geriatrin interventions
TRANSCRIPT

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 1/22
PROPOSED INTERVENTIONS FOR GERIATRIC CAREIn the previous article, an effort has been made to describe the multifaceted problems
faced by the geriatric population. This article will focus upon the various proposed
interventions regarding the geriatric care
Old age can be termed as second childhood because an aged person needs the
same amount of care and attention as a child. In India there are few hospitals which are
providing specialized care for aged people. Those hospitals are either private hospitals or
apex institutions but patients find it difficult to locate the unit. Private hospitals and
nursing homes rarely invest in geriatric health care. Doctors and nurses don’t consider as
prolific field. Geriatric health care is capital intensive and at the same time it does not
yield much profit.
The status of existing infrastructure is such that the patients are admitted along
with other patients and so they do not get the special attention they are supposed to.
Although India participated in the world health assembly in 1982, there is great
reluctance in caring for aged people and this concept is still not popular among
professionals, family members, community, popular media or the government.
Geriatric health care unit: Geriatric health care unit consists of several experts
to converge on the problems of elderly and these include physician, physiotherapist,
psychologist, surgeon, nurse, dietician, caretaker, occupation therapist, geroorthopedician
and gerogynecologist. Such teams are possible in the near future as the new generation is
finding work more satisfying in different and challenging fields with the involvement of
NGOs in geriatric health care support.
EXISTING PROGRAMMES
The constitution of India encourages the State to shield older people from undeserved want in their oldage. An old age pension scheme has been introduced to meet the needs of people who have no means to
support themselves. The ministry of welfare makes financial assistance available to voluntary agencies torun daycare centers, often called activity centre, hobby club or golden age centers. However, even in urban
areas, many older people do not have any idea of the relevance of such centers. The scheme of givingrebate on income tax was introduced in 1992. Law also helps retired citizens in evicting tenants who
occupy their houses and concessions in train and airfare but environment is not as elderly-friendly as in
developed countries. There is no serious efforts to redesign public transport, public buildings, govt offices
to make their use easier for older people. However, India today has a vast network of governmental,
voluntary and private infrastructure manned by large number of medical and paramedical persons. Current
problems faced by the healthcare services has been listed but no special emphasis has been given in the 9thfive year plan for elderly health. However, integrated program for older persons through Panchayati Raj
resulted in financial assistance to 323 old age homes, 281 daycare centers and 42 mobile units in different
parts of the country during 2003-04.
1

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 2/22

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 3/22
Geriatric care is also capital intensive, but non-profitable. According to Dr. D.M.
Gamadia, medical adviser, Masina Hospital, Mumbai, to have a separate geriatric unit
would be ideal, but no one wants to invest in a full-fledged geriatric unit as the returns are poor. (Masina Hospital has a geriatric home, which is open only for the Parsi
community.)
Though government hospitals provide geriatric care, it is not a speciality, says Neha
Dalal, a social worker with Dignity Foundation. Most doctors in India have notspecialised in geriatrics. There is only one hospital in Chennai that gives post-graduate
(M.D.) education in geriatric medicine. Yesudian suggests having geriatric departments
in teaching hospitals
According to the ICMR study, geriatric clinics can be set up successfully at the rural
primary health centres with the existing infrastructure. The paramedical staff can be
trained to recognise major physical illnesses and find appropriate medical, community or
social interventions. The study showed that sleeplessness, vague body pain and backache
responded well to intervention by health workers, while other symptoms such as a visualhandicap, giddiness and pain in the joints showed marginal improvement. Counselling
proved very useful in cases where lack of family and social integration led to depression,which was the most common problem. Such patients responded well to intervention.
Among those living with their families, many reported lack of integration.
Screening and referrals greatly decrease the load on tertiary care services for the elderly.
Some hospitals do have geriatric outpatient services, but very few have in-patientfacilities, especially for the aged. This may be because the elderly are mostly in the
"young elderly" group (60-75 years), in which case there is little demand for long-term
health care.
The government, instead of dealing with the problem of the elderly by itself, isimplementing schemes to assist voluntary organisations to help senior citizens. These
organisations are provided financial assistance - grants up to 90 per cent of the project
expenditure - to set up day-care centres, old-age homes and mobile medicare units for theelderly. There are 186 old-age homes, 223 day-care centres and 28 mobile medicare units
under these projects. The Centre's direct contribution for the elderly comes in the form of
tax rebates and travel concessions.
The responsibility of the state for its senior citizens is enshrined in Article 41 of theConstitution. While the welfare of the aged is a State subject, the nodal responsibility for
the aged is vested with the Centre. The public policies of old-age income support takes
three forms: retirement benefits for those in the formal sector, voluntary insuranceschemes encouraged through tax exemptions, and direct government programmes to help
the needy elderly. The eligibility rules are often complicated and the pension amount
varies across States - from Rs.55 to Rs.300 a month. The National Old Age Pensionscheme offers a mere Rs.75 a month for those over 65. And even these inadequate
schemes together cover only 10 per cent of the elderly. An NSS survey (52 Round, 1995-
96) shows that 79 per cent of the elderly in the rural areas (who were engaged in
3

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 4/22
wage/salaried jobs or were casual labourers) and 35 per cent in the urban areas did not
receive any benefit after retirement.
With such a rapid increase in the proportion of the elderly, this is hardly the way for thegovernment to respond. It should, as Dr. Koshy Eapen, a researcher on geriatric care in
the University of London, points out, put in place a comprehensive geriatric care systemThe Geriatric Resources for Assessment and Care of Elders (GRACE) model of
primary care was developed specifically to improve the quality of care for low-income
seniors.
Features of the GRACE intervention include in-home assessment and care
management provided by a nurse practitioner and social worker team; extensive use
of specific care protocols for evaluation and management of common geriatric
conditions; utilization of an integrated electronic medical record and a Web-based
care management tracking tool; and integration with affiliated pharmacy, mental
health, home health, community-based and inpatient geriatric care services.
National Policy for aged under the Ministry of Social Justice and Empowerment
seeks health security of older people and it recognizes special health needs of the
older persons to be met through strengthening and reorienting of public health
services at Primary Health Care level and creation of health facilities.
•A few Societies and NGOs viz. Association of Gerontology, Geriatric Society of
India, Parkinson’s & Ageing Research Foundation, Helpage India, Age well
Foundation etc. are engaged in support activities related to Geriatric Care.
•Geriatrics clinics and M.D. course in Geriatric are functioning at BHU, AIIMS,
and Maulana Azad Medical College etc.
•Promotion of time-tested AYUSH practices for holistic health care viz. Rasayana
therapy of Ayurveda in particular for Geriatric Care.
Many countries have initiated programmes to tackle the issue of ageing population.
Japan has put in place a health-care financing system that gives essentially free care
(only a 5% of copayment is required) for all persons over age. A 'Golden Plan' was
announced in 1990 for expanding home and community-based services, particularlyrehabilitation and adult day care.
The People's Republic of China having world's largest population has initiated the
policy of one child per family, if fully implemented, would alter remarkably the
responsibility of the individual to his or her parents and grandparents; potentially, the onechild would bear responsibility to two parents and four grandparents.
4

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 5/22
The United Kingdom has incorporated Geriatric medicine in the postwar National
Health Service.
The Union of Soviet Socialist Republics (USSR) has one of the first research instituteson ageing.
Australia has developed an extensive health care policy, including programs for geriatric
assessment. Social security benefits are based on need.
As of now, not much importance has been given to geriatric care in India. The time has
come to plan cost effective, and community friendly approach for comprehensive healthcare delivery to the large geriatric population.
Existing facilities in geriatric care - India
1. Helpage India
2. Societies
1. Association of Gerontology (India), started in 1978, at Banaras Hindu University.Members of this association are clinicians, basic scientists, sociologist,
psychologist and clinical gerontologist. This has 250 members.
2. Geriatric society of India affliated to Association of Physicians of India started in
1982. It has about 500 members. It is Delhi based.3. Alzeihmer's diseases and related disorders society.
3. Government of India has formulated a National Policy for aged under the Ministry of
Social Justice and Empowerment.
4. National Blindness control programme.
5. Deafness programme run by Delhi government.
6. Existing medical facilities
1. Only one medical college in the country is running a M.D. course in Geriatric
Medicine.
2. Geriatrics out-patient clinics are being run at BHU, AIIMS, Maulana Azad
Medical College, LTMN College at Madurai.3. Some states as running old age homes.
7. Government of India has undertaken a programme to develop training modules for
medical colleges Teachers in Medicine and P.S.M. (as Trainer's) who will in turn trainthe doctors in primary and secondary health care setup.
5

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 6/22
Goals of Geriatric Care
1. Provide a safe and supportive environment for chronically ill and dependent
people.2. Restore and maintain the highest possible level of functional independence.
3. Preserve individual autonomy.
4. Maximize quality of life, perceived well-being, and life satisfaction.5. Provide comfort and dignity for terminally ill patients and their loved ones.
6. Stabilize and delay progression, whenever possible, of chronic medical
conditions.7. Prevent acute medical and iatrogenic illnesses and identify and treat them rapidly
when they do occur.
Elements of comprehensive geriatric health care in India
As the issue of providing care to the elderly population is of recent origin dueconsiderations are not being given to the comprehensive geriatric health care which
comprises of home care and institutional care.
In Indian socio economic situation the elderly population in majority of cases (upto 70%)
are living in a joint family set up and members of the family provide them care andcomfort. But the situation is changing because of industrialisation and post liberalisation
economic scenario resulting in migration of younger population in search of better future.
In India there is a great need for development of health care facilities for geriatric patients
which should be comparatively cheaper and cost effective so that they are easilyaccessible to vast majority of population who otherwise are unable to afford the services
offered by various expensive institutions. Certain Non-Government Organisation,
Charity-Welfare Organisations and Public Sector Undertakings etc. could contribute inthis direction.
Comprehensive geriatric health care comprises of physical,psychiatric, social, family, economic, nutritional andrehabilitation aspects.
Acute Hospitals
In India there are approx. 12000 hospitals comprising of about 7 lakhs hospital beds.
Most of the hospital beds are under government sector. There has been tremendous
growth in recent years in hospitals under private sector. The elderly populationapproaches hospitals mostly during acute illness depending upon physical and financial
accessibility. A fractured hip, pneumonia stoke or heart attack may necessitate immediate professional attention.
Problems in these hospital are that most of these hospitals have no geriatric wards
fulfilling the specific requirements and needs of geriatric patients. Also these hospitals
6

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 7/22
are not designed to provide long term care so as soon as the patient's condition improves
he or she is sent home.
Keeping in view the delay in convalescence of the geriatric patient, once a patients isadmitted, beds are occupied for a long time and thus hospital are also hesistant to admit
such patients. As a
economically inaccessible. After discharge patients are looked after by relations. There is
a need for low-cost convalescence homes atleast in all districts of country i.e. approx.550. In this area, N.G.O.'s and International agencies can contribute.
Hospice
In recent years a new movement for terminal care has developed. Beginning in England,
the hospice philosophy spread to the United States and has become in important aspect of terminal patient care. The philosophy is based on a belief that death is a normal process
which should neither be hastened or delayed.
Growing numbers of people concerned about protecting the dignity and comfort of the
terminally ill have developed units within hospitals and medical centers or have foundedspecific care facilities.
The goal of hospice care is to control pain so that the individual can remain an active
participant in life until death. Psychological, spiritual and social support, as well as legal
and financial counselling, should be available to both family and patient. Personal physical care for the patient is assured. A geriatric nursing assistant or home health aide
can provide most of the care under the direction of a professional hospice nurse.
Hospice care can meet the needs of terminal oncology patients (those with incurable
malignant tumors), and can also be extended to include others with a life expectancy of six months or less. Support groups can by formed to visit terminal patients in conjuction
with hospice teams. Many volunteers serve as "special friends," making regular visits and
working on a one-to-one basis with the patient and family.
In India, there are very few hospices, and most of them are only located in metropolitans.
Organisation like Mother Teresa has done lot of work in this direction to give dignity to
dyeing poor. First in Calcutta, later on other parts of country. Such facilities could also
exist in district level. Charitable and welfare organisation can play an active role.
Death and Dying
Postmortem Care
Postmortem care is the care given after death is pronounced. Death, like life, must be
handled with dignity and caring. Immediately following death, hospitals should makesure that the body is positioned with the limbs straight and that the bedding is clean and
7

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 8/22
neat. Equipment should be moved out of the unit. Family members may wish to view the
deceased and attention to these details makes the experience easier.
Day care/Day Hospital
One big advantage of day care is the cost, which is usually less than the cost of care in anursing home. In addition to providing treatment for the patient, the day care center can
assist families in making adjustments and finding aid. A day care facility can often make
it possible to avoid or delay institutionalization.
Day hospitals attempt to dissociate the investigational and therapeutic aspect of hospital
treatment from the hotel aspect which often requires patients to be looked after at night
and throughout the weekend when no investigation or treatment is carried out. The dayhospital also helps in a close and prolonged supervision of patients suffering from
chronic disease who, if isolated completely from hospital care, would almost certainly
deteriorate and require readmission.
Day care centres could also be business investments incorporating social as well as health benefits, where health examination and health screening can be routinly carried through
agencies such as local health department, doctors, nurses, dieticians and social workers
visiting the centre. Doctors and nurses could use their visits to do the health screening
and referals. Special programmes on nutrition and general preventive health measurescould be conducted on monthly basis.
Variants in day hospitals could have provisions for a travelling day hospital in which a
group of staff move between different centres on each day in the week for managementof psychogeriatric need for patients.
Rehabilitation Centres and Teams
Rehabilitative services are offered through centres, some of which specialize in specific
types of rehabilitation. Such units are frequently part of large metropolitan hospitals or are associated with independent agencies.
Rehabilitation services can be directed by a team of professional people, working
together to establish and reach realistic goals. At times, the team will consist of medicine,
recreational therapy, occupational therapy, psychotherapy, physiotherapy, social serviceand nursing. The nurse can serve as coordinator for the combined effort. At other times,
the nurse, doctor, and a few specialists make up the team. With team approach, each teammember sees the patient from a slightly different viewpoint. From the consensus, a
specific rehabilitation plan is devised and recorded on the patient care plan.
Patients hospitalized in institutions with rehabilitation units can take advantage of these
services. Many other patients utilize them on out-patient basis. Outside of the centres,
rehabilitative planning and services are provided by the physician, family, and publichealth nurse. The home health aide/geriatric nursing assistant/health workers can play an
8

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 9/22
important role in the rehabilitation of the home patient, supplying encouragement and
assisting in therapy as directed.
Home Care
In India because of close social links, families and also because of economic compulsion,geriatric population has to entirely depend upon near and dear ones. Lack of health
education and awareness of geriatric needs, certain practices may actually harm the
health of geriatric patient. Therefore, there is need for development of reading materialfor home care of geriatic patients. Audiovisual media (T.V., Radio etc.) could greatly
help in this regard.
Safety considerations for elderly (institutional as well as home care)
Safety is the concern both of the elderly person and of those responsible for the elder'shealth care.
Persons aged sixty and above account for approx. 20 percent of all accidental death and
13 percent of all hospitalized accident victims. Therefore constant vigilance is needed to
safeguard the elderly both at home and in patient care facilities.
Manpower Development
Medical Manpower
Undergraduate and post graduate courses should have curriculum for geriatric medicine.
In service training for doctors at all levels of health car (primary, secondary, tertiary)
should be imparted.
Nursing Manpower
Geriatric nursing care should be part of curriculum for nursing courses or a special post
graduate course could be designed for geriatric nursing.
Geriatric Health Care Assistant/Home Health Assistant
This category of workers should be trained in gereotology and basic nursing skills.Geriatric health care Assistant may function as home health aids or may be employed in a
nursing facility.
At the peripheral level, male and female health workers should be imarted this training to
help the chunk of elderly population living in rural areas and dependent on primary healthcare centres.
The curriculum for this category could be developed, Paramedical vocational education at
10+2 level. (Such courses are being developed in the field of Dental Technician,
9

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 10/22
hygenist, Radio-grapher, Hospital housekeeper, Record keeping etc. by Pandit Sunderlal
Sharma Central Institute of Vocational Education, Bhopal under NCERT, Ministry of
HRD.) This is going on as per the recommendation of Bajaj Committee.
Conclusion
The percentage of elderly population is continously increasing in India due to decline in
overall death rate, decline in fertility and sustained improvement in survival. There is also
revolutionary change in health care delivery system in the country as a result of privatisation and globalisation. To evolve a comprehensive health care for elderly
population we have to think in terms of all the elements of comprehensive health care
such as :
1. Care at home
2. Health education.
3. Institutional care - facility planning for elderly population.
4. Human resource development for creation of medical and pare-medical expertise.5. Sensitisation and involvement of NGO's and voluntary organisation.
6. Health insurance programme.
Experts say India stands far behind other countries in this respect. In European countries
and Japan, the hospitals have a separate geriatric unit. They also have Geriatric SpecialCare Hospitals. “Hospitals in Japan are equipped with latest technology instruments and
they have specialised doctors in the geriatric field,’’informs Yesudian.
According to reports, Heritage Medical Centre, a healthcare institute based in Hyderabad,is trying to help the elderly to face life’s troubles. The centre offers many facilities for the
elderly sick including skilled nursing care, physical rehabilitation, speech therapy,clinical psychology, a day hospital, surgical and post-operative care, a non-ambulatory
unit and an intensive care unit.
It also has a senior citizen forum, with a membership of Rs 50, which holds meetings and
dinners, and offers a social situation for the elderly. It is said that though the Centre is
inspired by institutions in the US, the longterm goal is home-nursing and not providing
high-tech facilities.
Fighting all constraints is KEM Hospital which has been providing the geriatric care
service since 1986. The hospital has a Geriatric Functional Assessment (GFA) team of in-
house doctors working for the OPD geriatric service.
The team comprises physician, dieticians, medical social workers (MSWs), psychiatrists, physiotherapists, orthopaedic surgeons, nurses, caretakers, occupation therapists, gero-
orthopaedicians and gero-gynaecologists.
10
7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 11/22
However, for these doctors, this is an additional duty as they have not done geriatric
schooling. There are no separate wards or beds for these patients. When patients need
hospitalisation, they are admitted along with other patients.
‘‘There is limited interest on the part of doctors. Doctors find it difficult to stretch the
working hours. These doctors are not specialised in geriatric care and they do not work specially for geriatric care,’’ informs Dr Yogini V Meisheri, professor of Medicine, Unit
head, Seth GS Medical College and KEM Hospital who has been heading the KEMGeriatric service since 1991.
LTMG Hospital also provides referral geriatric service backed by the dean and resident
doctors. Patients above 60 years of age are given priority, explains Dr Nitin Karnik,associate professor, Department of Medicines, LTMG Hospital.
‘‘The various tests are done free of cost for individuals. We have the poor box charity
funds and social workers who help with the medicines. And if the patient is a pensioner,
he can pay whatever he can afford and the rest is taken care of,’’ adds Dr Karnik.
The drugs which are provided free are generally taken from hospital dispensaries,doctors’ donations and `Drug Banks’ formed by collecting drugs which pharma
companies leave behind as samples. ``We are requesting pharmaceutical companies to
come forward and provide drugs,’’ says Dr Meisheri.
‘‘We also have social organisations sponsoring the drugs for them,’’ says Dr Karnik. Hefurther adds that that drugs should be sponsored on a continuous basis as most of the
times the drugs are not available.
‘‘What is happening now is that all these hospitals as well as social organisations areworking individually. If a common body is formed, then it might help to improve theworking of these services and streamline the work and help cater to the correct need
jointly Also, so far, there is no law that every hospital must have a geriatric unit. If such a
law is enacted than the working of our services will become systematic,’’ suggests Dr Meisheri.
This apart, another major problem faced is lack of funds due to which most of the times
the doctors end up paying from their pockets. These hospitals are highly dependent on
donations. ‘Funds have always been a problem. We should have the backing of specialfunds in the form of relief funds,’’ avers Dr Karnik.
Experts say India needs specialised medical education in geriatric care. As of now there
is only one hospital, in Chennai, which gives post-graduate (MD) education in geriatrics
medicines.
“Doctors who are trained abroad should be introduced here who can in turn teach other
doctors. We should have geriatric departments in teaching hospitals, suggests Yesudian.
11
7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 12/22
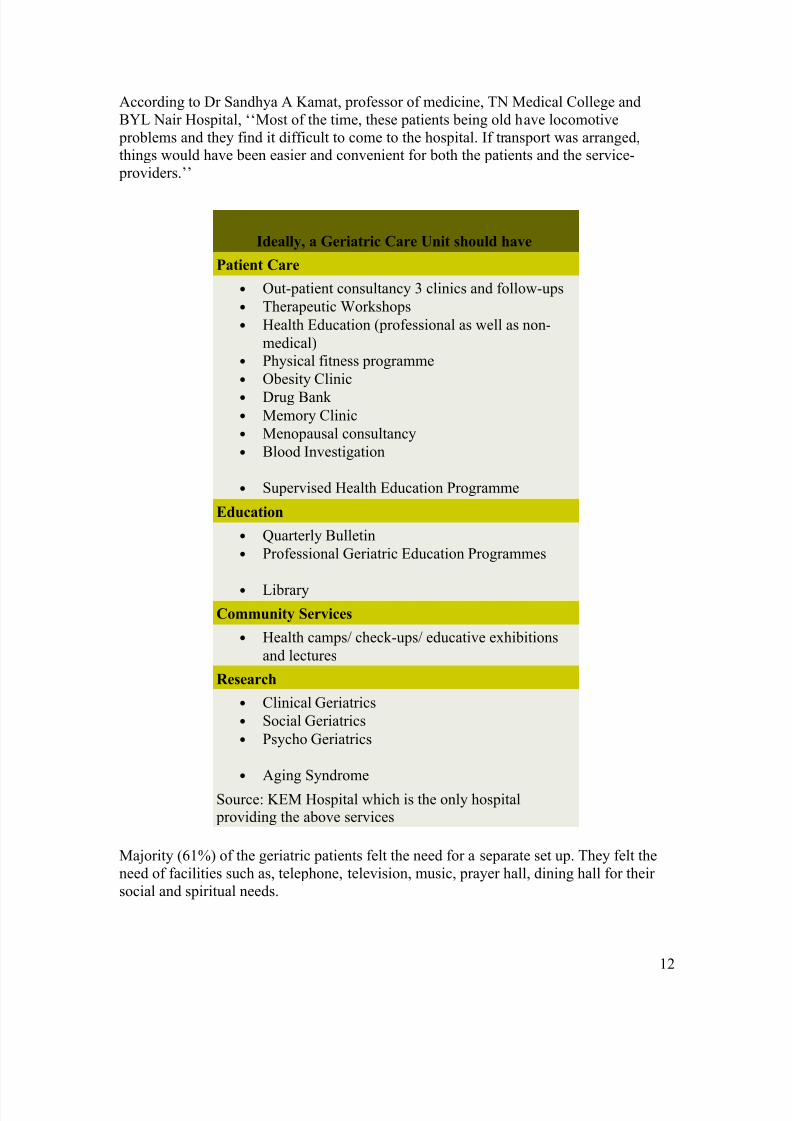
According to Dr Sandhya A Kamat, professor of medicine, TN Medical College and
BYL Nair Hospital, ‘‘Most of the time, these patients being old have locomotive
problems and they find it difficult to come to the hospital. If transport was arranged,things would have been easier and convenient for both the patients and the service-
providers.’’
Ideally, a Geriatric Care Unit should have
Patient Care
• Out-patient consultancy 3 clinics and follow-ups
• Therapeutic Workshops
• Health Education (professional as well as non-
medical)
• Physical fitness programme
• Obesity Clinic
• Drug Bank • Memory Clinic
• Menopausal consultancy
• Blood Investigation
• Supervised Health Education Programme
Education
• Quarterly Bulletin
• Professional Geriatric Education Programmes
• Library
Community Services
• Health camps/ check-ups/ educative exhibitions
and lectures
Research
• Clinical Geriatrics
• Social Geriatrics
• Psycho Geriatrics
• Aging Syndrome
Source: KEM Hospital which is the only hospital providing the above services
Majority (61%) of the geriatric patients felt the need for a separate set up. They felt the
need of facilities such as, telephone, television, music, prayer hall, dining hall for their
social and spiritual needs.
12

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 13/22
Most of them (78%) were satisfied with clinical and supportive service, Majority (90%)
of them did not face any problem in the physical facilities provided except non-slippery
floor and cot adjustments.
There is a need for a separate geriatric unit in a teaching hospital utilized by significant
number of geriatric population. However modification of the existing facility would atleast result in a better care being provided to geriatric population.
Over the years, the government has launched various schemes and policies for older persons. These schemes and
policies are meant to promote the health, well-being and independence of senior citizens around the country. Some
hese programmes have been enumerated below.
The central government came out with the National Policy for Older Persons in 1999 to promote the health and welof senior citizens in India. This policy aims to encourage individuals to make provision for their own as well as thei
spouse’s old age. It also strives to encourage families to take care of their older family members. The policy enables
and supports voluntary and non-governmental organizations to supplement the care provided by the family and provcare and protection to vulnerable elderly people. Health care, research, creation of awareness and training facilities
geriatric caregivers have also been enumerated under this policy. The main objective of this policy is to make older
people fully independent citizens.
This policy has resulted in the launch of new schemes such as –
1. Strengthening of primary health care system to enable it to meet the health care needs of older persons2. Training and orientation to medical and paramedical personnel in health care of the elderly.
3. Promotion of the concept of healthy ageing.
4. Assistance to societies for production and distribution of material on geriatric care.
5. Provision of separate queues and reservation of beds for elderly patients in hospitals.6. Extended coverage under the Antyodaya Scheme with emphasis on provision of food at subsidized rates for
benefit of older persons especially the destitute and marginalized sections.
The Integrated Programme for Older Persons is a scheme that provides financial assistance up to 90 per cent of theproject cost to non-governmental organizations or NGOs as on March 31, 2007. This money is used to establish and
maintain old age homes, day care centres, mobile Medicare units and to provide non-institutional services to older
persons. The scheme also works towards other needs of older persons such as reinforcing and strengthening thefamily, generation of awareness on related issues and facilitating productive ageing.
Another programme of the government is the Scheme of Assistance to Panchayati Raj Institutions voluntary
organisations and self help groups for the construction of old age homes and multi service centres for older personsThis scheme provides a one time construction grant.
Central Government Health Scheme provides pensioners of central government offices the facility to obtain medicinfor chronic ailments up to three months at a stretch. For more details, click here.
The National Mental Health Programme focuses on the needs of senior citizens who are affected with Alzheimer’s
other dementias, Parkinson’s disease, depression and psycho geriatric disorders.
13
7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 14/22
New Schemes
Well, the journey towards financial security does not end here. The Central Government is in the process of develop
newer plans and schemes to benefit senior citizens. In the 2007-08 Budget, the Finance Minister has proposed to
provide monthly income to seniors and develop new health insurance schemes.
For the benefit of senior citizens it has been proposed that –
The National Housing Bank will introduce a 'reverse mortgage' scheme under which a senior citizen who ow
a house can avail of a monthly stream of income against mortgage of the house. The senior citizen remains t
owner and occupies the house throughout his or her lifetime, without repayment or servicing of the loan.Regulations are to be put in place to allow creation of mortgage guarantee companies.
An exclusive health insurance scheme for senior citizens is to be offered by the National Insurance Compan
Three other public sector insurance companies as mentioned in the Medical Insurance section, are to offer a
similar product to senior citizens.
The Maintenance of Parents and Senior Citizens Bill o f 2007 – This bill has been recently introduced inParliament. It provides for the maintenance of parents, establishment of old homes, provision of medical car
and protection of life and property of senior citizens.
These new developments for senior citizens are meant to get them on the path to a better, peaceful and financially
sound life.
CONCESSIONS AND FACILITIES GIVEN TO SENIOR CITIZENS BY DIFFERENT MINISTRIES/DEPARTMENTS OF THE
GOVT.
Sl.No.
Name of theMin./Department
Facilities/Benefits given to Senior Citizens
1 Ministry of Social Justice& Empowerment
Ministry of Social Justice & Empowerment is the nodal Ministryresponsible for welfare of the Senior Citizens. It has announced theNational Policy on Older Persons covering all concerns pertainingto the welfare of older persons. The National Policy on Older Persons recognizes a person aged 60 years and above as a senior citizen.
2. The Ministry is also implementing following schemes for thebenefit of Senior Citizens:
(a) An Integrated Programme for Older Persons (Plan Scheme) –This Scheme has been formulated by revising the earlier scheme of “Assistance to Voluntary Organisations for Programmes relating tothe Welfare of the Aged”. Under this Scheme, financial assistanceupto 90% of the project cost is provided to NGOs for establishingand maintaining Old Age Homes, Day Care Centres, MobileMedicare Units and to provide non-institutional services to older persons.
14
7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 15/22
(b) The Scheme of Assistance to Panchayati Raj Institutions/Voluntary Organizations/Self Help Groups for Construction of Old
Age Homes/Multi-Service Centres for older persons (Non PlanScheme) - Under this Scheme, one time construction grant for Old
Age Homes/Multi-Service Centre is provided to non-governmentalorganizations on the recommendation of the State Governments/UT Administrations.
2 Ministry of Finance Income tax rebate upto an income of Rs. 1.85 lakh p.a.
Higher rates of interest on saving schemes of senior citizens.
A Senior Citizens Savings Scheme offering an interest rate is 9%per annum on the deposits made by the senior citizens in postoffices has been introduced by the Government through PostOffices in India doing savings bank work.
3 Ministry of RoadTransport and Highways
i) Reservation of two seats for senior citizens in front row of thebuses of the State Road Transport Undertakings.ii) Some State Governments are giving fare concession to senior citizens in the State Road Transport Undertaking buses and are
introducing Bus Models, which are convenient to the elderly.4 Ministry of Health &Family Welfare
Separate queues for older persons in hospitals for registration andclinical examination.
5. Department of Telecommunications
i) Faults/complaints of senior citizens are given priority byregistering them under senior citizens category with VIP flag, whichis a priority category.ii) Senior citizens are allowed to register telephone connectionunder N-OYT Special Category, which is a priority category.
6 Ministry of Railways a) Indian Railways provide 30% fare concession in all Mail/Expressincluding Rajdhani/Shatabadi/Jan Shatabadi trains for senior citizens aged 60 years and above.
b) Indian Railways also have the facility of separate counters for
Senior Citizens for purchase/booking/cancellation of tickets.
c) Wheel Chairs for use of older persons are available at all junctions, District Headquarters and other important stations for theconvenience of needy persons including the older persons.
d) Ramps for wheel chairs movement are available at the entry toimportant stations.
d) Specially designed coaches with provisions of space for wheelchairs, hand rail and specially designed toilet for handicappedpersons have been introduced.
7 Ministry of Civil Aviation 1. Indian Airlines is providing 50 per cent Senior Citizen Discount
on Normal Economy Class fare for all domestic flights to Indiansenior citizens who have completed the age of 65 years in the caseof male senior citizens and 63 years in the case of female senior citizens subject to certain conditions.
2. Air India is offering discount to senior citizens of 60 plus onflights to USA , UK and Europe . Further, Air India has now decidedto reduce the age of 60 plus for discount on their domestic routes
15
7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 16/22
as well with immediate effect.
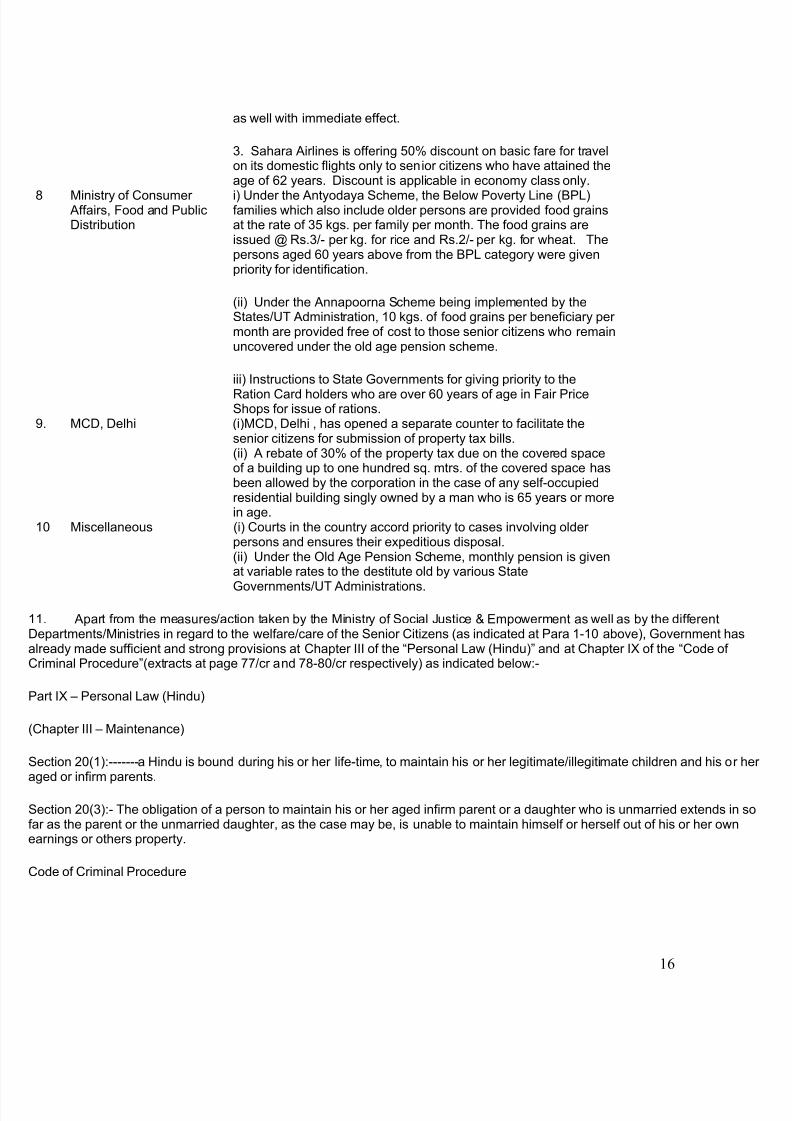
3. Sahara Airlines is offering 50% discount on basic fare for travelon its domestic flights only to senior citizens who have attained theage of 62 years. Discount is applicable in economy class only.
8 Ministry of Consumer Affairs, Food and PublicDistribution
i) Under the Antyodaya Scheme, the Below Poverty Line (BPL)families which also include older persons are provided food grainsat the rate of 35 kgs. per family per month. The food grains areissued @ Rs.3/- per kg. for rice and Rs.2/- per kg. for wheat. Thepersons aged 60 years above from the BPL category were givenpriority for identification.
(ii) Under the Annapoorna Scheme being implemented by theStates/UT Administration, 10 kgs. of food grains per beneficiary per month are provided free of cost to those senior citizens who remainuncovered under the old age pension scheme.
iii) Instructions to State Governments for giving priority to the
Ration Card holders who are over 60 years of age in Fair PriceShops for issue of rations.
9. MCD, Delhi (i)MCD, Delhi , has opened a separate counter to facilitate thesenior citizens for submission of property tax bills.(ii) A rebate of 30% of the property tax due on the covered spaceof a building up to one hundred sq. mtrs. of the covered space hasbeen allowed by the corporation in the case of any self-occupiedresidential building singly owned by a man who is 65 years or morein age.
10 Miscellaneous (i) Courts in the country accord priority to cases involving older persons and ensures their expeditious disposal.(ii) Under the Old Age Pension Scheme, monthly pension is givenat variable rates to the destitute old by various State
Governments/UT Administrations.
1. Apart from the measures/action taken by the Ministry of Social Justice & Empowerment as well as by the differentDepartments/Ministries in regard to the welfare/care of the Senior Citizens (as indicated at Para 1-10 above), Government hasalready made sufficient and strong provisions at Chapter III of the “Personal Law (Hindu)” and at Chapter IX of the “Code of Criminal Procedure”(extracts at page 77/cr and 78-80/cr respectively) as indicated below:-
Part IX – Personal Law (Hindu)
Chapter III – Maintenance)
Section 20(1):-------a Hindu is bound during his or her life-time, to maintain his or her legitimate/illegitimate children and his or aged or infirm parents.
Section 20(3):- The obligation of a person to maintain his or her aged infirm parent or a daughter who is unmarried extends in ar as the parent or the unmarried daughter, as the case may be, is unable to maintain himself or herself out of his or her own
earnings or others property.
Code of Criminal Procedure
16

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 17/22
17

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 18/22
18

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 19/22
19

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 20/22
20

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 21/22

7/28/2019 Geriatrin Interventions
http://slidepdf.com/reader/full/geriatrin-interventions 22/22