dr tristan gr dyer rcsed fellow in pre-hospital emergency medicine
TRANSCRIPT
What Can We Do For The Patient?
Dr Tristan GR DyerRCSEd Fellow in Pre-hospital Emergency Medicine

Aims
To discuss methods of ventilation To discuss mechanical ventilation To introduce some difficult patient
groups that make ventilation more challenging
To look at future tools to aid ventilatory strategies

How Can We Ventilate The Patient?
Let the patient do it themselves! Manually Mechanically

Self-Ventilation
Deliver oxygen Work with the patient to optimise
their position Analgesia Therapeutic interventions (e.g.
drugs)

Indications for Ventilatory Support
Failure to Ventilate Failure to Oxygenate

Manual Ventilation
Manual Ventilation
Can be used with basic and advanced airway adjuncts.
BUT Ties operator up! Inaccurate tidal volumes. Tendency for operator to hyperventilate
(the patient!) May not be able to effectively ventilate
the patient. Risk of aspiration.

Predictors for Difficult Manual Ventilation

Mechanical Ventilation

How does it work?
Intermittent application of positive pressure to the upper airway.
Inspiration – gas flows into alveoli until the alveolar pressure equals the upper airway pressure.
Expiration – positive airway pressure is removed/decreased so the gradient reverses and gas flows out of the alveoli.
Pre-hospital Mechanical Ventilation
Patient has to be anaesthetised or crash intubation.
BUT Delivers 100% FiO2
Accurate tidal volumes. Accurate respiratory rate. Alarms to warn of emergencies
developing. Allows inline capnography. Frees up the operator.

Modes of Ventilation
Controlled Mechanical Ventilation Assist-Control Ventilation Intermittent Mandatory Ventilation Pressure Support Ventilation Pressure Control Ventilation Inverse I:E Ratio Ventilation

Controlled Mechanical VentilationCMV

Patient Factors To Optimise Ventilation
Ensure adequate sedation and paralysis
Patient position Clear secretions Treat underlying pathology

Basic Settings
Respiratory Rate 10-12 breaths/min. Tidal Volume 6-8 ml/Kg.
Aim to balance adequate ventilation with risk of pulmonary barotrauma and volutrauma at inflation pressures of >35-40 cm H2O.
Lower mean airway pressures (<20-30 cm H2O) can help preserve cardiac output and V/Q relationships.
May build TV up to 10ml/Kg.

Advanced Ventilators

Allow for...

Positive End-Expiratory Pressure(PEEP)
Used to improve a symptomatic decrease in the Functional Residual Capacity that causes hypoxaemia.
Provided by an extra valve applied to the breathing circuit or within the ventilator.

Pulmonary Effects of PEEP
In patients with a reduced lung volume, PEEP stabilizes and expands
partially collapsed alveoli.
This... Increases FRC and tidal ventilation Improves lung compliance Corrects V/Q abnormalities

Adverse Pulmonary Effects
Worse at levels >20 cm H20. Barotrauma Worse with underlying lung disease,
high rate of breaths, large tidal volumes and young age.

Adverse Non-Pulmonary Effects
Transmission of elevated airway pressure to the contents of the chest.
Reduced cardiac output. Elevated central venous pressure.

PEEP Settings
Starting PEEP 5-8 cm H2O used to compensate for the reduced FRC in anaesthetised patients.
Add in increments of 5 cm H2O up to 15 cm H2O.
Aim to improve oxygen saturations.

Lung Protective Strategy
Low Tidal Volume Low Airway Pressure Modest PEEP

Difficult Patient Groups

Trauma


Asthmatics

Pregnant

Bariatric

Elderly

Children

The Future
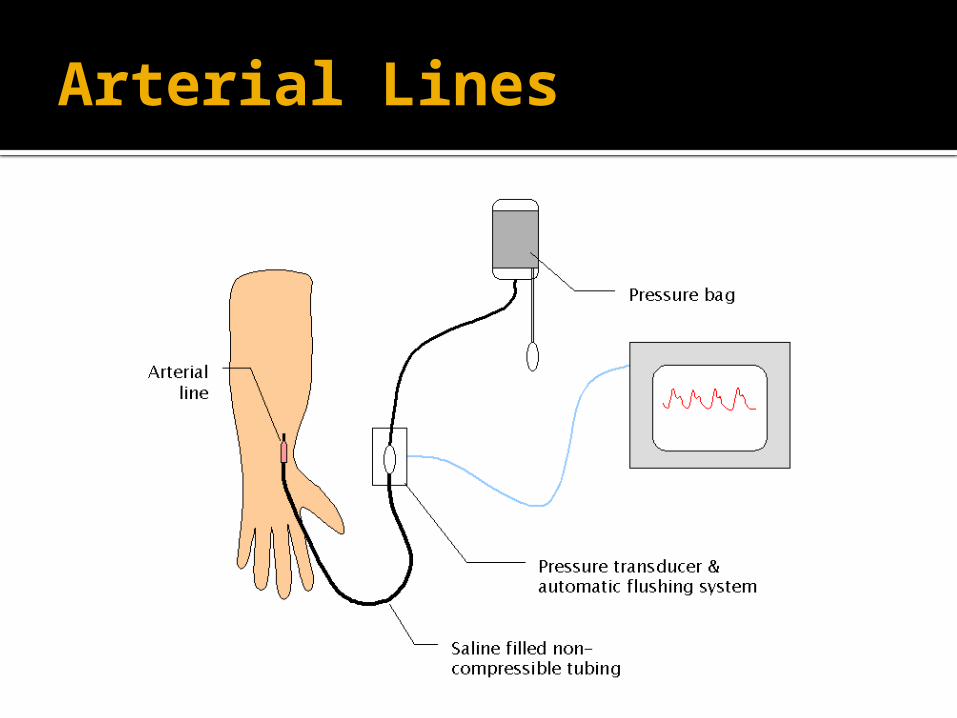
Arterial Lines

iSTAT

Portable Ultrasound

Inotropes

Any Questions?

Summary
Discussed means of ventilation Focused on mechanical ventilation Talked about difficult patient groups Looked at future adjuncts that may
help with ventilatory support