nej mp 1209051
TRANSCRIPT

8/10/2019 Nej Mp 1209051
http://slidepdf.com/reader/full/nej-mp-1209051 1/3
Perspective
The NEW ENGLAND JOURNAL of MEDICINE
august 30, 2012
n engl j med 367;9 nejm.org august 30, 2012 785
in 50 years. Why has this theoreti-cally vaccine-preventable diseasebeen on the upswing?
The past 45 years have seenconcern about the safety of thediphtheria–tetanus–pertussis (DTP) vaccine, epidemics stemming fromthe vaccine’s decreased use, andthe development of new vaccines
using acellular pertussis compo-nents (DTaP). In the prevaccineera, the number of reported casesof pertussis reached epidemic pro-portions every 2 to 5 years.1,2 Per-tussis immunization in the UnitedStates reduced the average inci-dence from 157 per 100,000 pop-ulation in the early 1940s to less
than 1 per 100,000 in 1973. Never-theless, the cycles of outbreakscontinued to occur, because nei-ther infection nor immunizationproduces lifelong immunity topertussis, as they do for diseasessuch as measles; as measles wasbeing brought under control, theperiod between epidemics length-
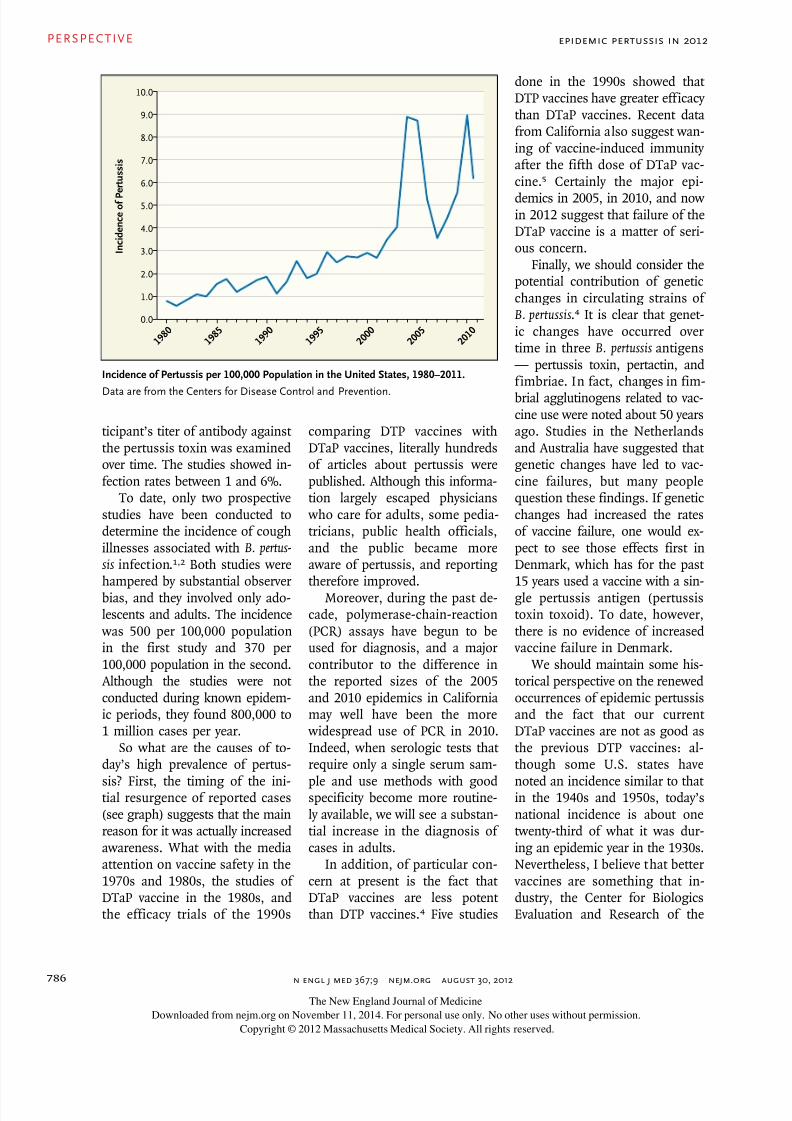
ened, and there was less clinicaldisease and less circulation of the virus. Since cycles of pertussiscontinue to occur today, we knowthat Bordetella pertussis is continu-ing to circulate in a manner sim-ilar to that of the prevaccine era.Around 1982, the incidence ofpertussis started to gradually in-
crease; in 2005 and 2010, sub-stantial epidemics occurred, andanother epidemic is now under way (see graph).1-5
There are actually two relevantepidemiologies to consider: theepidemiology of reported pertus-sis cases and the epidemiology ofB. pertussis infection.2 The formerdepends on the surveillance pro-gram we have in place: the morecomplete it is, the higher the re-ported incidence will be. As forthe latter, over the past 25 years,three types of studies have been
performed to gain insight intoB. pertussis infection.1,2 The firsttype examined the cause of pro-longed illnesses involving coughin adolescents and adults; thefindings suggested that 13 to 20%of these cough illnesses were at-tributable to B. pertussis infection.In the second type of study, a par-
Epidemic Pertussis in 2012 — The Resurgenceof a Vaccine-Preventable Disease James D. Cherry, M.D.
According to the Centers for Disease Controland Prevention, the United States is currently
experiencing what may turn out to be the largestoutbreak of reported pertussis (whooping cough)
The New England Journal of Medicine
Downloaded from nejm.org on November 11, 2014. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.
8/10/2019 Nej Mp 1209051
http://slidepdf.com/reader/full/nej-mp-1209051 2/3
PERSPECTIVE
n engl j med 367;9 nejm.org august 30, 2012786
ticipant’s titer of antibody againstthe pertussis toxin was examinedover time. The studies showed in-fection rates between 1 and 6%.
To date, only two prospectivestudies have been conducted todetermine the incidence of coughillnesses associated with B. pertus-
sis infection.1,2 Both studies werehampered by substantial observerbias, and they involved only ado-lescents and adults. The incidence was 500 per 100,000 populationin the first study and 370 per100,000 population in the second.Although the studies were notconducted during known epidem-ic periods, they found 800,000 to1 million cases per year.
So what are the causes of to-day’s high prevalence of pertus-
sis? First, the timing of the ini-tial resurgence of reported cases(see graph) suggests that the mainreason for it was actually increasedawareness. What with the mediaattention on vaccine safety in the1970s and 1980s, the studies ofDTaP vaccine in the 1980s, andthe efficacy trials of the 1990s
comparing DTP vaccines withDTaP vaccines, literally hundredsof articles about pertussis werepublished. Although this informa-tion largely escaped physicians who care for adults, some pedia-tricians, public health officials,and the public became moreaware of pertussis, and reportingtherefore improved.
Moreover, during the past de-cade, polymerase-chain-reaction(PCR) assays have begun to beused for diagnosis, and a majorcontributor to the difference inthe reported sizes of the 2005and 2010 epidemics in Californiamay well have been the more widespread use of PCR in 2010.Indeed, when serologic tests thatrequire only a single serum sam-
ple and use methods with goodspecificity become more routine-ly available, we will see a substan-tial increase in the diagnosis ofcases in adults.
In addition, of particular con-cern at present is the fact thatDTaP vaccines are less potentthan DTP vaccines.4 Five studies
done in the 1990s showed thatDTP vaccines have greater efficacythan DTaP vaccines. Recent datafrom California also suggest wan-ing of vaccine-induced immunityafter the fifth dose of DTaP vac-cine.5 Certainly the major epi-
demics in 2005, in 2010, and nowin 2012 suggest that failure of theDTaP vaccine is a matter of seri-ous concern.
Finally, we should consider thepotential contribution of geneticchanges in circulating strains ofB. pertussis .4 It is clear that genet-ic changes have occurred overtime in three B. pertussis antigens— pertussis toxin, pertactin, andfimbriae. In fact, changes in fim-
brial agglutinogens related to vac-cine use were noted about 50 yearsago. Studies in the Netherlandsand Australia have suggested thatgenetic changes have led to vac-cine failures, but many peoplequestion these findings. If geneticchanges had increased the ratesof vaccine failure, one would ex-pect to see those effects first inDenmark, which has for the past15 years used a vaccine with a sin-gle pertussis antigen (pertussistoxin toxoid). To date, however,there is no evidence of increased vaccine failure in Denmark.
We should maintain some his-torical perspective on the renewedoccurrences of epidemic pertussisand the fact that our currentDTaP vaccines are not as good asthe previous DTP vaccines: al-though some U.S. states have
noted an incidence similar to thatin the 1940s and 1950s, today’snational incidence is about onetwenty-third of what it was dur-ing an epidemic year in the 1930s.Nevertheless, I believe that better vaccines are something that in-dustry, the Center for BiologicsEvaluation and Research of the
Epidemic Pertussis in 2012
I n c i d e n c e
o f P
e r t u s s i s
10.0
4.0
5.0
1.0
6.0
2.0
3.0
0.0
7.0
8.0
9.0
1 9 8 0
1 9 8 5
1 9 9 0
1 9 9 5
2 0 0 0
2 0 0 5
2 0 1 0
Incidence of Pertussis per 100,000 Population in the United States, 1980–2011.
Data are from the Centers for Disease Control and Prevention.
The New England Journal of Medicine
Downloaded from nejm.org on November 11, 2014. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.

8/10/2019 Nej Mp 1209051
http://slidepdf.com/reader/full/nej-mp-1209051 3/3
n engl j med 367;9 nejm.org august 30, 2012
PERSPECTIVE
787
Food and Drug Administration,and pertussis experts should be-gin working on immediately.
In the interim, we need to usethe vaccines we have (DTaP andTdap [tetanus–diphtheria–acellu-lar pertussis]) in the best ways
possible. Of particular concernare the frightening rates of com-plications and death associated with pertussis in unimmunized young infants. The “cocooning”strategy — vaccinating people who have contact with infants —has been implemented but is oftenimpeded by logistics. Immuniz-ing pregnant women is funda-mentally sound because it reducesthe risk that the mother will ac-
quire pertussis around the timeof delivery, and it gives the infantsome protection for perhaps 1 to2 months. But women who havemultiple pregnancies within a few years present a problem, sinceimmunization with a vaccine con-
taining tetanus toxoid (i.e., Tdap)could result in increased local re-actions.
Another approach would be tostart DTaP immunization at a younger age, with shorter intervalsbetween doses. This schedulecould be started at birth, and thefirst three doses could be com-pleted by 3 months of age. Nota-bly, during the period of greatestreduction in pertussis incidence
in the United States (1954–1974),the three-dose primary series wascompleted between 3 and 5 monthsof age.
In 2012, it is time to recog-nize the successes of the past andto implement new studies and di-
rection for the control of pertus-sis in the future.
Disclosure forms provided by the authorare available with the full text of this arti-cle at NEJM.org.
From the Department of Pediatrics, DavidGeffen School of Medicine, University ofCalifornia at Los Angeles, Los Angeles.
This article was published on August 15,2012, at NEJM.org.
1. Mattoo S, Cherry JD. Molecular patho-
genesis, epidemiology, and clinical manifes-tations of respiratory infections due to Bor-detella pertussis and other Bordetellasubspecies. Clin Microbiol Rev 2005;18:326-82.2. Cherry JD. The present and future controlof pertussis. Clin Infect Dis 2010;51:663-7.3. Pertussis epidemic — Washington, 2012.MMWR Morb Mortal Wkly Rep 2012;61:517-22.4. Cherry JD. Why do pertussis vaccines fail?Pediatrics 2012;129:968-70.5. Winter K, Harriman K, Zipprich J, et al.California pertussis epidemic, 2010. J Pediatr2012 July 20 (Epub ahead of print).
DOI: 10.1056/NEJMp1209051Copyright © 2012 Massachusetts Medical Society.
Epidemic Pertussis in 2012
Getting the Methods Right — The Foundation of Patient-CenteredOutcomes ResearchSherine E. Gabriel, M.D., and Sharon-Lise T. Normand, Ph.D.
Health care in the UnitedStates has changed dramati-
cally over the past several decades.
Today, patients have more optionsthan ever. Making the right choic-es, whether for prevention, diag-nosis, or treatment, requires acritical appraisal of the potentialbenefits and harms of the op-tions, within the context of thepatient’s characteristics, condi-tions, and preferences.
Many of these choices are avail-able thanks to advances in medi-cal research. Yet most patients
and many clinicians find researchsomewhat mysterious. They havedifficulty sorting through themountains of medical evidenceto identify information that is re-liable and actionable for theirunique circumstances. Patient-centered outcomes research andcomparative-effectiveness research
promise to enhance decision mak-ers’ ability to fully understandand weigh alternatives. But just
as health care interventions anddelivery strategies have advancedmarkedly in recent decades, sohave research methods (see table).Without systematic guidance forthe appropriate and efficient useof these methods, their rapidgrowth and complexity will onlyadd to the confusion.
Although some U.S. states have noted an incidence
similar to that in the 1940s and 1950s,
today’s national incidence is about one twenty-third
of what it was during an epidemic year in the 1930s.
Nevertheless, better vaccines are something
that industry, the FDA, and pertussis experts
should begin working on immediately.
The New England Journal of Medicine
Downloaded from nejm.org on November 11, 2014. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.