edema leyi gu renal division, renji hospital. definition expansion of the interstitial (间质)...
TRANSCRIPT
EDEMAEDEMA
Leyi Gu
Renal Division, Renji Hospital
DEFINITION
• Expansion of the interstitial (间质) fluid volume.
• Weight gain precedes overt edema
• Massive and generalized edema is called anasarca(全身性水肿)
• Pitting (压凹性 ) and non-pitting (非压凹性 ) edema
Schroth BE, JAAPA 2005 11

Edema
Pitting edemaPitting edema Non-pitting edemaNon-pitting edema

Anatomy and pathophysilolgy
• 1/3 of total body water is extracellular space, and 2/3 is intracellular space;
• Extracellular space is composed of the intravascular plasma volume (25%) and the extravascular interstitial spaces (75%);
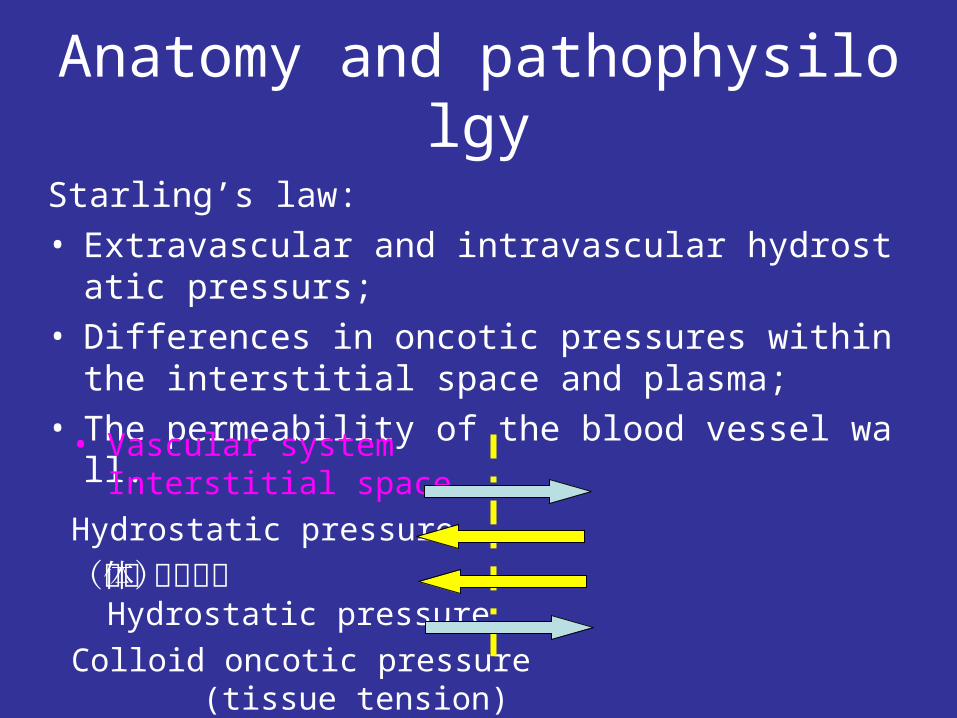
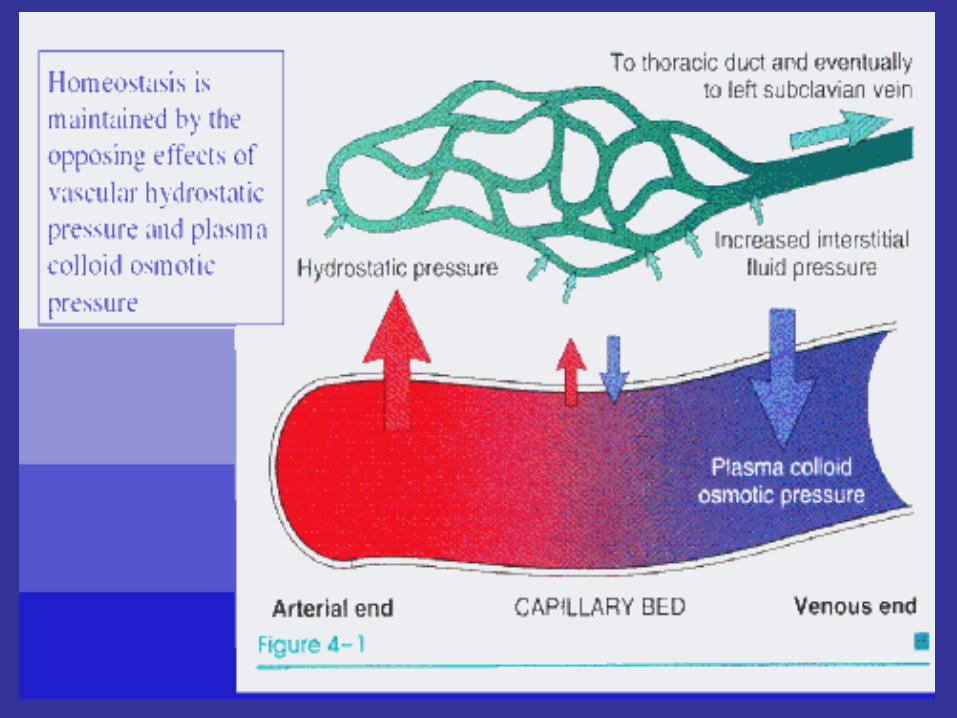
Starling’s law:
• Extravascular and intravascular hydrostatic pressurs;
• Differences in oncotic pressures within the interstitial space and plasma;
• The permeability of the blood vessel wall.
Anatomy and pathophysilolgy
• Vascular system Interstitial space
Hydrostatic pressure
(流体静水压) Hydrostatic pressure
Colloid oncotic pressure (tissue tension)
(胶体渗透压) Colloid oncotic pressure

Reduced Plasma Osmotic Pressure
Albumin is the serum protein MOST responsible for the maintenance of colloid osmotic pressure
A decrease in osmotic pressure can result from increased protein loss or decreased protein synthesis

Capillary Damage
• Damage to the capillary endothelium• Increase its permeability and permits the transfer of protein into interstitial compartment• Injury agents
Drugs Viral/bacterial agents
Thermal/mechanical trauma Immune• Responsible for inflammatory edema• Nonpitting localized redness and tenderness

Clinical Causes of Edema
Systemic edema
• Congestive heart failure• Cirrhosis • Nephrotic syndrome/other
hypoalbuminemia• Drug-induced • Idiopathic
Localized edema
• Venous/lymphatic
obstruction

Systemic EdemaCongestive heart failure

Congestive heart failure
• Left-sided heart failure: shortness of breath with exertion and when lying down at night (orthophea, 端坐呼吸 ) -- pulmonary edema
• Right-sided heart failure: swelling in the legs and feet --peripheral edema
•The physician examining a patient who has congestive heart failure with fluid retention looks for certain signs: pitting edema; rales in the lungs, a gallop rhythm and distended neck veins.

Systemic Edema

Nephrotic Syndrome/Hypoalbuminemic states
• The primary alteration: decreased colloid
oncotic pressure protein loss in the urine severe nutritional deficiency
protein loss enteropathy congenital hypoalbuminemia
liver cirrhosis
• Promotes fluid move into the interstitium
• Causes hypovolemia salt/water retention activation RAA axis etc
Idiopathic Edema
• Diurnal alterations in weight occurring with
orthostatic retention of sodium and water• Increase in capillary permeability
fluctuate in severity
aggravated by hot weather• Reduction in plasma volume in this condition with secondary activation of the RAA system
Drug-induced edema
Nonsteroidal anti-inflammatory drugs
Antihypertensive agents Direct arterial/arteriolar vasodilators
Calcium channel antagonists a-Adrenergic antagonists
Steroid hormones Glucocorticoids Anabolic steroids Estrogens Progestines
Cyclosporine
Growth hormone
Immunotherapies Interleukin 2 OKT3 monoclonal antibody
Localized edema
• Inflammation
• Venous/lymphatic obstruction
• Chronic lymphangitis
• Resection of regional lymph nodes
• Filariasis ( 丝虫病 )
Diagnosis
• Of particular importance is excluding major organ system dysfunction, especially cardiac, liver, and renal dysfunction.
• Ask questions such as the following: Do the rings on your fingers get tight? Have you had to let your belt out? Have your clothes or shoes gotten too tight? • Pay special attention to the patient’s medications; • Also, obtain a thorough dietary history, paying careful attentio
n to the patient’s dietary sodium intake, total daily fluid intake;

Physical examination & Diagnostic testing
• In addition to the standard physical examination, chart the patient’s weight and note general appearance, paying special attention to the edema with respect to location, symmetry, pitting or nonpitting appearance, tenderness, and associated skin changes. Assess the severity of edema with a method such as the four-point scale (+1, slight, to +4, very marked) ;
• Including a chemistry panel and urinalysis to evaluate renal and liver function and albumin levels to assess nutritional status. Consider measuring the thyrotropin level to rule out hypothyroidism. In cases where screening for a cardiac etiology is required, an ECG and chest radiograph may be helpful in assessing cardiac function.

Differential diagnosis
• Heart failure
• Renal diseases
• Cirrhosis
• Nutritional origin
• Idiopathic
• Others

Differential diagnosisHeart Failure
• Edema initially occurs at lower part of the body (lower extremities)
• symmetric location
• The presence of heart diseasescardiac enlargement gallop rhythm dyspnea
basilar rales venous distention hepatomegaly
• Noninvasive tests may be helpful echocardiography radionuclide angiography

Differential diagnosisRenal diseases
• Mainly due to hypoabluminemia and
salt/water retention
• Associated with hematuria, proteinuria,
hypertention and impaired renal functional
• Characteriastic of edema of renal origin:
puffiness of the face
prominent in the periorbital areas
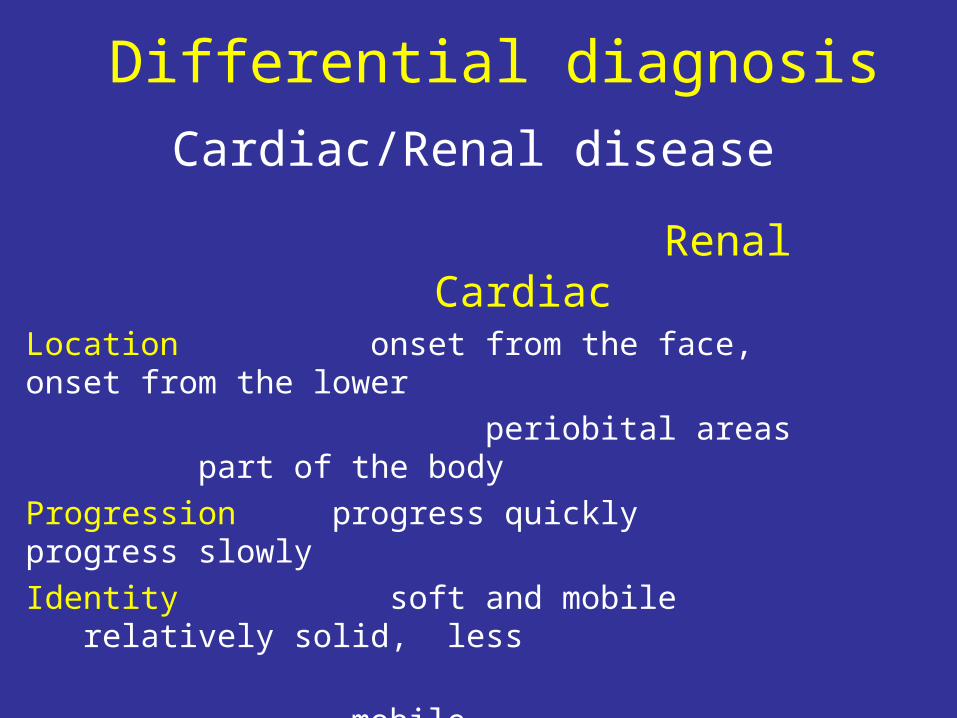
Differential diagnosis
Cardiac/Renal disease Renal CardiacLocation onset from the face, onset from the lower
periobital areas part of the body
Progression progress quickly progress slowly
Identity soft and mobile relatively solid, less
mobile
Other signs proteinuria signs of heart failure:
hypertension cardiac enlargement
impaired renal venous distention
functional test hepatomegaly

Differential diagnosisLiver diseases (cirrhosis)
• Clinical evidence of hepatic disease
jaundice spider angiomas ascites
• Ascites refractory to the treatment
• Edema may also occur in other parts of the body due to: •Hypoalbuminemia•increased intraabdominal pressure•impede venous return from the lower extremities

Differential diagnosisIdiopathic edema
• Exclusive in women
• periodic episodes
• accompanied by abdominal distention

Differential diagnosisOther Causes of Edema
• Hypothyroidism (myxedema, 粘液水肿 )
periorbital puffiness nonpitting• Exogenous hyperadrenoncortism• Pregnancy• Estrogens• angioneurotic

Approach to the patient
GeneralizedGeneralized
LocalizedLocalized
or
HeartLiver
Kidney
Venous obstruction
Lymphatic obstruction

Thanks for your attention