
1
October 2017
Byron K. Lee MDProfessor of MedicineDirector of the EP LaboratoryDivision of CardiologyUniversity of California, San Francisco
Disclosures
Research Medtronic
Zoll
Apama
Consulting CardioNet
2
Secretary of Defense: Donald Rumsfeld
3
Importance
AF is the most common sustained arrhythmia in adults
Affects 4% of everyone over age 60
10% of everyone over age 80
Aging leads to atrial fibrosis which predisposes to AF
2
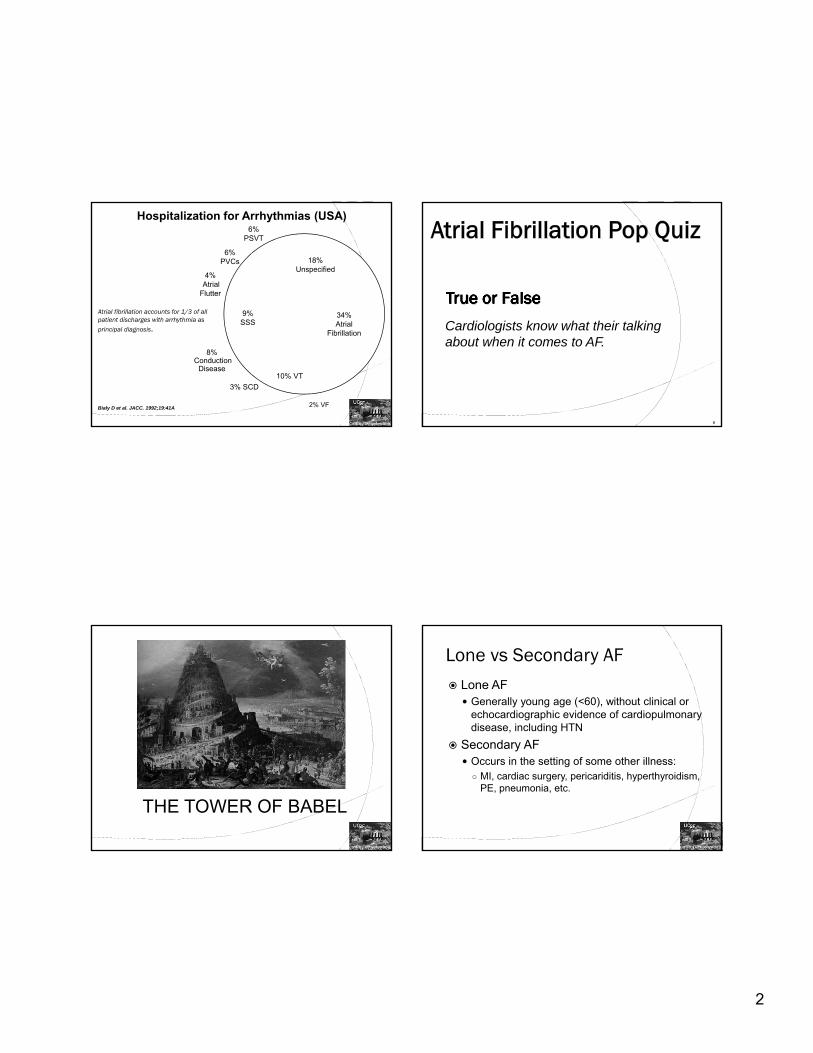
Atrial fibrillation accounts for 1/3 of all patient discharges with arrhythmia as
principal diagnosis.
2% VF
34% Atrial
Fibrillation
18% Unspecified
6% PSVT
6% PVCs
4%Atrial
Flutter
9% SSS
8%Conduction
Disease
3% SCD
10% VT
Hospitalization for Arrhythmias (USA)
Bialy D et al. JACC. 1992;19:41A
Cardiologists know what their talking about when it comes to AF.
6
THE TOWER OF BABEL
Lone vs Secondary AF Lone AF
Generally young age (<60), without clinical or echocardiographic evidence of cardiopulmonary disease, including HTN
Secondary AF Occurs in the setting of some other illness: ○ MI, cardiac surgery, pericariditis, hyperthyroidism,
PE, pneumonia, etc.

3
Classification of Atrial Fibrillation
Gallagher MM, Camm AJ. Classification of atrial fibrillation. PACE. 1992;20:1603-1605
With better treatment of HTN and valvular heart disease, AF incidence is decreasing.
10
Miyasaka, Y. et al. Circulation 2006;114:119-125
Incidence of Atrial Fibrillation in different age groups
Miyasaka, Y. et al. Circulation 2006;114:119-125
Overall and sex-specific trends in age-adjusted incidence of AF between 1980 and 2000 (age
adjustment to the 1990 US population)
4
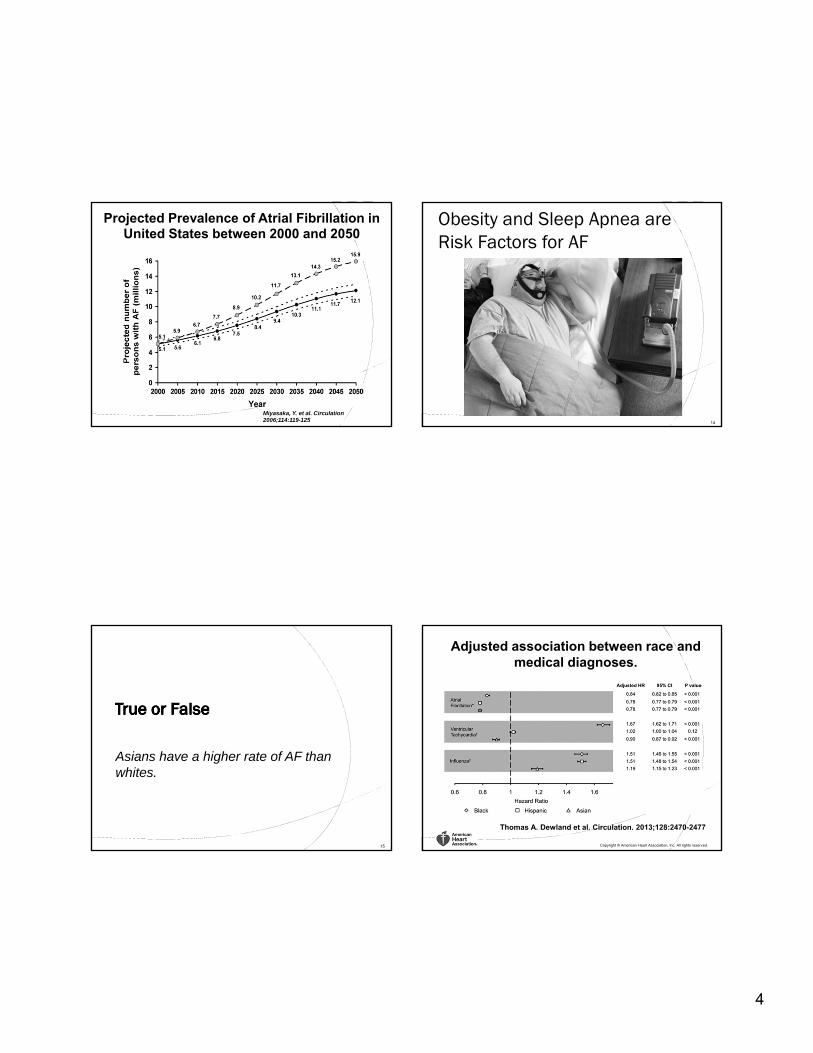
Miyasaka, Y. et al. Circulation 2006;114:119-125
Projected Prevalence of Atrial Fibrillation in United States between 2000 and 2050
Obesity and Sleep Apnea are Risk Factors for AF
14
Asians have a higher rate of AF than whites.
15
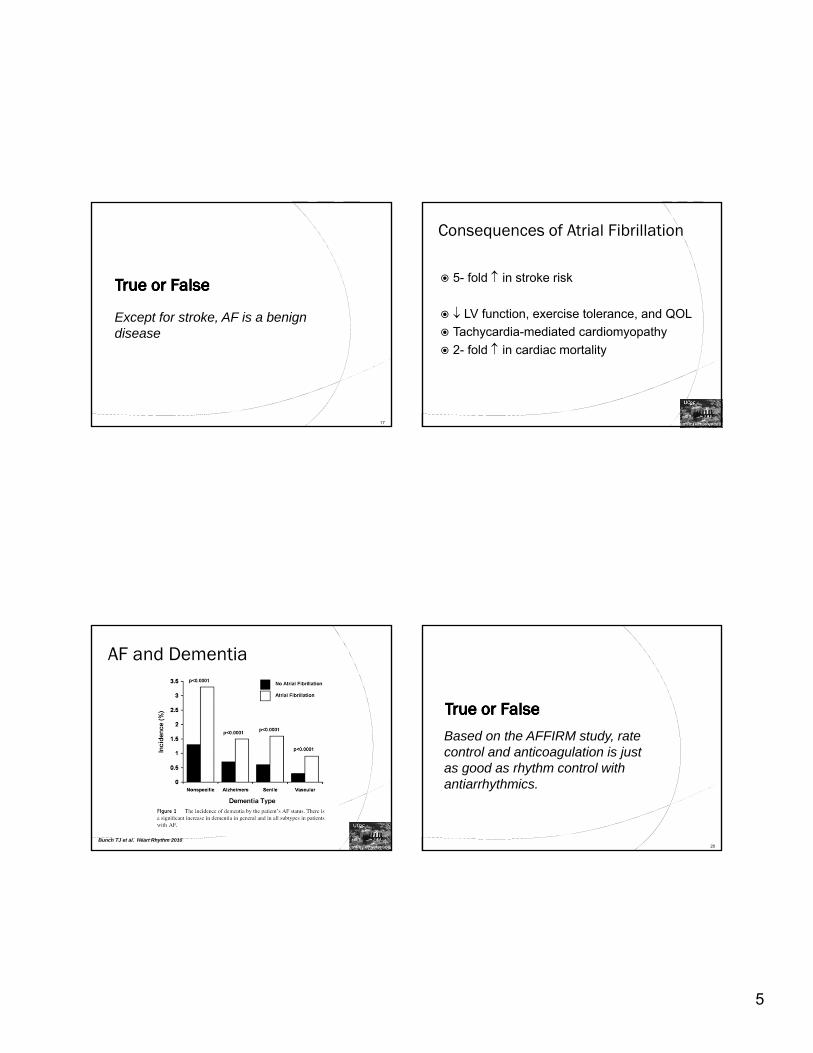
Adjusted association between race and medical diagnoses.
Thomas A. Dewland et al. Circulation. 2013;128:2470-2477
Copyright © American Heart Association, Inc. All rights reserved.
5
Except for stroke, AF is a benign disease
17
Consequences of Atrial Fibrillation
5- fold in stroke risk
LV function, exercise tolerance, and QOL
Tachycardia-mediated cardiomyopathy
2- fold in cardiac mortality
AF and Dementia
19
Bunch TJ et al. Heart Rhythm 2010
Based on the AFFIRM study, rate control and anticoagulation is just as good as rhythm control with antiarrhythmics.
20

6
The Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) Investigators. N Engl J Med 2002;347:1825-1833.
Cumulative Mortality from Any Cause in the Rhythm-Control Group and the Rate-Control Group. AF Symptoms
Feeling overtired or a lack of energy (most common)
Pulse that is faster than normal or changing between fast and slow and feels irregular
Shortness of breath
Heart palpitations (feeling like your heart is racing, pounding, or fluttering)
Trouble with everyday exercises or activities
Pain, pressure, tightness, or discomfort in your chest
Dizziness, lightheadedness, or fainting
Increased urination (using the bathroom more often)
1. http://www.hrsonline.org/Patient-Resources/Heart-Diseases-Disorders/Atrial-Fibrillation-
CHADS2 is an outdated approach to determine which patients need anticoagulation
23
Anticoagulation in AF: Who needs it?
CHADS 2 score:1
1 point for:CHF (or reduced systolic function), HTN, age ≥ 75 years, DM
2 points for:History of stroke or TIA
0: very low risk 1: low risk
2-3: moderate risk4-6: high risk
1. JAMA 2001;285:2864-2870

7
Adapted from Olesen JB. BMJ 2011;342:d124
CHA2DS2-VASc score
27
CHA2DS2-VASc scoreCHA2DS2-VASc Improves Risk Stratification of
AF Patients With a CHADS2 Score of 0–1
28
1 Year Follow-up
Person-years Events Stroke Rate (95% CI)
CHADS2 score=0 17,327 275 1.59 (1.41-1.79)
CHA2DS2-VASc=0 6919 58 0.84 (0.65-1.08)
CHA2DS2-VASc=1 6811 119 1.75 (1.46-2.09)
CHA2DS2-VASc=2 3347 90 2.69 (2.19-3.31)
CHA2DS2-VASc=3 250 8 3.20 (1.60-6.40)
CHADS2 score=1 22,945 1130 4.92 (4.65-5.22)
CHA2DS2-VASc=1 2069 40 1.93 (1.42-2.64)
CHA2DS2-VASc=2 8516 345 4.05 (3.65-4.50)
CHA2DS2-VASc=3 11,223 652 5.81 (5.38-6.27)
CHA2DS2-VASc=4 1137 93 8.18 (6.68-10.02)
Olesen JB.Tromb Haemost 2012;107:1172-1179

8
29
Lip et al. Journal of Internal Medicine 201530
Lip et al. Journal of Internal Medicine 2015
Amiodarone is a dangerous drug and it should be not be used first line to prevent AF.
31
AF Guidelines 2011

9
Ablation can cure AF.
33
Focal Atrial Fibrillation
Spontaneous Initiation of Atrial Fibrillation by Ectopic Beats Originating in the Pulmonary Veins
Michel Haïssaguerre, M.D., Pierre Jaïs, M.D., Dipen C. Shah, M.D., Atsushi Takahashi, M.D., Mélèze Hocini, M.D., Gilles Quiniou, M.D., Stéphane Garrigue, M.D., Alain Le Mouroux, M.D.,
Philippe Le Métayer, M.D., and Jacques Clémenty, M.D.
1998
Anatomic PV Isolation
Pappone, et al. JACC 2003

10
Cryoballoon (Arctic Front)
• Paroxysmal AF (STOP AF 69% success at 1 year
compared to drugs 7%)
• PV stenosis, phrenic nerve palsy (6%)
• Decreased risk of esophageal injury
Website of a Bay Area Hospital
38
“Treating Atrial fibrillation (AF) with ablation or pulmonary vein antral isolation, results in a complete cure from atrial fibrillation in more than 90% of patients.”
Long Term Success After 1 Ablation
39Ouyang et al. Circulation 2010
Long Term Success After 1-3 ablations
40Ouyang et al. Circulation 2010

11
Cappato et al. Circ Arrhythm Electrophysiol. 2010
Success Based on Type of Atrial Fibrillation
Complications CVA, TIA, air embolism Left sided atrial arrhythmias Pulmonary vein stenosis AV fistulae, femoral pseudoaneurysm Coronary artery occlusion Death (1/1000) Mechanical
Perforation○ During transseptal puncture- aorta, LA○ During ablation- LA appendage○ Atrio Esophageal Fistula
Phrenic nerve paralysis Valve damage
Who is a candidate for AF Catheter Ablation?
Paroxysmal Symptomatic
Failed antiarrhythmics or young and want to avoid meds
Persistent and Permanent Highly symptomatic
Poor hemodynamics
Tachycardia induced cardiomyopathy
Failed antiarrhythmics
If you fail PV isolation you will have to live with the symptoms of AF.
44

12
(b)
(c)
(d)
(e)(f)
1
(a)
Method #1
HOW TO STOP A RUNAWAY STAGE
2Method #2
(b)
(c)
(d)
(e)(f)
(a)
1
(a)
Method #1
HOW TO STOP A RUNAWAY STAGE
Complete AV Node Ablation Complete AV Node AblationPM

13
Complete AV Node Ablation
Yeung-Lai-Wah, 1991
Trohman, 1992
Olgin, 1993 54
61
32
9.7±4.7
24±8
87.3% 12±6
98%
98%
AUTHOR Pt No. LONG-TERMSUCCESS
F/U (months)
SYMPTIMPROV
97%
100%
84%
Jensen, 1995 50 1794% 88%
Surgical AF Ablation (MAZE) Procedure
Wolf et al. J Thorac Cardiovasc Surg.2005;130:797-802.
Video-assisted bilateral pulmonary vein isolation and left atrial appendage exclusion for atrial fibrillation
If you have a CHADS2VASc of 6+ and recurrent bleeding on anticoagulation, you’re out of luck.
51
Watchman Device to occlude Left Atrial Appendage
Holmes et al. PROTECT AF. Lancet 2009

14
PROTECT AF STUDYProvided Proof of Principle
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
DEVICE CONTROL
2.4%
1.6%
0.2%
1.9%
2.6%
3.5%
ISCHEMIC
HEMORRHAGIC
ALL
Device is non‐inferiorto warfarin in stroke
May provide analternative to warfarin
Conclusions:STROKE RATES(95% CI)
Thrombus after Watchman Implant
54Patel et al. Cardiol Resid Pract 2012
Percutaneous Epicardial Left Atrial Appendage Ligation
Bartus, et al. JACC 2013;62:108-18.
76 year old Caucasian man presents for routine device check
PMH: SSS, s/p DDD pacemaker, HTN, CAD
Pacer interrogation: 3 AF episodes – lasting 5, 15 and 90 minutes. Ventricular rate up to 130 bpm. Mean VR in AF 88 bpm.
Asymptomatic: Does not recall the episodes of AF
15
QuestionAsymptomatic AF on Cardiac Device lasting 90 minutes : a) Do nothing
b) Start ASA
c) Anticoagulate with warfarin or NOAC
TRENDS TrialAF Burden & Thromboembolic Events
Annualized Rate
(Stroke & TIA)
Annualized Rate
(Stroke only)
Zero burden 1.1% 0.5%
Low burden < 5.5 hours
1.1% 1.1%
High burden ≥ 5.5 hours
2.4% 1.8%
Glotzer TV, et al. Circ Arrhythm Electrophysiol. 2009;474-480.
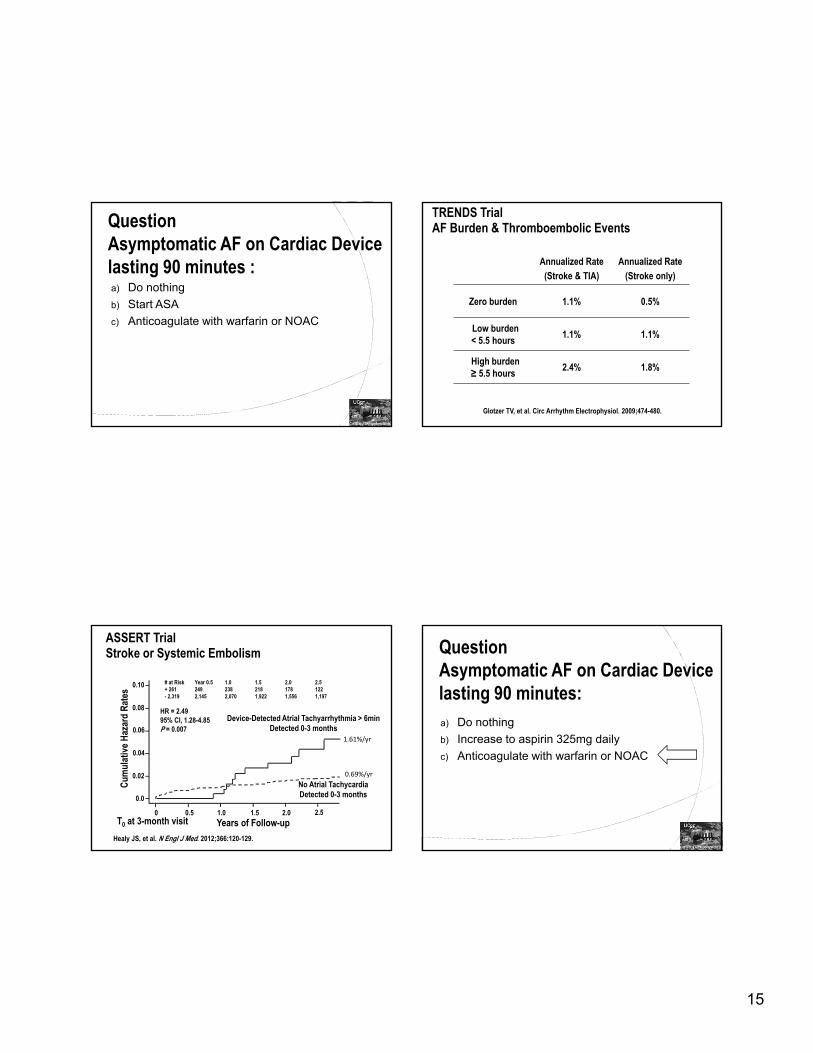
ASSERT TrialStroke or Systemic Embolism
Healy JS, et al. N Engl J Med. 2012;366:120-129.
Device-Detected Atrial Tachyarrhythmia > 6minDetected 0-3 months
No Atrial TachycardiaDetected 0-3 months
HR = 2.4995% CI, 1.28-4.85P = 0.007
# at Risk Year 0.5 1.0 1.5 2.0 2.5+ 261 249 238 218 178 122- 2,319 2,145 2,070 1,922 1,556 1,197
Years of Follow-upT0 at 3-month visit
Cum
ulat
ive
Haz
ard
Rat
es
0 0.5 1.0 1.5 2.0 2.5
0.0
0.02
0.04
0.06
0.08
0.10
0.69%/yr
1.61%/yr
QuestionAsymptomatic AF on Cardiac Device lasting 90 minutes: a) Do nothing
b) Increase to aspirin 325mg daily
c) Anticoagulate with warfarin or NOAC

16
90 year old frail Asian woman is found to have new onset AF Presentation: New palpitations and found on ECG
to have AF at 85 bpm
PMH: HTN, DM
Meds: Toprol XL
Echo: LVH, Sclerotic AV, EF 66%
a) Start aspirin 81 mg daily
b) Start aspirin 325mg daily
c) Adjusted dose warfarin INR 2-3
d) Start NOAC
90 year old frail Asian woman found to have new onset AF
Date of download: 4/14/2015
From: Warfarin Use among Ambulatory Patients with Nonvalvular Atrial Fibrillation: The AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study
Ann Intern Med. 1999;131(12):927-934. doi:10.7326/0003-4819-131-12-199912210-00004
Prevalent warfarin use by age among 11 082 ambulatory patients with nonvalvular atrial fibrillation and no identified contraindications to warfarin therapy.Numbers in parentheses represent the number of patients in the denominator of each category. Error bars represent upper 95% confidence limits.
Figure Legend:
Copyright © American College of Physicians. All rights reserved.64
ATRIA Study Data Singer et al. Annals of Internal Medicine 2009

17
a) Start aspirin 81 mg daily
b) Start aspirin 325mg daily
c) Adjusted dose warfarin INR 2-3
d) Start NOAC
90 year old frail Asian woman found to have new onset AF
Apixiban
88 year old frail Black woman found to have new onset AF PMH: HTN, GERD
Meds: Metoprolol XL 25mg daily, lisinopril 10mg daily, ASA 81mg daily
Upon further questioning you find out that she has mild Parkinson’s disease with 4 mechanical falls over the past year. No head injury
No LOC.
a) Start aspirin 81 mg daily
b) Start aspirin 325mg daily
c) Start aspirin and plavix
d) Start warfarin or NOAC
88 year old frail Black woman found to have new onset AF and frequent falls
Estimated that a patient had to fall 295x per year for the risk of intracranial hemorrhage to outweigh the benefit of warfarin!
68

18
a) Start aspirin 81 mg daily
b) Start aspirin 325mg daily
c) Start aspirin and plavix
d) Start warfarin or NOAC
88 year old frail Black woman found to have new onset AF and frequent falls
Summary: AF Truths Cardiologists do not always know what their talking
about when it comes to AF.
Despite better treatment of HTN and valvular heart disease, AF incidence is still increasing.
AF is not a benign disease. It causes stroke, decreased EF, adverse symptoms, and possibly dementia.
Based on the AFFIRM study, rate control and anticoagulation is just as good as rhythm control with antiarrhythmics only for asymptomatic or minimally symptomatic patients.
70
Summary: AF Truths CHADS2 should be replaced by CHADS2VASc to
determine which patients need anticoagulation
Amiodarone is a potentially dangerous drug and but should be used first line to prevent AF in patients with LVH.
Ablation cannot cure AF.
If you fail PV isolation you do not have to live with the symptoms of AF.
For patients who bleed on AC, LA appendage closure is an option.
71
Summary: AF Truths AC for high CHADS2VASc patients even if AF is
asymptomatic and discovered by an implantable device
Elderly patients are more likely to benefit from AC for AF
Patients need to fall 295x per year before the risk of intracranial bleeds outweigh the benefit of AC to prevent ischemic stroke.
72

19
UCSF Cardiac Electrophysiology
Dr. Nitish Badhwar
Dr. Edward Gerstenfeld
Dr. Henry Hsia
Dr. Byron Lee
Dr. Randy Lee
Dr. Gregory Marcus
Dr. Joshua Moss
Dr. Jeffrey Olgin
Dr. Melvin Scheinman
Dr. Zian Tseng
Dr. Vasanth Vendantham
73
MD Referral Coordinator:Ms. Deanna Galvan415-476-8237
74
Hope I did Not Lose You
Laser Balloon Ablation
Compliant Balloon
Visualization of PV to avoid stenosis
Avoid use of Imaging of LA
Phrenic nerve palsy
AF Burden and Risk of StrokeAF Burden value Hazard Ratio 95% Confidence
IntervalP value
< 5 vs. > 5 min 1.76 1.02‐3.02 p=0.041
< 1 vs. > 1 hr 2.11 1.22 to 3.64 p=0.008
< 6 vs. > 6 hr 1.74 0.96 to 3.41 p=0.067
< 12 vs. > 12 hr 1.72 0.92 to 3.22 p=0.090
< 23 vs. > 23 hr 1.44 0.69 to 3.01 p=0.332

20
Atrial fibrillation
Valvular AF*
VKA
Yes
No antithrombotic therapy
Yes
0
* Includes rheumatic valvular AF, hypertrophic cardiomyopathy, etc.
** Antiplatelet therapy with aspirin plus clopidogrel, or – less effectively – aspirin only, may be considered in patients who refuse any OAC.
Colour: CHA2DS2‐VASc score; green = 1, blue = 2, red = ≤2. Line: Solid: best option; Dashed: alternative option. If absolute contraindications to any OAC or anti‐platelet therapy, left atrial appendage closure device can be considered.AF = atrial fibrillation; CHA2DS2‐VASc = see text; HAS‐BLED = see text; NOAC = novel anticoagulants; VKA = vitamin K antagonist.
1** ≥2
NOAC
Oral anticoagulant therapy
Assess bleeding risk (HAS‐BLED score)Consider patient values and preferences
No (i.e. non‐valvular AF)
Assess risk of stroke (CHA2DS2‐VASc score)
No
< 65 years and lone AF (including females)
Choice of Anticoagulant
Eur Heart J 2012;33:2719‐2747
Pulmonary Vein Isolation
Lasso Catheter
Ablation Catheter
51 yo fireman presents with newly diagnosed asymptomatic persistent AF. With CHADS2 and CHADS2VASc of zero, we can externally cardiovert and put him on ASA 325 mg daily.
79
External CV
• Most thrombi in atrial fibrillation arise from the left atrial appendage
• Cardioversion can reduce left atrial appendage function
-- Even after conversion from AF to sinus
• The pericardioversion is a particularly pro-thrombotic time
-- Regardless of mode: DC/ electrical, pharmacologic, spontaneous
• During and after cardioversion:1, 2
-- Anticoagulation for at least 4 weeks
-- Applies even to those who would otherwise not require anticoagulation 1. JACC 2006;48:e149-246
2. Chest 2004;126:429S-456

21
Final Word on Nutritional Studies
It's a relief to know the truth after all those conflicting reports.
1. The Japanese eat very little fatand suffer fewer heart attacks than Americans.
2. The Mexicans eat a lot of fatand suffer fewer heart attacks than Americans.
81
Final Word on Nutritional Studies
3. The Chinese drink very little red wineand suffer fewer heart attacks than Americans.
4. The Italians drink a lot of red wineand suffer fewer heart attacks than Americans.
5. The Germans drink a lot of beers and eat lots of sausages and fats and suffer fewer heart attacks than Americans.
82
Final Word on Nutritional Studies
1. Eat and drink what you like.
2. Speaking English is apparently what kills you.
83
Conclusions:
SECTION HEADING
84







