modified iaea template - الفيزياء الطبية · 137cs 30.0 years 0.662 5.5 192ir 74.2...
TRANSCRIPT

Interstitial
Interstitial implant for breast
radiotherapy
Seven 192-Ir wires
Brachytherapy The use of radioactive sources in close
proximity to the target area for radiotherapy

Intracavitary
Intracavitary
gynecological implant
Three 137-Cs sources

Brachytherapy overview
Brachytherapy uses encapsulated
radioactive sources to deliver a high
dose to tissues near the source
brachys (Greek) = short (distance)
Inverse square law determines most of
the dose distribution

Brachytherapy
Characterized by strong
dose gradients
Many different techniques
and sources available
Implants are highly
customized for individual
patients

Brachytherapy
Use of radioactive materials in direct contact
with patients - more radiation safety issues
than in external beam radiotherapy
Less than 10% of radiotherapy patients are
treated with brachytherpay
Per patient treated the number of accidents in
brachytherapy is considerably higher than in
EBT

Contents
Brachytherapy Sources and equipment
Brachytherapy techniques

Objectives
To understand the concept of „sealed‟ source
To know the most common isotopes used for brachytherapy
To be familiar with general rules for source handling and testing
To be aware of differences between permanent implants, low (LDR) and high dose rate (HDR) applications
To understand the basic fundamentals of brachytherapy equipment design.
Brachytherapy Sources and Equipment

1. Sealed sources
IAEA BSS glossary: “Radioactive material that is a) permanently sealed in a capsule or b) closely bound and in a solid form.”
In other words: the activity is fixed to its carrier and contamination of the environment is not possible as long as the source is intact
Have an activity which can be derived from a calibration certificate and the half life of the isotope (nothing is lost)
MUST be checked for integrity regularly - a good means of doing this is by wipe tests

Sealed and unsealed sources in
radiotherapy
Both are used to treat cancer
Sealed sources are used for EBT and Brachytherapy - the Brachytherapy sources are discussed here
Unsealed sources may be used for systemic treatments – (Nuclear Medicine) as: 131-I for thyroid treatment
89-Sr and 153-Sm for treatment of bone metastasis.

2. The ideal source in Brachytherapy What do you think one would expect from and ideal
Brachytherapy source?
Clinical usefulness determined by
Half life = the time after which half of the
original activity is still present in the source
Specific activity = activity per gram of material.
The higher the smaller a source of a
particular activity can be made
Radiation energy determines the range of
radiation in tissue (AND the requirements for
shielding)

The Ideal Brachytherapy source
Pure gamma emitter - betas or alphas are too
short in range and result in very high doses to
small volumes around the source
Medium gamma energy
high enough to treat the target with homogenous
dose
low enough to avoid normal tissues and reduce
shielding requirements
High specific activity
suitable also for high dose rate applications
small

The Ideal Brachytherapy source
Stable daughter product
For temporaryمؤقت implants: long half life
allows economical re-use of sources
For permanent implants: medium half life

3. Real brachytherapy Sources
A variety of source types and isotopes are
currently in use
They differ for different applications because
of
half life,
size (specific activity) and
radiation energy
When deciding on a source one must also
keep the shielding requirements in mind.

Brachytherapy Sources Radionuclide Half-life Photon Energy (MeV) Half-value Layer (mm lead)
226Ra 1600 years 0.047 - 2.45 (0.83 ave) 8.0
222Rn 3.83 days 0.047 - 2.45 (0.83 ave) 8.0
60Co 5.26 years 1.17, 1.33 11.0
137Cs 30.0 years 0.662 5.5
192Ir 74.2 days 0.136 - 1.06 (0.38 ave) 2.5
198Au 2.7 days 0.412 2.5
125I 60.2 days 0.028 ave 0.025
103Pd 17.0 days 0.021 ave 0.008

Brachytherapy sources
The first isotope used clinically was radium
around 1903
However, radium and radon have only
historical importance - they should not be used
in a modern radiotherapy department

Brachytherapy sources
Because:
wide energy spectrum leading to high dose
close to the source and still high dose
around the patient - shielding difficult
Radon, the daughter product of radium, is a
noble gas which is very difficult to contain -
contamination risk
The long half life means disposal is very
difficult

Popular sources: 137-Cs
“Cesium 137”
Main substitute for radium
Mostly used in gynecological
applications
Long half life of 30 years ---> decay
correction necessary every 6 months
Sources are expensive and must be
replaced every 10 to 15 years

Popular sources: 192-Ir
“Iridium 192”
Many different forms available
Most important source for HDR applications
Medium half life (75 days) - decay correction
necessary for each treatment
Needs to be replaced every 3 to 4 months to
maintain effective activity and therefore an
acceptable treatment time

Popular sources: 192-Ir
“Iridium 192”
High specific activity - therefore even high
activity sources can be miniaturized essential
for HDR applications
A bit easier to shield than 137-Cs - because
the gamma energies of 192-Ir range from 136
to 1062keV (effective energy around 350keV)


Popular sources: 125-I
Very low energy - therefore shielding is
easy and radiation from an implant is
easily absorbed in the patient:
permanent implants are possible
Mostly used in the
form of seeds

125-I seeds
Many different designs

125-I seeds
Design aims and
features:
sealed source
non-toxic tissue
compatible encapsulation
isotropic dose distribution
radio-opaque for
localization
Mentor

X-ray visibility of 125-I seeds

Other isotopes used for seeds
Gold 198
Half Life = 2.7 days -
short enough to let
activity decay in the
patient
Energy = 412 keV
TVL lead = around
8mm
Palladium 103
Half Life = 17 days -
dose rate about 2.5
times larger than for
125-I
Energy = 22 keV
TVL lead = 0.05mm

Brachytherapy Sources A variety of source shapes and forms:
pellets = balls of approximately 3 mm diameter
seeds = small cylinders about 1 mm diameter and 4 mm
length
needles = between 15 and 45 mm active length
tubes = about 14 mm length, used for gynaecological
implants
hairpins = shaped as „hairpins‟, approximately 60 mm active
length
wire = any length, usually customised in the hospital -
inactive ends may be added
HDR sources = high activity miniature cylinder sources
approximately 1mm diameter, 10mm length

Source form examples
Seeds (discussed before): small containers for activity
usually 125-I, 103-Pd or 198-Au for permanent
implant such as prostate cancer
Needles and hairpins: for „life‟ implants in the operating theatre - activity
is directly introduced in the target region of the
patient
usually 192-Ir for temporary implants eg. of the
tongue
Scale in mm

Source form: 192-Ir wire
Used for LDR interstitial implants
Cut to appropriate length prior to implant to
suit individual patient
Cutting using manual technique or cutter...

Source form 192-Ir wires
192-Ir wire: activity between 0.5 and
10mCi per cm
used for interstitial
implants
low to medium dose rate
can be cut from 50 cm
long coils to the desired
length for a particular
patient Wire cutter
Movement
controls
Length
measurement Shielding

Source form example
192-Ir wire: activity between 0.5 and
10mCi per cm
used for interstitial
implants
low to medium dose rate
can be cut from 50 cm
long coils to the desired
length for a particular
patient Wire cutter
Movement
controls
Length
measurement Shielding

Question:
Why would people use 198-Au for brachytherapy?

Some clues for an answer
Key features of 198-Au are:
small sources (seed)
short half life (2.7 days)
inert material
photon energy 412keV
Therefore, ideal for permanent implant

Brachytherapy
Brachytherapy installations cover
direct source loading
137-Cs sources for gynaecological applications
(radium should not be used)
permanent seed implants (gold or 125-I)
surface applicators (moulds, 125-I, strontium
and ruthenium plaques
manual afterloading (137-Cs, 192-Ir)
automatic afterloading (LDR, PDR and
HDR)

Brachytherapy
Highly customized treatment techniques
- each patient is treated differently
Techniques depend on
Disease site and stage
Operator/clinician
Technology/equipment available
Many of the points covered for External Beam
installations also apply to Brachytherapy
installations, particularly for automatic
afterloading systems

Preparation of sources for
brachytherapy
Choosing the correct sources is an important
part of the implant optimization
This is applicable for situations when:
there are several different sources available (eg
137-Cs source with slightly different length and
activity for gynecological implants)
sources are ordered and customized for an
individual patient (eg. 192-Ir wire)

Require a pre-implant plan...

Choosing the correct sources
Prepare a plan for a
particular implant
following the prescription
Select appropriate
sources
If existing sources are to
be used select sources
from the safe and place in
transport container
Document what is done
safe
source
shielding

Interstitial implants
For LDR usually use
192-Ir wire
(compare part VI)
Optimization is
possible as the
length of the wire
can be adjusted for
a particular implant

HDR sources
No preparation necessary
Ensure
source calibration
optimized plan

Implant techniques
Permanent implants patient discharged with implant in place
Temporary implants implant removed before patient is discharged
Here particular emphasis on radiation
protection issues in medical exposures

Permanent Implants: Radiation
protection issues
Implant of activity in theatre:
Radiation protection of staff from a variety
of professional backgrounds - radiation
safety training is essential
RSO or physicist should be present
Source transport always necessary
Potential of lost sources

Problems with handling activity in
the operating theatre
The time to place the sources in the best possible locations is
typically limited
Work behind shields
or with other
protective equipment
may prolong
procedure and result
in sub-optimal access
to the patient

Working behind shields

Permanent Implants: Radiation
protection issues
Patients are discharged with radioactive
sources in place:
lost sources
exposure of others
issues with accidents to the patient, other
medical procedures, death, autopsies and
cremation - compare part XV of the course

Temporary implants
Mostly done in afterloading technique
Radiation safety issues for staff:
Source handling and preparation
Exposure of nursing staff in manual
afterloading
Radiation safety issues for patients:
Source placement and removal

Afterloading
Manual The sources are placed
manually usually by a
physicist
The sources are
removed only at the end
of treatment
Remote The sources are driven
from an intermediate
safe into the implant
using a machine
(“afterloader”)
The sources are
withdrawn every time
someone enters the
room

Afterloading advantages
No rush to place the sources in theatre -
more time to optimize the implant
Treatment is verified and planned prior
to delivery
Significant advantage in terms of
radiation safety (in particular if a remote
afterloader is used)

Use of lead shield reduces scatter to the patient

High Dose Rate Brachytherapy
Most modern
brachytherapy is
delivered using HDR
Reasons?
Outpatient procedure
Optimization
possible

HDR brachytherapy
In the past possible using 60-Co pellets
Today, virtually all HDR brachytherapy
is delivered using a 192-Ir stepping
source Source moves step by step
through the applicator - the
dwell times in different locations
determine the dose distribution

HDR unit
interface

4. Brachytherapy equipment
Design considerations
often similar to external
beam therapy
Nucletron

Remote Afterloading Equipment
The most complex
pieces of equipment
in brachyhterapy
Low dose rate units
High dose rate units
Many important
design consideration
in IEC standard

Low dose rate brachytherapy
Selectron for gynecological
brachytherapy
137-Cs pellets pushed into the
applicators using compressed
air
Location of active and inactive
pellets can be chosen by the
operator to optimize the source
loading for an individual patient
Shown are 6 channels - the red
lights indicate the location of an
active source
Nucletron

Other features
No computer required
Two independent timers
Optical indication of
source locations
Permanent record
through printout
Key to avoid
unauthorized use

HDR brachytherapy units
Must be located in a
bunker
Have multiple
channels to allow
the same source to
drive into many
catheters/needles
MDS Nordion

Nucletron HDR unit control
Keypad
Display
Emergency off button
Key for source out
Memory card for transfer of the dwell positions
for the treatment of a particular patient - labeled
Key
Printout =
permanent record

Catheters are indexed to avoid
mixing them up
Transfer catheters are locked into
place during treatment - green light
indicates the catheters in use

Regular maintenance is required
Source drive must be
working within
specified accuracy
(typically 1-2mm)
Emergency buttons
must work
Manual retraction of
the source in case of
power failure must
work

Regular maintenance is required
Maintenance work
should follow
manufacturers
recommendations
All modifications
MUST be
documented
A physicists should
be notified to perform
appropriate tests
LDR and HDR units are not all...
Other brachytherapy equipment:
PDR (pulsed dose rate) units
Seed implant equipment
Endovascular brachytherapy

LDR and HDR units are not all...
Other brachytherapy equipment:
PDR units - similar to HDR
Seed implant equipment - discussed in
more detail in the second lecture of part VI
Endovascular brachytherapy

Typical Radiation Levels
Selectron LDR (Cs-137) Cervix insertion
10 pellets of 15 mCi/seed = 150 mCi
20 mR/h at 1m 0.2 mSv/h
5 days for 1 mSv (Background)
this is inside the room!
microSelectron HDR (Ir-192) turned ON!
10 Ci source = 10 000 mCi
4700 mR/h at 1m 47 mSv/h
1.3 minutes for 1 mSv (Background)
door interlock ensures that no-one is in room

Brachytherapy Techniques 1. Clinical brachytherapy applications
2. Implant techniques and applicators
3. Delivery modes and equipment

Brachytherapy
Very flexible radiotherapy delivery
Source position determines treatment success
Depends on operator skill and experience
In principle the ultimate „conformal‟
radiotherapy
Highly individualized for each patient
Typically an inpatient procedure as opposed to
external beam radiotherapy which is usually
administered in an outpatient setting

Clinical brachytherapy
History
Brachytherapy has been one of the
earliest forms of radiotherapy
After discovery of radium by M Curie,
radium was used for brachytherapy
already late 19th century
There is a wide range of applications -
this versatility has been one of the most
important features of brachytherapy

Today
Many different techniques and a large
variety of equipment
Less than 10% of radiotherapy patients
receive brachytherapy
Use depends very much on training and
skill of clinicians and access to
operating theatre

A brachytherapy patient
Typically localized cancer
Often relatively small tumor
Often good performance status (must
tolerate the operation)
Sometimes pre-irradiated with external
beam radiotherapy (EBT)
Often treated with combination
brachytherapy and EBT

1. Clinical brachytherapy
applications
A. Surface moulds
B. Intracavitary (gynaecological, bronchus,..)
C. Interstitial (Breast, Tongue, Sarcomas, …)

A. Surface moulds
Treatment of superficial lesions with
radioactive sources in close contact
with the skin
A mould for the back
of a hand including
shielding designed to
protect the patient
during treatment
Hand
Catheters for
source transfer


Surface mould advantages
Fast dose fall off in tissues
Can conform the activity to any surface
Flaps available

B. Intracavitary implants
Introduction of radioactivity using an
applicator placed in a body cavity
Gynaecological implants
Bronchus
Oesophagus
Rectum

Gynaecological implants
Most common
brachytherapy application -
cervix cancer
Many different applicators
Either as monotherapy or
in addition to external
beam brachytherapy as a
boost

Gynecological applicators
Different design - all Nucletron

Vaginal applicators
Single source line
Different diameters
and length
Nucletron
Gammamed - on the right with shielding

Bronchus implants
Often palliative to
open air ways
Usually HDR
brachytherapy
Most often single
catheter, however
also dual catheter
possible

Dual catheter bronchus implant
Catheter placement via
bronchoscope
Bifurcation may create
complex dosimetry

C. Interstitial implants
Implant of needles or flexible catheters
directly in the target area
Breast
Head and Neck
Sarcomas
Requires surgery - often major
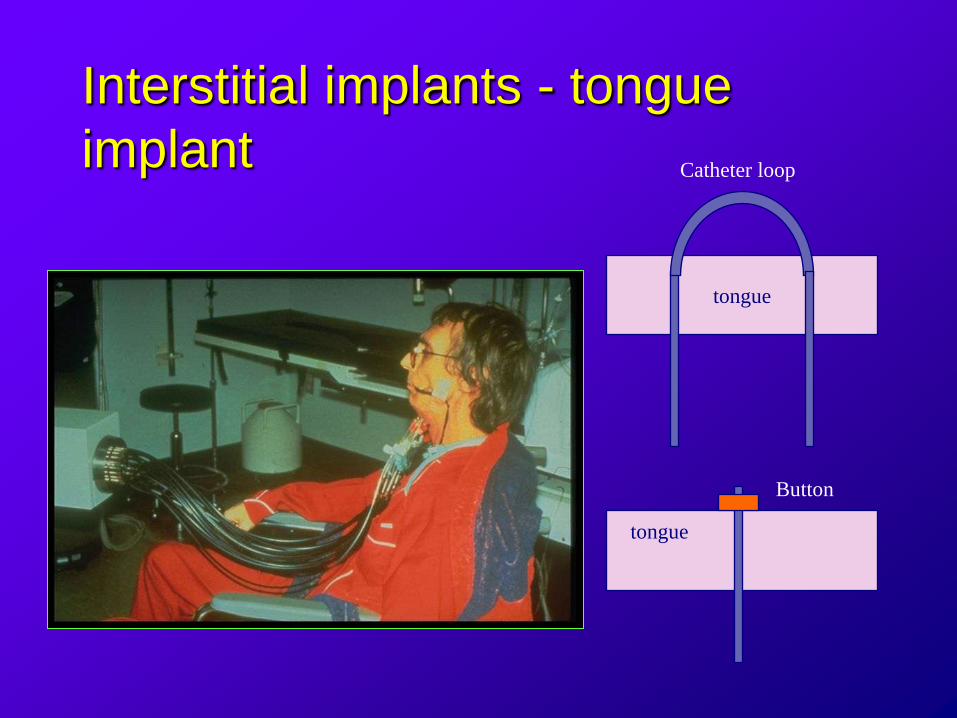
Interstitial implants - tongue
implant
tongue
tongue
Catheter loop
Button

Breast implants
Typically a boost
Often utilizes templates to improve
source positioning
Catheters or needles

2. Implant techniques and
applicators
Permanent implants
patient discharged with implant in place
Temporary implants
implant removed before patient is
discharged from hospital

Source requirement for
permanent implants
Low energy gammas or betas to
minimize radiation levels outside of the
patient (125-I is a good isotope)
May be short-lived to reduce dose with
time (198-Au is a good isotope)
More details on most common 125-I
prostate implants in section 4A of the
lecture

Temporary implants
Implant of activity in theatre
Manual afterloading
Remote afterloading

3. Delivery modes and
equipment
Low Dose Rate (LDR)
Medium Dose Rate
High Dose Rate (HDR)
Pulsed Dose Rate (PDR)

Delivery modes - different
classifications are in use
Low Dose Rate
Medium Dose Rate
High Dose Rate
Pulsed Dose Rate
< 1Gy/hour
around 0.5Gy/hour
> 1Gy/hour
not often used
>10Gy/hour
pulses of around
1Gy/hour

Low dose rate brachytherapy
The only type of brachytherapy possible
with manual afterloading
Most clinical experience available for
LDR brachytherapy
Performed with remote afterloaders
using 137-Cs or 192-Ir

Low dose rate brachytherapy
Selectron for
gynecological
brachytherapy
137-Cs pellets pushed
into the applicators
using compressed air
6 channels for up to two
parallel treatments
Nucletron

Simple design
No computer required
Two independent timers
Optical indication of
source locations
Permanent record
through printout
Key to avoid
unauthorized use

Treatment process
Implant of applicator (typically in the
operating theatre)
Verification of applicator positioning
using diagnostic X-rays (eg
radiotherapy simulator)

Treatment planning
Most commercial treatment planning
systems have a module suitable for
brachytherapy planning:
Choosing best source configuration
Calculate dose distribution
Determine time required to give desired
dose at prescription points
Record dose to critical structures

Treatment planning of different
brachytherapy implants

High Dose Rate Brachytherapy
Most modern
brachytherapy is
delivered using HDR
Reasons?
Outpatient procedure
Optimization
possible

HDR brachytherapy
In the past possible using 60-Co pellets
Today, virtually all HDR brachytherapy
is delivered using a 192-Ir stepping
source Source moves step by step
through the applicator - the
dwell times in different locations
determine the dose distribution

HDR 192-Ir source
From presentation by Pia et al
Source length 5mm, diameter 0.6mm
Activity: around 10Ci

Optimization of dose distribution
adjusting the dwell times of the
source in an applicator
Nucletron

HDR brachytherapy procedure
Implant of applicators, catheters or needles in
theatre
For prostate implants as shown here use transrectal
ultrasound guidance

HDR brachytherapy procedure
Localization using diagnostic X-rays
HDR prostate
implant:
Simulator image
Scout image for
CT scan

Treatment planning
Definition of the desired
dose distribution
(usually using many
points)
Computer optimization
of the dwell positions
and times for the
treatment

Treatment
Transfer of date to
treatment unit
Connecting patient
Treat... Gammamed
Nucletron

HDR unit
interface

HDR brachytherapy
Usually fractionated (eg. 6 fractions of
6Gy)
Either patient has new implant each
time or stays in hospital for bi-daily
treatments
Time between treatments should be
>6hours to allow normal tissue to repair
all damage

HDR units:
different designs
available

Catheters are indexed to avoid
mixing them up
Transfer catheters are locked into
place during treatment - green light
indicates the catheters in use

HDR systems
Can be moved eg
between different
facilities or into
theatre for intra-
operative work

Pulsed dose rate
Unit has a similar design as HDR, however the
activity is smaller (around 1Ci instead of 10Ci)
Stepping source operation - same optimization
possible as in HDR
Treatment over same time as LDR treatment to
mimic favorable radiobiology
In-patient treatment: hospitalization required
Source steps out for about 10 minutes per hour and
then retracts. Repeats this every hour to deliver
minifractions (‟pulses‟) of about 1Gy

Feras Mansour Jargon
فراس منصور جرغون
IAEA Training Course: Radiation Protection in Radiotherapy slide 109