la salute sessuale nella donna dalla età fertile alla ... del tibolone in... · ruolo del tibolone...
TRANSCRIPT

Ruolo del Tibolone in MenopausaA chi. Quali vantaggi. Quali svantaggi
La Salute Sessuale nella Donna dallaEtà fertile alla Menopausa
Bologna, 16 Maggio 2009
A chi. Quali vantaggi. Quali svantaggi
Stefano Lello
Ginecologia Endocrinologica, Fisiopatologia della Menopausa e dell’Osteoporosi
IRCCS-Istituto Dermopatico dell’Immacolata - Roma

Tibolone: un composto STEARSTEAR:
Selective, Tissue Estrogenic Activity Regulator
(Regolatore Tessuto-Selettivo della Attività Estrogenica)

TiboloneTibolone -- metabolismometabolismo
Pool ofPool ofSulfatedSulfated
compoundscompounds
SulfotransferaseSulfotransferase
SulfataseSulfatase
HO
HH
HO
HH33ββββββββ--HSDHSD--IsomeraseIsomerase
HOHO
OH
H
H
H
3 OH tiboloneα- -
TiboloneO
H
HH
H
∆4 isomerO
H
HH
H
∆4 isomer-
33ββββββββ--HSDHSD--IsomeraseIsomerase
HOHO
OH
H
H
H
3 OH tiboloneβ- -Tibolone

Regolazione degli enzimi nella mammellaRegolazione degli enzimi nella mammella
Estradiol
17 -HSDβType I
Estradiol
17 -HSDβType II
Estrone sulfate3OH-tibolone sulfate
SulfotransferaseSulfotransferase
Estrone sulfate3OH-tibolone sulfate
Sulfatase
DHEA AndrostenedioneAndrostenedioneDHEADHEASDHEAS
Estrone3OH-tibolone
Estrone3OH-tibolone
Aromatase
SulfotransferaseSulfotransferase

Effetti sul sistema solfotransferasiEffetti sul sistema solfotransferasi--solfatasi solfatasi previene la stimolazione della mammellapreviene la stimolazione della mammella
CompostiComposti
SolfotrasferasiSolfotrasferasi
CompostiComposti
SulfatasiSolfatasi
CompostiCompostiattiviattivi
CompostiCompostiinattiviinattivi

Regolazione degli enzimi a livello endometriale
EstradiolEstrone sulfate
3OH-tibolone sulfate
Solfotrasferasi
17β-HSDTipo I
17β-HSDTipo II
Sulfatase
EstradioloEstrone solfato3OH-tibolone solfato
∆4∆4
∆∆Estrone
3OH-tibolone
Solfotrasferasi
∆4-tibolone
Estrone3OH-tibolone
Tibolone ∆4-tibolone
∆4∆4
3β-HSD-iso

Meccanismo di azione del tibolone
Bone(Brain, CVS, Vagina)
Breast Endometrium
ER activation
Tibolone
Active metabolites
Receptors and Enzymes
yes minor minorER activation
PR activation
Sulfatase inhibition
Sulfo transferase induction
Tissue stimulation
Estrogenicstimulation
Absence of tissue stimulation
Less activeestrogenic compounds
Progestagenicdominant
yes
no
no
enzymeabsent
minor
no
yes
yes
minor
yes
yes
yes

• Obiettivo primario: confrontare il pattern di sanguinamentovaginale durante la somministrazione per 48 mesi di Tibolone 2.5mgeHRT combinatacontinualow-dose(E2 1 mg + NETA 0.5 mg)mgeHRT combinatacontinualow-dose(E2 1 mg + NETA 0.5 mg)
• Obiettivo secondario: efficacia su sintomi vasomotori e atrofiavaginale
• Campione studiato: 572 PMW (range età: 45-65 aa: media 55)
Hammar et al, BJOG 2007Studio TOTAL

Studio TOTALPercentuale di donne con sanguinamento
(B o S per almeno 1 giorno) durante 4 trimestri di studio
Hammar et al, BJOG 2007

Studio TOTAL Numero mediano di vampate durante il periodo di
trattamento
Hammar et al, BJOG 2007

Studio TOTAL Citologia Vaginale
Hammar et al, BJOG 2007
Studio TOTAL Segni e sintomi mammari (dolore/tensione)
Gruppo E2/NETA: 9.8 %
vsvs
Gruppo Tibolone: 3.2 %
p < 0.001
Hammar et al, BJOG 2007

- AIM OF THE STUDYTo compare the treatment effect of tibolone (2.5 mg)
J Sex Med, 2008
To compare the treatment effect of tibolone (2.5 mg) to continuous combined transdermal E2/NETA
(50/140µg) on sexual functioning in healthy postmenopausal women with sexual dysfunction.
- Main Outcome Measure: Female Sexual Function Index (FSFI)

% changefrom baseline
TIBOLONE
FSFI and TIBOLONE IN NATURALLYMENOPAUSAL WOMEN - LISA STUDY
Per Protocol Analysis
30
40 E2/NETA
*<
**
FSFI-CS
Nijiland et al, 2008
0
10
20
30
FSFI-TS
<
Of the 403 women randomized 293 (73%) completed the 24-week treatment period*p < 0.036 for Tib vs E2/NETA**p< 0.025 for Tib vs NETA FSFI-CS = Female Sexual Funtion Index Compositte Score:
arousal, desire, satisfaction

LISA StudyCambiamento medio % vs baseline per i diversi domini del
FSFI per gruppo di trattamento alla settimana 24
p< 0.001 vs baseline per tutti i singoli dominiper entrambi i gruppi di trattamento
Nijiland et al, 2008

Lisa Studyconclusions
Both treatments resulted to improved overall sexual function, as determined by scores on the FSFI, with an
increase in the frequency of sexual events, and a reduction in sexuality-related personal distress. in sexuality-related personal distress.
The statistically
significant higher FSFI scores in the tibolone group, when compared to the E2/NETA group, may be because of
tibolone’s combined estrogenic and androgenic properties.

Studio THEBES(Tibolone Histology of the Endometrium and Breast
Endpoints Study)
• Trial randomizzato in doppio cieco, a gruppi paralleli• Obiettivo primario: confermare la sicurezza
endometriale del tibolone (1,25 e 2,5 mg/die)• Obiettivo secondario: valutare il profilo di tollerabilità • Obiettivo secondario: valutare il profilo di tollerabilità
confrontando l’incidenza di sanguinamenti vaginali e di mastodinia in pazienti trattate con tibolone vs ECE/MAP
• Trattate in tutto 3224 pazienti (range età: 45-65 aa; media 54.4)
• 792: 1,25 mg tibolone• 806: 2,5 mg tibolone• 1626: ECE/MAP Archer et al, JCEM 2007
3 gruppi di trattamento

Studio THEBESrisultati
• Non casi di iperplasia nei due gruppi di trattamento con tibolone
• Nel gruppo con ECE/MAP 2 casi di iperplasia
• Ecopattern endometriale (TVS): • Ecopattern endometriale (TVS):
• Tibolone: basale 3,1 mm; dopo 2 aa: 3,6 mm
• ECE/MAP: 3,0 mm; dopo 2 aa: 3,4 mm
Archer et al, JCEM 2007
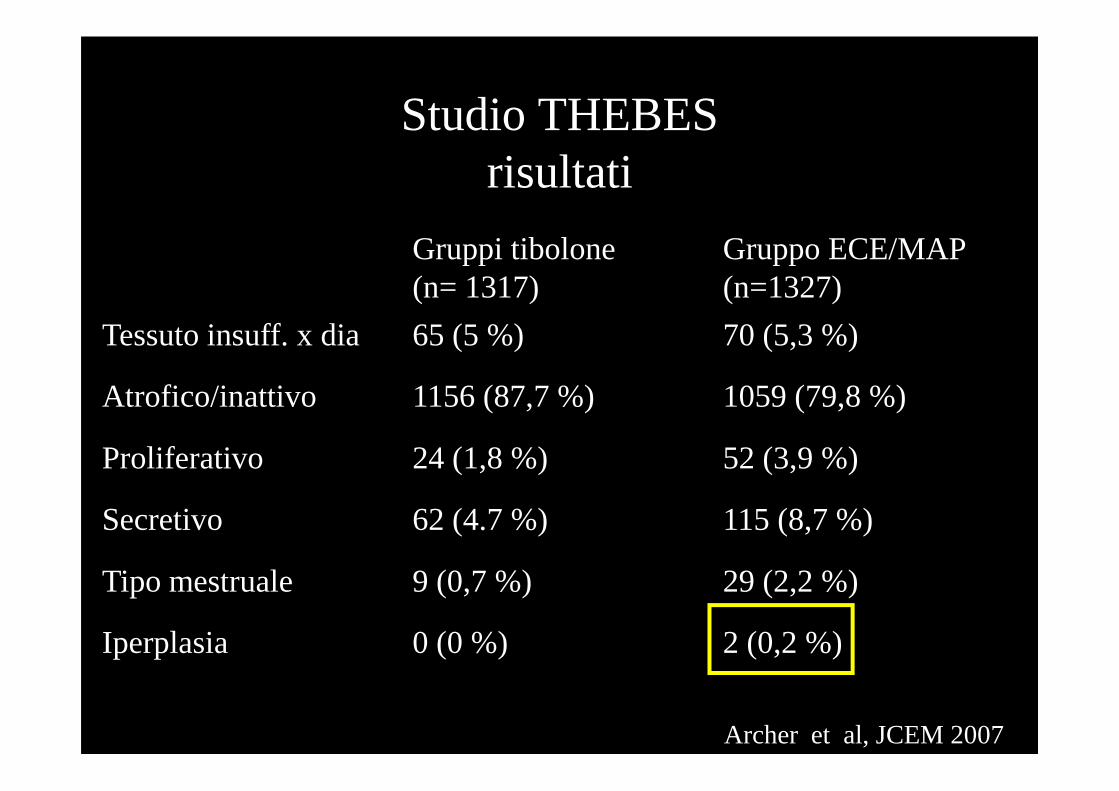
Studio THEBESrisultati
Gruppi tibolone(n= 1317)
Gruppo ECE/MAP (n=1327)
Tessuto insuff. x dia 65 (5 %) 70 (5,3 %)
Atrofico/inattivo 1156 (87,7 %) 1059 (79,8 %)Atrofico/inattivo 1156 (87,7 %) 1059 (79,8 %)
Proliferativo 24 (1,8 %) 52 (3,9 %)
Secretivo 62 (4.7 %) 115 (8,7 %)
Tipo mestruale 9 (0,7 %) 29 (2,2 %)
Iperplasia 0 (0 %) 2 (0,2 %)
Archer et al, JCEM 2007

Percentuale di soggetti senza episodi di B/S Vaginale – Studio THEBES
Archer et al, JCEM 2007

Studio THEBESIncidenza di eventi avversi cardiovascolari (tutti i soggetti
trattati) (range età: 45-65 aa; media 54.4 )
Archer et al, JCEM 2007

Studio THEBESConclusioni
• Il tibolone non induce iperplasia o carcinoma endometriale
• L’incidenza di endometrio atrofico/inattivo risultava maggiore nelle pazienti trattate con tibolone vs ECE/MAP (87,9 % vs 79,8 %)(87,9 % vs 79,8 %)
• Il tibolone ha un profilo di sanguinamento migliore vs ECE/MAP: 75 % no sanguinamento/spotting con tib. vs 45 % con ECE/MAP
• Mastodinia meno frequente con tib. (2,3 %) vs ECE/MAP (9,7 %)
Archer et al, JCEM 2007

Eur Heart J, 2006

Studio OPAL(Osteoporosis Prevention and Arterial effects of tiboLone
study)
Bots et al, EHJ, 2006

OPAL StudyObjective:The primary objective was to compare the effect of tibolone and placebo on theprogression of the common carotid artery intima-medial thickness; A secondary objectivewas to assess the effects of tibolone (2.5 mg), continuous combined CEE/MPAe [0.625/2.5mg], and placeboon the endometrium and vaginal bleeding.
Design:3-year, three-arm, randomized, double-blind, parallel group, placebo-controlled clinical trial
Partecipants:866 postmenopausal women (aged 45-79 years).
Results (I):Endometrial thicknessincreased slightly during the first year with tiboloneand HRT without any further progression .

Studio OPALbiopsie endometriali
Langer et al, Am J Ob Gyn, 2006

Studio OPALepisodi di bleeding/spotting
Vaginal bleeding was more commonly reported as an
adverse event with CEE/MPA than tibolone (26.4% vs 10.8%,
Langer et al, Am J Ob Gyn, 2006
than tibolone (26.4% vs 10.8%, P < .0001)

TIBOLONE AND ENDOMETRIUM
OPAL Study
Objective:The primary objective was to compare the effect of tibolone and placebo on theprogression of the common carotid artery intima-medial thickness; A secondary objectivewas to assess the effects of tibolone (2.5 mg), continuous combined CEE/MPAe [0.625/2.5mg], and placeboon the endometrium and vaginal bleeding.Design:3-year, three-arm, randomized, double-blind, parallel group, placebo-controlled clinical trialPartecipants:866 postmenopausal women (aged 45-79 years).
Results (I):
After 3 years, there were no significant differences between the tibolone, HRT andplacebo groups in:
- incidence of proliferation (1.4%, 4.8%, and 0%, respectively),
- endometrial hyperplasia (0% in all groups),
- cancer (1, 0, and 1 case, respectively).

Tibolone (STEAR) e Tessuto Osseo
• Azione estrogenica mediata dal legame e dall’attiv azione
dei recettori per gli E
• Nessuna inibizione della solfatasi (disponibilità di
composti estrogenici attivi)
Prevenzione della perdita di massa ossea e aumento della densità minerale ossea

Osteoporotic Fracture Rate, BMD, and Absolute Number of Women
with a Fracture by Baseline T-score
25
30
35
40
45
50
Fra
ctur
e R
ate
Per
1,0
00 P
erso
n-Y
ears
Fracture rate
BMD distribution
n=149,524
250
300
350
400
450
No.
of W
omen
With
Fra
ctur
es
Absolute no. fractures
Siris ES, et al. Arch Intern Med 2004; 164:1108-1112.
5
10
15
20
25
BMD
Fra
ctur
e R
ate
Per
1,0
00 P
erso
n
0>1.0 1.0 to
0.50.5 to
0.00.0 to –0.5
–0.5 to –1.0
–1.0 to –1.5
–1.5 to –2.0
–2.0 to –2.5
–2.5 to –3.0
–3.0 to –3.5
<–3.50
50
100
150
200
No.
of W
omen
With
Fra
ctur
es
52 % donne con Fx ha T-score tra -1.0 e -2.5

Effetti di precedenti Fratture Vertebrali sul Rischio di Fratture Vertebrali successiveEffetti di precedenti Fratture Vertebrali sul Rischio di Fratture Vertebrali successive
10
15
Inci
denz
a di
Nuo
ve F
rattu
re
Ver
tebr
ali (
%)
RR=7.3
RR=5.1
Primo anno di studio
Mod. da Lindsay R et al., JAMA 2001;285:320-23
0
5
Inci
denz
a di
Nuo
ve F
rattu
re
Ver
tebr
ali (
%)
Numero di Fratture Vertebrali all’inizio dell’osservazione
RR=2.6
0 1 ≥1 ≥2

Effect of tibolone and anti-hormones on bone
Tibolone and its effects on bone
Placebo
Tibolone
Tibolone +
Tibolone + anti-
androgen
Tibolone + anti-
progestogen**
400
300*
*
BMD
(mg/cm³)
Adapted from Ederveen and Kloosterboer, J Bone Min Res 2001
Tibolone acts as an estrogen on bone
Tibolone + anti-estrogen
p<0.05 vs OVX
p<0.05 vs Tib.
*
#
#
Treatment (µg/rat/day, orally)
Placebo
200
100
0INT OVX 2 x 125 2 x 125 2 x 125 2 x 125
BMD
(mg/cm³)

The OPAL study BMD data from a three-year, double-blind, randomized study comparing the effects of
tibolone, CEE/MPA and placebo in postmenopausal women.
Tibolone 2.5 mg(n = 247)
CEE/MPA(n= 255)
Placebo(n = 257)
Percentage of change in bone mineral density from baseline to 36 months of treatment (ITT)
Langer et al., 2003
(n = 247) (n= 255)
Lumbar spine (L2–L4) +4.22%
Total hip
Femoral neck
Femoral trochanter
CEE/MPA 0.625 mg conjugated equine estrogens/ 2.5 mg medroxyprogesterone acetate
+ 3.61%
+ 3.10%
+ 6.18%
+4.56%
+ 3.01%
+ 3.31%
+ 5.61%
- 1.96%
- 1.05%
- 0.27%
+ 0.36%

1.5
2
2.5
3
% Change from Baseline
Spine BMD at the End of 24 months *
*
n = 770
Tibolone is Effective in Preventing Postmenopausal Bone Loss
Tibolone and its effects on bone
-2.5
-2
-1.5
-1
-0.5
0
0.5
1
1.5
Placebo Tibolone
0.3 mg
Tibolone
0.625 mgTibolone 1.25 mg
Tibolone
2.5 mg
Adapted from Gallagher et al., J Clin Endocrinol Metab 2001
* p < 0.05 vs. placebo
*
*

1.5
2
2.5
% Change from Baseline
Total hip BMD at the End of 24 months
**
*
n = 770
Tibolone is Effective in Preventing Postmenopausal Bone Loss
Tibolone and its effects on bone
-2
-1.5
-1
-0.5
0
0.5
1
Placebo Tibolone
0.3 mg
Tibolone
0.625 mgTibolone
1.25 mg
Tibolone
2.5 mg
Adapted from Gallagher et al., J Clin Endocrin Metab 2001
* p < 0.001 vs. placebo
*

30
40
50
30
40
50
30
40
50
N-Telopeptides ofBone Collagen
Bone-SpecificAlkaline Phosphatase
Osteocalcin
Change in bone markers after 24 months
Tibolone and its effects on bone
-50
-40
-30
-20
-10
0
10
20
placebo 0.3 mg
0.625 mg
1.25 mg
2.5 mg
-50
-40
-30
-20
-10
0
10
20
placebo 0.3 mg
0.625 mg
1.25 mg
2.5 mg
-50
-40
-30
-20
-10
0
10
20
placebo 0.3 mg
0.625 mg
1.25 mg
2.5 mg
TibolonePlacebo n = 770
Adapted from Gallagher et al., J Clin Endocrin Metab 2001

Efficacia del Tibolone
2
4
6
8
10
Per
cent
age
chan
ge in
BM
D
** ****
**** **
** ** ****
Tibolone (n=59)
Controlli (n=51)
Collo Femorale (+3.7 %)
Colona Lombare(+4.8 %)
* *
**
** **** ** **
-10
-8
-6
-4
-2
0
0 1 2 3 4 5 6 7 8 9 10
Per
cent
age
chan
ge in
BM
D
Years
*p<0.01 vs control**p<0.0001 vs control
**
Colonna Lombare(-8.5 %)
Collo Femorale(-8.9 %)
Rymer et al., Climacteric 2002,
* *
** **
** **** **

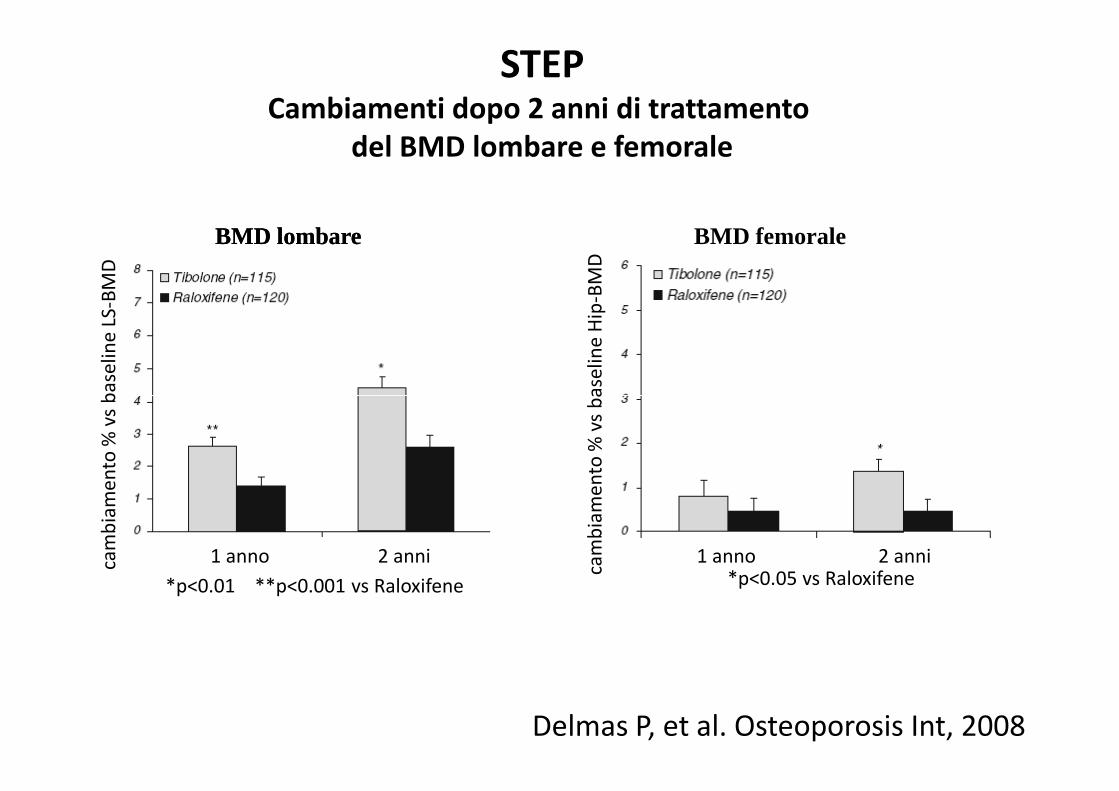
Effects of tibolone and raloxifene on bone mineral
density in osteopenic postmenopausal women [Study of Tibolone’s Effects on osteoPenia (STEP)]
Confronto tra
tibolone 1,25 mg e raloxifene 60 mg tibolone 1,25 mg e raloxifene 60 mg
in un trattamentodi 2 anni:
effetti su BMD e markers del turnover osseo
Delmas P, et al. Osteoporosis Int, 2008
cam
bia
me
nto
% v
s b
ase
lin
e L
S-B
MD
cam
bia
me
nto
% v
s b
ase
lin
e H
ip-B
MD
STEPCambiamenti dopo 2 anni di trattamento
del BMD lombare e femorale
BMD lombareBMD lombare BMD femorale
*p<0.01 **p<0.001 vs Raloxifene
1 anno 2 annicam
bia
me
nto
% v
s b
ase
lin
e L
S
cam
bia
me
nto
% v
s b
ase
lin
e H
ip*p<0.05 vs Raloxifene
1 anno 2 anni
Delmas P, et al. Osteoporosis Int, 2008

STEPCambiamenti dopo 2 anni di trattamento
dei markers del metabolismo osseo
Delmas P, et al. Osteoporosis Int, 2008

Long-Term Intervention on Fractures with Tibolone (LIFT)


Effetti di tibolone 1,25 mg su BMD(Studio LIFT)
Cummings et al, NEJM, 2008

Effetti di tibolone 1,25 mg su fratture non vertebrali(Studio LIFT)
Cummings et al, NEJM, 2008

Principali risultati di tibolone 1,25 mg vs PBO(Studio LIFT)
Cummings et al, NEJM, 2008

Effetti di tibolone 1,25 mg su fratture vertebrali enon vertebrali(Studio LIFT)
Cummings et al, NEJM, 2008
L’entità delle riduzione del rischio di FXs Vertebrali è simile a quella dimostrata con Estrogeni, Bisfosfonati e Raloxifene

Effetti di tibolone 1,25 mg sul Rischio di Cancro Mammario Invasivo
(Studio LIFT)
Cummings et al, NEJM, 2008

Effetti di tibolone 1,25 mg sul Rischio di Stroke
(Studio LIFT)
Cummings et al, NEJM, 2008

Studio THEBESIncidenza di eventi avversi cardiovascolari (tutti i soggetti
trattati) (range età: 45-65 aa; media 54.4 )
Archer et al, JCEM 2007

E. Løkkegaard,EHJ 2008
Hormone therapy and risk of myocardial infarction: a national register study
The age-stratified risk of myocardial infarction with various Hormone Therapy regimens from multivariable model.

VCAM-1
120
60
80
100
**
*
Effect of tibolone and anti-hormones on vessel wall
Tissue-Selective effects
Tibolone acts as an estrogen on vessel wall
VCAM-1 expression (% vs LPS)
LPS
0
20
40
60
Tib Tib+ICI
3α 3β 3β +ICI
∆4 ∆4 +ICI
3α +ICI
C* denote significantdifference vs.LPS-treated cells
Simoncini et al., MCE 2000; 162: 87-94

Aumento dello Stroke considerazioni
• Fattori di rischio più frequenti e di maggiore entità con l’aumentare dell’età (ipertensione, dislipidemia, aterosclerosi)
• Conclusioni: come per la HRT è opportuno non utilizzare tibolone nelle donne anziane o quelle con fattori di rischio per stroke (ipertensione, fumo, diabete non in buon compenso metabolico, fibrillazione atriale)

Meccanismo potenziale per l’effetto deltibolone sul tessuto mammario
• No attività antagonista per ER
• No inibizione dell’aromatasi
• Omeostasi cellulare
(aumento dell’apoptosi & diminuzione della (aumento dell’apoptosi & diminuzione della
proliferazione)
• Inibizione della Solfatasi

E2/NETA Tibolone Placebo
Basale
Sicurezza del Tibolone :Mammella:MammellaStudio sulla densità mammografica Studio sulla densità mammografica
Sei mesi di trattmento
Lundström et al., Am J Obstet Gynecol 2002

Sicurezza del Tibolone: MammellaEffetto del tibolone sulla proliferazione delle cellule epiteliali Effetto del tibolone sulla proliferazione delle cellule epiteliali
normali umane mammarienormali umane mammarie
% aumento
200
250
Adapted from Gompel et al., Fertil Steril 1998
1 2 3 4 5 6 7
Giorni
0
50
100
150

Sicurezzarezza del del TiboloneTibolone::MammellaMammellaProliferazioneProliferazione delledelle ghiandoleghiandole mammariemammarie didi cynomolguscynomolgus monkeys
Proliferazione Lobuloalveolare
20
25
Gruppi di confronto
Cline et al, Menopause 2002; 9:242
0
5
10
15
Controlli Tib a bassodosaggio
Tib adAltodosaggio
CEE CEE+MPA
Ki67
Labeling
(%)

ProliferazioneProliferazione delledelle cellule cellule mammariemammarieCambiamentiCambiamenti del Ki67 del Ki67 mediomedio dopodopo 12 12 mesimesi
didi trattamentotrattamento con HRT e con HRT e TiboloneTibolone
8.0
10.0
12.0%
of cells
Valdivia I, Campodónico I, et al. IMS June 2002.
6.0 10.7 6.4 4.2
0.0
2.0
4.0
6.0
Basal 12 month
CEE + MPABasal 12 month
Tibolone
% o
f cells

Conclusions… tibolone and its 3betaOH metabolite have an anti-invasive
effect on the tested breast cancer cell lines in vitro.This effect on invasion is not correlated with an effect on
cell-cell adhesion or motility but coincides with a decreased release of pro-MMP-9 in the medium

Tabella 1. Incidenza di cancro mammario in seguito a
somministrazione di tibolone o di placebo (dati da studi di III
e IV fase con tibolone)
Placebo Tibolone
(tutti i dosaggi)
Tolerability and Safety of TiboloneTolerability and Safety of TiboloneHRT and cancer: the current status of research and Practice 2002HRT and cancer: the current status of research and Practice 2002
Helmond & KloosterboerHelmond & Kloosterboer
(tutti i dosaggi)
Soggetti (numero) 1.194 3.343
Donne - anno 1269 3150
Cancri mammari (numero) 4 5
Incidenza di ca mammario /
1000 donne - anno
3.15 1.59
Rischio relativo (Intervallo di
Confidenza 95 %)
0.50 (0.11-2.54)

MILLION WOMEN STUDYObjective: to investigate the relation between various patterns of use of HRTand breast cancer incidence and mortality.
Partecipants: 1 084 110 UK women aged 50–64 years were recruited
Results: relative risk for breast cancer following tibolone therapy wasincreased (1.45 [1·25–1·68], p<0·0001), similar to that of ET (1.3[1·21–1·40], p<0·0001) but significantly less than that for CCHT (2.0[1·88–2·12], p<0·0001).
Lancet, 2003

Objective:To determine the effect of different types and formulations of HRT on the risk ofbreast cancer in postmenopausal women.Design:Population-based case–control studySetting:UK, 1998-2004Partecipants:Women 50–75 yearsfrom GPRD (General Practice Research Database);6347 incident cases of breast cancer that were matched with 31 516 controls.
HORMONE REPLACEMENT THERAPY USE AND VARIATIONSIN THE RISK OF BREAST CANCERL. Opatrny, et al 2008
Results: The rate of breast cancer was not increased among exclusive users ofunopposed estrogens (RR 0.97; 95% CI 0.86–1.09) or of tibolone(RR 0.86; 95% CI0.65–1.13). Users of tibolone who had switched from opposed estrogens, however, hadan elevated rate (RR 1.29; 95% CI 1.09–1.52).
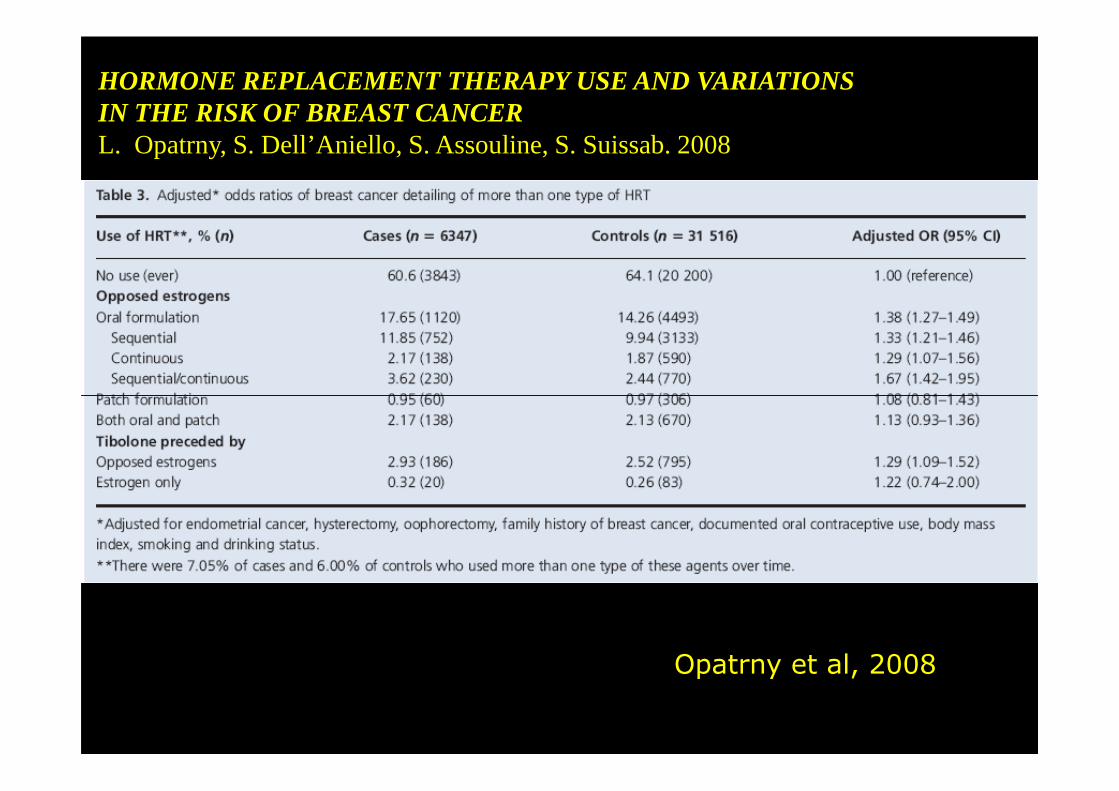
HORMONE REPLACEMENT THERAPY USE AND VARIATIONSIN THE RISK OF BREAST CANCERL. Opatrny, S. Dell’Aniello, S. Assouline, S. Suissab. 2008
Opatrny et al, 2008

Menopausa/Osteopenia/OsteoporosiTiming del trattamento
Menopausa/Osteopenia/OsteoporosiTiming del trattamento
Premenopausa Postmenopausa iniziale Postmenopausa (sintomatica) avanzata
Ca+Vit.D; E/P ERT/HRT Bisfosfonati Esercizio fisico Tibolone PTH –S. Ranelato
SERMs (o dopo 5 aa di HRT)
Mod. da:Del Puente, Migliaccio, Esposito, Lello, Ott. Aging, 2004Gandolini, Migliaccio, Lello, Bevilacqua, Malavolta. Aging, 2004