parkinson’s disease dr. m. sofi md; frcp (london); frcpedin; frcsedin
TRANSCRIPT

PARKINSON’S DISEASE
Dr. M. Sofi MD; FRCP (London); FRCPEdin;
FRCSEdin

James Parkinson Born 11 April 1755
Shoreditch, London, England
Died 21 December 1824 (aged 69)Langthorne, North Yorkshire, England
Cause of death Stroke Nationality British Ethnicity White British Occupation Surgeon Known for First description
of Parkinson's disease
Spouse(s) Mary Dale

James ParkinsonFour generations of family were surgeon-apothecaries in LondonHe was initially medical apprentice with his fatherBecame medical student at London Hospital (1776)Awarded diploma of the company of surgeons (1784)Founding member Medico-Chirurgical Society (1812)Founding member of Huntarian Society (1819)Gold Medalist of Royal College of Surgeons (1822)

Classification of Parkinson Syndromes in a
Community Idiopathic PD ~ 85% of all PS cases Neuroleptic-induced parkinsonism (DIP)
7% - 9% MSA (SDS, SND, OPCD) ~ 2.5% PSP ~ 1.5% Vascular parkinson syndrome ~ 3% PS due to MPTP, CO, Mn, recurrent head
trauma is extremely rare No new cases of postencephalitic
parkinsonism since l960s

Descriptive Epidemiology of Parkinson Syndrome
• Incidence– 5-24/ 105 worldwide (USA: 20.5/105)– Incidence of PS/PD rising slowly with aging
population• Prevalence– 57-371/105 worldwide (USA/Canada 300/105)– 35%-42% of cases undiagnosed at any time
• Onset–mean PS 61.6 years; PD 62.4 years– rare before age 30; 4-10% cases before age
40
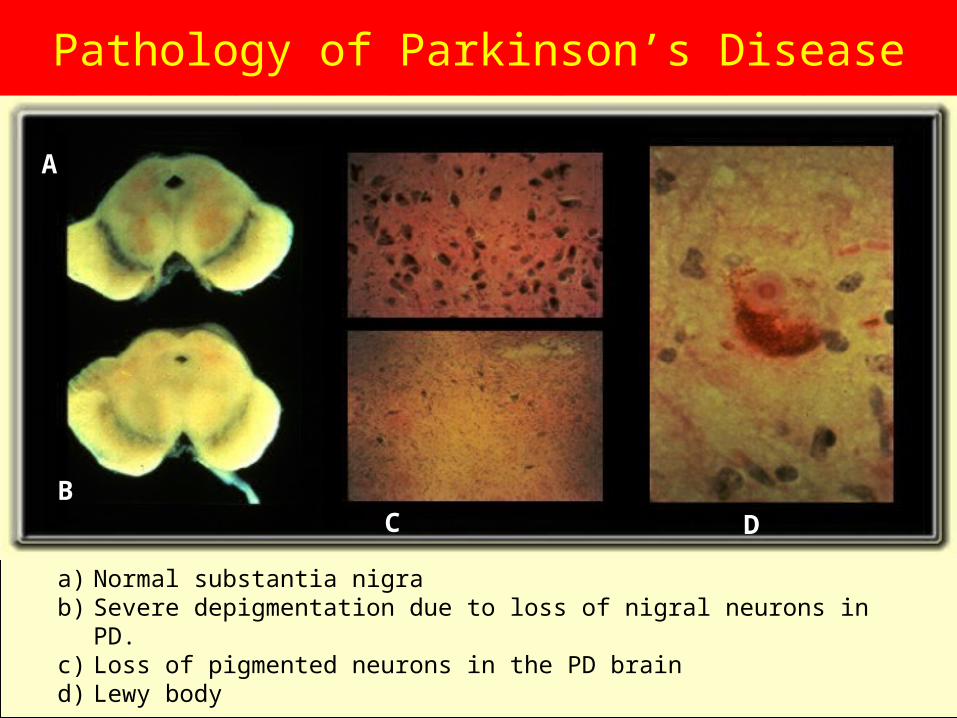
Pathology of Parkinson’s Disease
a) Normal substantia nigrab) Severe depigmentation due to loss of nigral neurons in PD.c) Loss of pigmented neurons in the PD braind) Lewy body
A
BC D

Main Biochemical Abnormality
• Marked striatal DA depletion–“Striatal dopamine deficiency syndrome”
• At death, DA loss > 90%• <50% DA loss is asymptomatic• ~70% DA loss for symptom
manifestations• Severity of DA loss best correlates
with bradykinesia in PD

Normal Basal Ganglia Functional Anatomy
C ortex
P refrontalInsular
C ingulateS ensoryMotor
S uppl. MotorP remotor
P remotorP refrontal
S triatum
D 2 D 1Thalamus
VA /VL
+ = exc itatory
- = inhib itory
B rainstemS C
S N c
S N r
G P i
S TN
G Pe
-
+
+
+-
-
---
-
+
++
+
+
+
N ormal

Functional Anatomy of Parkinson’s Disease
C ortex
P refrontalInsular
C ingulateS ensoryMotor
S uppl. MotorP remotor
P remotorP refrontal
S triatum
D 2 D 1Thalamus
VA /VL
+ = exc itatory
- = inhibitory
B rainstemS C
S N c
S N r
G P i
S TN
G Pe
-
-
++
++++
-
---
--
+
++
+
+
+ - -
Parkinson’s D isease

Parkinson’s Disease Risk Factors
• Definite: Old age• Highly likely: MZ co-twin with early-
onset PD• Probable: Positive family history• Possible: Herbicides, pesticides,
heavy metals, proximity to industry, rural residence, well water, repeated head trauma, etc.
• Possible protective effect: Smoking

Cause of PD• Unknown in most
cases; not accelerated aging
• Genes– AD inheritance
very rare; mutation unknown
–mutation of Alpha synuclein gene (chromosome 4q) identified in one large Italian (Contursi) and 5 Greek autosomal dominant families
–mutation of parkin gene in autosomal-recessive juvenile parkinsonism
• Environment–Majority of cases
believed caused by environmental factor (s) but none identified so far
• Genes plus environment?

Environmental Toxin Model: MPTP
• Reproduces all the major motor features of PD
MAO-BMPTP MPP+
(In astrocytes)• Dopaminergic neuron mitochondria• Inhibits NADH--CoQ1 (Complex I) of
mitochondrial respiratory chain• ATP production falls• Cell death

Schematic representation of the mechanisms involved in toxicity of 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP). BBB, blood—brain barrier;MPDP+, 1-methyl-4-phenyl-2,3-dihydropyridinium; MPTP 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine; MPP+, its four-electron oxidation product 1-methyl-4-phenylpyridinium; MAO, monoamine oxidase.
Early Signs and Symptoms
• Cardinal Characteristics–Resting tremor–Bradykinesia–Rigidity–Postural instability
• Other–Micrographia–Masked face–Slowing of ADLs–Stooped, shuffling gait–Decreased arm swing when walking

• Difficulty arising from a chair• Difficulty turning in bed• Hypophonic speech• Sialorrhea• Loss of the sense of smell• Foot dystonia
Additional Signs and Symptoms

• At least two of three: resting tremor, bradykinesia, rigidity• Absence of a secondary cause—drugs, metabolic, etc.• Definitive diagnosis can only be made by autopsy
Criteria for Diagnosis
• Early onset of, or rapidly progressing, dementia
• Rapidly progressive course• Supranuclear gaze palsy• Upper motor neuron signs• Cerebellar signs—dysmetria,
ataxia• Urinary incontinence• Early symptomatic postural
hypotension
Clues Suggesting Atypical Parkinsonism

• Progressive supranuclear palsy–Supranuclear downgaze palsy,
square wave jerks–Upright posture/frequent falls–Pseudobulbar emotionality–Furrowed brow/stare
• Corticobasal degeneration–Unilateral, coarse tremor–Limb apraxia/limb dystonia/alien
limb
Neurodegenerative disorders with Parkinsonism (I)

Neurodegenerative disorders with
Parkinsonism (II)• Multiple system atrophy–Shy-Drager syndrome•Autonomic insufficiency—orthostasis, impotence
–Striatonigral degeneration•Tremor less prominent
–Olivopontocerebellar atrophy•Cerebellar signs
Neurodegenerative Disorders with Parkinsonism
(III)• Diffuse Lewy body disease–Early onset of dementia–Delusions and hallucinations–Agitation
• Alzheimer’s disease–Dementia is the primary clinical syndrome–Rest tremor is rare

Differential Diagnosis of PD:
• Drug-induced• Toxin-induced• Metabolic• Structural lesions (vascular
parkinsonism, etc.)• Normal pressure
Hydrocephalus• Infections
Secondary Parkinsonism

Toxin-induced Parkinsonism
•MPTP•Carbon monoxide•Manganese•Cyanide

Vascular Parkinsonism• Abrupt onset, usually unilateral• Step-wise or no progression• Other signs—hemiparesis, aphasia, hyperreflexia• Infarcts on neuroimaging helpful in confirming diagnosis

Hydrocephalus-induced Parkinsonism (NPH)
• Can be communicating or obstructive• Normal pressure hydrocephalus
—idiopathic• Clinical triad:–parkinsonism/gait disorder–urinary/fecal incontinence–dementia

Treatment Options• Preventive treatment–No definitive treatment available
• Symptomatic treatment–Pharmacological–Surgical
• Non-motor management• Restorative—experimental only–Transplantation–Neurotrophic factors
Drug Classes in PD• Dopaminergic agents–Levodopa–Dopamine agonists
• COMT inhibitors •MAO-B inhibitors• Anticholinergics• Amantadine

DA GABA
ACh
Striatum
Substantia Nigra
levodopaAmantadine*
selegiline Dopamine agonists bromocriptine pergolide pramipexole ropinirole
baclofen
trihexiphenidyl
BBB carbidopa benserazide tolcapone entacapone
Sites of Action of PD Drugs

Anticholinergics• Dopaminergic depletion cholinergic
overactivity• Initially used in the 1950s• Effective mainly for tremor and rigidity• Common agents (Start low, go slow):–Trihexyphenidyl: 2-15 mg/day–Benztropine: 1-8 mg/day
• Side effects:–Dry mouth, sedation, delirium,
confusion, hallucinations, constipation, urinary retention

Levodopa• Most effective drug for parkinsonian
symptoms• First developed in the late 1960s; rapidly
became the drug of choice for PD• Large neutral amino acid; requires active
transport across the gut-blood and blood-brain barriers
• Rapid peripheral decarboxylation to dopamine without a decarboxylase inhibitor (DCIs: carbidopa, benserazide)
• Side effects: nausea, postural hypotension, dyskinesias, motor fluctuations

Selegiline• Irreversible MAO-B inhibitor• Clinically active by inhibiting
dopamine metabolism in brain• May be neuroprotective• Dosage: 5 mg at breakfast and lunch• Side effects: insomnia, hallucinations,
nausea (rarely), OH• Potential interactions with tricyclic and
SSRI antidepressants

Levodopa/Carbidopa Formulations
Onset Duration
Immediate Release10/100, 25/100, 25/250
20-40 min 2-4 hr
Controlled Release25/100, 50/200
30-60 min 3-6 hr
“Liquid levodopa” (dissolved tablets)
10-20 min 0.5-1 hr

DAs: Common Adverse Effects
• Nausea, vomiting• Dizziness, postural hypotension• Headache• Dizziness• Drowsiness & somnolence• Dyskinesias• Confusion, hallucinations, paranoia• Erythromelalgia; pulmonary &
retroperitoneal fibrosis; pleural effusion & pleural thickening; Raynaud’s phenomena. May be more common with ergotoline DAs

Levodopa-Induced Dyskinesias• Manifestation of excessive dopaminergic
stimulation• Typically late effect, and with higher doses• Narrowing of therapeutic window• Rare in LD-naive patients on DA monotherapy • Most common is “peak dose” dyskinesia–disappears with dose reduction
• Choreiform, ballistic and dystonic movements• Most patients prefer some dyskinesias over
the alternative of akinesia and rigidity

COMT Inhibitors• Newest class of antiparkinsonian drugs:
tolcapone, entacapone• MOA similar to dopa decarboxylase inhibitors• Potentiate LD: prevent peripheral
degradation by inhibiting catechol O-methyl transferase
• Reduces LD dose necessary for a given clinical effect
• Helpful for both early and fluctuating Parkinson’s disease
• May be particularly useful for patients with “brittle” PD, who fluctuate between off and on states frequently throughout the day

Entacapone• Dosage: 200 mg w/each levodopa
dose• Parkinson’s Study Group 1997:
Increased on time by 5%, more in pts w/least on time• Rinne et al., 1998: Increased on
time by ~10%; decreased levodopa• Diarrhea, dopaminergic SEs

Dopamine Receptor Subtypes
• D1, D2 subcortical• D3, D4, D5 cortical• Differentiated biochemically & pharmacologically into two families:–D1 family: D1, D5–D2 family: D2, D3, D4
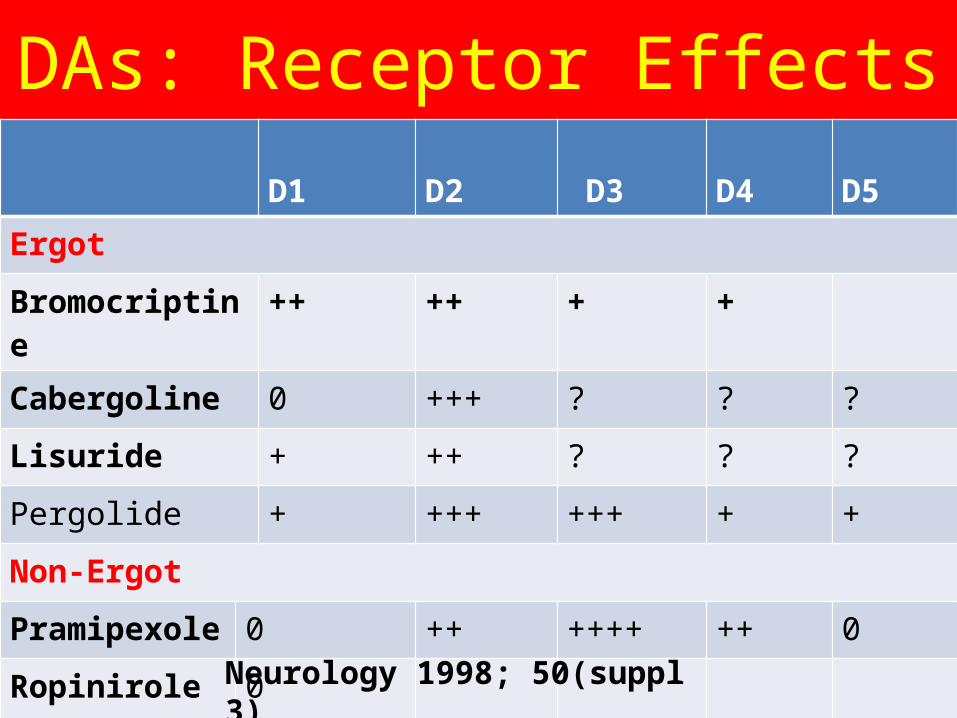
DAs: Receptor Effects D1
D2 D3
D4 D5
Ergot
Bromocriptine
++ ++ + +
Cabergoline 0 +++ ? ? ?
Lisuride + ++ ? ? ?
Pergolide + +++ +++ + +
Non-Ergot
Pramipexole
0 ++ ++++ ++ 0
Ropinirole 0Neurology 1998; 50(suppl 3)

Off-period Dystonia• Appears when LD level is low,
especially early AM• w/ or w/o parkinsonism• Dose adjustments, add-ons:–more frequent LD dosing to avoid low plasma levels–add DA, COMT inhibitor, MAO-B inhibitor

Apomorphine• D1/D2 agonist• Parenteral delivery (s/c., i/v., sublingual,
intranasal, rectal)• Rapid “off” period rescue– 2-5 mg s.c.; pen injection systems
• Treatment of unpredictable, frequent motor fluctuations– continuous s/c. infusion via mini-pump
• SE: nausea, vomiting, hypotension– trimethobenzamide 250 mg TDS.– domperidone 20 mg TDS; not available in
U.S.

Managing Early Complications:
Altered Mental States• Confusion, sedation, dizziness, hallucinations, delusions
• Reduce or eliminate CNS-active drugs of lesser priority–anticholinergics – sedatives–amantadine – muscle
relaxants–hypnotics – urinary
spasmodics • Reduce dosage of DA, COMT inhibitor,
or LD

Initial Therapy: What is the Chief Complaint?
Predominant Symptom Clinical Options
No functional impairment Delay therapy
Mild symptoms Amantadine, selegiline
Discrete symptoms Tremor—anticholinergic
Depression—antidepressantAnxiety—anxiolytic
Functionally disabling Levodopa, dopamine symptoms agonist, COMT inhibitor

Managing Early Complications: Wearing Off/Mild Dyskinesia
• For pts on DA monotherapy:–elevate dosage of agonist–add LD, w/ or w/o COMT inhibitor
• For pts on LD:–add DA, COMT inhibitor, or MAO inhibitor–reduce LD dosage–use combination of immediate and CR

Late Complications• Motor– response fluctuations, dyskinesias,
dystonia, freezing, falls• Behavioral/neuropsychological–depression, sleep disorders,
psychosis• Autonomic–orthostatic hypotension;
hyperhidrosis, constipation, impotence, urinary incontinence or retention

Peak Dose Dyskinesia or Dystonia
• Chorea more common than dystonia• May be worse on more affected side• May not be as disabling as
akinesia/rigidity• Dose adjustments, add-ons:– reduce LD dose, increase dose
frequency–convert to LD-CR– reduce LD, add DA, COMT inhibitor,
or MAO-B inhibitor

Wearing Off• Regular and predictable decline in
response 2-4 hours after LD dose• Most common motor fluctuation• Dose adjustments, add-ons:–change to LD-CR, or increase LD frequency–reduce LD, add DA or COMT inhibitor

On-off Response• Sudden and unpredictable off periods unrelated to dosing schedule• One of the hardest features to manage• Dose adjustments, add-ons:–reduce LD, add DA

Other Motor Complications• Diphasic dyskinesia–dyskinesia at beginning and end of
dose–Dose adjustments, add-ons: add DA
• Drug failure– late afternoon, probably related to
poor gastric emptying or absorption– liquid preparations; increase gastric
motility; decrease dietary protein–apomorphine rescue

Freezing and Falls• Freezing–motoric block; at initiation of gait, turning, narrow spaces–use auditory, visual, proprioceptive cues
• Falls–physical therapy evaluation–cane, scooter, wheelchair may be necessary
Cognitive Assessment• Memory difficulties: 11-29% of PD patients– Benign forgetfulness– Delirium– Alzheimer’s disease– Other dementias
• Evaluation– Brain imaging– Lumbar puncture– EEG– Blood work for thyroid profile, vitamin
B12, serology, chemistry panel

Orthostatic Hypotension• Light-headedness, dizziness,
fatigue, shoulder or neck pain, blood pressure drops when standing
• Taper anti-hypertensive agents• Taper non-PD drugs• Increase salt intake• Compression stockings• Fludrocortisone (0.1-0.4 mg/d)• Midodrine (2.5 - 20 mg/d)

Surgical Treatments for Parkinson’s Disease
• Ablative–thalamotomy–pallidotomy
• Electrical stimulation–VIM thalamus, globus pallidus internus, sub-thalamic nucleus
• Transplant–autologous adrenal, human fetal, xenotransplants, genetically engineered transplants

Improvements with Pallidotomy
• Specific Features:–Dyskinesia 70-90 %–Wearing off dystonia 70-90 % –Tremor 25-60 %–Rigidity 25-50 %–Bradykinesia 25-50 %–Gait 25-50 %

Deep Brain Stimulation (DBS)
• High frequency, pulsatile, bipolar electrical stimulation
• Stereotactically placed into target nucleus
• Can be activated and deactivated with an external magnet
• Exact physiology unknown, but higher frequencies mimic cellular ablation, not stimulation

Cell Transplants• Autologous adrenal transplants–No efficacy
• Allogenic human fetal transplants–Initial encouraging clinical results
• Xenogenic fetal transplant (porcine and bovine) –Preliminary results pending
• Genetically engineered cells–Research ongoing

• Efficacy– Encouraging
preliminary results in young (<60) PD pts
– Patients greater than 50 years did not improve
– PET studies consistent with cell functioning
– Autopsies (2) show cell survival
• Problems– 4-10 embryos <
10 weeks gestation needed
– Immunosuppression requirements unknown
–Numerous technical problems
– Potential for dyskinesias, even without any PD medications
Human Fetal Transplants