hyperthyroidism & anaesthetic implications
TRANSCRIPT
Chairperson – Dr.S.B.Gangadhar
Moderator – Dr. Amitha
Presenter – Dr. Daber Pareed
HyperthyroidismAnaesthetic implications
Introduction
• Anterior to trachea
• Just below cricoid cartilage
• Covering second through fourth tracheal rings
• Thyroid gland weighs about 20 gm
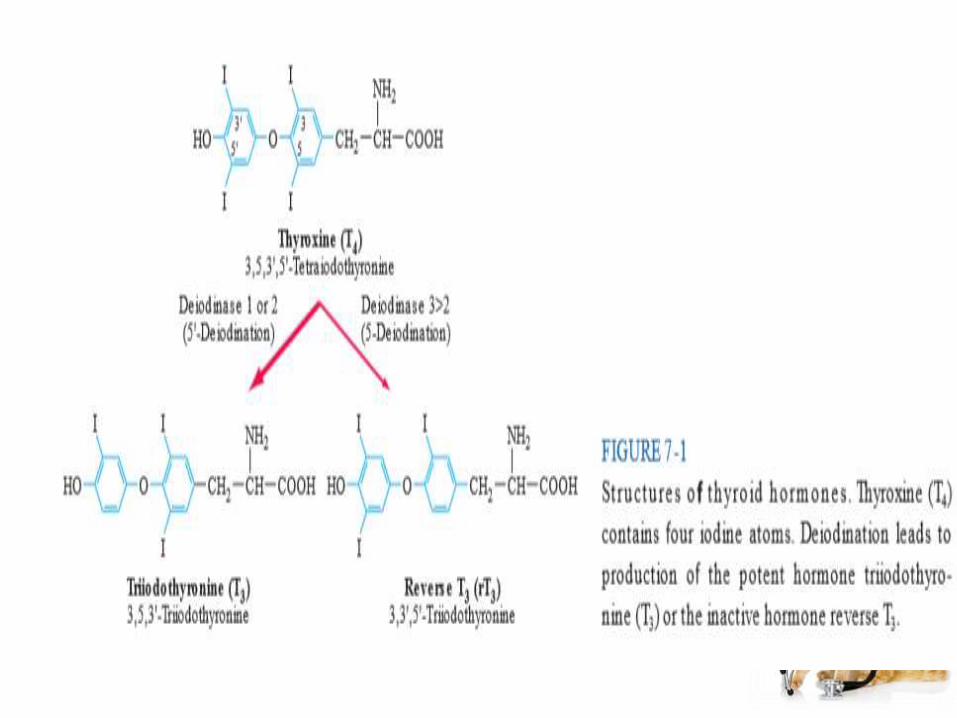
• Thyroid gland produces two related hormones, thyroxine ( T4) and triiodothyronine ( T3).
• Acting through thyroid hormone receptors α and β, these hormones play a critical role in cell differentiation during development and help maintain thermogenic and metabolic homeostasis in the adult.
• Autoimmune disorders of the thyroid gland can stimulate overproduction of thyroid hormones (thyrotoxicosis) or cause glandular destruction and hormone deficiency (hypothyroidism).
Anatomy & Development
• Thyroid (Greek thyreos, shield, plus eidos, orm) consists of two lobes connected by an isthmus.
• It is located anterior to the trachea between the cricoid cartilage and the suprasternalnotch
• Four parathyroid glands, which produce parathyroid hormone, are located posterior to each pole of the thyroid.
• The recurrent laryngeal nerves traverse the lateral borders o the thyroid gland and must be identified during thyroid surgery to avoid injury and vocal cord paralysis.
• The thyroid gland develops from the floor of the primitive pharynx during the third week of gestation.
• The developing gland migrates along the thyroglossal duct to reach its final location in the neck.
• This feature accounts or the rare ectopic location of thyroid tissue at the base of the tongue (lingual thyroid) as well as the occurrence of thyroglossal duct cysts along this developmental tract.
• Thyroid hormone synthesis normally begins at about 11 weeks’ gestation.
• Neural crest derivatives from the branchialbody give rise to thyroid medullary C cells that produce calcitonin, a calcium-lowering hormone.
• The cells are interspersed throughout the thyroid gland, although their density is greatest in the juncture of the upper one-third and lower two-thirds of the gland.
• Calcitonin plays a minimal role in calcium homeostasis in humans but the C-cells are important because of their involvement in medullary thyroid cancer.
• The thyroid gland consists of numerous spherical follicles composed of thyroid follicular cells that surround secreted colloid, a proteinaceous fluid containing large amounts of thyroglobulin, the protein precursor of thyroid hormones.
• The thyroid follicular cells are polarized—the basolateral surface is apposed to the bloodstream and an apical surface faces the follicular lumen.
• Increased demand for thyroid hormone is regulated by thyroid-stimulating hormone ( TSH), which binds to its receptor on the basolateral surface of the follicular cells.
Regulation of the Thyroid axis
• TSH, secreted by the thyrotrope cells of the anterior pituitary, plays a pivotal role in control of the thyroid axis and serves as the most useful physiologic marker of thyroid hormone action.
• TSH is a hormone composed of α and β subunits; the α subunit is common to the other glycoprotein hormones (luteinizing hormone, follicle-stimulating hormone, human chorionic gonadotropin [hCG]), whereas the TSH β subunit is unique to TSH.
• The extent and nature of carbohydrate modification are modulated by thyrotropinreleasing hormone (TRH) stimulation and influence the biologic activity of the hormone.
• The thyroid axis is a classic example of an endocrine feedback loop.
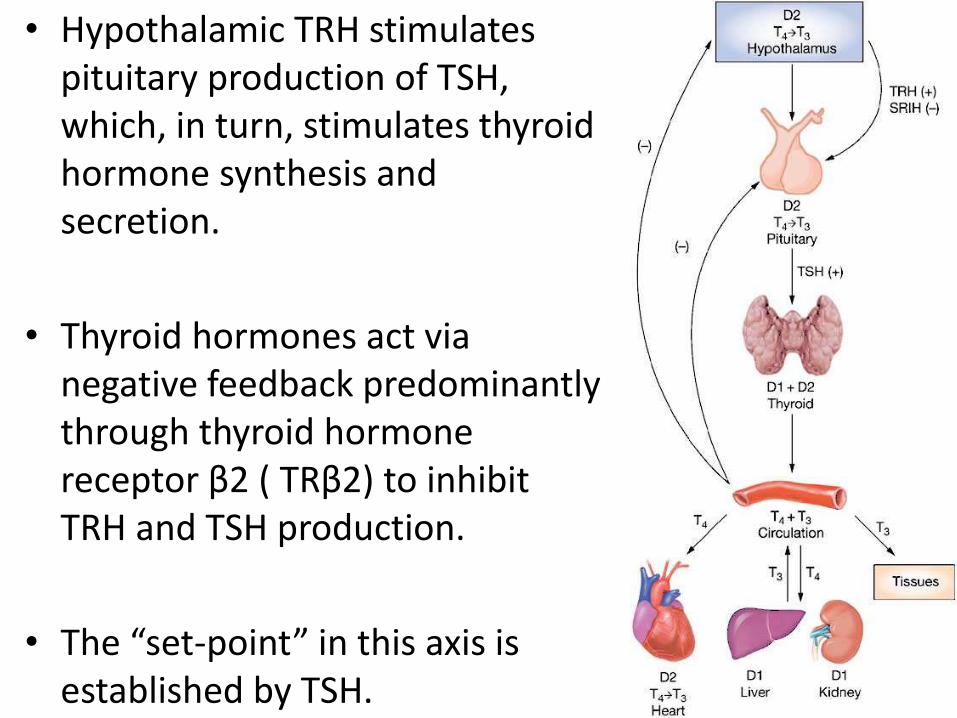
• Hypothalamic TRH stimulates pituitary production of TSH, which, in turn, stimulates thyroid hormone synthesis and secretion.
• Thyroid hormones act via negative feedback predominantly through thyroid hormone receptor β2 ( TRβ2) to inhibit TRH and TSH production.
• The “set-point” in this axis is established by TSH.
• TRH is the major positive regulator of TSH synthesis and secretion.
• Peak TSH secretion occurs within 15mins after administration of exogenous secretion TRH.
• Dopamine, glucocorticoids and somatostatin suppress TSH but are not of major physiological importance except when these agents are administered in pharmacological doses.
• Reduced levels of thyroid hormone increase basal TSH production and enhance TRH-mediated stimulation of TSH.
• High thyroid hormone levels rapidly and directly suppress TSH gene expression secretion and inhibit TRH stimulation of TSH, indicating that thyroid hormones are the dominant regulator of TSH production
Hyperthyroidism
• Clinical hyperthyroidism, also called thyrotoxicosis, is caused by the effects of excess thyroid hormone and can be triggered by different disorders.
• The prevalence of hyperthyroidism in community-based studies has been estimated at 2 percent for women and 0.2 percent for men.
• As many as 15 percent of cases of hyperthyroidism occur in patients older than 60 years.
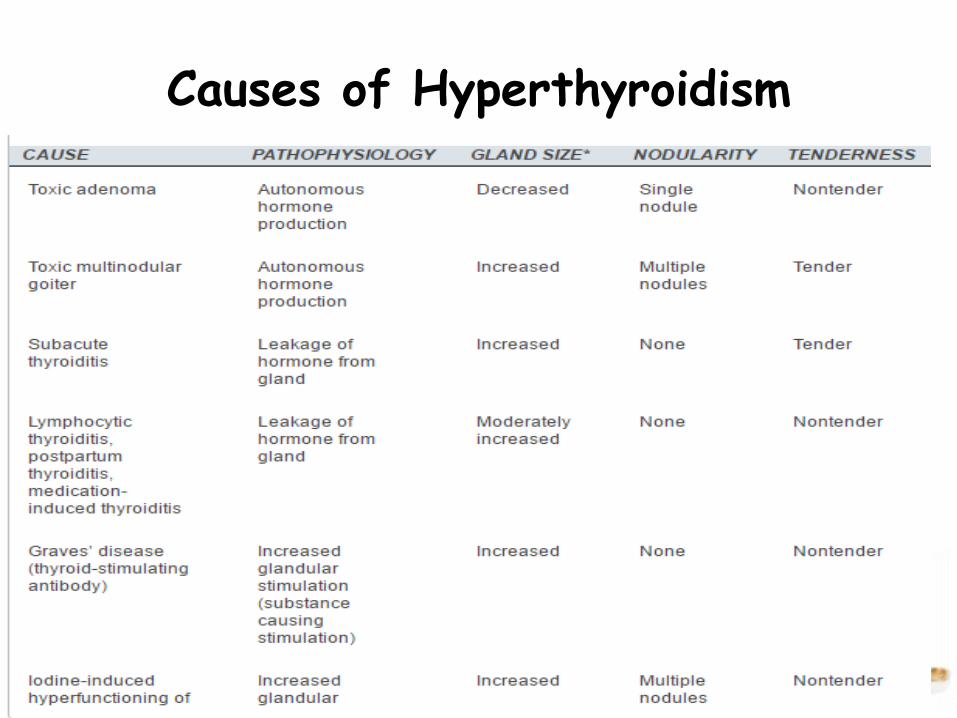
Causes of Hyperthyroidism
Clinical features
General-
Weight loss, tremor and heat intolerance, sweating, fatigue
CVS-
Tachycardia, Cardiac arrhythmias, Wide pulse pressure, heart failure.
Respiratory - Dyspnoea
GIT- Diahorrea,Nausea and vomiting
CNS- Anxiety, irritability, insomnia, Depression
Neuromuscular- Proximal myopathy, muscular weakness.
Ophthalmic-
Lid lag, Lid retraction reduced blinking, exophthalmos, corneal ulceration, loss of visual acuity.
Reproductive-
Amenorrhea, Oligomenorrhea infertility, impotence.
Thyroid hormones cause uncoupling of oxidative phosphorylation such that energy cannot be stored and increase heat production. They also have impact on rate and speed at biochemical reactions, total body oxygen consumption and energy production.
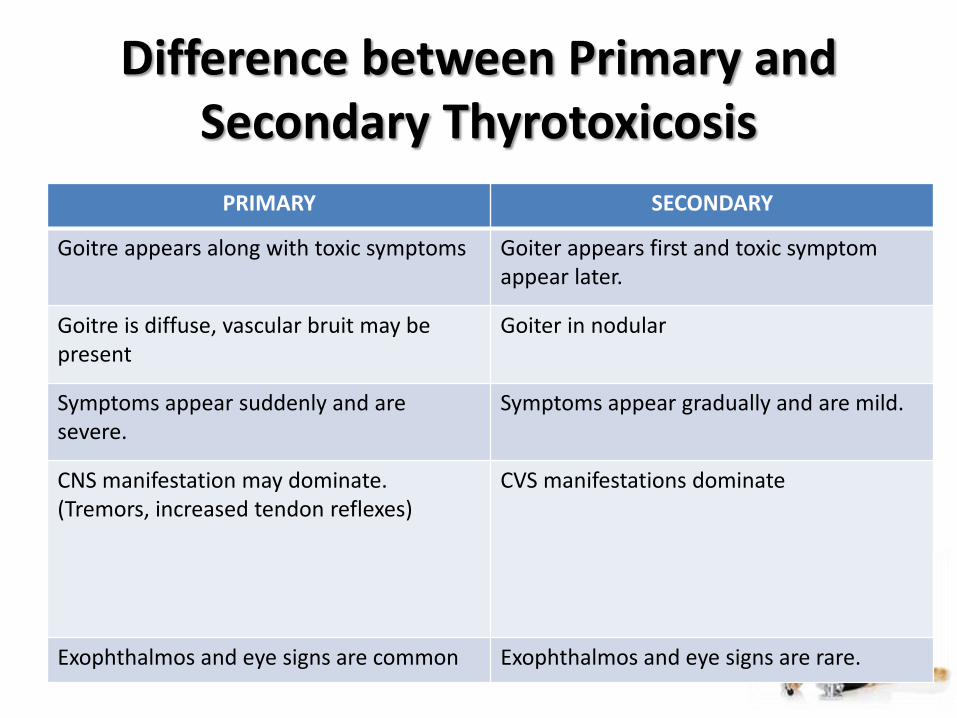
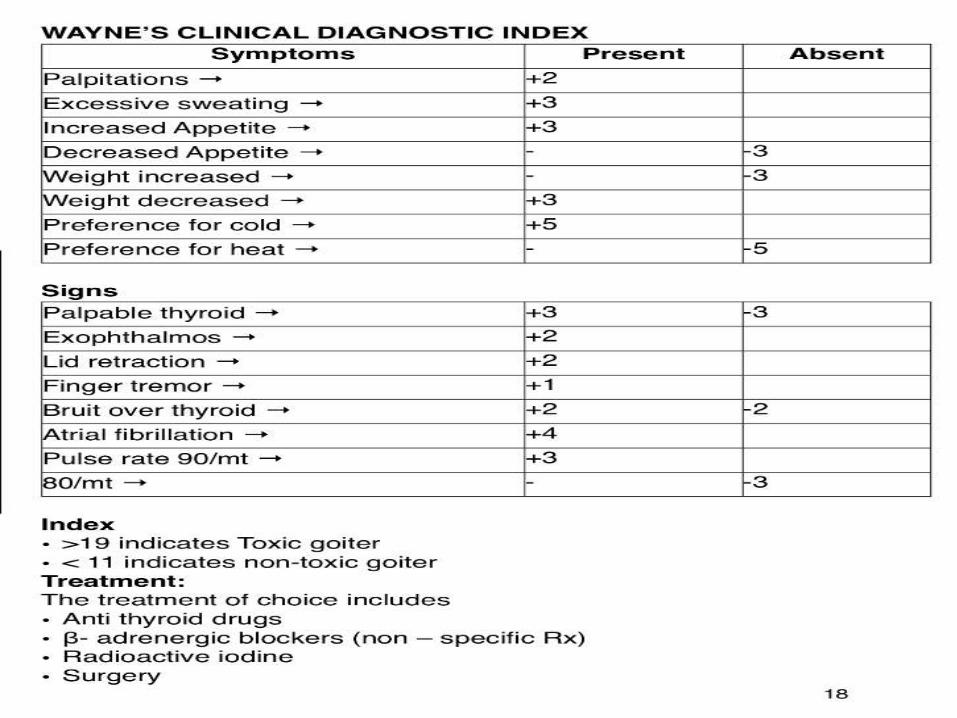
Difference between Primary and Secondary Thyrotoxicosis
PRIMARY SECONDARY
Goitre appears along with toxic symptoms Goiter appears first and toxic symptom appear later.
Goitre is diffuse, vascular bruit may be present
Goiter in nodular
Symptoms appear suddenly and are severe.
Symptoms appear gradually and are mild.
CNS manifestation may dominate.(Tremors, increased tendon reflexes)
CVS manifestations dominate
Exophthalmos and eye signs are common Exophthalmos and eye signs are rare.
Anti thyroid Drugs
Ion inhibitors – Perchlorate, Thiocynate
Thiourea derivatives – Propylthiouracil
Imidazole Derivatives – Carbimazole, Methimazole
Iodides- Lugol’s iodine.
Pre- Operative Evaluation
History – Elicit
• H/o pressure symptoms – Dysphagia (Oesophagus)
• Stridor / Dysponea (trachea)
• Hoarsness of Voice (RLN Involved)
• H/O Symptoms of primary and secondary toxicity.
• H/O pain of the goiter
• Personal history/ past history/ family history
• Drug History
Physical Examination – Look for
• Built, nourishment
• Anemia, Jaundice, edema, cynanosis, clubbing, ascites
• Involvment of bone, spleen, liver for secondaries.
• Temprature, resting/sleeping PR, BP
• Skin cold/warm, moist/dry
• Tremors
• Mental status (anxiety, nervousness)
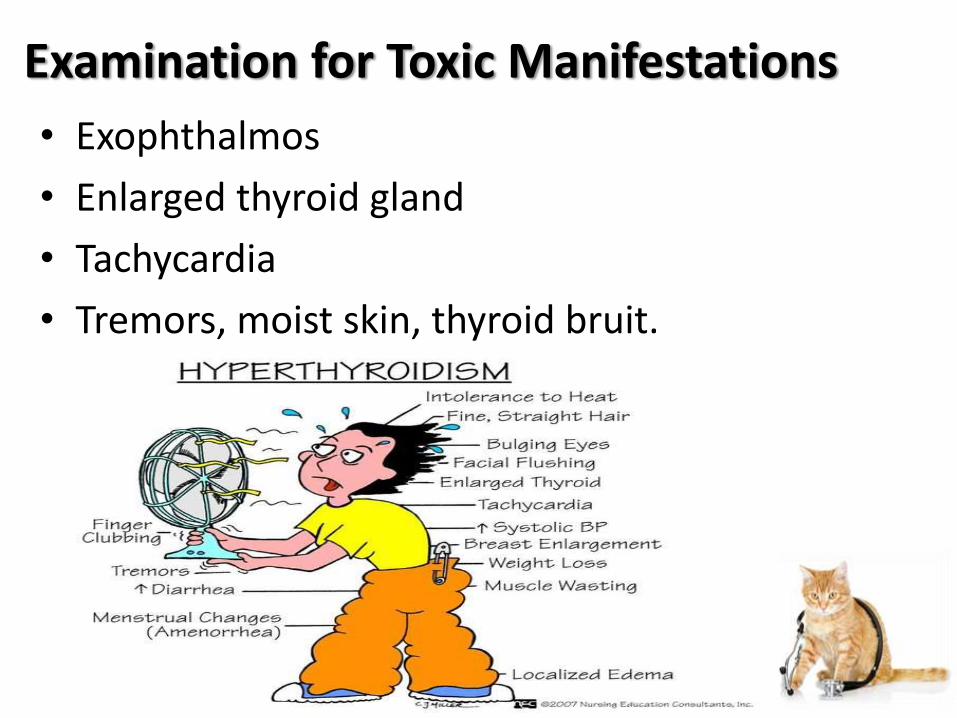
Examination for Toxic Manifestations
• Exophthalmos
• Enlarged thyroid gland
• Tachycardia
• Tremors, moist skin, thyroid bruit.
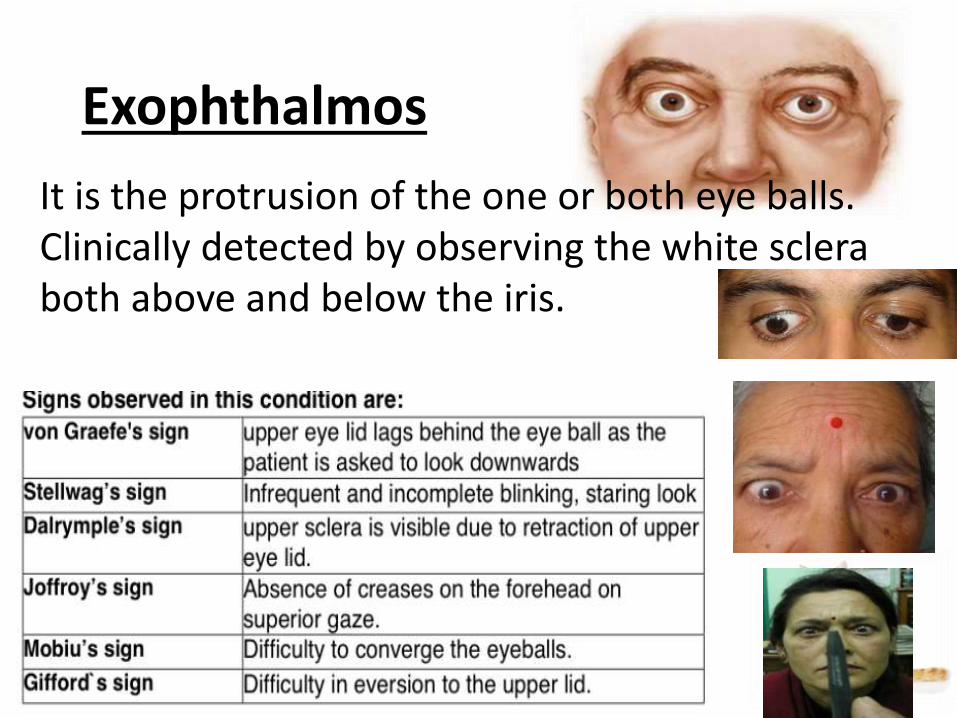
Exophthalmos
It is the protrusion of the one or both eye balls. Clinically detected by observing the white sclera both above and below the iris.
• Tachycardia – sleeping pulse rate
– < 80-90 – mild
– 90-110 – moderate
– 110 – severe.
• Tremors- When the patient asked to hold his hand straight in front of him with fingers spread out – FINE TREMORS ARE SEEN IN THE FINGERS.
Systemic Examination
• CVS –
– Signs and symptoms of CCF, AF
– Enlarged heart
– Systolic murmur may be due to hyper dynamic circulation.
• CNS- temors, myopathy
• Assesment of airway
Investigations
• Hb%• TC, DC, ESR- (Patients on ATD therapy may have anemia)• BT,CT, Platelet count.• Urine- albumin, sugar, microscopy• RBS/BU/SC ( Blood sugar may increased in hyperthyroidism)• Recording sleeping PR• ECG• Serum Electrolytes• Indirect laryngoscopy by ENT surgeon – To asses the vocal cord
movements• Medico legal importance – to know the pre-op and post –op
difference.
X-rayAP view- Position of trachea – deviation, compression.Mediastinal extension in cases of retro. Sternal Goiter.
PA view- Cardiomegaly in CCF Pulmonary congestion in patients with CCF.
Lateral view Barium Swallow – To detect pressure effect on trachea and oesophagus
Flow Volume loops- Best indicators of airway obstruction.
Thyroid Function Tests-
• In vitro Test
• In vivo test
• Miscellaneous test
In Vitro Test
• Estimation of Serum protein Bound iodine (PBI)
Normal – 4-8 𝜇g/dl
• Estimation of total serum T3 and T4
– Measured by radio immune assay
– Normal T4- 5-10 𝜇g/dl
– T3 – 80- 220 ng/dl
In vitro Test
• Influenced by TBG levels.
– T3, T4 levels are increase in Hyperthyrodism.
– Decreased in Hypothyrodism
• T3 – resin uptake
– Normal – 0.9 – 1.2 taking 100 % as the mean normal value.
– 89% or <suggests – Hyperthyrodism
– 121% or > suggests - Hypothyrodism
In vitro Test
• Free Thyroxin index
– F.T.I – serum T4 x T3 uptake %
– Normal – 3.7 – 8.6 %
• Serum TSH
– Normal 1-5 𝜇U/ml
– Increase in Hyperthyrodismupto 40𝜇U/ml
– Decreased in Hypothyrodism
In vivo Test
• Uptake tests –– Thyroid uptake normal 30% in 24 hrs
– In hyperthyroidism increase > 55%
– In Hypothyrodism decreased.
• T3 Suppression test (Werner)– Helps to differentiate thyrotoxicosis from other causes
of raised uptake
– Initial uptake is measured.
– In thyrotoxicosis – suppression is only by 10-20%
TSH stimulation Test
• Helps in distinguishing between primary and secondary hypothyroidism.
– Initial thyroid uptake is measured.
– Increase in uptake in Hypopitutarism
– No increase in uptake primary thyroid failure.
Pre- operative Prepration of the patient
• Before elective surgeries patient must be made euthyroid.
• Euthyroid state is clinically assessed by
– Sleeping PR< 80bpm
– Normal TFT
– Disappearance of Toxic symptoms like nervousness, anxiety, tremors, etc.
During Emergency Surgery
• Measures should be taken prevent thyroid storm.
• ATD should start immediately
• Esmolol 100 -300𝜇g/kg/min IV until HR comes <100/hr
• Dexamethasone 2mg 6th hourly IV
• Hydrocortisone 40mg 6th hourly IV
• Kl drops (60 mg) PO every 6 hourly– Or Lugols solution 30 drops 6-8hourly.
• Antithyroid drugs and beta blockers should be continued till the morning of the surgery.
Premedication
• To prevent the sympathetic activity• To relieve anxiety• Tab. Diazepam - 5-10mg PO• Inj. Promethazine 50mg IM or ½ hr – 1 hr before
surgery.• Inj. Morphine 10mg IM
• No premedication– If airway problem is anticipated. Anticholinergic drugs
are not recommended.
Intra-Op monitoring
• HR
• BP
• Oxygen saturation
• ECG
• Body temperature
• ET CO2
• CVP
• Doppler, Echocardiography– To detect air embolism
General Anaesthesia
Preoxygenation with 100% O2 is a must
• Increased Basal metabolic rate
• Hypoxia may stimulate sympathetic nervous system
Induction
• Before induction all the emergency drugs & equipment required during difficult intubation should be kept ready.
• If no airway problem is anticipated.– Induction with Thiopentone sodium 3-5mg IV
– Inj. Lidocaine 2 %- To attenuate pressure response during laryngoscopy
– Relaxation with Inj. Scholine 1-2 mg IV
– Intubation with cuffed armoured tube.
• If airway problem is anticipated
(dyspnea, dysphagia, hoarsness of voice etc)
– Induction with O2 + N2O+ Isoflurane
– Intubation with cuffed armoured tube.
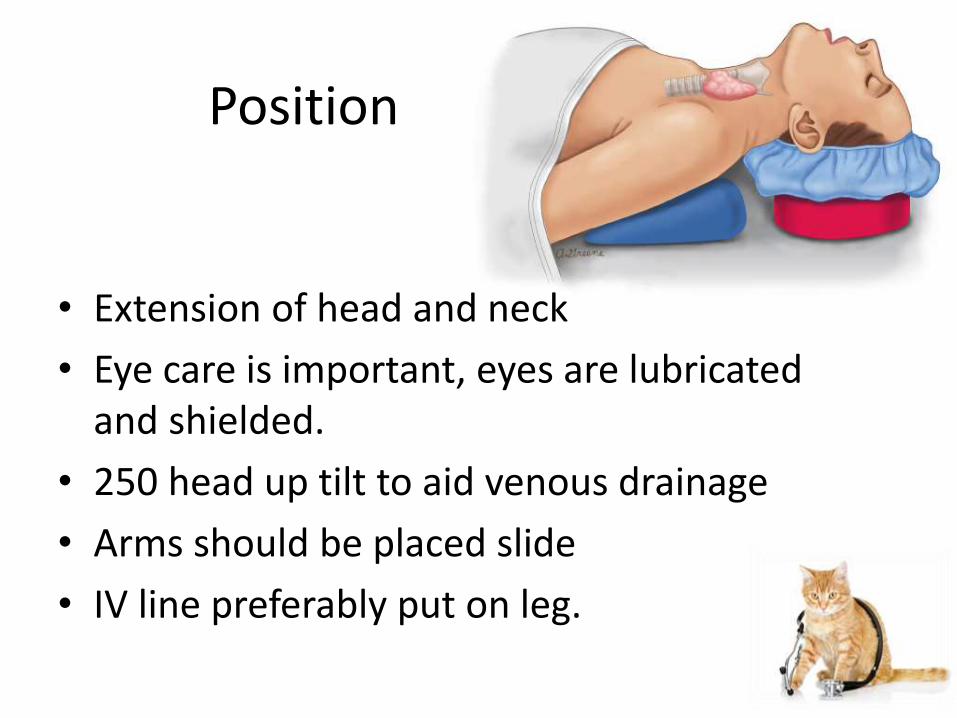
Position
• Extension of head and neck
• Eye care is important, eyes are lubricated and shielded.
• 250 head up tilt to aid venous drainage
• Arms should be placed slide
• IV line preferably put on leg.
Maintenance of Anaesthesia
GOALS
• Avoid drugs which stimulate SNS
• Provide sufficient anaesthetic depth to prevent exaggerated response to surgical stimulation.
• Isoflurane is the volatile anaesthetic of choice.
Muscle relaxants
• In Vecronium – 0.03-0.05mg/Kg IV
• In Atracurium – 0.3-0.5 mg/Kg IV
• Pancuronium and Gallamine are not the better choice as they increase HR
• The existing skeletal muscle weakness and incidence of mysthenia gravis in hyperthyroid patients emphasizes the need to reduce initial dose of muscle relaxant.
REVERSAL
• Inj. Neostigmine 0.05mg/Kg
+
Inj. Glycopyrolate 8-10 µg/Kg
• Glycopyrolate is preferred than atropine – less chromotropic effect than atropine.
EXTUBATION
• Deep extubation
• Laryngoscopic vision is preffered to assess the vocal cord function
• Administration of lidocaine IV 60-90mg prior to extubation.
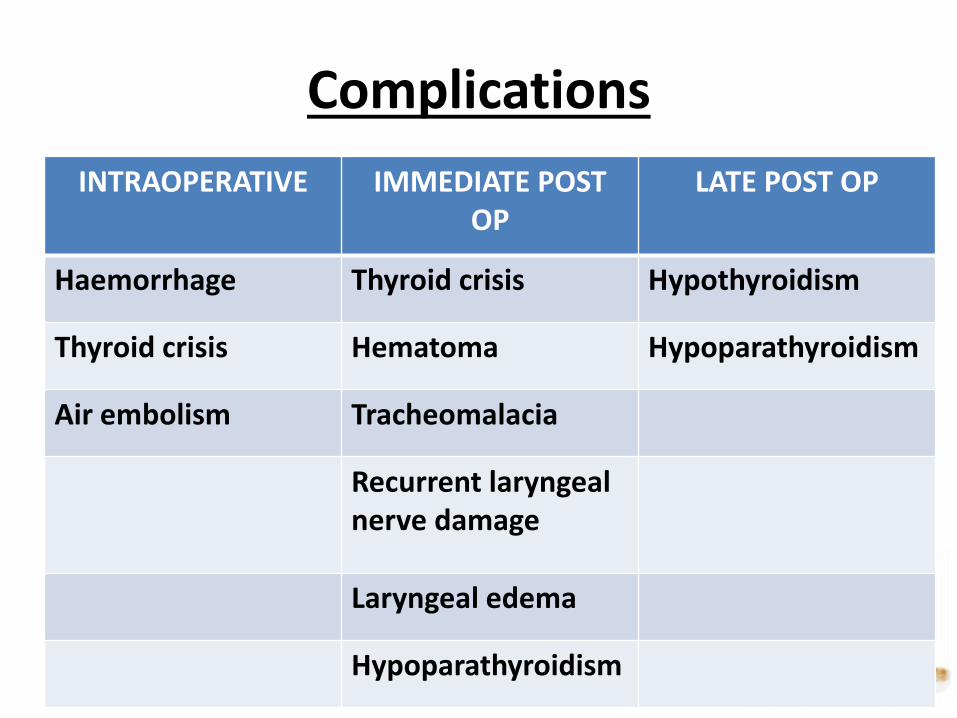
Complications
INTRAOPERATIVE IMMEDIATE POST OP
LATE POST OP
Haemorrhage Thyroid crisis Hypothyroidism
Thyroid crisis Hematoma Hypoparathyroidism
Air embolism Tracheomalacia
Recurrent laryngeal nerve damage
Laryngeal edema
Hypoparathyroidism
Thyroid storm
• It is an abrupt exacerbation of hyperthyroidism caused by sudden excessive release of thyroid gland hormones in the circulation.
• Predisposing factors-
– Medical factors
– Surgical factors
Medical factors
a) Infection, fever, uncontrolled toxicity
b) Improper treatment
1. Irregular drug intake
2. Improper/ inadequate investigation
3. Stopping drug well in advance to surgery
c) Pregnancy
d) Anxious and nervous patients before surgery
Surgical factors
a) Too much handling of gland before surgery
b) Rough handling of gland during surgery
• This complication can occur both intra-operatively or in the immediate post-op periods.
• It is common in post-operative period. It occurs between 6-18 hours post operatively.
Clinical features
Hyperthermia
Rise of 2 degree Celsius/hr over normal temperature.
It may be difficult to notice during operation because the surgery may not last for more than 1 -1 ½ hr.
Clinical features
TachycardiaArrhythmias of any kind may occur, atrial fibrillation is
the commonest.
Initially there is flushing and sweating, later leading to dehydration.
CCF Initially high output failure, later may go for low output failure.
Electrolyte imbalance
Marked agitation, anxiety and psychosis.
Clinical features under anaesthesia
1. Hyperthermia
2. Tachycardia
3. Hypertension
4. High output failure and then low output failure
5. Arrhythmia
6. Flushing or sweating
7. Increase ETCO2
8. Hypo/ hyperglycemia
Differential diagnosis
A. Malignant hyperthermia
B. Pheochromocytoma
Treatment
General Measures
I. Increase the percentage of inspired O2 concentration.
II. Cooling measuresA. Surface cooling sponging, Icepack, decreasing OT
temperature.
B. Administration of cold IV fluid.
III. Avoid Aspirin- as it competes for thyroxinebinding globulin and hence releases more T3-T4 into circulation, aggravating the condition
Suppression of hormone activity:
1. Propylthiouracil 200-400 mg IV/orally through Ryle’s tube 8th hrly.
2. Carbimazole50-100mg Orally (RT) followed by 20mg 6th hrly.
3. Na iodide 500-1000 mg IV 8th hrly.
Treatment
TreatmentSuppression of sympathetic activity
I. Propanolol 1-2 mg IV sufficient to decrease HRII. Esmolol 50-300 µg/Kg/minIII. Treatment of shock and CCFIV. CCF due to increase in ventricular rate, it will respond to
esmolol – by decreasing HRV. Digoxin High output failure may not respond to
digoxin.VI. IV fluids should be given with reference to CVP.VII. IV fluid preferbly the crystalloid containing glucose to
supply enough energy for increased metabolism.VIII. Supplementation of corticosteroid.IX. Hydrocorticosone 100-200mg IV 8th or sometimes as high
as 500mg initial dose may be given.
Treatment
• Dexamethasone prevent conversion of T4 T3, prevents release of T4.
• If it is during intraoperative handling of gland should be stopped and should stabilize the patient.
Tracheomalacia
• It occurs after removal of long standing goiter, especially the thoracic inlet, that has compressed and weakened cartilaginous rings supporting the tracheal wall.
• Immediate intubation or tracheostomy should be performed.
• Later options include stenting, extrinsic tracheal support, tracheoplasty.
Hematoma
• Haemorrage into tracheal bed following surgery results in tracheal compression and respiratory distress.
• The wound should be reopened immediately at the bedside to relieve the compression and patient should be shifted to OT secure homeostasis.
Hypoparathyroidism
• Result from accidental removal of parathyroid gland.
• Hypocalcemia develops typically 24-72 hrs post operatively, but may manifest as early as as 1-3 hrs after surgery.
• Laryngeal muscles are sensitive to hypocalcemiaand inspiratory stridor progressing to laryngospasm, may be the first indication.
• TREATMENT – IV Calcium until laryngeal stridorceases.
Regional anaesthesia
• Regional anaesthesia is a potentially useful choice for hyperthyroid patient.
• Epidural anaesthesia is preferred over spinal because of slower onset of sympathetic system blockade.
• If hypotension occurs, decreased dose of phenylephrine is recommended.
• Ephedrine increases catecholamine release and increases symapthetic nervous system activity, so better avoided.
References
• Harrison’s Endocrinology – 4th Edition
• Tripati book for Parmocology
• Millers Text book of anaesthesiology
• Spotlight Text book for anaesthesiology
• Barash clinical anaesthesia 7th edition
• Stoelting’s Pharmocology and Physiology in anaesthetic practice
Thank you....