospital, Sungkyunkwan UniversitySchool of Medicine, 78 Saemunan-gil, Jongno-Gu, Seoul 110-746,South Korea. Tel: +82 220012392, Fax: +82 220012398, e-mail:[email protected]
Key Words: Extragastrointestinal stromal tumors, DOG-1, PKC-θ,KIT gene, PDGFRA gene.
ANTICANCER RESEARCH 32: 923-938 (2012)
Diagnostic Relevance of Overexpressions of PKC-θ and DOG-1and KIT/PDGFRA Gene Mutations in ExtragastrointestinalStromal Tumors: A Korean Six-Centers Study of 28 Cases
KYUNG-HEE KIM1, SCOTT D. NELSON2, DONG-HOON KIM3, KYUNG UN CHOI4, SU JIN KIM5, KYUENG-WHAN MIN6, KI-SEOK JANG6, SEUNG SAM PAIK6, YOUNG-HA OH6, SEOUNG WAN CHAE3,
JIN HEE SOHN3, HONG JOO KIM7, YONG KYUN CHO7, BYUNG IK KIM7, DONG IL PARK7, CHONG IL SOHN7, SUKJOONG OH7, SEON HYEONG CHOI8, YOON JUNG CHOI8, HEE-YEON WOO9,
YONG LAI PARK10, SE JIN PARK11, SANG HYUK LEE12, SEUNGHO RYU13, SUNG-IM DO3, GUHYUN KANG3, KYUNGEUN KIM3, YOUNG HYE CHO3 and JUNG-SOO PYO3
1Department of Pathology, Cancer Research Institute,Chungnam National University, School of Medicine, Daejeon, South Korea;
2Department of Pathology, Santa Monica-UCLA Medical Center and Orthopedic Hospital, Santa Monica, CA, U.S.A.;Departments of 3Pathology, 7Internal Medicine, 8Radiology, 9Laboratory Medicine, 10Surgery,
11Orthopedic Surgery, 12Otorhinolaryngology-Head and Neck Surgery and13Medical Screening Center/Department of Occupational Medicine, Kangbuk Samsung Hospital,
Sungkyunkwan University School of Medicine, Seoul, South Korea;4Department of Pathology, School of Medicine, Pusan National University, Yangsan, Gyeongnam, South Korea;
5Department of Pathology, Dong-A University College of Medicine, Busan, South Korea;6Department of Pathology, College of Medicine, Hanyang University, Seoul, South Korea
0250-7005/2012 $2.00+.40

most common being missense mutations or deletions affectingexon 11 of the KIT gene (n=9) or exon 18 of the PDGFRAgene (n=6). Three cases showed co-existence of both KIT andPDGFRA gene mutations. There were no mutations of exon17 of KIT and exon 12 of PDGFRA genes. Conclusion: The c-KIT, PKC-θ and DOG-1 antigens are the most sensitive andspecific immunomarkers for confirming EGISTs. PKC-θ andPDGFRA immunostains are helpful markers for c-KIT-negative EGISTs. Survival analyses indicated that tumor size>10 cm, mitotic rate >10/50 HPFs, tumor necrosis, obviousnuclear atypia, and epithelioid or mixed cell type weresignificant predictors of survival. We found that thecombination of these parameters helped to predict aggressivetumor behavior and may be useful for predicting theprognosis of EGISTs. The majority of gene mutations wereidentified in exon 11 of the KIT gene or exon 18 of thePDGFRA gene. The pattern of KIT and PDGFRA mutationsin EGISTs was essentially similar to the one in GISTs. Fromthe immunohistochemistry and molecular geneticsperspective, EGISTs may be a special subtype of GISTs. Bothimmunohistochemical and molecular evaluation are useful forclassifying tumors as EGISTs.
Extragastrointestinal stromal tumors (EGISTs) are neoplasmswith histology and immunohistochemistry similar to those ofgastrointestinal stromal tumors (GISTs) but are locatedoutside the gastrointestinal tract, such as in the soft tissue ofthe intra-abdominal cavity, including the omentum,mesentery, retroperitoneum, pancreas, spleen or vulvovaginal/rectovaginal septum. The histogenesis of EGISTs has notbeen elucidated, but the expression of the c-KIT, a tyrosinekinase receptor in EGISTs indicates the presence ofpacemaker cells from outside the gastrointestinal tract (1-9).
Most EGISTs are thought to be malignant, but due to theirrarity, little is known about their pathogenesis, incidence,prognosis and genetic background. Currently, the malignantpotential of EGISTs is determined by the same parametersused for GISTs, such as tumor size, mitotic rate and presenceof necrosis, but it remains unclear whether this is a rationalapproach. The guidelines for risk assessment of primaryGISTs are different according to the gastrointestinal organ(10), so we anticipate that the guidelines for risk assessmentof primary EGISTs will be different from those for GISTs.As the risk factors of EGISTs remain unknown, comparisonsbetween EGISTs and GISTs are important to determinewhether they have similar clinicopathological behaviors andare caused by the same mutations.
Most EGISTs express the KIT protein, based on previousstudies demonstrating immunohistochemical staining for c-KIT (CD117), which is thought to a useful marker fordistinguishing EGISTs from other mesenchymal tumors ofsoft tissue, such as desmoid tumors, leiomyosarcomas, andmalignant peripheral nerve sheath tumors (1, 2, 4-7).
Recently, protein kinase C theta (PKC-θ), a novel PKCisotype involved in T-cell activation, skeletal muscle signaltransduction, and neuronal differentiation (11, 12), andDOG-1 (discovered on GIST 1) (13), were shown to beoverexpressed in GISTs. PKC-θ and DOG-1 expression inGISTs has been studied previously, but there have only beena few studies of these two markers in only a small numbersof EGISTs (9).
Recent advances in the study of the KIT gene and theplatelet- derived growth factor receptor alpha (PDGFRA)gene revealed that GISTs are closely related to gain-of-function mutations in the KIT and PDGFRA genes. KITmaps to chromosome 4q12 and encodes a 109870 Dtransmembrane glycoprotein. KIT gene mutations have beenfound in exon 11, which encodes the juxtamembranedomain; in exon 9, which encodes the extracellular domain;in exon 13, which encodes the tyrosine kinase domain; and inexon 17, which also encodes the tyrosine kinase domain.PDGFRA is located adjacent to KIT and encodes a 122676 Datransmembrane glycoprotein that is highly similar to KIT.The PDGFRA gene mutations are present in exon 12, whichencodes the juxtamembrane domain and in exon 18, whichencodes the tyrosine kinase domain (14, 15).
The aim of this study was to analyze the immunohisto-chemical markers and the genetic mutations associated withEGISTs and to assess any correlations between clinico-pathological parameters of EGISTs and survival rate.
Patients and Methods
Patients. Tumor samples were obtained from 28 patients withEGISTs. We reviewed cases of EGISTs that arose from the intra-abdominal cavity, abdominal wall, prostate and retroperitoneum,collected at Kangbuk Samsung Hospital (Seoul, South Korea), EuljiUniversity Hospital (Daejeon, South Korea), Chungnam NationalUniversity (Daejeon, South Korea), Hanyang University (Seoul,South Korea), Dong-A University Hospital (Pusan, South Korea)and Pusan National University Hospital (Pusan, South Korea) from1997 to 2007. In addition, 28 non-EGIST tumors, includingleiomyomas, leiomyosarcomas, schwannoma, malignant peripheralnerve sheath tumors and desmoid tumors were included as a controlgroup. The follow-up data for these patients were analyzedretrospectively. Clinical information regarding the locations andsizes of tumors, patient status and follow-up period were obtainedby reviewing the medical records. The histopathologic tumor celltypes, mitotic counts per 50 high power fields (HPFs), obviousnuclear atypia and tumor necrosis were reviewed in thehematoxylin-eosin (H-E) stained slides of each case. Overallsurvival (OS) was calculated as the period from surgery until thedate of the death. The study was performed according to theDeclaration of Helsinki and approved by the local Ethics Committeeof the Kangbuk Samsung Hospital.
Immunohistochemical staining. We produced tissue microarray(TMA) blocks containing 2-mm diameter cores of the EGISTtissues from the enrolled cases. One core was obtained from the
ANTICANCER RESEARCH 32: 923-938 (2012)
924

central portion of the mass of each case. The TMA blocks weresectioned at a 4 μm thickness and were processed for immuno-histochemistry. Immunohistochemical studies were performed usingDAKO’s Envision method. The vendors that supplied the primaryantibodies and dilution factors are listed in Table I. Theimmunostaining was performed using a compact polymer method(from Bond Intense Detection Kit, Leica Biosystems, Newcastle,UK). Diaminobenzidine (DAB) was the chromogen. Clinicalpositive control cases for all markers were included in every stainingbatch. The immunostained slides were scored on the basis of thepercentage of positive tumor cells staining above background, asnegative (0%), weakly stained (<10%), moderately positive (10-50%) or strongly positive (>50%).
Scores were entered into a Microsoft Excel spreadsheet. Scoringresults were separated into two categories, either negative (score of0 or 1) or positive (score of 2 or 3). The uninterpretable results wereeliminated from further consideration.
Polymerase chain reaction (PCR) for the KIT and PDGFRA genes.Genetic analyses of the KIT gene (exons 9, 11, 13 and 17) and thePDGFRA gene (exons 12 and 18) were performed by directsequencing of PCR products. Genomic DNA was extracted fromparaffin-embedded tissues using standard proteinase K digestion andphenol/chloroform extraction. The sequences of each primer aresummarized in Table II.
Statistical analysis. PASW Statistics 18.0 (SPSS Inc., Chicago, IL,USA) was used for statistical analysis. Survival curves were plottedusing Kaplan-Meier methods, with significance assessed using log-rank tests and based on OS over 10 years. Multivariate analyseswere analyzed using Cox regression model. For correlations, thePearson χ2 test was used.
Results
Clinicopathological findings. Out of the EGISTs included inthis study, 78.6% (22/28) were located in the intra-abdominalcavity including the omentum and mesentery and 10.7%(3/28) were retroperitoneal. The ages of the patients rangedfrom 39 to 78 years (mean, 58 years). There were no child oradolescent patients. There was a slight male predominancein the study group (M:F=15:13). The sizes of the tumorsranged from 3 to 47 cm (median 10 cm) in maximumdiameter. A total of 5 tumors out of the 28 defined EGISTswere from 2 to 5 cm in size, 7 tumors were 6 to 10 cm and16 tumors were larger than 10 cm. There were no EGISTssmaller than 2 cm. Upon initial detection, 57.1% (16/28) ofEGISTs were large, measuring more than 10 cm. Regarding
Kim et al: Diagnostic Relevance of Overexpressions of PKC-θ and DOG-1 and KIT/PDGFRA in EGIST
925
Table I. Antibodies used for immunohistochemical staining.
Antibody Company Clone Dilution
c-KIT DAKO (Glostrup, Denmark) Rabbit polyclonal 1:1,000DOG-1 Novocastra (Newcastle, UK) Mouse monoclonal (K9) 1:100PKC-θ Abcam (Cambridge, UK) Mouse monoclonal (MC5) 1:100PDGFRA NeoMarkers (Fremont, CA, USA) Rabbit polyclonal 1:100Vimentin DAKO (Glostrup, Denmark) Mouse monoclonal vim3B4 1:1,000CD34 DAKO (Glostrup, Denmark) Mouse monoclonal QBEnd-10 1:1,000α-SMA DAKO (Glostrup, Denmark) Mouse monoclonal 1A4 1:1,000Desmin DAKO (Glostrup, Denmark) Mouse monoclonal D33 1:400S-100 protein DAKO (Glostrup, Denmark) Rabbit anti-cow 1:400
Table II. Sequences of PCR primers.
Forward Reverse
KIT exon 95’-TCC TAG AGT AAG CCA GGG CTT-3’ 5’-TGG TAG ACA GAG CCT AAA CAT CC-3’
KIT exon 115’-CCT TTG CTG ATT GGT TTC GT-3’ 5’-AAA CAA AGG AAG CCA CTG GA-3’
KIT exon 135’-ACT GTC GCT GTA AAG ATG CT-3’ 5’-CTA GCA TTG CCA AAA TCA TA-3’
KIT exon 175’-CAT CAT TCA AGG CGT ACT TTT G-3’ 5’-TCA CAG GAA ACA ATT TTT ATC GAA-3’
PDGFRA exon 125’-AAG CTC TGG TGC ACT GGG ACT T-3’ 5’-ATT GTA AAG TTG TGT GCA AGG GA-3’
PDGFRA exon 185’-TAC AGA TGG CTT GAT CCT GAG T-3’ 5’-AGT GTG GGA GGA TGA GCC TG-3’
ANTICANCER RESEARCH 32: 923-938 (2012)
926
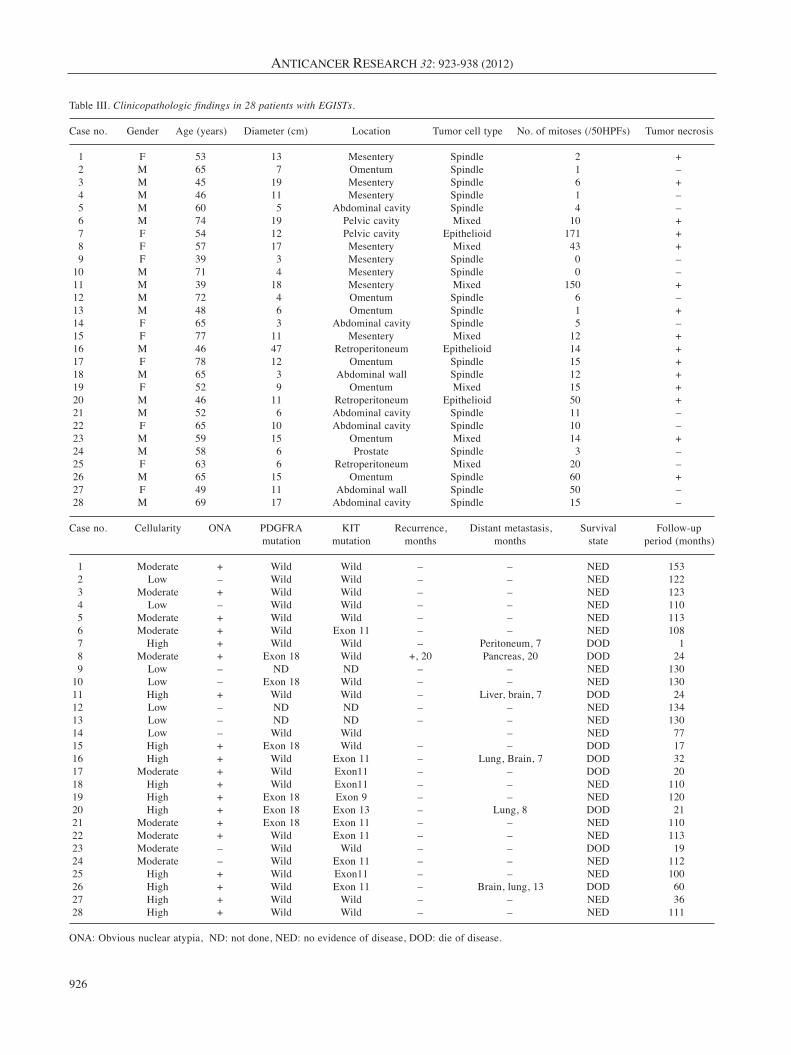
Table III. Clinicopathologic findings in 28 patients with EGISTs.
Case no. Gender Age (years) Diameter (cm) Location Tumor cell type No. of mitoses (/50HPFs) Tumor necrosis
1 F 53 13 Mesentery Spindle 2 +2 M 65 7 Omentum Spindle 1 –3 M 45 19 Mesentery Spindle 6 +4 M 46 11 Mesentery Spindle 1 –5 M 60 5 Abdominal cavity Spindle 4 –6 M 74 19 Pelvic cavity Mixed 10 +7 F 54 12 Pelvic cavity Epithelioid 171 +8 F 57 17 Mesentery Mixed 43 +9 F 39 3 Mesentery Spindle 0 –
10 M 71 4 Mesentery Spindle 0 –11 M 39 18 Mesentery Mixed 150 +12 M 72 4 Omentum Spindle 6 –13 M 48 6 Omentum Spindle 1 +14 F 65 3 Abdominal cavity Spindle 5 –15 F 77 11 Mesentery Mixed 12 +16 M 46 47 Retroperitoneum Epithelioid 14 +17 F 78 12 Omentum Spindle 15 +18 M 65 3 Abdominal wall Spindle 12 +19 F 52 9 Omentum Mixed 15 +20 M 46 11 Retroperitoneum Epithelioid 50 +21 M 52 6 Abdominal cavity Spindle 11 –22 F 65 10 Abdominal cavity Spindle 10 –23 M 59 15 Omentum Mixed 14 +24 M 58 6 Prostate Spindle 3 –25 F 63 6 Retroperitoneum Mixed 20 –26 M 65 15 Omentum Spindle 60 +27 F 49 11 Abdominal wall Spindle 50 –28 M 69 17 Abdominal cavity Spindle 15 –
Case no. Cellularity ONA PDGFRA KIT Recurrence, Distant metastasis, Survival Follow-up mutation mutation months months state period (months)
1 Moderate + Wild Wild – – NED 1532 Low – Wild Wild – – NED 1223 Moderate + Wild Wild – – NED 1234 Low – Wild Wild – – NED 1105 Moderate + Wild Wild – – NED 1136 Moderate + Wild Exon 11 – – NED 1087 High + Wild Wild – Peritoneum, 7 DOD 18 Moderate + Exon 18 Wild +, 20 Pancreas, 20 DOD 249 Low – ND ND – – NED 130
10 Low – Exon 18 Wild – – NED 13011 High + Wild Wild – Liver, brain, 7 DOD 2412 Low – ND ND – – NED 13413 Low – ND ND – – NED 13014 Low – Wild Wild – NED 7715 High + Exon 18 Wild – – DOD 1716 High + Wild Exon 11 – Lung, Brain, 7 DOD 3217 Moderate + Wild Exon11 – – DOD 2018 High + Wild Exon11 – – NED 11019 High + Exon 18 Exon 9 – – NED 12020 High + Exon 18 Exon 13 – Lung, 8 DOD 2121 Moderate + Exon 18 Exon 11 – – NED 11022 Moderate + Wild Exon 11 – – NED 11323 Moderate – Wild Wild – – DOD 1924 Moderate – Wild Exon 11 – – NED 11225 High + Wild Exon11 – – NED 10026 High + Wild Exon 11 – Brain, lung, 13 DOD 6027 High + Wild Wild – – NED 3628 High + Wild Wild – – NED 111
ONA: Obvious nuclear atypia, ND: not done, NED: no evidence of disease, DOD: die of disease.
the number of mitoses per 50 HPFs, 5 out of the 28 caseshad 0 or 1, 4 had 2-5, 4 had 6-10 and 15 had more than 10.The tumor cell components included spindle cells (64.3%),epithelioid cells (10.7%), and mixed cells (25%). Sixteencases (57.1%) of EGISTs had tumor necrosis and most werelarger than 10 cm with obvious nuclear atypia and highmitotic counts (>10/50 HPFs). In 7 patients, tumors hadmetastasized to distant organs. Eight patients died. The meanfollow-up period was 90±52 months (1-153 months). Theclinicopathological data of the patients are summarized inTable III.
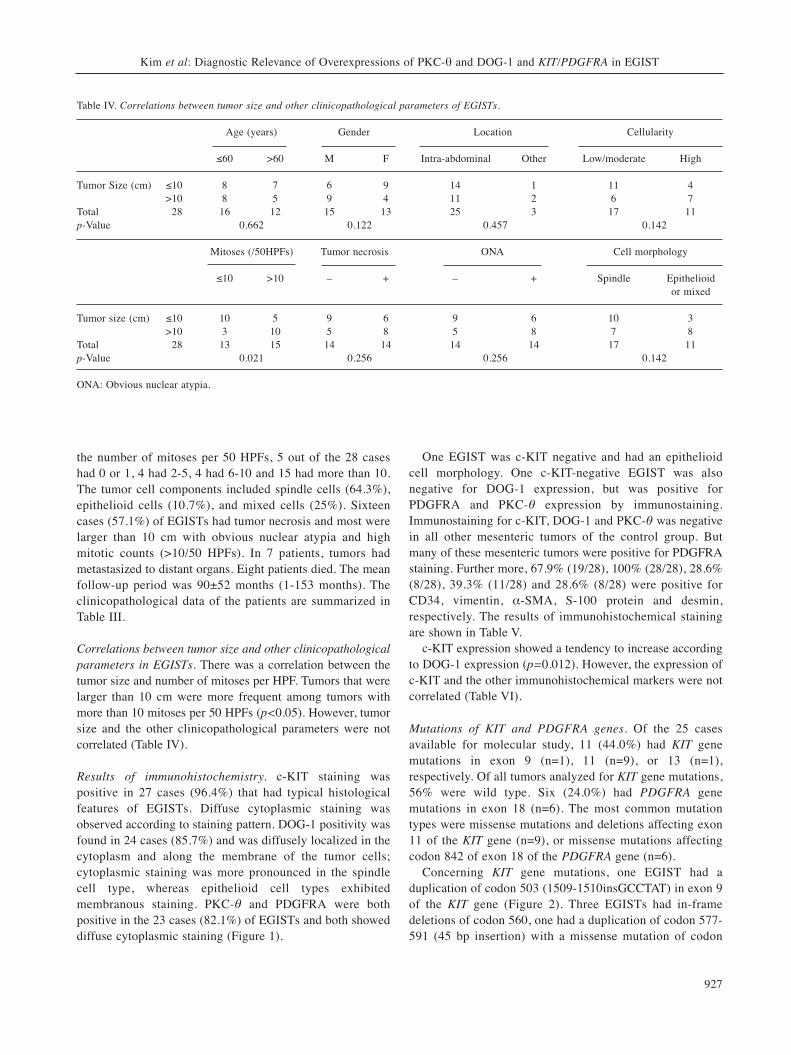
Correlations between tumor size and other clinicopathologicalparameters in EGISTs. There was a correlation between thetumor size and number of mitoses per HPF. Tumors that werelarger than 10 cm were more frequent among tumors withmore than 10 mitoses per 50 HPFs (p<0.05). However, tumorsize and the other clinicopathological parameters were notcorrelated (Table IV).
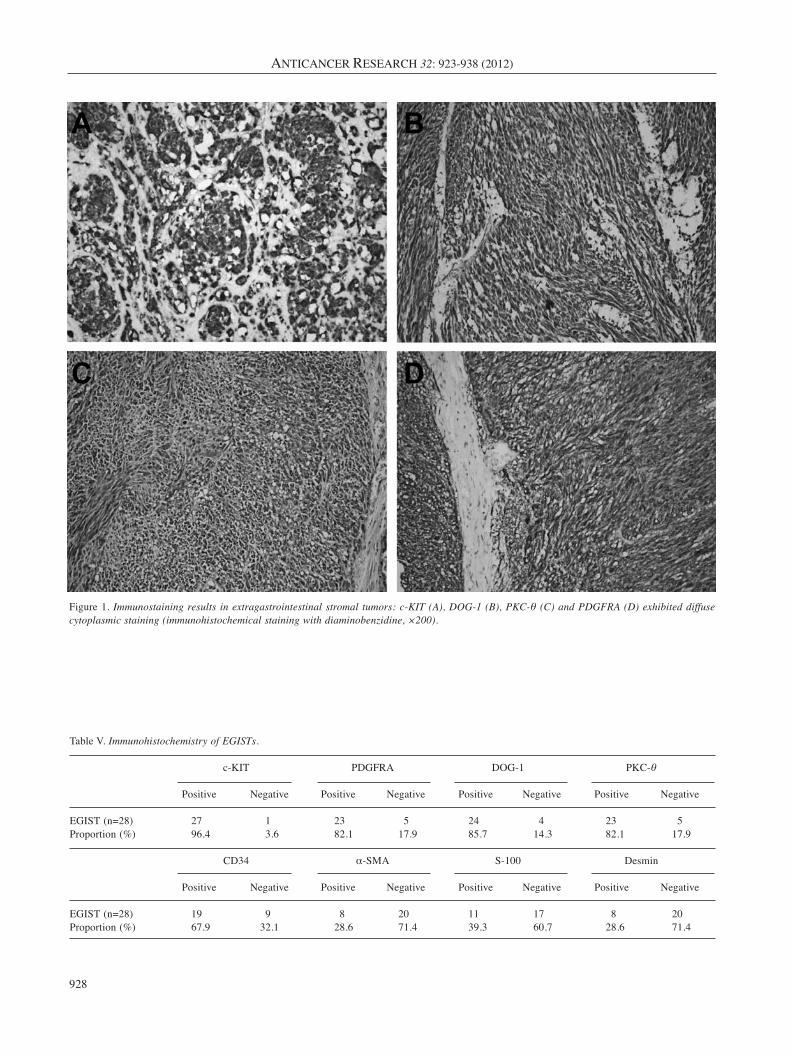
Results of immunohistochemistry. c-KIT staining waspositive in 27 cases (96.4%) that had typical histologicalfeatures of EGISTs. Diffuse cytoplasmic staining wasobserved according to staining pattern. DOG-1 positivity wasfound in 24 cases (85.7%) and was diffusely localized in thecytoplasm and along the membrane of the tumor cells;cytoplasmic staining was more pronounced in the spindlecell type, whereas epithelioid cell types exhibitedmembranous staining. PKC-θ and PDGFRA were bothpositive in the 23 cases (82.1%) of EGISTs and both showeddiffuse cytoplasmic staining (Figure 1).
One EGIST was c-KIT negative and had an epithelioidcell morphology. One c-KIT-negative EGIST was alsonegative for DOG-1 expression, but was positive forPDGFRA and PKC-θ expression by immunostaining.Immunostaining for c-KIT, DOG-1 and PKC-θ was negativein all other mesenteric tumors of the control group. Butmany of these mesenteric tumors were positive for PDGFRAstaining. Further more, 67.9% (19/28), 100% (28/28), 28.6%(8/28), 39.3% (11/28) and 28.6% (8/28) were positive forCD34, vimentin, α-SMA, S-100 protein and desmin,respectively. The results of immunohistochemical stainingare shown in Table V.
c-KIT expression showed a tendency to increase accordingto DOG-1 expression (p=0.012). However, the expression ofc-KIT and the other immunohistochemical markers were notcorrelated (Table VI).
Mutations of KIT and PDGFRA genes. Of the 25 casesavailable for molecular study, 11 (44.0%) had KIT genemutations in exon 9 (n=1), 11 (n=9), or 13 (n=1),respectively. Of all tumors analyzed for KIT gene mutations,56% were wild type. Six (24.0%) had PDGFRA genemutations in exon 18 (n=6). The most common mutationtypes were missense mutations and deletions affecting exon11 of the KIT gene (n=9), or missense mutations affectingcodon 842 of exon 18 of the PDGFRA gene (n=6).
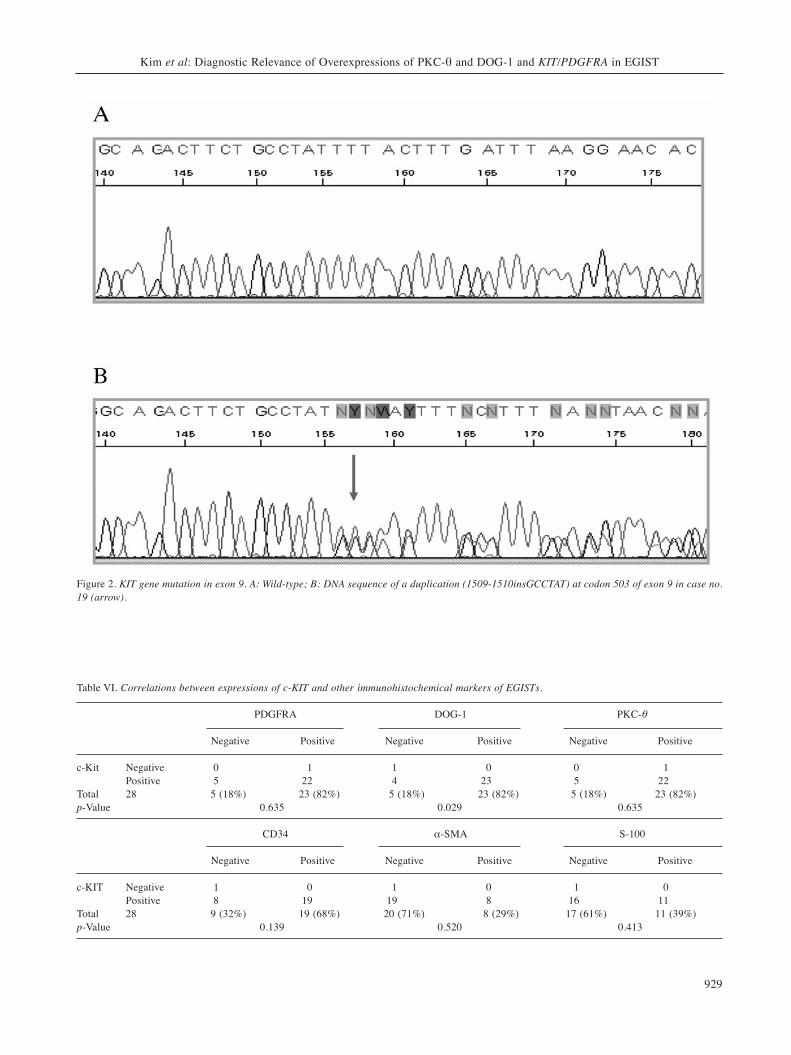
Concerning KIT gene mutations, one EGIST had aduplication of codon 503 (1509-1510insGCCTAT) in exon 9of the KIT gene (Figure 2). Three EGISTs had in-framedeletions of codon 560, one had a duplication of codon 577-591 (45 bp insertion) with a missense mutation of codon
Kim et al: Diagnostic Relevance of Overexpressions of PKC-θ and DOG-1 and KIT/PDGFRA in EGIST
927
Table IV. Correlations between tumor size and other clinicopathological parameters of EGISTs.
Age (years) Gender Location Cellularity
≤60 >60 M F Intra-abdominal Other Low/moderate High
Tumor Size (cm) ≤10 8 7 6 9 14 1 11 4>10 8 5 9 4 11 2 6 7
Total 28 16 12 15 13 25 3 17 11p-Value 0.662 0.122 0.457 0.142
Mitoses (/50HPFs) Tumor necrosis ONA Cell morphology
≤10 >10 – + – + Spindle Epithelioid or mixed
Tumor size (cm) ≤10 10 5 9 6 9 6 10 3>10 3 10 5 8 5 8 7 8
Total 28 13 15 14 14 14 14 17 11p-Value 0.021 0.256 0.256 0.142
ONA: Obvious nuclear atypia.
ANTICANCER RESEARCH 32: 923-938 (2012)
928
Table V. Immunohistochemistry of EGISTs.
c-KIT PDGFRA DOG-1 PKC-θ
Positive Negative Positive Negative Positive Negative Positive Negative
EGIST (n=28) 27 1 23 5 24 4 23 5Proportion (%) 96.4 3.6 82.1 17.9 85.7 14.3 82.1 17.9
CD34 α-SMA S-100 Desmin
Positive Negative Positive Negative Positive Negative Positive Negative
EGIST (n=28) 19 9 8 20 11 17 8 20Proportion (%) 67.9 32.1 28.6 71.4 39.3 60.7 28.6 71.4
Figure 1. Immunostaining results in extragastrointestinal stromal tumors: c-KIT (A), DOG-1 (B), PKC-θ (C) and PDGFRA (D) exhibited diffusecytoplasmic staining (immunohistochemical staining with diaminobenzidine, ×200).
Kim et al: Diagnostic Relevance of Overexpressions of PKC-θ and DOG-1 and KIT/PDGFRA in EGIST
929
Table VI. Correlations between expressions of c-KIT and other immunohistochemical markers of EGISTs.
PDGFRA DOG-1 PKC-θ
Negative Positive Negative Positive Negative Positive
c-Kit Negative 0 1 1 0 0 1Positive 5 22 4 23 5 22
Total 28 5 (18%) 23 (82%) 5 (18%) 23 (82%) 5 (18%) 23 (82%)p-Value 0.635 0.029 0.635
CD34 α-SMA S-100
Negative Positive Negative Positive Negative Positive
c-KIT Negative 1 0 1 0 1 0Positive 8 19 19 8 16 11
Total 28 9 (32%) 19 (68%) 20 (71%) 8 (29%) 17 (61%) 11 (39%)p-Value 0.139 0.520 0.413
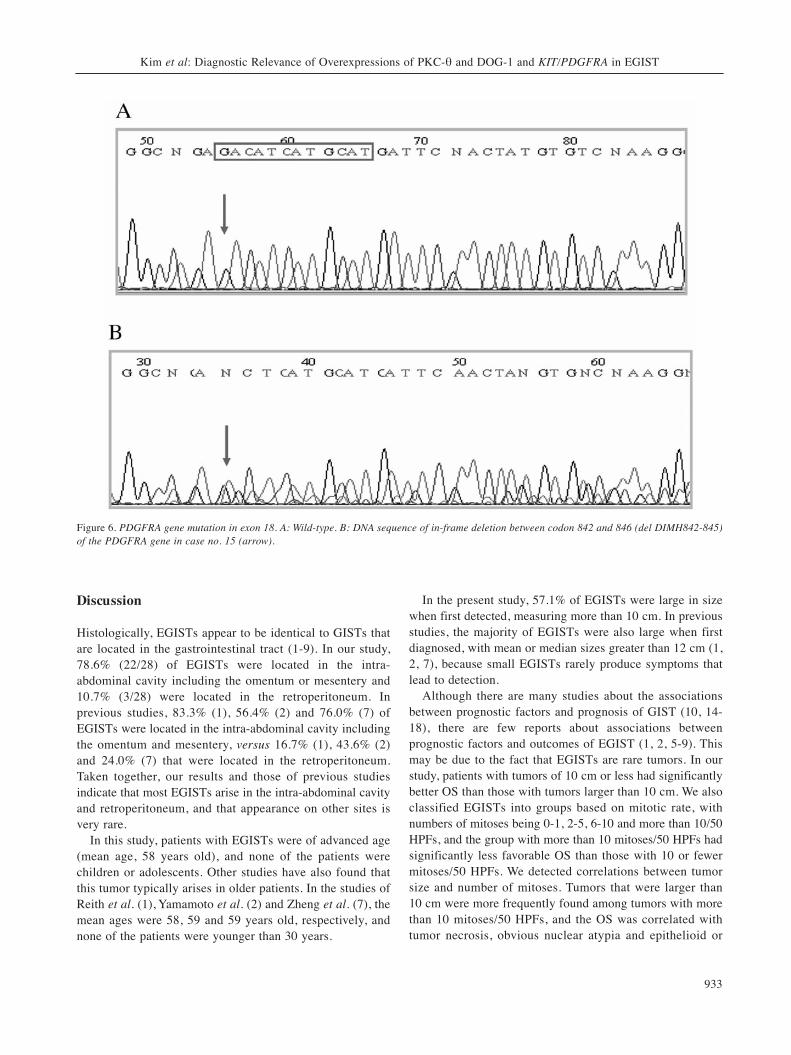
Figure 2. KIT gene mutation in exon 9. A: Wild-type; B: DNA sequence of a duplication (1509-1510insGCCTAT) at codon 503 of exon 9 in case no.19 (arrow).
ANTICANCER RESEARCH 32: 923-938 (2012)
930
Figure 3. Continued
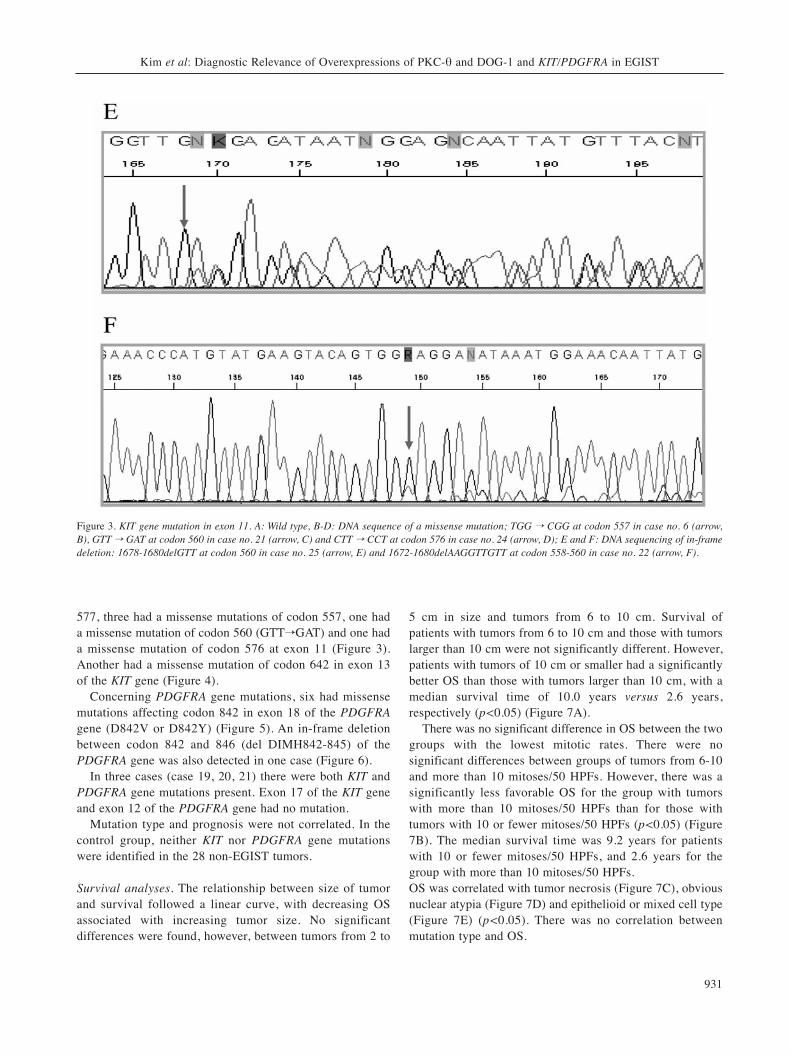
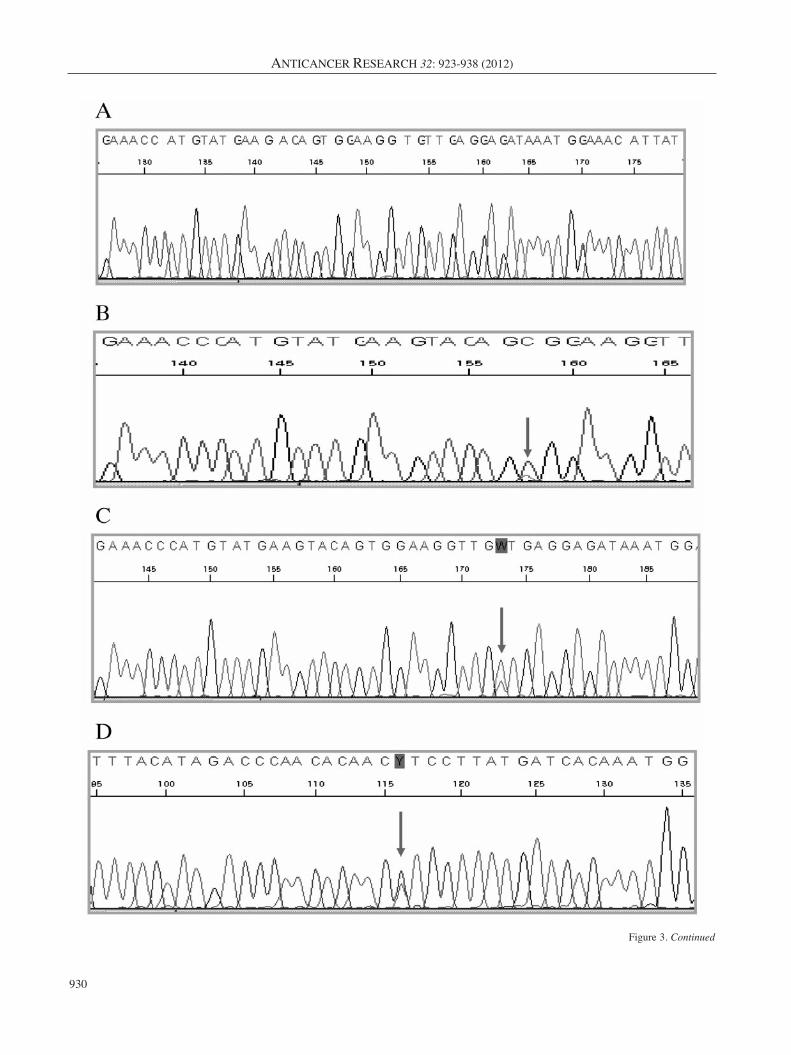
577, three had a missense mutations of codon 557, one hada missense mutation of codon 560 (GTT�GAT) and one hada missense mutation of codon 576 at exon 11 (Figure 3).Another had a missense mutation of codon 642 in exon 13of the KIT gene (Figure 4).
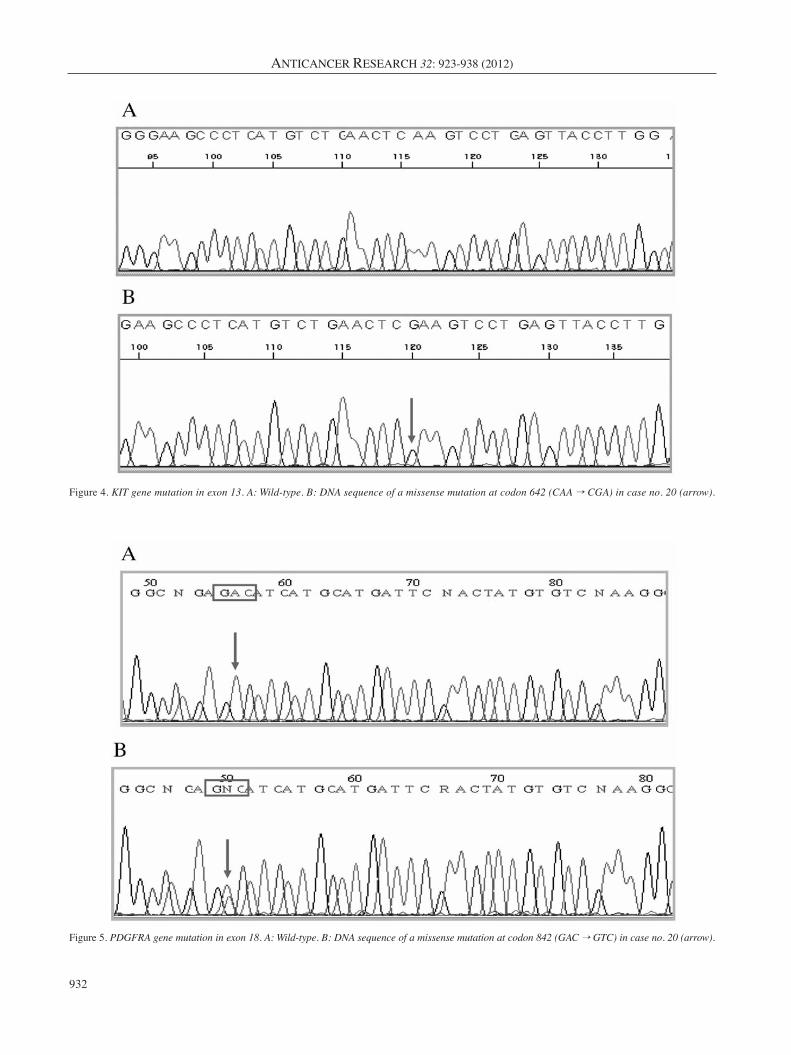
Concerning PDGFRA gene mutations, six had missensemutations affecting codon 842 in exon 18 of the PDGFRAgene (D842V or D842Y) (Figure 5). An in-frame deletionbetween codon 842 and 846 (del DIMH842-845) of thePDGFRA gene was also detected in one case (Figure 6).
In three cases (case 19, 20, 21) there were both KIT andPDGFRA gene mutations present. Exon 17 of the KIT geneand exon 12 of the PDGFRA gene had no mutation.
Mutation type and prognosis were not correlated. In thecontrol group, neither KIT nor PDGFRA gene mutationswere identified in the 28 non-EGIST tumors.
Survival analyses. The relationship between size of tumorand survival followed a linear curve, with decreasing OSassociated with increasing tumor size. No significantdifferences were found, however, between tumors from 2 to
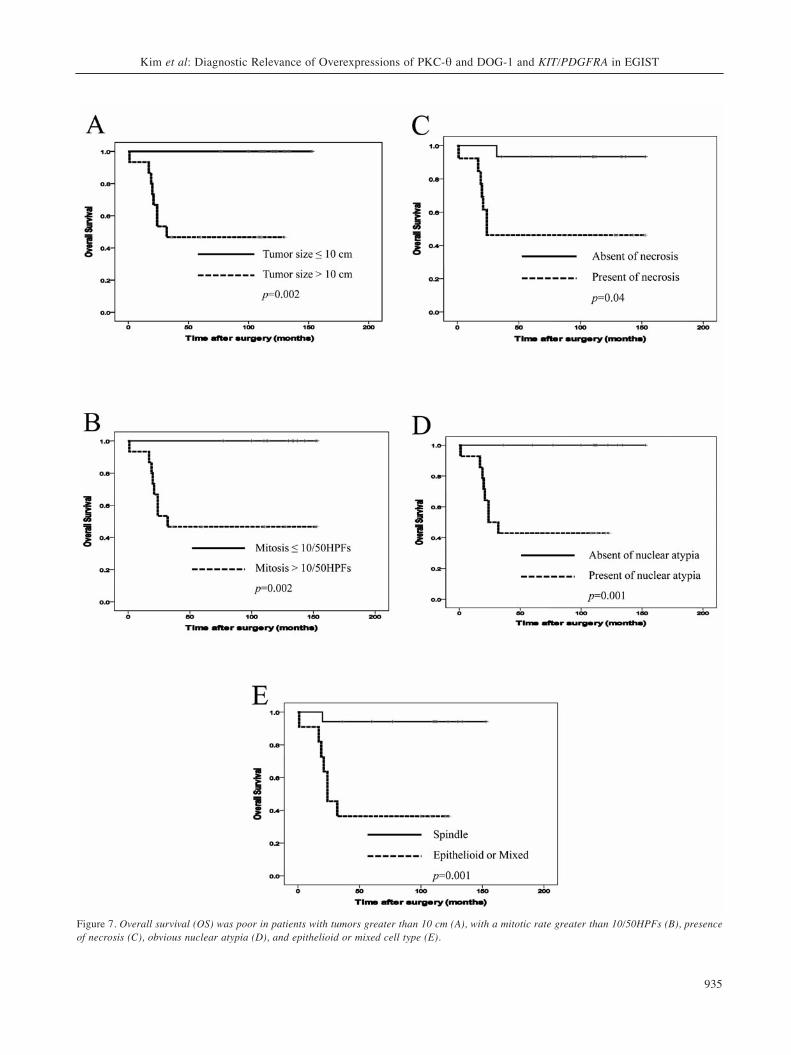
5 cm in size and tumors from 6 to 10 cm. Survival ofpatients with tumors from 6 to 10 cm and those with tumorslarger than 10 cm were not significantly different. However,patients with tumors of 10 cm or smaller had a significantlybetter OS than those with tumors larger than 10 cm, with amedian survival time of 10.0 years versus 2.6 years,respectively (p<0.05) (Figure 7A).
There was no significant difference in OS between the twogroups with the lowest mitotic rates. There were nosignificant differences between groups of tumors from 6-10and more than 10 mitoses/50 HPFs. However, there was asignificantly less favorable OS for the group with tumorswith more than 10 mitoses/50 HPFs than for those withtumors with 10 or fewer mitoses/50 HPFs (p<0.05) (Figure7B). The median survival time was 9.2 years for patientswith 10 or fewer mitoses/50 HPFs, and 2.6 years for thegroup with more than 10 mitoses/50 HPFs. OS was correlated with tumor necrosis (Figure 7C), obviousnuclear atypia (Figure 7D) and epithelioid or mixed cell type(Figure 7E) (p<0.05). There was no correlation betweenmutation type and OS.
Kim et al: Diagnostic Relevance of Overexpressions of PKC-θ and DOG-1 and KIT/PDGFRA in EGIST
931
Figure 3. KIT gene mutation in exon 11. A: Wild type, B-D: DNA sequence of a missense mutation; TGG � CGG at codon 557 in case no. 6 (arrow,B), GTT � GAT at codon 560 in case no. 21 (arrow, C) and CTT � CCT at codon 576 in case no. 24 (arrow, D); E and F: DNA sequencing of in-framedeletion: 1678-1680delGTT at codon 560 in case no. 25 (arrow, E) and 1672-1680delAAGGTTGTT at codon 558-560 in case no. 22 (arrow, F).
ANTICANCER RESEARCH 32: 923-938 (2012)
932
Figure 4. KIT gene mutation in exon 13. A: Wild-type. B: DNA sequence of a missense mutation at codon 642 (CAA � CGA) in case no. 20 (arrow).
Figure 5. PDGFRA gene mutation in exon 18. A: Wild-type. B: DNA sequence of a missense mutation at codon 842 (GAC � GTC) in case no. 20 (arrow).
Discussion
Histologically, EGISTs appear to be identical to GISTs thatare located in the gastrointestinal tract (1-9). In our study,78.6% (22/28) of EGISTs were located in the intra-abdominal cavity including the omentum or mesentery and10.7% (3/28) were located in the retroperitoneum. Inprevious studies, 83.3% (1), 56.4% (2) and 76.0% (7) ofEGISTs were located in the intra-abdominal cavity includingthe omentum and mesentery, versus 16.7% (1), 43.6% (2)and 24.0% (7) that were located in the retroperitoneum.Taken together, our results and those of previous studiesindicate that most EGISTs arise in the intra-abdominal cavityand retroperitoneum, and that appearance on other sites isvery rare.
In this study, patients with EGISTs were of advanced age(mean age, 58 years old), and none of the patients werechildren or adolescents. Other studies have also found thatthis tumor typically arises in older patients. In the studies ofReith et al. (1), Yamamoto et al. (2) and Zheng et al. (7), themean ages were 58, 59 and 59 years old, respectively, andnone of the patients were younger than 30 years.
In the present study, 57.1% of EGISTs were large in sizewhen first detected, measuring more than 10 cm. In previousstudies, the majority of EGISTs were also large when firstdiagnosed, with mean or median sizes greater than 12 cm (1,2, 7), because small EGISTs rarely produce symptoms thatlead to detection.
Although there are many studies about the associationsbetween prognostic factors and prognosis of GIST (10, 14-18), there are few reports about associations betweenprognostic factors and outcomes of EGIST (1, 2, 5-9). Thismay be due to the fact that EGISTs are rare tumors. In ourstudy, patients with tumors of 10 cm or less had significantlybetter OS than those with tumors larger than 10 cm. We alsoclassified EGISTs into groups based on mitotic rate, withnumbers of mitoses being 0-1, 2-5, 6-10 and more than 10/50HPFs, and the group with more than 10 mitoses/50 HPFs hadsignificantly less favorable OS than those with 10 or fewermitoses/50 HPFs. We detected correlations between tumorsize and number of mitoses. Tumors that were larger than 10 cm were more frequently found among tumors with morethan 10 mitoses/50 HPFs, and the OS was correlated withtumor necrosis, obvious nuclear atypia and epithelioid or
Kim et al: Diagnostic Relevance of Overexpressions of PKC-θ and DOG-1 and KIT/PDGFRA in EGIST
933
Figure 6. PDGFRA gene mutation in exon 18. A: Wild-type. B: DNA sequence of in-frame deletion between codon 842 and 846 (del DIMH842-845)of the PDGFRA gene in case no. 15 (arrow).

mixed cell type. The size, mitotic activity and cellularity ofEGISTs have been shown to be the most accurate predictorsof adverse outcome (1-3, 7). According to Reith et al. (1) andYamamoto et al. (2), the malignant potential of EGISTs maybe determined by tumor size, mitotic figures, necrosis, celltype and Ki-67 labeling indices. However, parameters andresults vary between studies (1-9).
Numerous antibodies have been produced and used for thepathological diagnosis of EGISTs. c-KIT is a 145 kDatransmembrane glycoprotein that serves as the receptor forstem cell factor (SCF) and exhibits tyrosine kinase activity(19). Binding of SCF to c-KIT results in receptorhomodimerization, activation of tyrosine kinase activity andphosphorylation of a variety of substrates (20). The mutant c-KIT isoforms demonstrated constitutive kinase activity, andtheir kinase domains were active even in the absence of SCF.In the present study, c-KIT was diffusely expressed in 96.4%of samples. c-KIT is overexpressed at a high frequency(100%) when detected by an immunohistochemical method,and was found to be a very good immunomarker fordiagnosing EGISTs in a 39-case study (2).
PKC is a serine/threonine kinase involved in the controlof cell proliferation, differentiation and motility (11, 12).PKC controls KIT/SCFR tyrosine kinase activity andmodulates cellular response to SCF. In this study, we foundthat PKC-θ was diffusely expressed in 82.1% of the cases.
The DOG-1 antibody, clone K9, worked well on paraffin-embedded tissues, showing high expression levels in EGISTs ofthe present study. DOG-1 staining was positive in 85.7% oftumor samples, and was diffusely localized in the cytoplasm andalong the membrane of the tumor cells. As described previously(13), cytoplasmic staining was more pronounced in the spindlecell type, whereas epithelioid cell types showed membranousstaining. DOG-1 expression was also correlated with c-KITexpression. DOG-1 and PKC-θ are overexpressed at a highfrequency (100%) when detected by an immunohistochemicalmethod and have been shown to be very good immunomarkersfor diagnosing GISTs (12, 13), but there have not been anystudies implicating these markers in EGISTs.
Our data suggest that the combined expressions of c-KIT,DOG-1 and PKC-θ are essential for diagnosis since thesemarkers can distinguish EGISTs from tumors with similarfeatures, such as other sarcomas or intra-abdominal desmoidtumors. However, KIT expression in EGISTs depends on theantibodies and the staining conditions used, includingdetection, dilution and antigen retrieval methods. It isdifficult to interpret the significance of weakly positive c-KIT staining and there are problematic tumors that have themorphological features of EGISTs, but do not exhibit c-KITexpression. Some pathologists have designated these as c-KIT-negative EGISTs (9). In these cases, diagnosis is verydifficult without genetic analysis. Our sample included onec-KIT-negative EGIST in which PDGFRA and PKC-θ were
valuable for making a definitive diagnosis. c-KIT-negativeEGISTs are more likely to have epithelioid cell morphology(9). In concordance with the previous study, our c-KIT-negative EGIST was indeed epithelioid in cell type.
Although some previous studies have demonstrated thatthe PDGFRA antibody is a sensitive and specificimmunomarker for GIST (21), there have not been anystudies of the role of this antibody in EGISTs. In the presentstudy, we found that PDGFRA expression was strong andsensitive, but was not a specific immunomarker for EGISTs.
In our molecular study, 44% of cases had KIT genemutations, and in most cases, the mutation was in exon 11.Our results are in partial agreement with those of Yamamotoet al. (2) and Zheng et al. (7). In the EGIST studies of Zhenget al. (7), KIT gene mutations were detected in 44% ofpatients with EGIST and all were exon 11 mutations. Thefour different regions in which KIT gene mutations are foundare exons 11, 9, 13, and 17, in order of high to lowfrequency. Most KIT gene mutations in EGISTs involve exon11, the juxtamembrane domain, which encodes a helicaldomain of KIT representing the inhibitory region regulatingKIT activation (2, 22, 23). In this study, 28.0% of EGISTsexhibited missense mutations in the KIT gene, and in all butone case, the mutation was in exon 11. As previouslyreported, missense mutations in KIT exon 11 are present in20% to 30% of EGISTs. They typically involve three codons,Trp557, Val559, and Val560 in the proximal part, and codonLeu576 in the distal part of exon 11 (1, 2, 7, 24). In thisstudy, one EGIST had a duplication of codons 577-591 inexon 11 of the KIT gene. Internal duplications of up to morethan 20 codons can be present in the distal part of KIT exon11. These relatively rare mutations often occur in EGISTsand are related to good prognosis (1, 24).
In this study, 8% of EGISTs (2/25) had deletions of theKIT gene; one had a deletion of Val560 and the other had adeletion of Lys558-Val560 of exon 11. In previous studies,the majority of deletions involved the proximal part of KITexon 11 and the deletions clustered between codons Gln550and Glu561 (1, 2, 7, 23, 25). It has been suggested that thelosses of Trp557, Lys558 and Val560, the most commondeletions in GISTs, are related to poor prognosis (26, 27).However, we found no correlation between KIT genemutation type and prognosis.
The presence of two different KIT gene mutationsaffecting the same exon has been previously reported (2, 17,18). In our study, one case had both a duplication and a pointmutation of exon 11 of the KIT gene. These rare mutationsmay reflect secondary changes that occurred during tumorprogression.
In the present study, 56% of EGISTs had wild-type KITgenes. In the studies of Antonescu et al. (28) and Wardelmannet al. (29), a majority of gastric GISTs had wild-type KITgenes. EGISTs may be subtypes with less frequent KIT gene
ANTICANCER RESEARCH 32: 923-938 (2012)
934
Kim et al: Diagnostic Relevance of Overexpressions of PKC-θ and DOG-1 and KIT/PDGFRA in EGIST
935
Figure 7. Overall survival (OS) was poor in patients with tumors greater than 10 cm (A), with a mitotic rate greater than 10/50HPFs (B), presenceof necrosis (C), obvious nuclear atypia (D), and epithelioid or mixed cell type (E).

mutations, although cell type was not correlated with thefrequency of KIT mutation in EGISTs (2).
The PDGFRA gene is similar in structure to other receptortyrosine kinases, such as KIT and FLT3 (Fms-like tyrosinekinase). Recent studies have described a gain-of-functionmutation of the PDGFRA gene in the juxtamembrane domain(exon 12) and tyrosine kinase II domain (exon 18) (2, 14,15). In this study, 24% of EGISTs had PDGFRA genemutations and all were exon 18 mutations. The mostcommon mutation type was a missense mutation affectingcodon 842 of exon 18. The other was an in-frame deletionbetween codon 842 and 846 (del DIMH842-845). Therewere no mutations in exon 12. In Zheng et al. (7), PDGFRAgene mutations were found in 12% of the 25 cases and allwere exon 18 mutations. According to their data, D842V atexon 18 is the most frequent mutation in the PDGFRA geneof EGISTs. In another study, mutations of the PDGFRA genewere found in exon 18 in 10% of cases, exon 12 in 2% ofcases, and exon 14 in 2% of cases (30). In our study, therewere no correlations between PDGFRA mutation andprognosis. The clinicopathological importance of PDGFRAgene mutations is still unclear. Further studies with largernumbers of EGISTs may be needed to determine therelationships between PDGFRA gene mutations andclinicopathological factors or biological behaviors.
In EGISTs and GISTs, KIT and PDGFRA gene mutationsare regarded as being reciprocally and mutually exclusive (2,16-18). PDGFRA gene mutations are present inapproximately 30% of KIT gene mutation-negative GISTcases (17, 18). However, in our study, KIT and PDGFRAgene mutations co-existed in three cases. The presence ofboth KIT and PDGFRA gene mutations was reported inanother recent study (5). It is not clear why the EGISTs inour sample had both KIT and PDGFRA gene mutations. Thismay be because both are gain-of-function mutations: one inthe juxtamembrane for KIT and the other in the activationloop for PDGFRA. The co-expression was not unexpectedbecause there is evidence that KIT and PDGFRA bothparticipate in the pathogenesis of EGISTs (21).
In conclusion, EGISTs have specific clinical behaviors.Immunohistochemical findings in EGISTs parallel those ofGISTs. Most EGISTs are c-KIT, DOG-1 and PKC-θ positive,but these immunostains are negative for other mesenchymaltumors. Therefore, these antigens are the most sensitive andspecific markers for confirming EGISTs. PKC-θ andPDGFRA immunostains are helpful markers for c-KIT-negative EGISTs. The parameters used for predicting theprognoses of patients with GISTs are generally applicable forthose with EGISTs. Survival analysis indicated that largetumor size (>10 cm), high mitotic rate (>10/50 HPFs), tumornecrosis, obvious nuclear atypia, and epithelioid or mixed celltype were significant predictors of survival. Our resultsshowed that the combination of these parameters helps to
predict aggressive tumor behavior and may be useful forpredicting the prognosis of patients with EGISTs.
The majority of gene mutations in EGISTs were identifiedin exon 11 of the KIT gene or exon 18 of the PDGFRA gene.The patterns of KIT and PDGFRA gene mutations in EGISTswere essentially similar to those in GISTs. From the contextof immunohistochemistry and molecular genetics, EGISTsmay be considered a special subtype of GISTs. Bothimmunohistochemical and molecular evaluations are usefulfor classifying tumors as EGISTs.
Acknowledgements
This work was supported by a grant from 2009 IN-SUNGFoundation for Medical Research (TA35), Seoul, South Korea.
References
1 Reith JD, Goldblum JR, Lyles RH and Weiss SW:Extragastrointestinal (soft tissue) stromal tumors: an analysis of48 cases with emphasis on histologic predictors of outcome.Mod Pathol 13: 577-585, 2000.
2 Yamamoto H, Oda Y, Kawaguchi K, Nakamura N, Takahira T,Tamiya S, Saito T, Oshiro Y, Ohta M, Yao T and Tsuneyoshi M:c-KIT and PDGFRA mutations in extragastrointestinal stromaltumor (gastrointestinal stromal tumor of the soft tissue). Am JSurg Pathol 28: 479-488, 2004.
3 Nakagawa M, Akasaka Y, Kanai T, Takabayashi T and MiyazawaN: Clinicopathological and immunohistochemical features ofextragastrointestinal stromal tumors: report of two cases. SurgToday 35: 336-340, 2005.
4 Lam MM, Corless CL, Goldblum JR, Heinrich MC, Downs-Kelly E and Rubin BP: Extragastrointestinal stromal tumorspresenting as vulvovaginal/rectovaginal septal masses: adiagnostic pitfall. Int J Gynecol Pathol 25: 288-292, 2006.
5 Kim JH, Boo YJ, Jung CW, Park SS, Kim SJ, Mok YJ, Kim SD,Chae YS and Kim CS: Multiple malignant extragastrointestinalstromal tumors of the greater omentum and results ofimmunohistochemistry and mutation analysis: a case report.World J Gastroenterol 13: 3392-3395, 2007.
6 Terada T: Primary multiple extragastrointestinal stromal tumorsof the omentum with different mutations of c-KIT gene. World JGastroenterol 14: 7256-7259, 2008.
7 Zheng S, Huang KE, Tao DY and Pan YL: Gene mutations andprognostic factors analysis in extragastrointestinal stromal tumorof a Chinese three-center study. J Gastrointest Surg 15: 675-681,2011.
8 Barros A, Linhares E, Valadão M, Gonçalves R, Vilhena B, GilC and Ramos C: Extragastrointestinal stromal tumors (EGIST): aseries of case reports. Hepatogastroenterology 58: 865-868, 2011.
9 Yamamoto H, Kojima A, Nagata S, Tomita Y, Takahashi S andOda Y: KIT-negative gastrointestinal stromal tumor of theabdominal soft tissue: a clinicopathologic and genetic study of10 cases. Am J Surg Pathol 35: 1287-1295, 2011.
10 Fletcher CD, Berman JJ, Corless C, Gorstein F, Lasota J, LongleyBJ, Miettinen M, O'Leary TJ, Remotti H, Rubin BP, ShmooklerB, Sobin LH and Weiss SW: Diagnosis of gastrointestinal stromaltumors: A consensus approach. Hum Pathol 33: 459-465, 2002.
ANTICANCER RESEARCH 32: 923-938 (2012)
936

11 Nishizuka Y: Intracellular signaling by hydrolysis ofphospholipids and activation of protein kinase C. Science 258:607-614, 1992.
12 Blay P, Astudillo A, Buesa JM, Campo E, Abad M, García-GarcíaJ, Miquel R, Marco V, Sierra M, Losa R, Lacave A, Braña A,Balbín M and Freije JM: Protein kinase C theta is highlyexpressed in gastrointestinal stromal tumors but not in othermesenchymal neoplasias. Clin Cancer Res 10: 4089-4095, 2004.
13 Espinosa I, Lee CH, Kim MK, Rouse BT, Subramanian S,Montgomery K, Varma S, Corless CL, Heinrich MC, Smith KS,Wang Z, Rubin B, Nielsen TO, Seitz RS, Ross DT, West RB,Cleary ML and van de Rijn M: A novel monoclonal antibodyagainst DOG1 is a sensitive and specific marker for gastrointestinalstromal tumors. Am J Surg Pathol 32: 210-218, 2008.
14 Corless CL, McGreevey L, Haley A, Town A and Heinrich MC:KIT mutations are common in incidental gastrointestinal stromaltumors one centimeter or less in size. Am J Pathol 160: 1567-1572, 2002.
15 Hirota S, Ohashi A, Nishida T, Isozaki K, Kinoshita K, ShinomuraY and Kitamura Y: Gain-of-function mutations of platelet-derivedgrowth factor receptor alpha gene in gastrointestinal stromaltumors. Gastroenterology 125: 660-667, 2003.
16 Bertolini V, Chiaravalli AM, Klersy C, Placidi C, Marchet S, BoniL and Capella C: Gastrointestinal stromal tumors - frequency,malignancy, and new prognostic factors: the experience of a singleinstitution. Pathol Res Pract 204: 219-233, 2008.
17 Lasota J and Miettinen M: KIT and PDGFRA mutations ingastrointestinal stromal tumors (GISTs). Semin Diagn Pathol 23:91-102, 2006.
18 Miettinen M and Lasota J: Gastrointestinal stromal tumors: reviewon morphology, molecular pathology, prognosis, and differentialdiagnosis. Arch Pathol Lab Med 130: 1466-1478, 2006.
19 Besmer P, Murphy JE, George PC, Qiu FH, Bergold PJ,Lederman L, Snyder HW Jr., Brodeur D, Zuckerman EE andHardy WD: A new acute transforming feline retrovirus andrelationship of its oncogene v-Kit with the protein kinase genefamily. Nature 320: 415-421, 1986.
20 Blume-Jensen P, Siegbahn A, Stabel S, Heldin CH andRönnstrand L: Increased KIT/SCF receptor induced mitogenicitybut abolished cell motility after inhibition of protein kinase C.EMBO J 12: 4199-4209, 1993.
21 Miselli F, Millefanti C, Conca E, Negri T, Piacenza C, PierottiMA, Tamborini E and Pilotti S: PDGFRA immunostaining canhelp in the diagnosis of gastrointestinal stromal tumors. Am JSurg Pathol 32: 738-743, 2008.
22 Hirota S, Isozaki K, Moriyama Y, Hashimoto K, Nishida T,Ishiguro S, Kawano K, Hanada M, Kurata A, Takeda M,Muhammad Tunio G, Matsuzawa Y, Kanakura Y, Shinomura Yand Kitamura Y: Gain-of-function mutations of c-kit in humangastrointestinal stromal tumors. Science 279: 577-580, 1998.
23 Longley BJ, Reguera MJ and Ma Y: Classes of c-KIT activatingmutations: proposed mechanisms of action and implications fordisease classification and therapy. Leuk Res 25: 571-576, 2001.
24 Miettinen M, Sobin LH and Lasota J: Gastrointestinal stromaltumors of the stomach: a clinicopathologic, immunohistochemical,and molecular genetic study of 1765 cases with long-term follow-up. Am J Surg Pathol 29: 52-68, 2005.
25 Corless CL, Fletcher JA and Heinrich MC: Biology ofgastrointestinal stromal tumors. J Clin Oncol 22: 3813-3825, 2004.
26 Wardelmann E, Losen I, Hans V, Neidt I, Speidel N, Bierhoff E,Heinicke T, Pietsch T, Büttner R and Merkelbach-Bruse S:Deletion of Trp-557 and Lys-558 in the juxtamembrane domain ofthe c-kit protooncogene is associated with metastatic behavior ofgastrointestinal stromal tumors. Int J Cancer 106: 887-895, 2003.
27 Martín J, Poveda A, Llombart-Bosch A, Ramos R, López-Guerrero JA, García del Muro J, Maurel J, Calabuig S, GutierrezA, González de Sande JL, Martínez J, De Juan A, Laínez N, LosaF, Alija V, Escudero P, Casado A, García P, Blanco R and BuesaJM; Spanish Group for Sarcoma Research: Deletions affectingcodons 557-558 of the c-KIT gene indicate a poor prognosis inpatients with completely resected gastrointestinal stromal tumors:a study by the Spanish Group for Sarcoma Research (GEIS). JClin Oncol 23: 6190-6198, 2005.
28 Antonescu CR, Sommer G, Sarran L, Tschernyavsky SJ, RiedelE, Woodruff JM, Robson M, Maki R, Brennan MF, Ladanyi M,DeMatteo RP and Besmer P: Association of KIT exon 9 mutationswith nongastric primary site and aggressive behavior: KITmutation analysis and clinical correlates of 120 gastrointestinalstromal tumors. Clin Cancer Res 9: 3329-3337, 2003.
29 Wardelmann E, Neidt I, Bierhoff E, Speidel N, Manegold C, FischerHP, Pfeifer U and Pietsch T: c-KIT mutations in gastrointestinalstromal tumors occur preferentially in the spindle rather than in theepithelioid cell variant. Mod Pathol 15: 125-136, 2002.
30 Hirota S and Isozaki K: Pathology of gastrointestinal stromaltumors. Pathol Int 56: 1-9, 2006.
Received December 28, 2011Revised January 27, 2012
Accepted January 30, 2012
Kim et al: Diagnostic Relevance of Overexpressions of PKC-θ and DOG-1 and KIT/PDGFRA in EGIST
937