global landscape of poc tests and their uptake · global landscape of poc tests and their uptake...
TRANSCRIPT
Global Landscape ofof
POC Tests and Their UptakePOC Tests and Their Uptake
Rosanna W PeelingProfessor and Chair, Diagnostic ResearchProfessor and Chair, iagnostic Research
London School of Hygiene & Tropical Medicine

Global Landscape of POC Tests and their Uptake
• Diagnostic landscape in the
p p
• Diagnostic landscape in the developing world
• The promise of Point‐of‐Care tests to improve global healthimprove global health
• Challenges in uptake• Challenges in uptake
• The way forwardy

Diagnostics Landscape in the Developing World
• Lack of accessAlthough high‐quality diagnostics are available for many infectious g g q y g ydiseases, they are neither affordable nor accessible to patients in the developing world
• Lack of investmentLittle industry interest in developing quality diagnostics for diseases prevalent in the developing world, due to a perceived lack of return for investment, and lack of investment by MOHs
• Lack of regulatory oversightLack of regulatory oversightTests are often sold and used without evidence of effectiveness, discouraging companies with quality products from competing
• Lack of quality standards for test evaluationsClaimed accuracy on product inserts often misleading

Inequity of Access to DiagnosticsThe 2004 Health Development Report cited the lack of access and
unaffordability as two major reasons why services fail
Distance to Nearest Medical Facility forthe Poorest 5th of the population: Pregnant women with syphilis
Country Distance (km)
Benin 7.5Bolivia 11.8
% who access ANC
% who access ANC
75%
50%Chad 22.9Haiti 8.0Madagascar 15.5Niger 26.9Tanzania 4 7
early in pregnancy% tested
for syphilis
50%
25%Tanzania 4.7Uganda 4.7Zimbabwe 8.6
Selected from the 2004 World Health Report, p.22%
treated
% giventest results 18%
15%

Balance between Access and Performance of Diagnostics
Source: Foundation for Innovative New Diagnostics (FIND)

Lack of Regulatory Oversight for Diagnostics
In Vitro Diagnostic Devices Regulation ByIn Vitro Diagnostic Devices
Regulated
In Vitro Diagnostic Devices Regulation By Region
No52%
Yes48%
Yes No No 11 9 5 2 2 15
Yes 4 9 4 14 3 7
AFRO AMRO EMRO EURO SEARO WPRO
TDR survey 2002
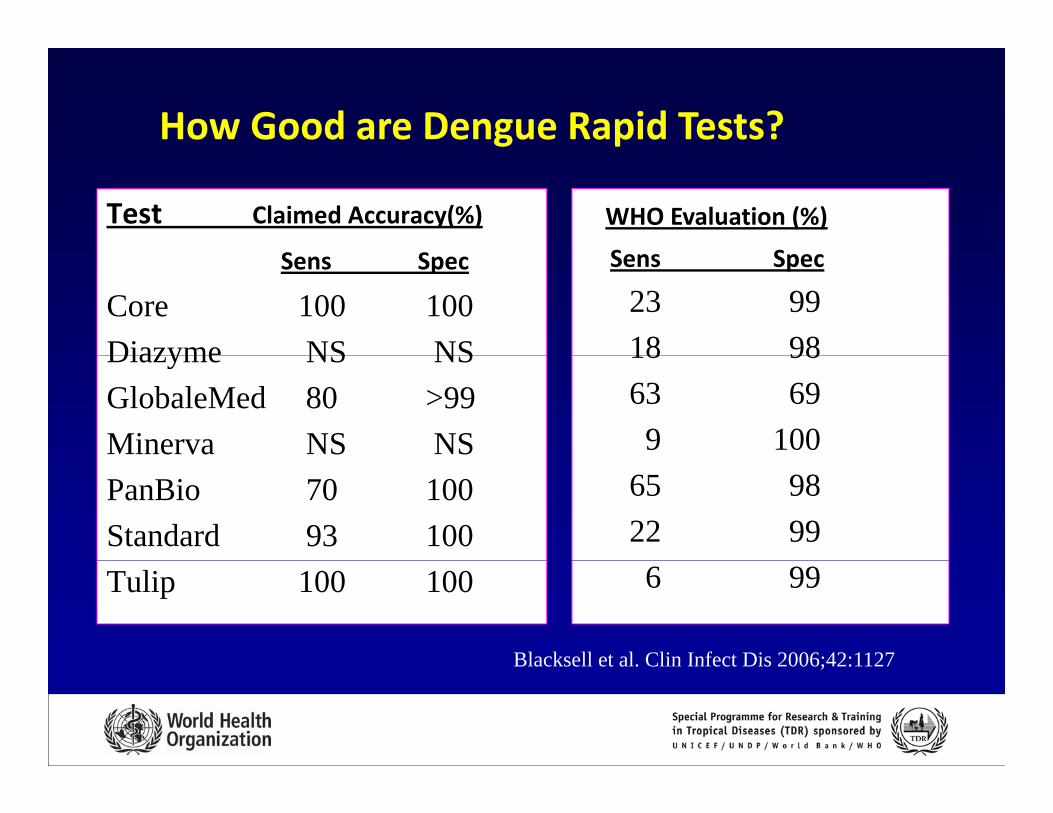
How Good are Dengue Rapid Tests?
Test Claimed Accuracy(%)
S S
WHO Evaluation (%)
S SSens Spec
Core 100 100Diazyme NS NS
Sens Spec
23 9918 98Diazyme NS NS
GlobaleMed 80 >99Minerva NS NS
18 9863 699 100
PanBio 70 100Standard 93 100
65 9822 99
Tulip 100 100 6 99
Blacksell et al Clin Infect Dis 2006;42:1127Blacksell et al. Clin Infect Dis 2006;42:1127
ASSURED Tests I Gl b l H l hto Improve Global Health
A = affordableS = sensitive S = specificU = user‐friendly R = rapid and robustE = equipment‐free D = deliverable

The Promise of POC Tests
Disease Population Sens/Spec(%)
Potential Impact(%)
ALRI Children <5 yrs
95/85 Save ~405,000 lives
HIV Infants <12 90/90 Save 2 5 million DALYs if 100%HIV Infants <12 months
90/90 Save 2.5 million DALYs if 100% access to treatment
Malaria Children <5 yrs
90/90 Save 2.2 million DALYS and prevent 447 million unnecessary treatmentyrs 447 million unnecessary treatment
TB Symptomatic 85/97 Save ~400,000 livesSyphilis prenatal 86/72 Save 201,000 DALYS, avert 215,000
tillbi thstillbirthsCt/Ng Sex workers 85/90 Save ~4 million DALYs, avert 16.5
million new cases and prevent 212 000 HIV212,000 HIV cases
Urdea M et al Nature 2006
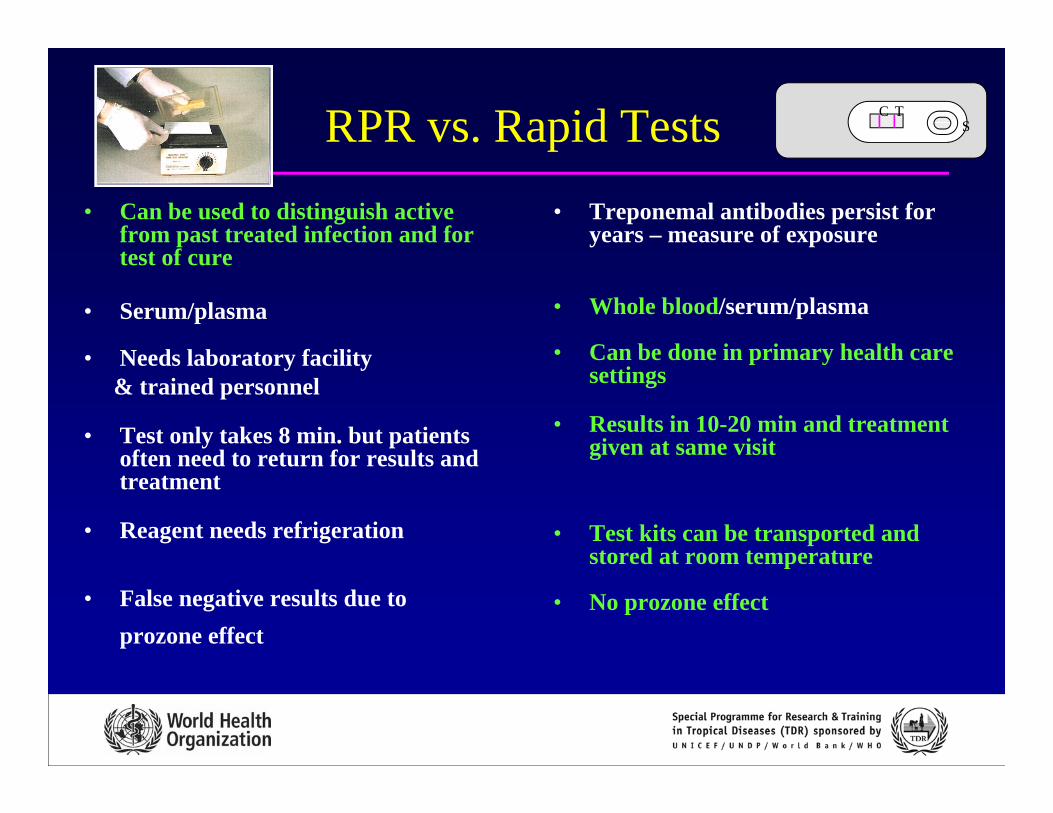
RPR vs. Rapid Tests C TSp
• Can be used to distinguish active from past treated infection and for t t f
• Treponemal antibodies persist for years – measure of exposure
test of cure
• Serum/plasma
• Needs laboratory facility
• Whole blood/serum/plasma
• Can be done in primary health care• Needs laboratory facility& trained personnel
• Test only takes 8 min. but patients often need to return for results and
Can be done in primary health care settings
• Results in 10-20 min and treatment given at same visitoften need to return for results and
treatment
• Reagent needs refrigeration
g
• Test kits can be transported and stored at room temperature
• False negative results due to prozone effect
stored at room temperature
• No prozone effect

Rapid Tests for SyphilisRapid Tests for SyphilisProcedure:1. Use dropper provided, dispense 1 drop of serum/whole blood to sample well S 2. Add 2 drops of diluent buffer to sample well S3 R d l f 15 i3. Read results after 15 minutes
C TS Negative
C TS Positive
C TS Invalid

Validating Rapid Syphilis Testsg p yp• Lab-based evaluation of 9 tests in 8 countries
• Field trials of 4 rapid tests in 4 countries
h i l d l• Mathematical models to:– Estimate impact– Estimate cost-effectiveness of different strategies for g
introduction
• 7 tests with acceptable performance included in WHO Bulk7 tests with acceptable performance included in WHO Bulk Procurement Scheme at $ .19 – 1.00

Laboratory based Evaluation of Rapid Syphilis Tests(China, Gambia, Haiti, Russian Federation, South Africa, Sri Lanka, Tanzania, USA)
Test whole blood Sensitivity(%)* Specificity %)*
( , , , , , , , )
Fujireibio Espline, Japan - 98 93Determine, UK + 97 94
CTK Bi t h USA 96 95CTK Biotech, USA - 96 95
Standard Bioline, KOREA + 95 95
Qualpro Syphicheck II, INDIA + 95 94
Pacific Biotech Bioline, THAI. - 93 97
Diesse Syphilis Fast, ITALY - 86 93
(Omega VisiTect UK + 85 98)
* Performance in serum compared to TPHA/TPPA
(Omega VisiTect, UK + 85 98)
Herring et al STI 2006; 82 Suppl V: v7 12Herring et al. STI 2006; 82 Suppl V: v7-12
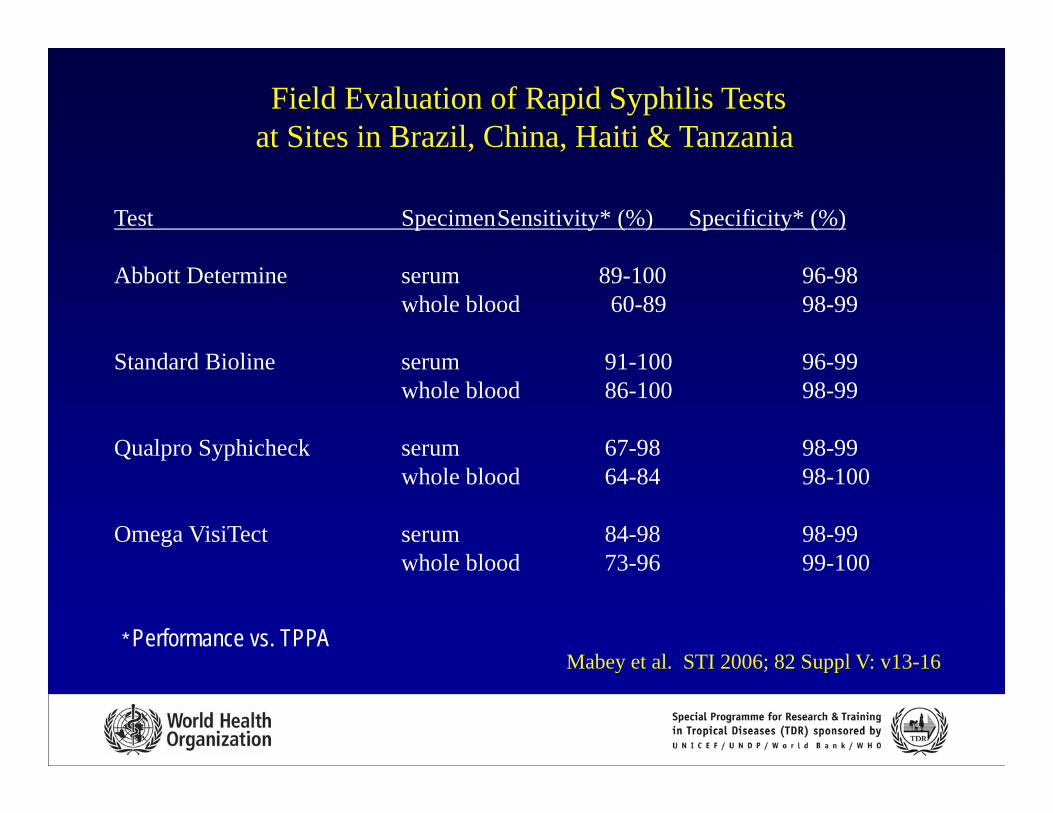
Field Evaluation of Rapid Syphilis Testsat Sites in Brazil, China, Haiti & Tanzania
Test SpecimenSensitivity* (%) Specificity* (%)
, ,
Abbott Determine serum 89-100 96-98whole blood 60-89 98-99
St d d Bi li 91 100 96 99Standard Bioline serum 91-100 96-99whole blood 86-100 98-99
Qualpro Syphicheck serum 67-98 98-99Q p ypwhole blood 64-84 98-100
Omega VisiTect serum 84-98 98-99whole blood 73 96 99 100
* Performance vs. TPPA
whole blood 73-96 99-100
Mabey et al STI 2006; 82 Suppl V: v13-16Mabey et al. STI 2006; 82 Suppl V: v13-16

Cost‐effectiveness of Antenatal Screening Using Rapid Syphilis Tests: Mwanza, Tz
Cost effecti eness of sing rapid tests depends on• Cost‐effectiveness of using rapid tests depends on: – Cost of rapid tests – Sensitivity of rapid test for high titre active syphilis (RPR>8)
• Rapid tests need to be < US$ 0.63 to be as cost‐effective as RPRRPR
• Cost‐effectiveness of RPR decreases by 25‐65% if 20‐40% of did t t f th i t t ltwomen did not return for their test results
Vickerman et al STI 2006;82:Suppl V; pp

Screening Using Rapid Syphilis Tests is Cost‐effectiveCost effective
• Cost of antenatal screening in Haiti using rapid tests:– Programme costs: 46% for test, 42% labour, 7% supplies, 6% for others
including treatment)– $2.15 per woman screened vs $1.43 for RPR
ff $ / f $ / f– Cost‐effectiveness: $10/DALY for urban and $7/DALY for rural areas– Cost/adverse outcome prevented: $108‐218
• Compares favourably with other child health interventions
• Rapid test is the preferred strategy as long as test sensitivity isRapid test is the preferred strategy as long as test sensitivity is >70% and return rate for 1st FU visit for RPR is >75%
Schackman et al PLoS Med May 2007Schackman et al PLoS Med May 2007

Increasing Access to Syphilis Screening
Goal:To reduce the burden associated with syphilis in the developing world through increased access to screeningdeveloping world through increased access to screening
Objectives:
1. To assess the feasibility of increasing access to antenatal screening using a Same Day Testing and Treatment Strategy (STAT)
2. To determine the cost-effectiveness of introducing quality-. o dete e t e cost e ect ve ess o t oduc g qua tyassured rapid syphilis testing into existing services for PMTCT/other prenatal services or high risk populations
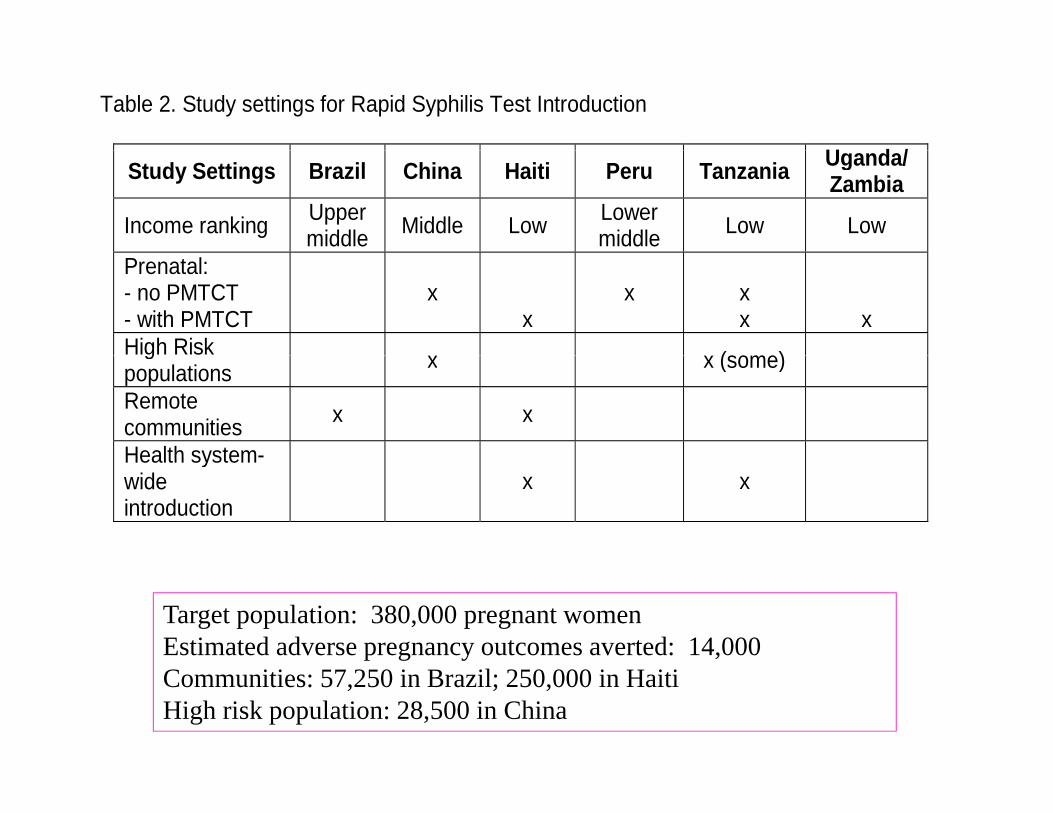
Table 2. Study settings for Rapid Syphilis Test Introduction
U d /Study Settings Brazil China Haiti Peru Tanzania Uganda/Zambia
Income ranking Upper middle Middle Low Lower
middle Low Low
Prenatal: - no PMTCT - with PMTCT
x
x
x
x x
x
High Risk ( )gpopulations x x (some)
Remote communities x x
Health system-Health systemwide introduction
x x
Target population: 380,000 pregnant womenEstimated adverse pregnancy outcomes averted: 14,000Communities: 57,250 in Brazil; 250,000 in HaitiHigh risk population: 28,500 in China

Rapid Test Project in Brazil

Rapid Syphilis Test Introduction & S i bl Ad iSustainable Adoption
Policy Technical Aspects of ImplementationAdvocacy
Procurement &GuidelinesSt t Stock management
Quality control of Tests &Quality assurance of Testing
Guidelines
T t S l ti
Status quo, identify barriers,design strategies, estimate potential
Cost Implications
Training& Training of Trainers
Q y gTest Selection p
impact & costs
Implementation:Cost-effective Strategies for Test introduction
Monitoring / Evaluation
Links to disease surveillance to validate impact
Generic Tool Kit for Use of Rapid Syphilis Tests
Advocacy
Policy platform: generic process for translating research findings into policy and practice; engagement with regulatoryfindings into policy and practice; engagement with regulatory authorities
Data collection and management, including cost data
Questionnaire to capture barriers to introduction
Setting up Quality Assurance/Quality Control systems
Training in Procurement/stock management
Training and Training-of-Trainers packages for test useTraining and Training of Trainers packages for test use
Study monitoring tools
W b b d I t ti th ti l d l t di tWeb based Interactive mathematical models to predict potential impact and cost-effectiveness of strategies for introduction

Buy-in: Introduction & Sustainability• AdvocacyAdvocacy
– Define disease burden, problems with status quo and what is needed to improve it, the attributable benefit of introducing new tool (such as a rapid test) e g lives saved orintroducing new tool (such as a rapid test) e.g. lives saved or morbidity prevented, cost-effectiveness of strategies for tool introduction
• Policy and Guidelines– Accrue evidence needed for development or change of
policy– implications of policy or policy change: determine fiscal and
human resources
S r eillance• Surveillance– ability to monitor disease trends as an attributable benefit of
test introduction– Links to STI surveillance?Links to STI surveillance?– What is reported and what is the mechanism?

Ensuring the Quality of Diagnostics• Procurement
– Selecting the best test that is fit for purpose– Based on test performance evaluations
• Quality during transport and storageQuality during transport and storage– Lot testing and periodic checks on test performance
• Quality of testing P fi i f t ti– Proficiency of testing

Genomics
Translation Research Pathway for Appropriate Diagnostics
Proteomics
PathogenesisEpidemiology Quality Standards for Host Immune
Response
Animal models
Regulatory Approval
Diagnostic Targets
Product Prototype
Lab & field evaluations
Test adoption
Test introduction: implementation research
Proof of PrincipleProduct
SpecificationsTechnology platform
Microscopy
serology
MicrofluidicsDiagnostics used appropriately to improve health outcomes
Nanotechnolgyto improve health outcomes
