principles of infectious diseases and antibiotics · 2011-05-06 · principles of infectious...
TRANSCRIPT
2011/3/25
11
指導幹部:湯珍珍藥師
指導藥師:盧志嘉、張佳鈴藥師
報告組員:陳琨勝、呂依真、曾詠新
Principles of Infectious Diseases
and Antibiotics
2011/3/25
22
Contents
Infectious Diseases
Classification of Antibiotics
Case Report
Case Discussion4
1
2
3
2011/3/25
33
Infectious Diseases
Introduction
Establishing the presence of infections
Identification of the pathogens
Selection of antimicrobial therapy
2011/3/25
4
2011/3/25
4
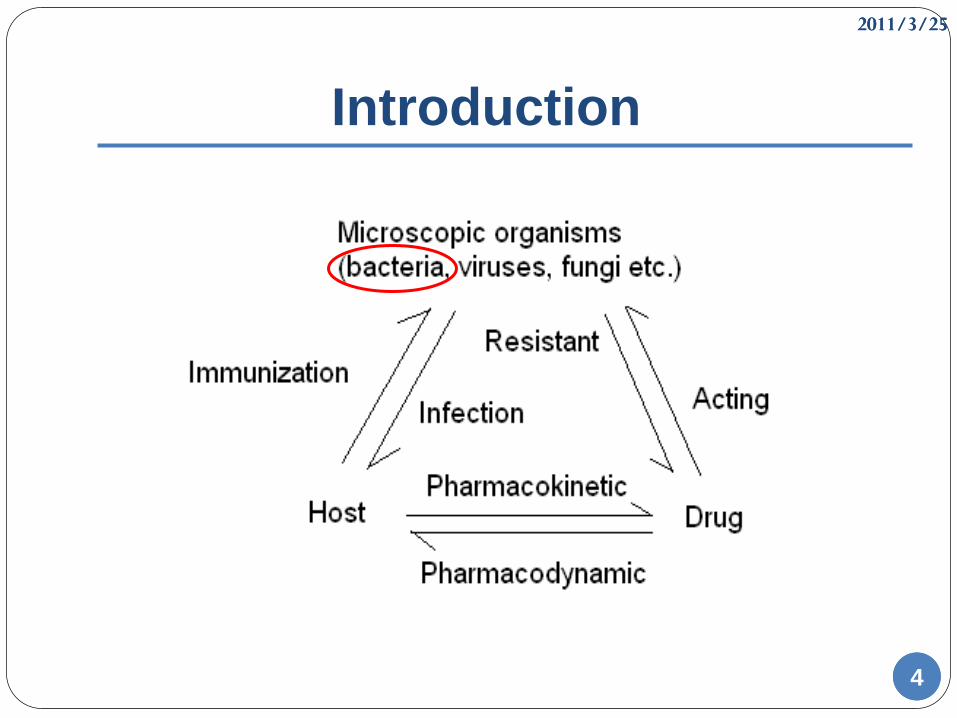
Introduction
2011/3/25
55
Establishing the presence of
infections(1)
Signs and symptoms
1. Fever:BT>37°C(axillary)
Infection induced (not always)
drug induced (Drug fever:phenytoin 、
amphotericin B)
other disease induced (autoimmune disease、
neoplasms)
2011/3/25
66
Establishing the presence of
infections(2)
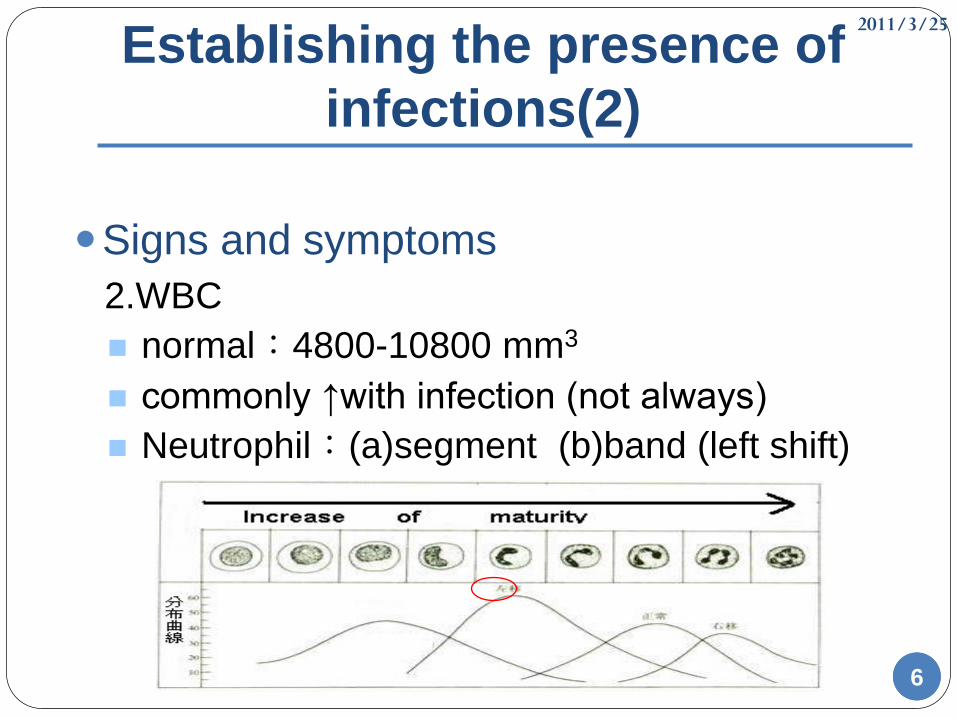
Signs and symptoms
2.WBC
normal:4800-10800 mm3
commonly ↑with infection (not always)
Neutrophil:(a)segment (b)band (left shift)
2011/3/25
77
Establishing the presence of
infections(3)
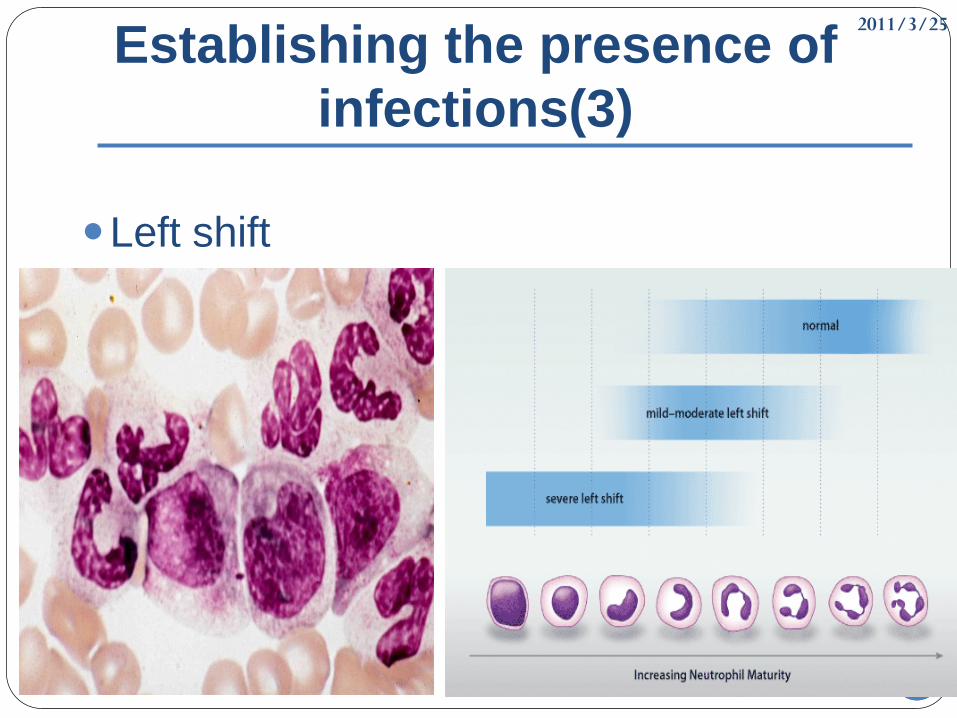
Left shift
2011/3/25
88
Establishing the presence of
infections(4)
Signs and symptoms
3.clinical symptoms
pulmonary:tachypenea、yellow-green
sputum、hypoxemia
gastrointestinal:abdominal pain、diarrh、
bowel sounds
urinary tract:dysuria、flank pain
superficial:erythema、abscess、swelling
2011/3/25
99
Establishing the presence of
infections(5)
Signs and symptoms
4.asymptom
immunodeficency: (a)drug related
(b)disease related
covert infection-virus
other infection
latent infection
opportunistic infection
2011/3/25
1010
Identification of the pathogens(1)
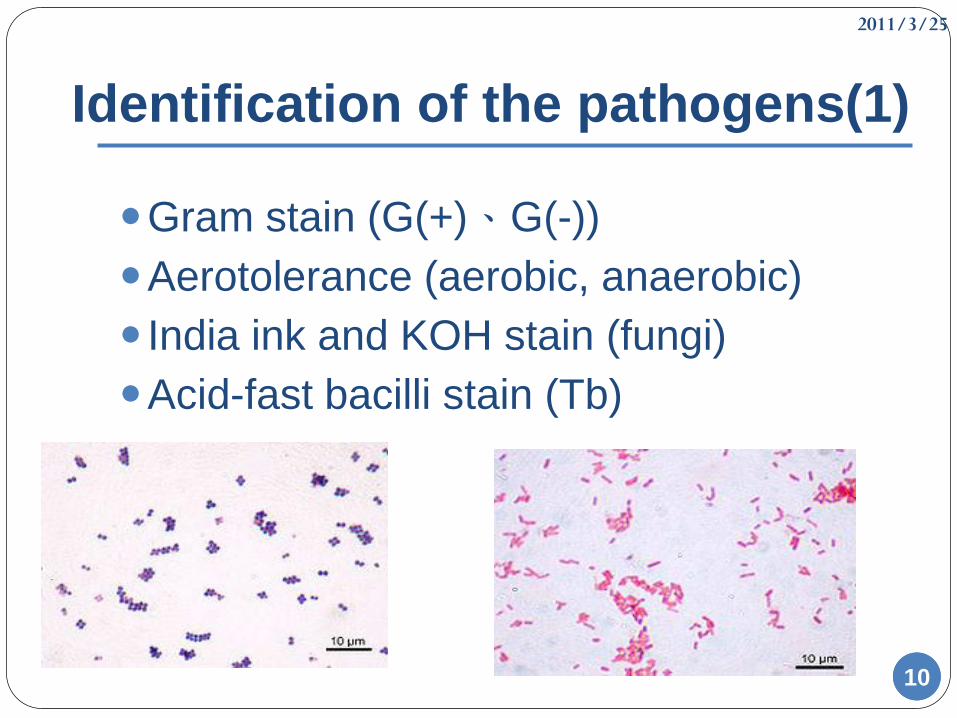
Gram stain (G(+)、G(-))
Aerotolerance (aerobic, anaerobic)
India ink and KOH stain (fungi)
Acid-fast bacilli stain (Tb)
2011/3/25
1111
Identification of the pathogens(2)
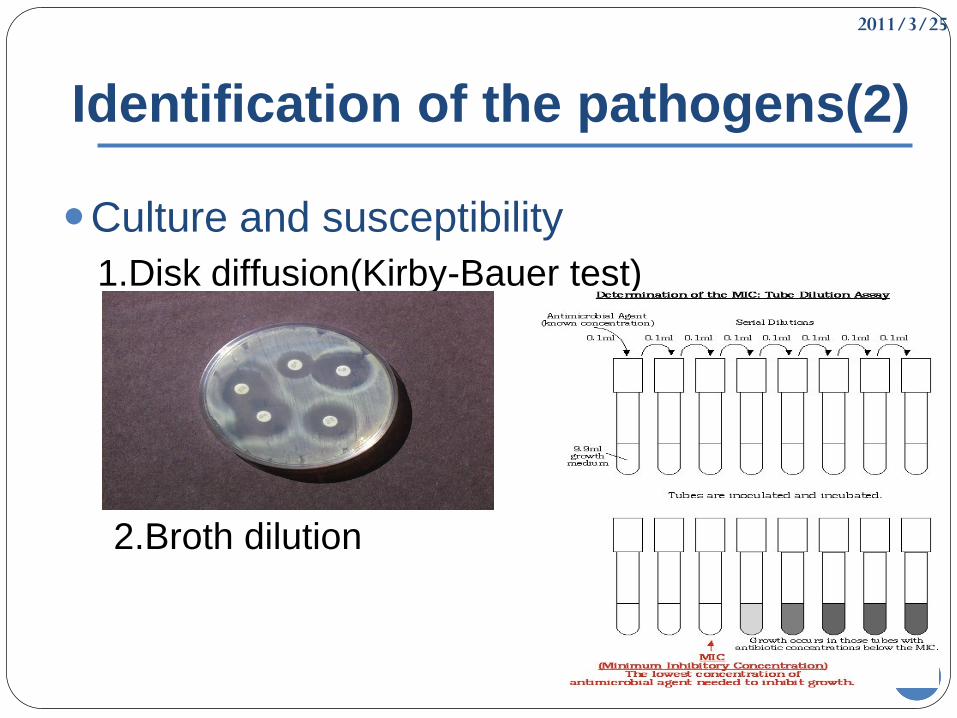
Culture and susceptibility
1.Disk diffusion(Kirby-Bauer test)
2.Broth dilution
2011/3/25
1212
Identification of the pathogens(3) Aerobic
Gram-positive Cocci
- Streptococci: pneumococcus, viridans streptococci; group A streptococci- Enterococcus
- Staphylococci: Staphylococcus aureus, Staphylococcus epidermidis
Rods (bacilli)
- Corynebacterium- Listeria
Gram-negative Cocci
- Moraxella- Neisseria (Neisseria meningitides. Neisseria gonorrhoeae)
Rods (bacilli)- Enterobacteriaceae (Escherichia coli, Klebsiella, Enterobacter, Citrobacter,
Proteus,Serratia, Salmonella, Shigella, Morganella, Providencia)- Campylobacter- Pseudomonas- Helicobacter- Haemophilus (coccobacilli morphology)- Legionella
2011/3/25
1313
Identification of the pathogens(4)
AnaerobicGram-positive Cocci
- Peptococcus- Peptostreptococcus
Rods (bacilli)- Clostridia (Clostridium perfringens, Clostridium tetani, Clostridium difficile)- Propionibacterium acnes
Gram-negative Cocci
- None Rods (bacilli)
- Bacteroides (Bacteroides fragilis, Bacteroides melaninogenicus)- Fusobacterium- Prevotella
2011/3/25
1414
Selection of antimicrobial therapy(1)
Empiric therapy
Host factors
Drug factors
Monitoring therapeutic response
Combination of antimicrobial therapy
Failure of antimicrobial therapy
2011/3/25
1515
Selection of antimicrobial therapy(2)
Empiric therapy1.before blood culture and sensitivity2.consideration: the site of infection localization antibiogram community or nosocomial host factors or drug factors
Broad spectrumNarrow spectrum
2011/3/25
1616
Selection of antimicrobial therapy(3)
Host factors1.the site of infection
(1) respiratory
(2) UTI
(3) skin and soft tissue
(4) intra-abdominal
(5) gastroenteritis
(6) endocarditis
(7) meningitis
2011/3/25
1717
Selection of antimicrobial therapy(4)
Host factors
2.age
(1) different pathogens
meningitis:
(a.) neonates(<1yr) (Escherichia coli, Listeria,
group B streptococci )
(b.) adults (Streptococcus pneumoniae, Neisseria
meningitides )
(2) drug toxicities:Tetracycline、FQs
2011/3/25
1818
Selection of antimicrobial therapy(5)
Host factors
3. Pregnancy
Avoid:Tetracycline、FQ、Chloramphenicol
4. Genetics
(a) allergy
(b) G6PD deficiency
(c) metabolism
2011/3/25
19
Selection of antimicrobial therapy(6)
Host factors
5. Organic dysfunction (Dose adjust):
Liver
dysfunction
Macrolides, Clindamycin, Chloramphenicol,
Linezolid
Renal
dysfunction
β-lactams, Tetracycline, FQs, AMGs,
TMP/SMX, Quinupristin/Dalfopristin
Liver: Cefoperazone, Ceftriaxone, Doxycyline,
Moxifloxacin
2011/3/25
2020
Selection of antimicrobial therapy(7)
Host factors
6. Concomitant disease
AIDS
DM
Neoplasm (chemotherapy)
2011/3/25
2121
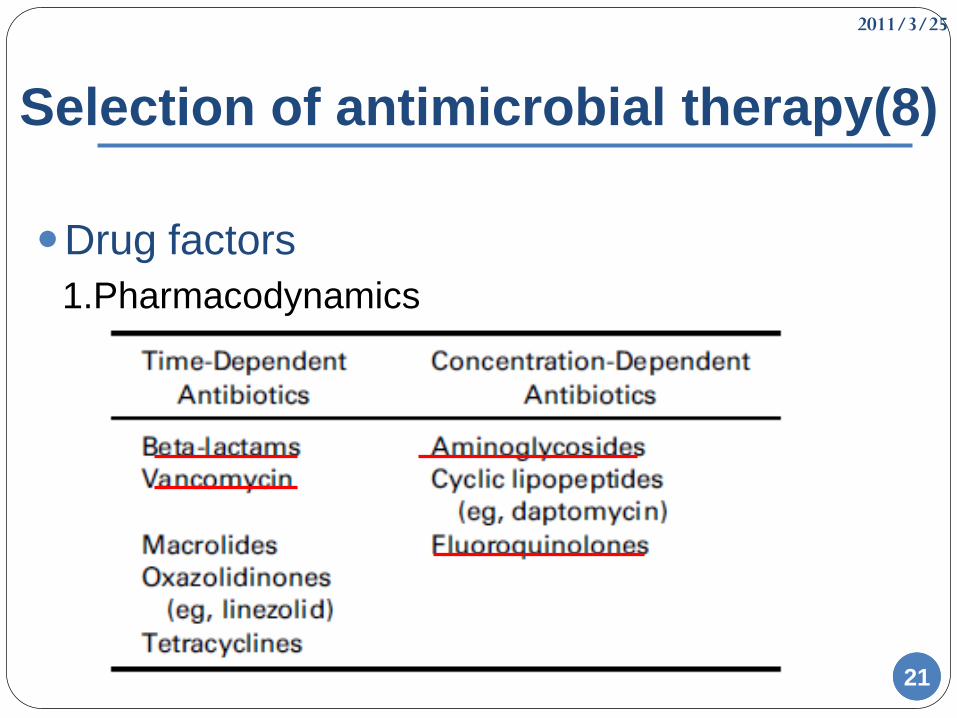
Selection of antimicrobial therapy(8)
Drug factors
1.Pharmacodynamics
2011/3/25
22
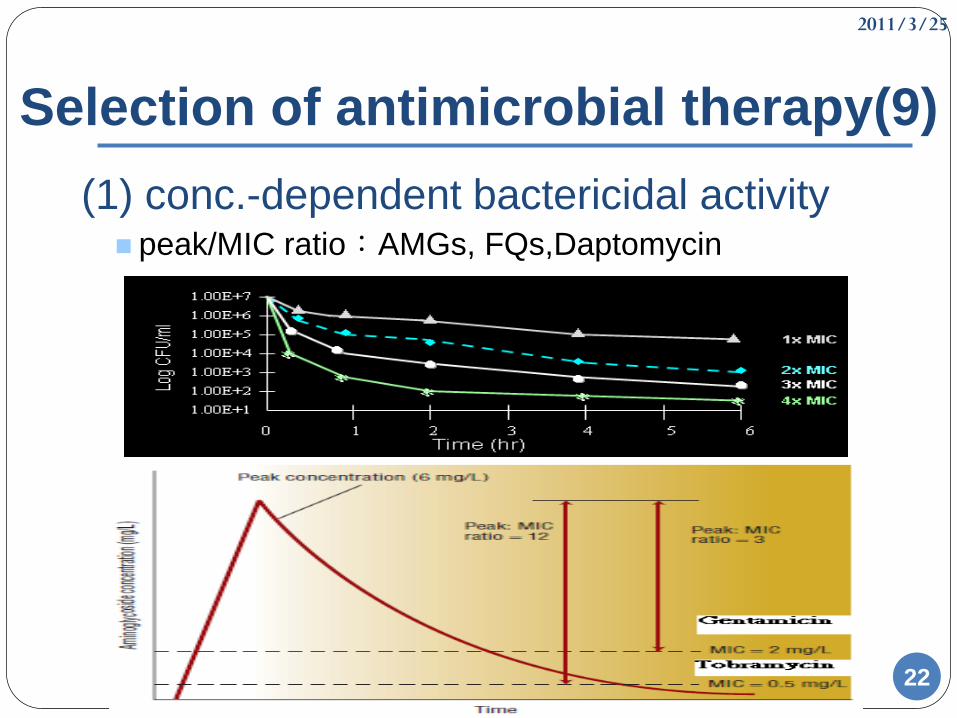
Selection of antimicrobial therapy(9)
(1) conc.-dependent bactericidal activity peak/MIC ratio:AMGs, FQs,Daptomycin
2011/3/25
23
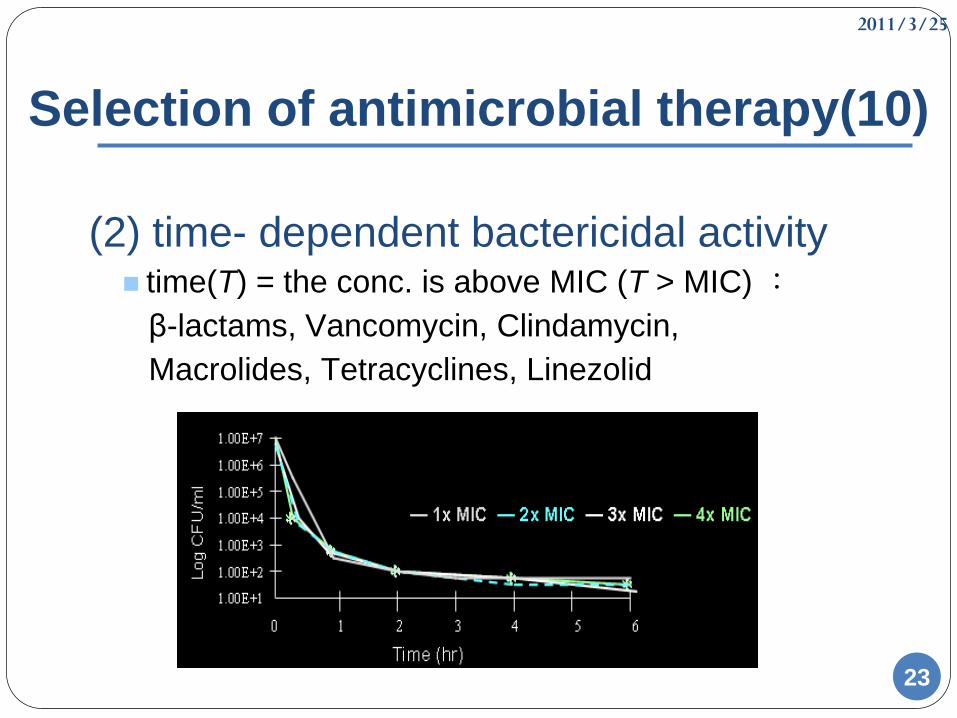
Selection of antimicrobial therapy(10)
(2) time- dependent bactericidal activity time(T) = the conc. is above MIC (T > MIC) :
β-lactams, Vancomycin, Clindamycin,
Macrolides, Tetracyclines, Linezolid
2011/3/25
2424
Selection of antimicrobial therapy(11)
Drug factors
2.Tissue penetration
The importance of tissue penetration varies with
site of infection.
Penetrate B.B.B:Ampicillin、Cefuroxime (2
generation)、Cephalosporins (3 generation)、
Chloramphenicol
2011/3/25
2525
Selection of antimicrobial therapy(12)
Drug factors3.Toxicity and side effectβ-lactams:Allergy (anaphylaxis), diarrheaAMGs:Nephrotoxicity, ototoxicityMacrolides:Nausea, vomiting, diarrheaTetracyclines:Teeth and bone deposition and
discoloration, photosensitivityFQs:Cartilage toxicity, CNS, QT prolong
4.Cost
2011/3/25
2626
Selection of antimicrobial therapy(13)
Monitoring therapeutic response1.CultureBroad spectrum Narrow spectrum
2.Clinical symptomsrelieve or not?
3.Serum concentrationaminoglycoside, chloramphecicol, vancomycin
4.Lab dataWBC count, seg./band, CRP, ESR
2011/3/25
2727
Selection of antimicrobial therapy(14)
Combination of antimicrobial therapy1.Broadening the Spectrum of Coverage
Empiric therapy
Mixed infections (DM,intraabdominal)
2.Decrease toxicity
Lower the dose
3.Synergism
1+1>2
4.Preventing Resistance
Especially for TB
2011/3/25
2828
Selection of antimicrobial therapy(15)
Failure of antimicrobial therapy
1.Drug factors
(1) Subtherapeutic dose
absorption
penetrate
protein binding
(2) Wrong drug
(3) Antagonism(1+1<2)
2011/3/25
2929
Selection of antimicrobial therapy(16)
Failure of antimicrobial therapy
2.Microbial factors (Resistance)
Overuse antibiotics
β-lactamases production
PBPs (penicillin-binding proteins) change
MRSA (Methicillin-resistant Staphylococcus Aureus)
VRE (Vancomycin-Resistant Enterococci)
2011/3/25
3030
Selection of antimicrobial therapy(17)
Failure of antimicrobial therapy
3.Host factors
immunosupressed patient
poor circulation
abscesses or necrotic tissue
2011/3/25
3131
Classification of Antibiotics
2011/3/25
3232
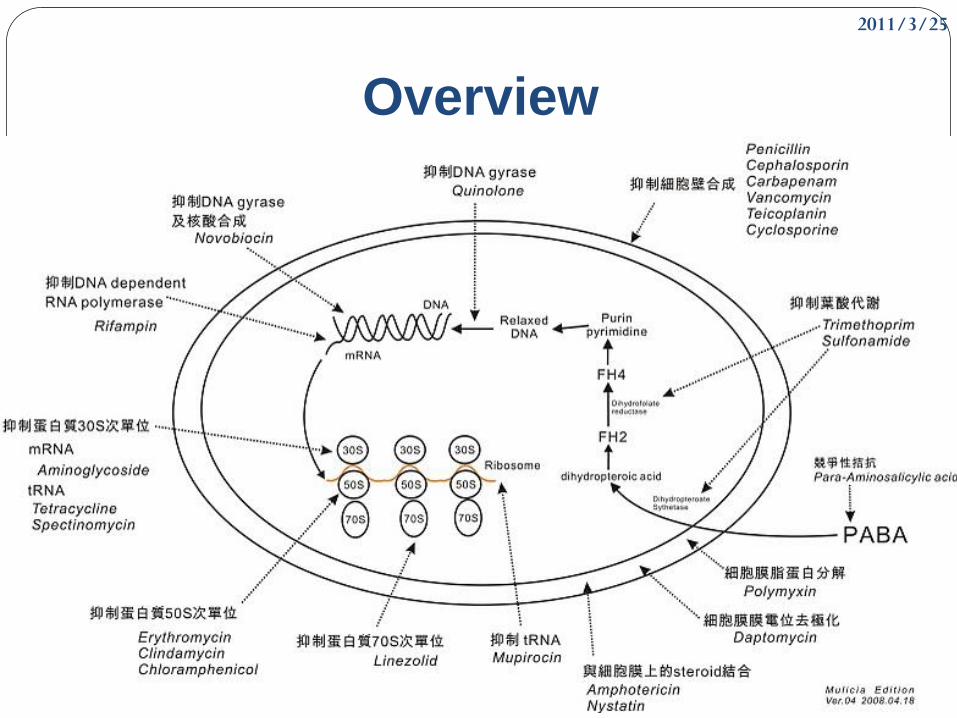
Classification
Bacterial cell wall synthesis inhibitors
Bacterial protein synthesis inhibitors
Antimetabolites
Fluoroquinolones
Antimycobacterial agents
Miscellaneous antimicrobial agent and
antiseptics
2011/3/25
3333
Overview
2011/3/25
3434
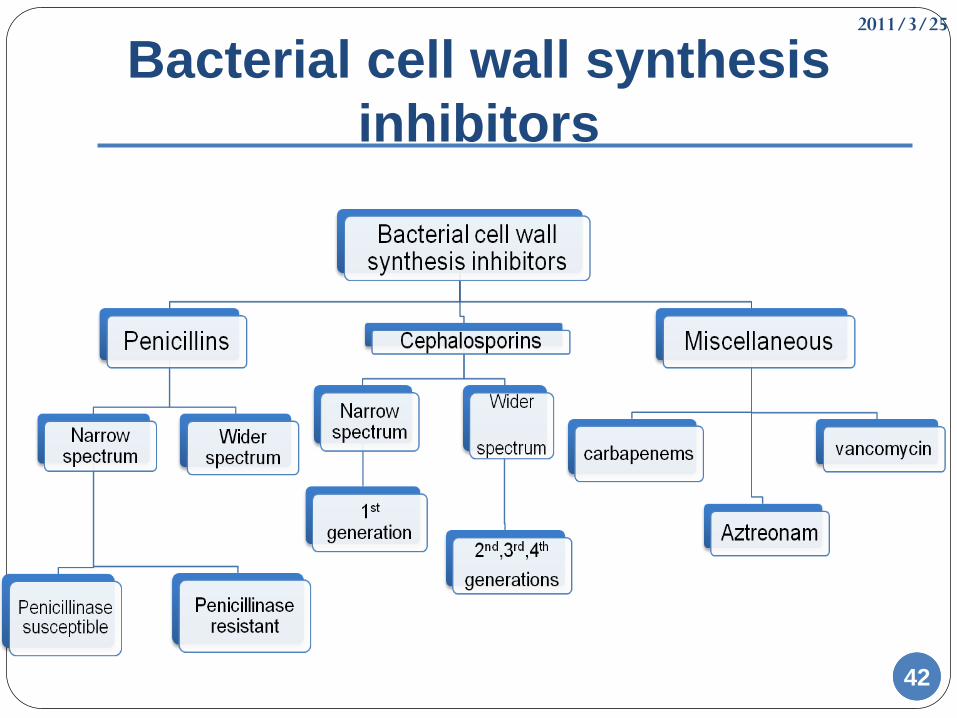
Bacterial cell wall synthesis
inhibitors
β-lactam antibioticsPenicillins
Cephalosporins
Carbapenems: Imipenem, meropenem, ertapenem
Monobactam : Aztreonam
Glycopeptides:Vancomycin, Teicoplanin
Lipopeptide:Daptomycin
2011/3/25
3535
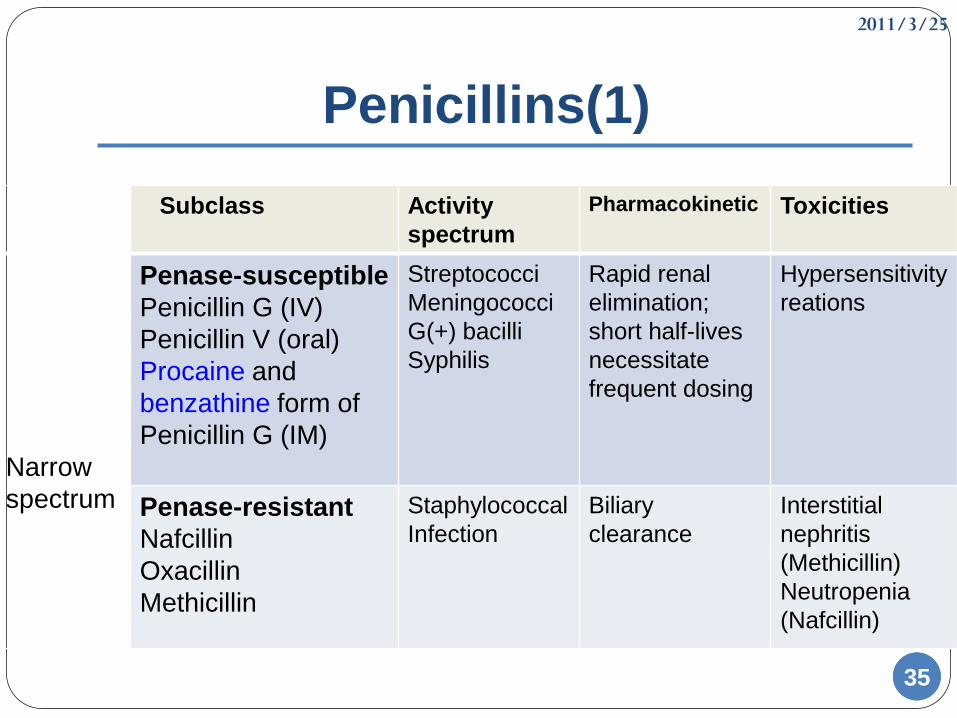
Penicillins(1)
Subclass Activity
spectrum
Pharmacokinetic Toxicities
Narrow
spectrum
Penase-susceptible
Penicillin G (IV)
Penicillin V (oral)
Procaine and
benzathine form of
Penicillin G (IM)
Streptococci
Meningococci
G(+) bacilli
Syphilis
Rapid renal
elimination;
short half-lives
necessitate
frequent dosing
Hypersensitivity
reations
Penase-resistant
Nafcillin
Oxacillin
Methicillin
Staphylococcal
Infection
Biliary
clearance
Interstitial
nephritis
(Methicillin)
Neutropenia
(Nafcillin)
2011/3/25
3636
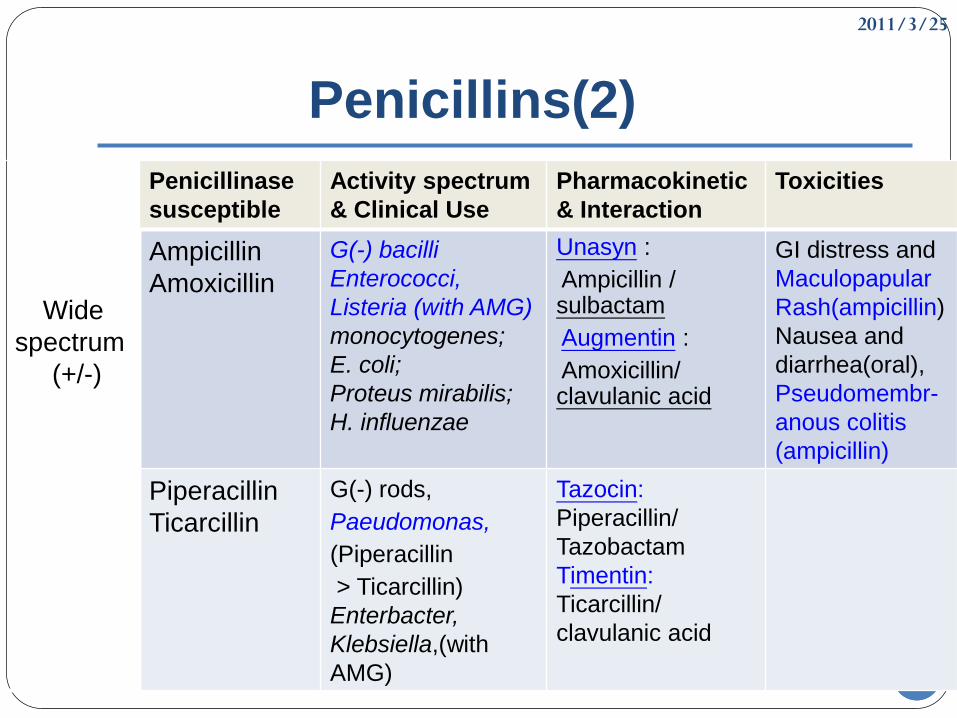
Penicillins(2)
Wide
spectrum
(+/-)
Penicillinase
susceptible
Activity spectrum
& Clinical Use
Pharmacokinetic
& Interaction
Toxicities
Ampicillin
Amoxicillin
G(-) bacilli
Enterococci,
Listeria (with AMG)
monocytogenes;
E. coli;
Proteus mirabilis;
H. influenzae
Unasyn :
Ampicillin / sulbactam
Augmentin :
Amoxicillin/ clavulanic acid
GI distress and
Maculopapular
Rash(ampicillin)
Nausea and
diarrhea(oral),
Pseudomembr-
anous colitis
(ampicillin)
Piperacillin
Ticarcillin
G(-) rods,
Paeudomonas,
(Piperacillin
> Ticarcillin)
Enterbacter,
Klebsiella,(with
AMG)
Tazocin:
Piperacillin/
Tazobactam
Timentin:
Ticarcillin/
clavulanic acid
2011/3/25
3737
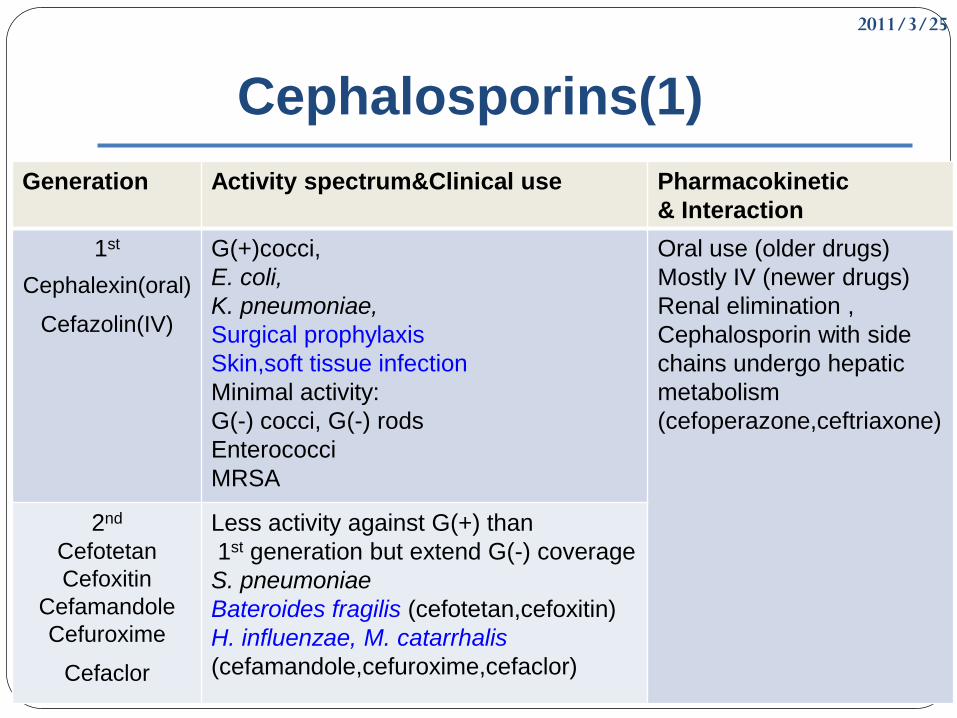
Cephalosporins(1)
Generation Activity spectrum&Clinical use Pharmacokinetic
& Interaction
1st
Cephalexin(oral)
Cefazolin(IV)
G(+)cocci,
E. coli,
K. pneumoniae,
Surgical prophylaxis
Skin,soft tissue infection
Minimal activity:
G(-) cocci, G(-) rods
Enterococci
MRSA
Oral use (older drugs)
Mostly IV (newer drugs)
Renal elimination ,
Cephalosporin with side
chains undergo hepatic
metabolism
(cefoperazone,ceftriaxone)
2nd
Cefotetan
Cefoxitin
Cefamandole
Cefuroxime
Cefaclor
Less activity against G(+) than
1st generation but extend G(-) coverage
S. pneumoniae
Bateroides fragilis (cefotetan,cefoxitin)
H. influenzae, M. catarrhalis
(cefamandole,cefuroxime,cefaclor)
2011/3/25
3838
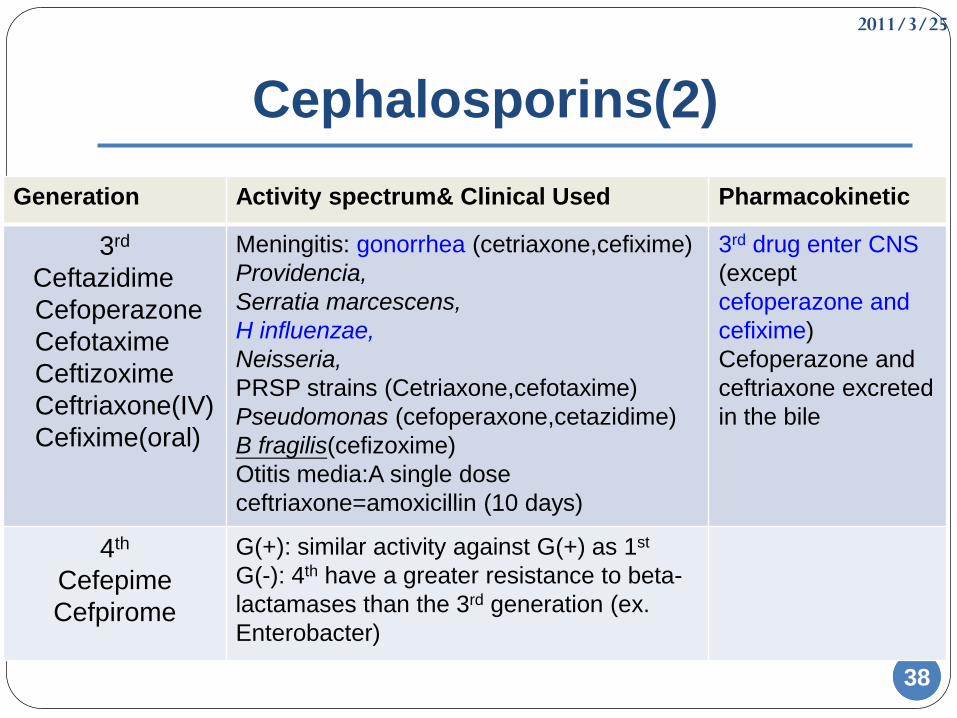
Cephalosporins(2)
Generation Activity spectrum& Clinical Used Pharmacokinetic
3rd
Ceftazidime
Cefoperazone
Cefotaxime
Ceftizoxime
Ceftriaxone(IV)
Cefixime(oral)
Meningitis: gonorrhea (cetriaxone,cefixime)
Providencia,
Serratia marcescens,
H influenzae,
Neisseria,
PRSP strains (Cetriaxone,cefotaxime)
Pseudomonas (cefoperaxone,cetazidime)
B fragilis(cefizoxime)
Otitis media:A single dose
ceftriaxone=amoxicillin (10 days)
3rd drug enter CNS
(except
cefoperazone and
cefixime)
Cefoperazone and
ceftriaxone excreted
in the bile
4th
Cefepime
Cefpirome
G(+): similar activity against G(+) as 1st
G(-): 4th have a greater resistance to beta-
lactamases than the 3rd generation (ex.
Enterobacter)
2011/3/25
3939
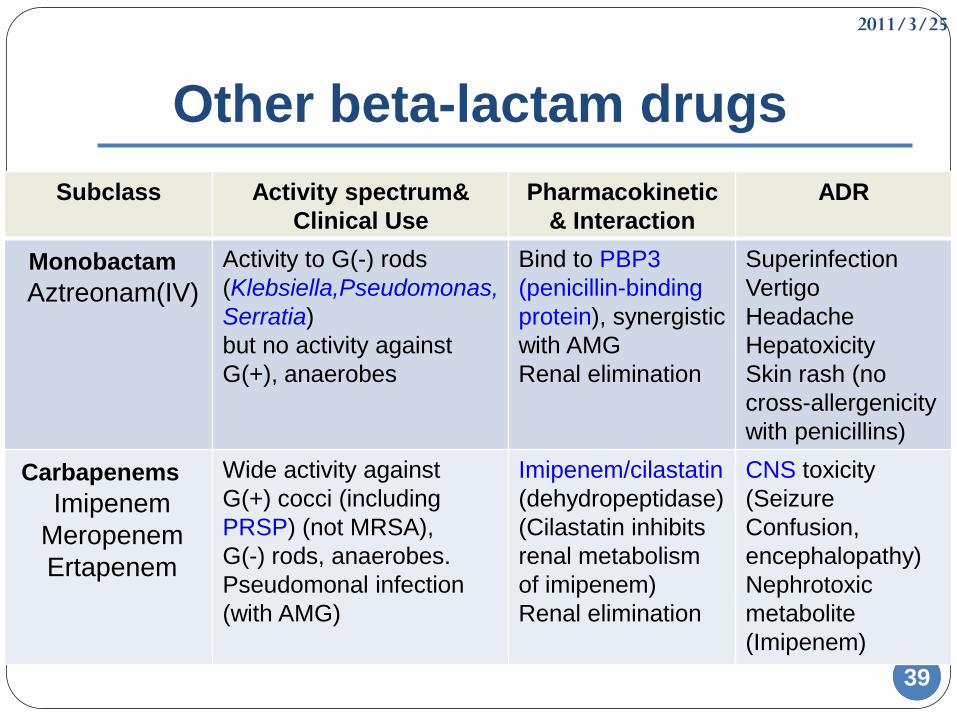
Other beta-lactam drugs
Subclass Activity spectrum&
Clinical Use
Pharmacokinetic
& Interaction
ADR
Monobactam
Aztreonam(IV)
Activity to G(-) rods
(Klebsiella,Pseudomonas,
Serratia)
but no activity against
G(+), anaerobes
Bind to PBP3
(penicillin-binding
protein), synergistic
with AMG
Renal elimination
Superinfection
Vertigo
Headache
Hepatoxicity
Skin rash (no
cross-allergenicity
with penicillins)
Carbapenems
Imipenem
Meropenem
Ertapenem
Wide activity against
G(+) cocci (including
PRSP) (not MRSA),
G(-) rods, anaerobes.
Pseudomonal infection
(with AMG)
Imipenem/cilastatin
(dehydropeptidase)
(Cilastatin inhibits
renal metabolism
of imipenem)
Renal elimination
CNS toxicity
(Seizure
Confusion,
encephalopathy)
Nephrotoxic
metabolite
(Imipenem)
2011/3/25
4040
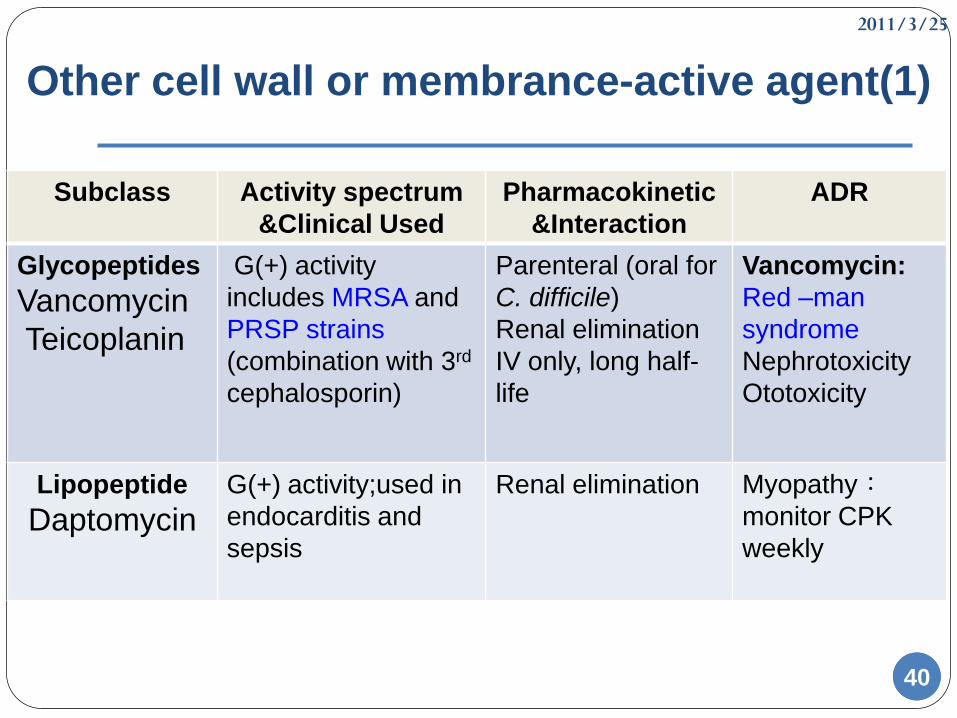
Other cell wall or membrance-active agent(1)
Subclass Activity spectrum
&Clinical Used
Pharmacokinetic
&Interaction
ADR
Glycopeptides
Vancomycin
Teicoplanin
G(+) activity
includes MRSA and
PRSP strains
(combination with 3rd
cephalosporin)
Parenteral (oral for
C. difficile)
Renal elimination
IV only, long half-
life
Vancomycin:
Red –man
syndrome
Nephrotoxicity
Ototoxicity
Lipopeptide
DaptomycinG(+) activity;used in
endocarditis and
sepsis
Renal elimination Myopathy:monitor CPK
weekly
2011/3/25
4141
Other cell wall or membrance-active
agent(2)
Fosfomycin
1. An antimetabolite inhibitor of cytosolic enolpyruvate
2. Minimal inhibitory concentrations for many UTI
3. Synergistic with B-lactam and quinolone antibiotics
4. Diarrhea is common
Cycloserine
only used to treat tuberculosis when first-line drug useless
Bacitracin
Because of its marked nephrotoxicity,the drug is limited to
topical use.
2011/3/25
4242
Bacterial cell wall synthesis
inhibitors
2011/3/25
43
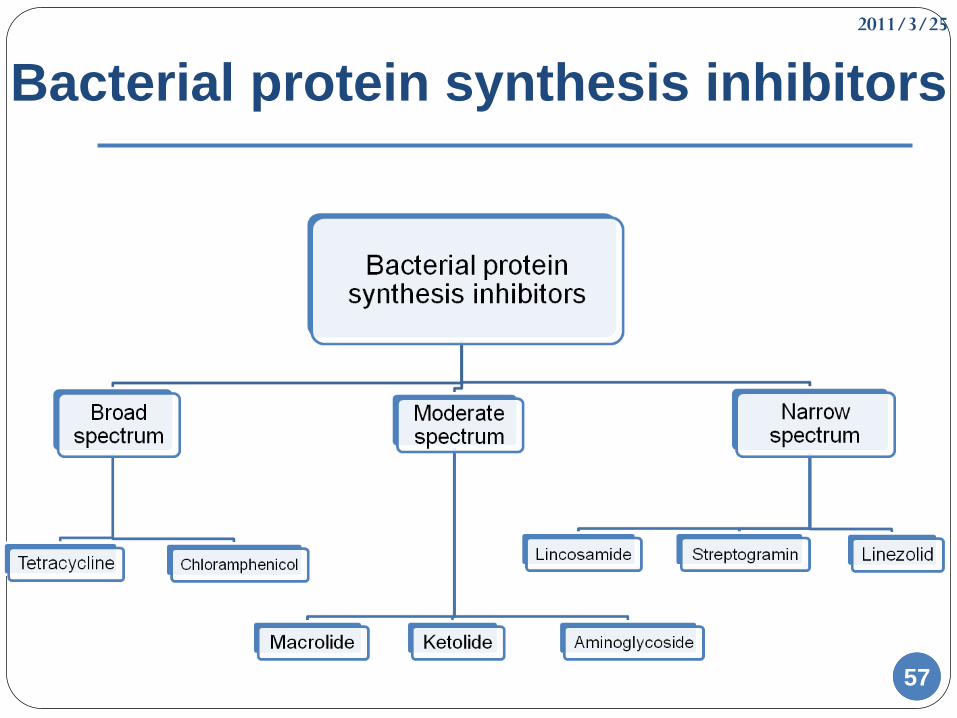
Bacterial protein synthesis
inhibitors
Bind to 30s:Tetracycline, Aminoglycoside
Bind to 50s:Chloramphenicol, Streptogramins,
Macrolides
Bind to 23s of 50s:Linezolid
43
2011/3/25
4444
Tetracycline(1)
Tetracycline der. : Tetracycline, Minocycline, Doxycycline
Glycylcycline der. : Tigecycline
Mechanism Bind 30s ,Broad-spectrum bacteriostatic antibiotics
Pharmacokinetics
Oral absorption is variable: May be impair by food and
multivalent cations
Wide tissue distribution and cross placental barrier
Drugs eliminated primarily in the urine (except doxycycline )
2011/3/25
4545
Tetracycline(2)
Activity1. G(+),G(-) bacteria (Rickettsia, Chlamydia, Mycoplasma),
some protozoa
2. Proteus, pseudomonas resistance to all of Tetracycline
(including Tigecycline)
Clinical use
1. Infections due to chlamydiae, mycoplasma, rickettsiae,
spirochetes ,and H.poly (Doxycycline is an alternative to
macrolide in the initial treatment of CA-pneumonia)
2.Treatment of acne (low dose)
3.Tetracycline: alternative drugs in the treatment of syphilis
4.Tigecycline : MRSA, VRE, anaerobes, Chlamydiae, mycobacteria
β-lactamase-producing G(-) bacteria
2011/3/25
4646
Tetracycline(3)
Toxicity
1. Gastrointestinal disturbances
2. Bony structures and teeth dysplasia
3. Hepatic toxicity : high dose
4. Photosensitivity : especially demeclocycline
5. Vestibular toxicity : doxycycline, minocycline
2011/3/25
4747
Chloramphenicol(1)
Mechanism
Bind to 50S ribosomal subunit ; usually bacteriostatic
Activity& Clinical use
1. Wide spectrum (H.influenzae, Nesseria menibgitidis,
bacteroides)
2. Backup drug for serve infection by Salmonella
3. Treatment Peumococcal and Meningococcal in the
person who is β-lactam hypersensitive
4. Topical use
2011/3/25
4848
Chloramphenicol(2)
Toxicity 1. Gastrointestinal disturbance
2. Bone marrow : dose dependent and reversible (except
aplastic anemia )
3. Gray baby syndrome
Drug interationChloramphenicol inhibits hapatic drug-metabolizing
enzymes
2011/3/25
4949
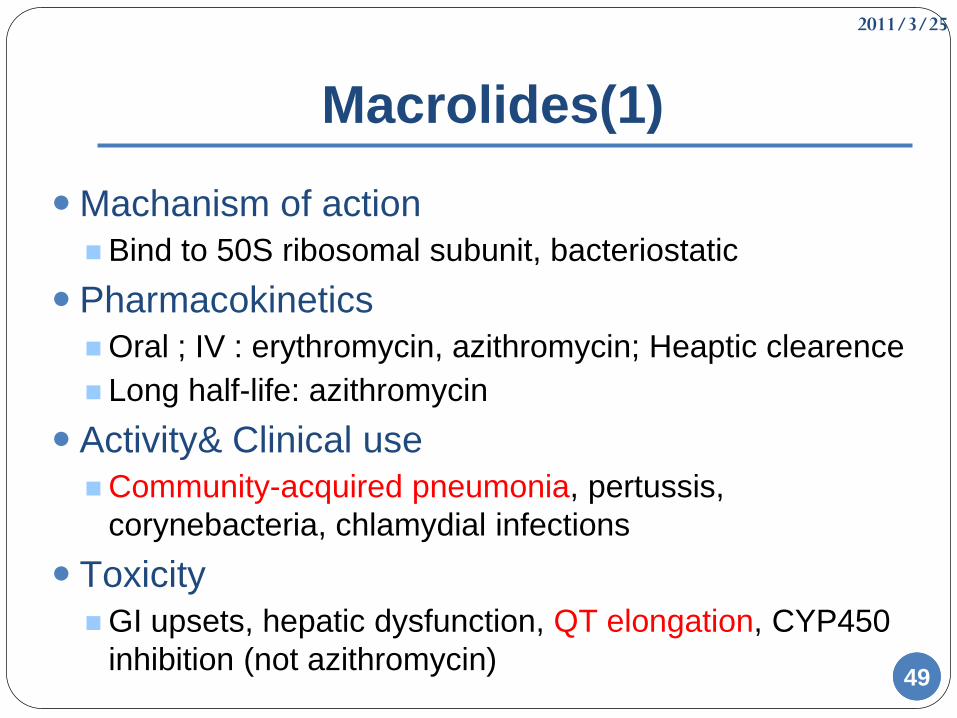
Macrolides(1)
Machanism of action
Bind to 50S ribosomal subunit, bacteriostatic
Pharmacokinetics
Oral ; IV : erythromycin, azithromycin; Heaptic clearence
Long half-life: azithromycin
Activity& Clinical use
Community-acquired pneumonia, pertussis,
corynebacteria, chlamydial infections
Toxicity
GI upsets, hepatic dysfunction, QT elongation, CYP450
inhibition (not azithromycin)
2011/3/25
5050
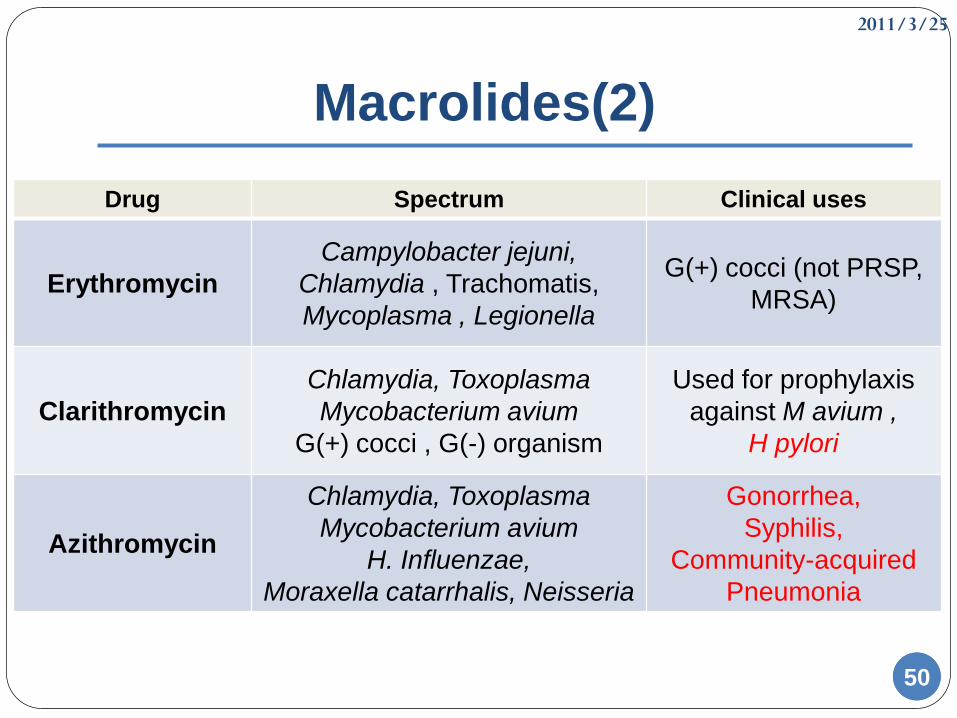
Macrolides(2)
Drug Spectrum Clinical uses
Erythromycin
Campylobacter jejuni,
Chlamydia , Trachomatis,
Mycoplasma , Legionella
G(+) cocci (not PRSP,
MRSA)
Clarithromycin
Chlamydia, Toxoplasma
Mycobacterium avium
G(+) cocci , G(-) organism
Used for prophylaxis
against M avium ,
H pylori
Azithromycin
Chlamydia, Toxoplasma
Mycobacterium avium
H. Influenzae,
Moraxella catarrhalis, Neisseria
Gonorrhea,
Syphilis,
Community-acquired
Pneumonia
2011/3/25
5151
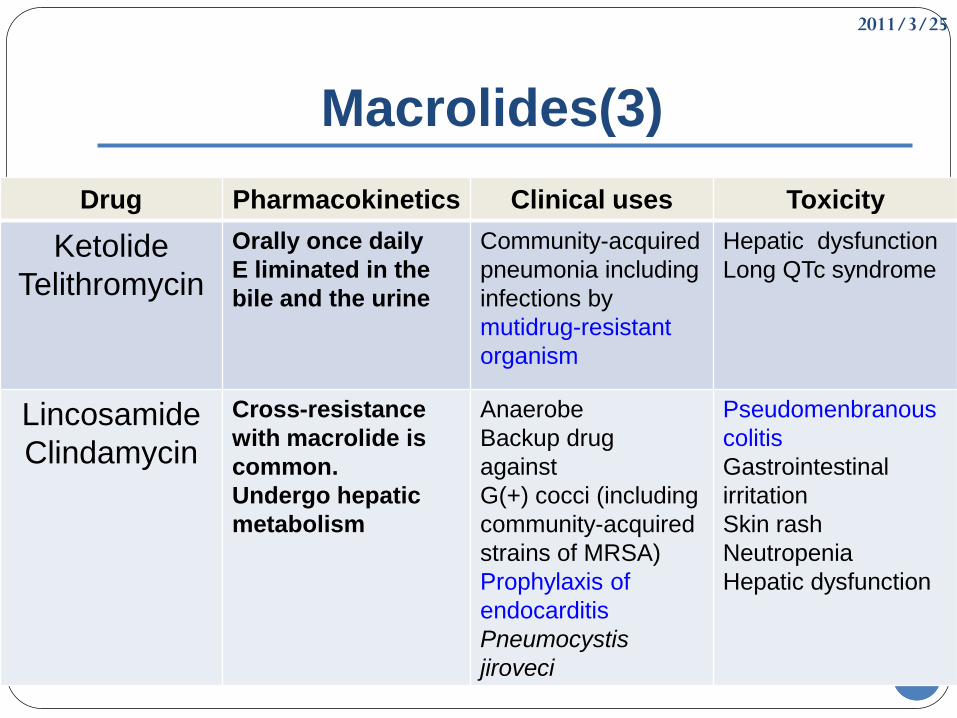
Macrolides(3)
Drug Pharmacokinetics Clinical uses Toxicity
Ketolide
Telithromycin
Orally once daily
E liminated in the
bile and the urine
Community-acquired
pneumonia including
infections by
mutidrug-resistant
organism
Hepatic dysfunction
Long QTc syndrome
Lincosamide
Clindamycin
Cross-resistance
with macrolide is
common.
Undergo hepatic
metabolism
Anaerobe
Backup drug
against
G(+) cocci (including
community-acquired
strains of MRSA)
Prophylaxis of
endocarditis
Pneumocystis
jiroveci
Pseudomenbranous
colitis
Gastrointestinal
irritation
Skin rash
Neutropenia
Hepatic dysfunction
2011/3/25
5252
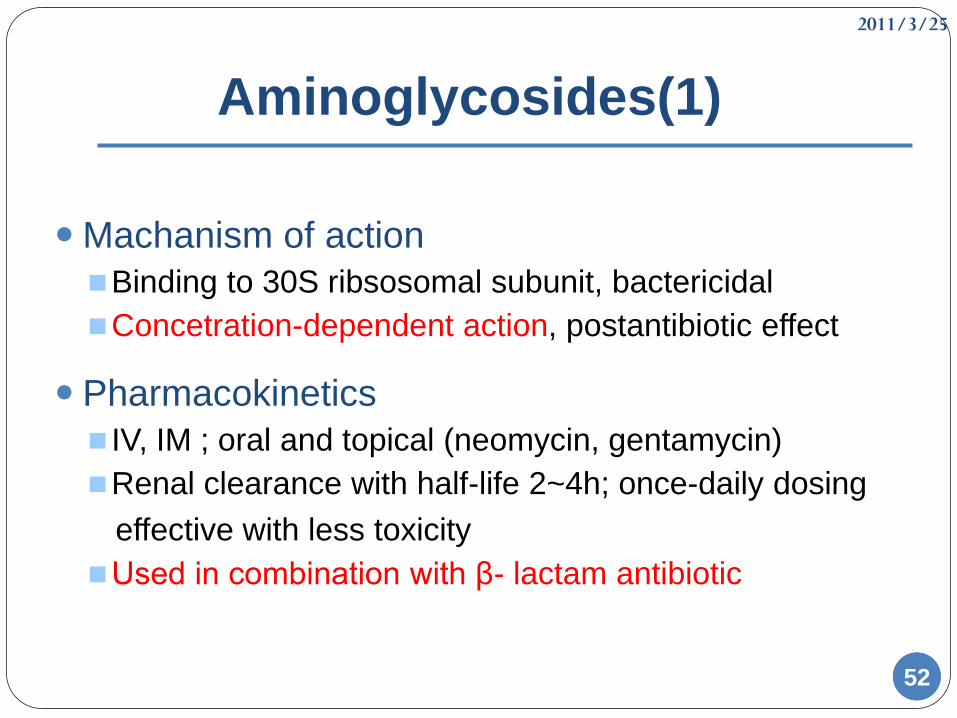
Aminoglycosides(1)
Machanism of action
Binding to 30S ribsosomal subunit, bactericidal
Concetration-dependent action, postantibiotic effect
Pharmacokinetics
IV, IM ; oral and topical (neomycin, gentamycin)
Renal clearance with half-life 2~4h; once-daily dosing
effective with less toxicity
Used in combination with β- lactam antibiotic
2011/3/25
5353
Aminoglycosides(2)
Activity& Clinical uses
1. Gentamicin, Tobramycin, Amikacin : Aerobic G(-) bacteria
(including E. coli, Enterobacter, Klebsiella, Proteus,
Providencia, Pseudomonas)
2. Streptomycin : enterocococcal carditis , tuberculosis,
plague, tularemia
3. Neomycin, Kanamycin: Topical or oral use (to eliminate
bowel flora)
4. Spectinomycin : It is a backup drug for treament of
gonorrhea
5. Netilmicin
2011/3/25
5454
Aminoglycosides(3)
Toxicity
1. Ototoxicity: auditory or vestibular damage, irreversible
2. Nephrotoxicity: reversible
3. Neuromuscular Blockade: curare-like block may occur
at high dose, may result in respiratory paralysis
4. Skin Reaction: neomycin usually occur
2011/3/25
5555
Streptogramins
Quinupristin-dalfopristin
Mechanism
Bind to 50S ribososomal subunit, bactericidal
Activity & Clinical uses
Staphyloccal infections, vancomycin-resistant E faecium
Pharmacokinetics
IV; renal clearance
Toxicity
Infusion-related arthralgia and myalgia, CYP450 inhibition

2011/3/25
5656
Oxazolidinone
Linezolid
Mechchanism
Bind to 23s RNA of 50S subnit; bacteriostatic
Activity & Clinical use
Including MRSA, PRSP and VRE strains
Pharmacokinetics
Oral, IV; hepatic clearance
Toxicity
1. Dose-related anemia, neuropathy, optic neuritis
2. serotonin syndrome with SSRIs
2011/3/25
5757
Bacterial protein synthesis inhibitors
2011/3/25
5858
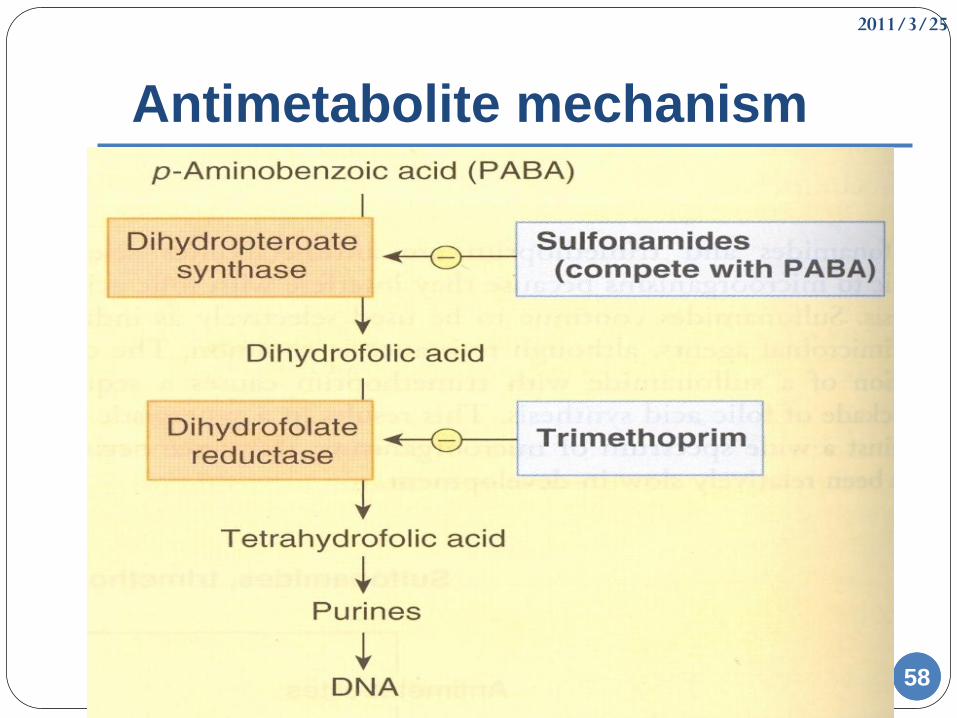
Antimetabolite mechanism
2011/3/25
5959
Trimethoprim-sulfamethoxazole
Mechanism
Synergistic inhibition of folic acid synthesis
The combination is bactericidal ”sequential blockade”
Activity & Clinical use
1. Urinary tract, respiratory, ear, sinus infections
2. P jiroveci pneumonia; Toxoplasmosis; Nocardiosis
Pharmacokinetics
Oral, IV
Renal clearance , half-life: 8h
Toxicity
1. Rash, fever, bone marrow supression, hyperkalemia
2. High incidence of aderse effects in AIDS
2011/3/25
6060
Other folate antagonist(1)
Sufonamides:
Sulfisoxazole: Simple UTI
Sulfacetamide: ocular infection
Mafenide, siver sulfadiazine: Burn infections
Sulfadiazine + pyrimethamine: Toxoplasmosis
Mechanism
Sulfonamides inhibit dihydropteroate synthase
Trimethoprim and pyrimethamine inhibit dihydrofolate
reductase
Activity
Most G(+),G(-),Chlamydia, Nocardia
2011/3/25
6161
Other folate antagonist(2)
Toxicity
1. Hypersentivity : cross-allergenicity
2. Gastrointestinal
3. Hematotoxicity
4. Nephrotoxicity
5. Kernicterus
Drug interaction
Competition with plasma protein binding
2011/3/25
6262
Fluoroquinolones(1)
Narrow spectrum
1st generation
Wide spectrum
2nd generation
3rd generation
4th generaion
Background
Nalidixic acid derivatives
2011/3/25
6363
Fluoroquinolones(2)
Mechanism
Inhibits DNA replication via binding to DNA gyrase, and
topoisomerase Ⅳ; bactericidal
Pharmacokinetics
Oral
Interaction with multivalent cations
Renal elimination
Resistance
Production of efflux pump or change in the porin
2nd : Campylobacter jejuni, gonococci, G(+) cocci,
P.aeruginosa
2011/3/25
6464
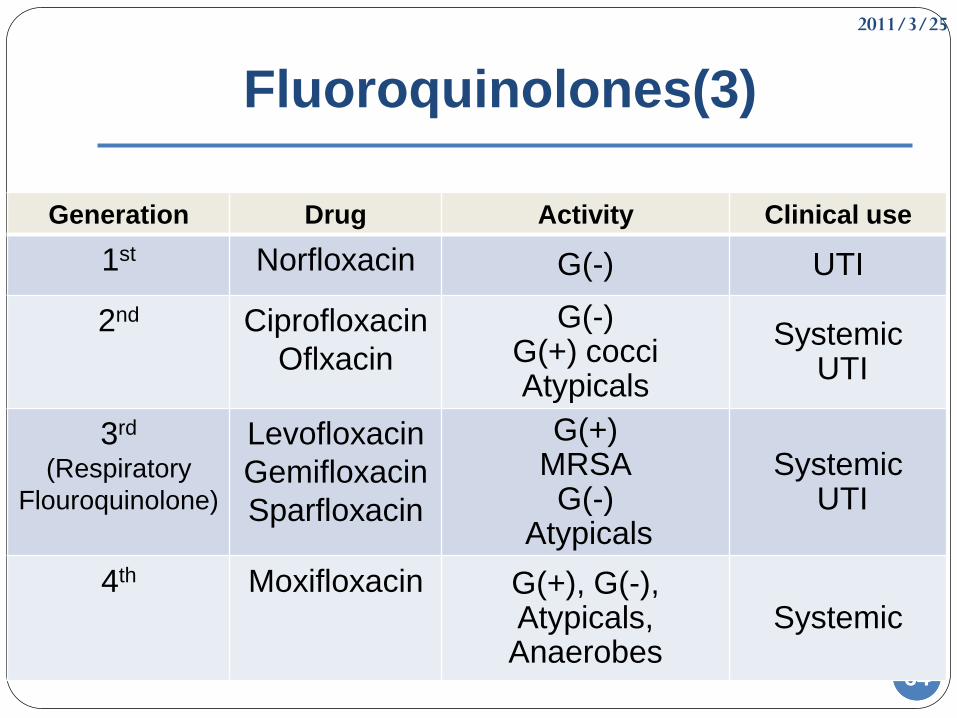
Fluoroquinolones(3)
Generation Drug Activity Clinical use
1st Norfloxacin G(-) UTI
2nd Ciprofloxacin
Oflxacin
G(-) G(+) cocciAtypicals
SystemicUTI
3rd
(Respiratory
Flouroquinolone)
Levofloxacin
Gemifloxacin
Sparfloxacin
G(+) MRSAG(-)
Atypicals
SystemicUTI
4th Moxifloxacin G(+), G(-), Atypicals,
AnaerobesSystemic
2011/3/25
6565
Fluoroquinolones(4)
Toxicity
GI distress
Abnomal liver function
Phototoxicity
Damage growing cartilage and cause arthropathy
Newer fluoroquinolones prolong the QTc interval
(gemifloxacin, levofloxacin, moxifloxacin)
2011/3/25
6666
Case Report
2011/3/25
6767
Patient profile(1)
Patient information
L女士 68y/o 158cm 55kg
DOA: 2010/12/28
DOD: 2011/01/22
Chief complaint
Fever with chillness since 3 days ago
2011/3/25
6868
Patient profile(2)
History of present illness
Fever up to 38℃ with chills
Elevated blood pressure (SBP 210mmHg)
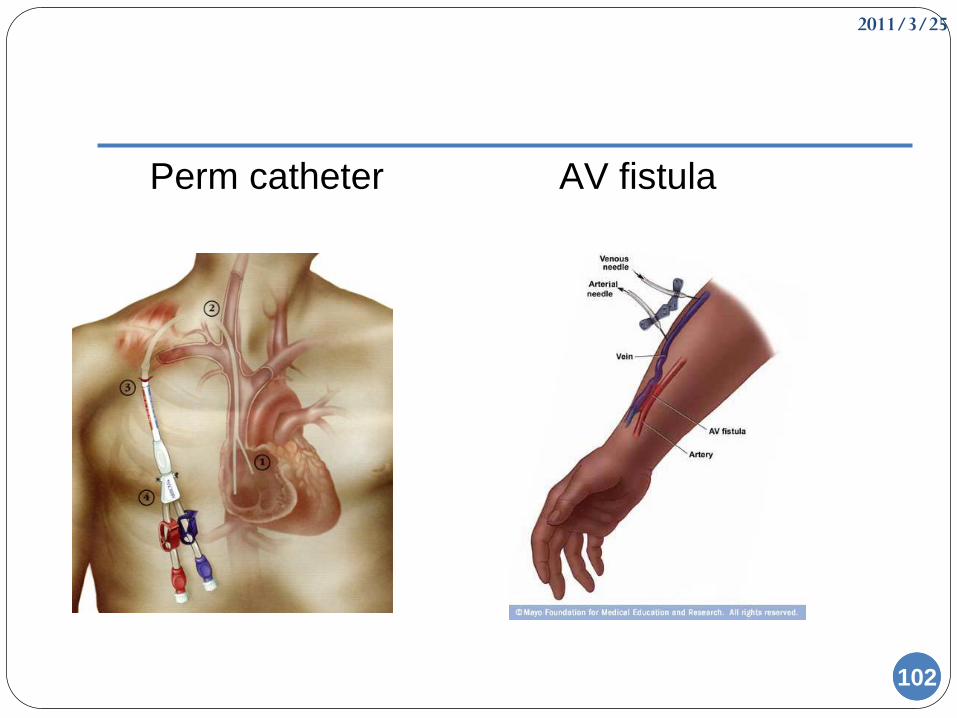
A Perm catheter over right subclavian area, an AV fistula over right forearm and a wound with discharge over right big toe
Hemogram: WBC 11900/cumm WBC 15300/cumm
CRP 1.26mg/dL CRP 11.07mg/dL
Blood culture yielded GPC in cluster (x2)
Urine routine showed proteinuria (100mg/dL)
Antibiotic: Tazocin and then Teicoplanin+ Ceftazidime
Teicoplanin+ Ciprofloxacin for bacteremia
(Perm-cath infection), IE
2011/3/25
6969
Patient profile(3)
Past History
Catheter infection related infective endocarditisSepsis, septic arthritis at right knee End stage renal disease with uremic syndrome Hypertension ,Type II DM , Hyperlipidemia Heart failure, NYHA Fc II Coronary artery disease Duodenal ulcer Chronic obstructive pulmonary disease Cerebellar infarction with hydrocephalus
2011/3/25
7070
Patient profile(4)
Personal History
Alcohol: denied
Betel nut: denied
Cigarette smoking: denied
Drugs allergy: denied
Travel: denied
Animal contact: denied
Family History
diabetes
2011/3/25
7171
Patient profile(5)
Physical Examination
General appearance: ill-looking; conscious: clear
Skin: dry, eczema on left elbow, obvious
erythematous papules (-)
Chest: (+)Symmetric expansion
Extremities: A wound, about 0.2 cm in diameter over
right big toe, discharge freely movable(-), pitting
edema(-), clubbing fingers(-)
Back: lower back and CP angle knocking pain (-)
2011/3/25
7272
Patient profile(6)
Impression
MRSA related perm catheter infection
Plan to do & Goal
Keep antibiotic use : Teicoplanin + Ciprofloxacin
Follow blood culture
Keep hemodialysis
Wound care over right big toe
2011/3/25
7373
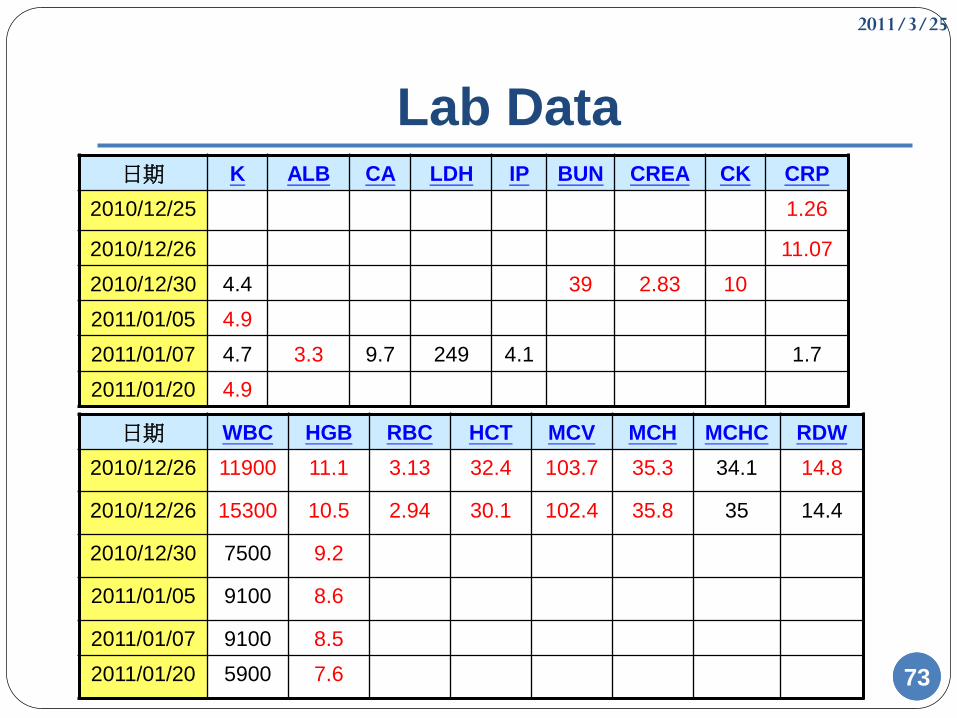
Lab Data日期 K ALB CA LDH IP BUN CREA CK CRP
2010/12/25 1.26
2010/12/26 11.07
2010/12/30 4.4 39 2.83 10
2011/01/05 4.9
2011/01/07 4.7 3.3 9.7 249 4.1 1.7
2011/01/20 4.9
日期 WBC HGB RBC HCT MCV MCH MCHC RDW
2010/12/26 11900 11.1 3.13 32.4 103.7 35.3 34.1 14.8
2010/12/26 15300 10.5 2.94 30.1 102.4 35.8 35 14.4
2010/12/30 7500 9.2
2011/01/05 9100 8.6
2011/01/07 9100 8.5
2011/01/20 5900 7.6
2011/3/25
74
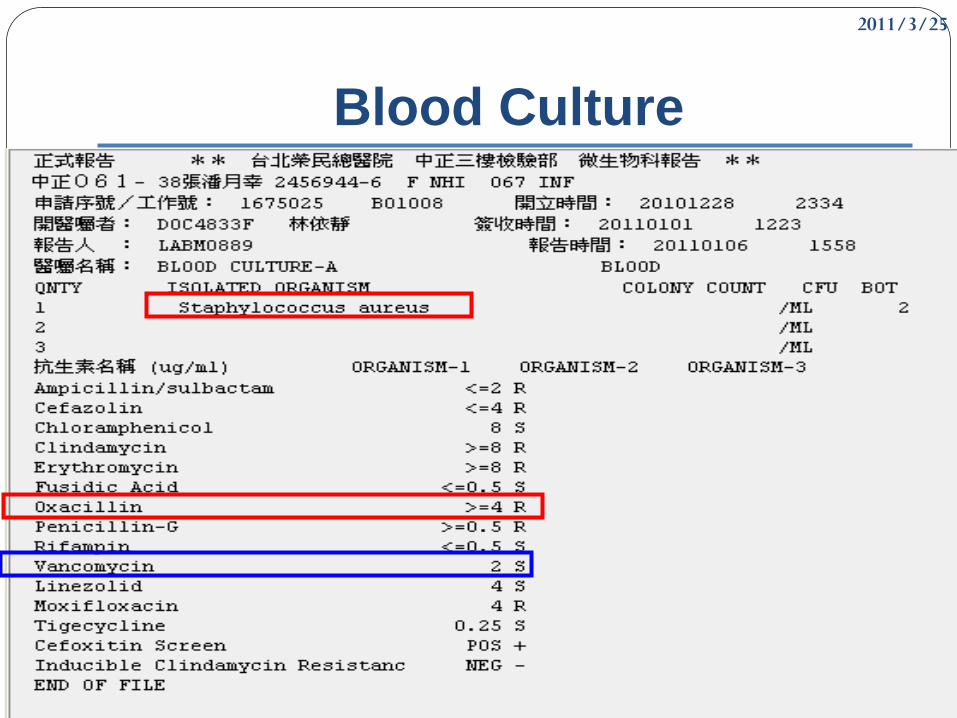
Blood Culture
2011/3/25
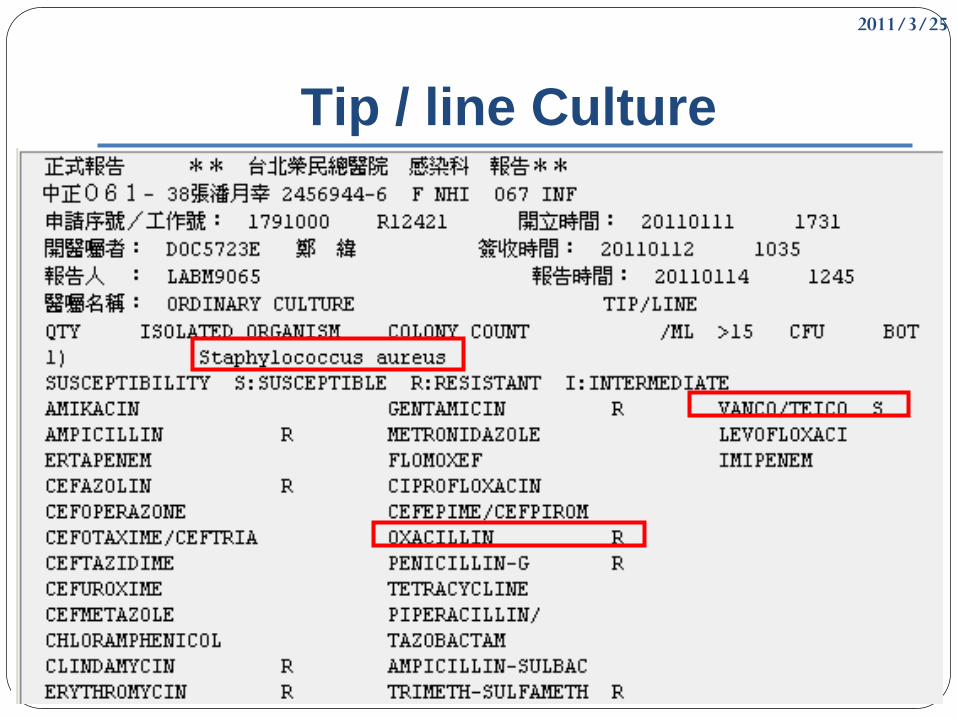
75
Tip / line Culture
2011/3/25
7676
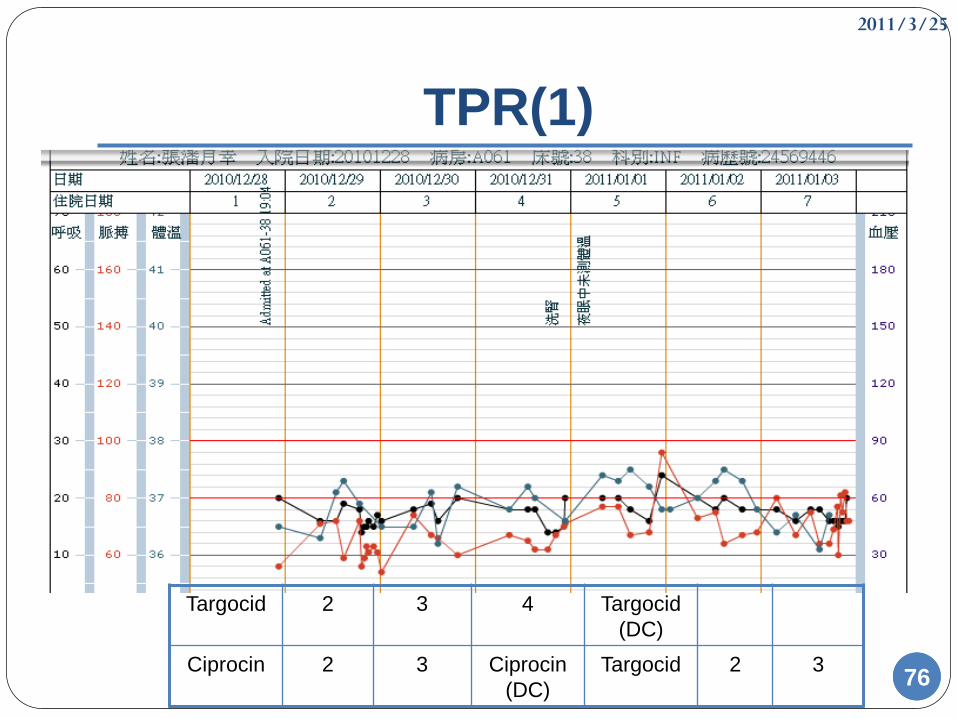
TPR(1)
Targocid 2 3 4 Targocid
(DC)
Ciprocin 2 3 Ciprocin
(DC)
Targocid 2 3
2011/3/25
7777
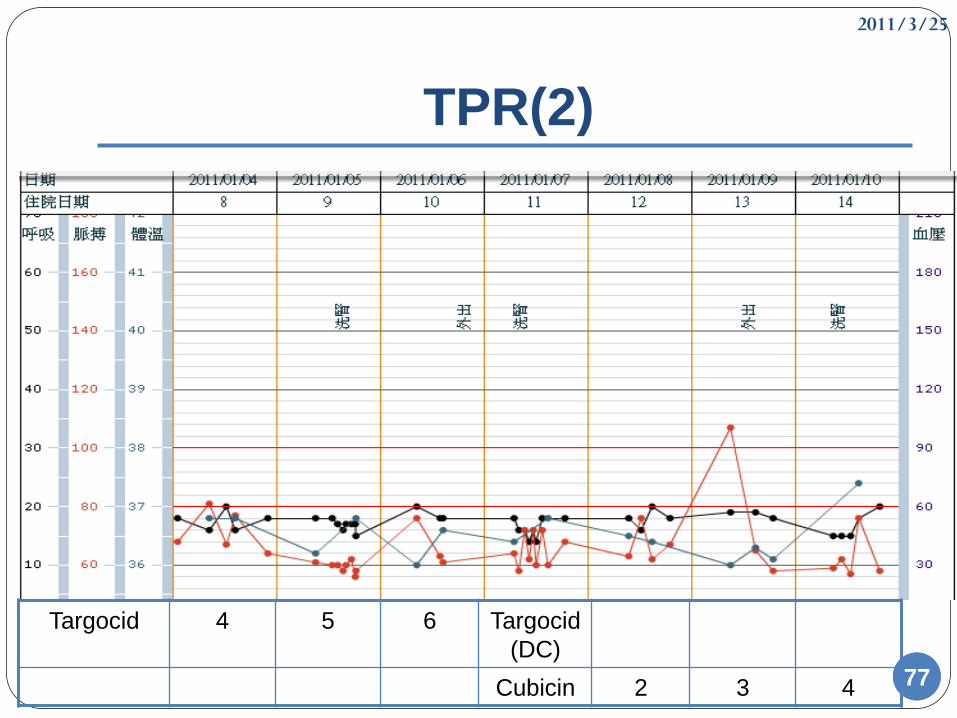
TPR(2)
Targocid 4 5 6 Targocid
(DC)
Cubicin 2 3 4
2011/3/25
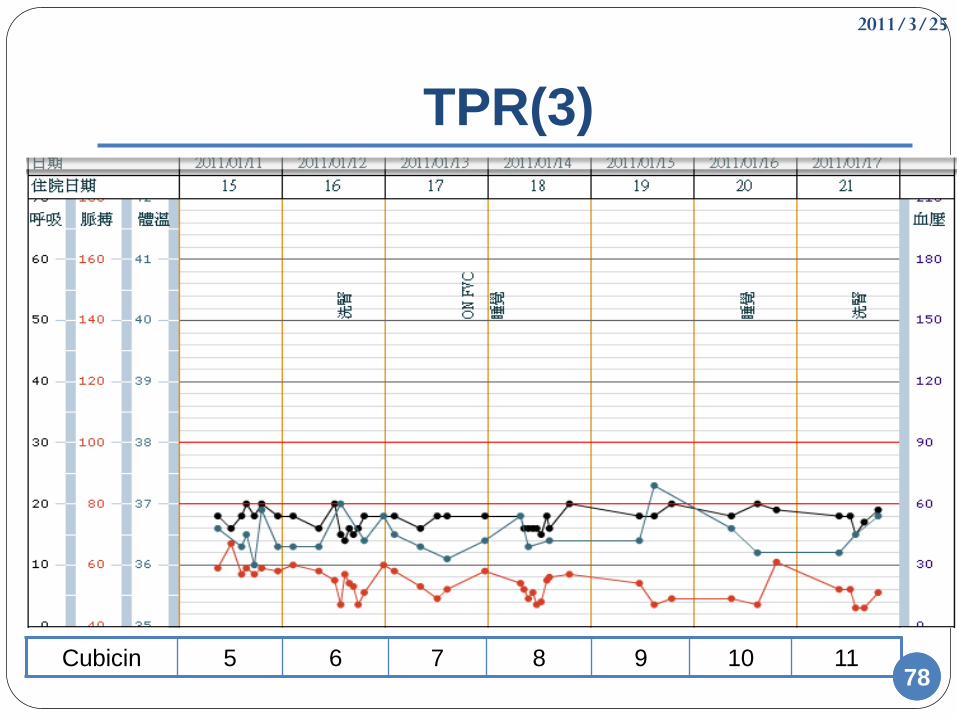
7878
TPR(3)
Cubicin 5 6 7 8 9 10 11
2011/3/25
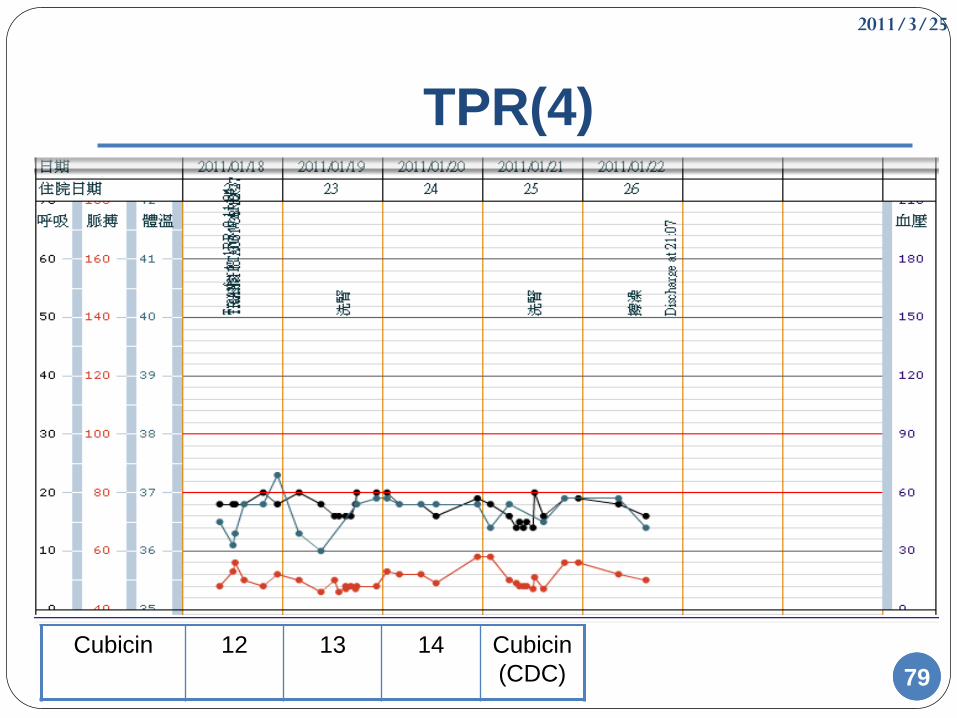
7979
TPR(4)
Cubicin 12 13 14 Cubicin
(CDC)
2011/3/25
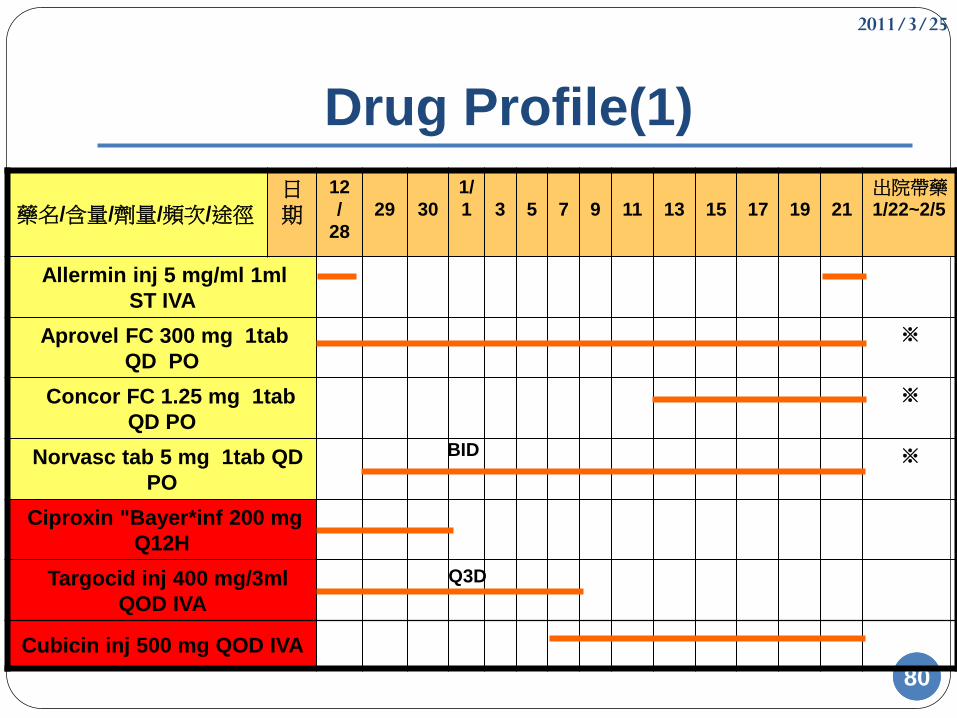
8080
Drug Profile(1)
藥名/含量/劑量/頻次/途徑日期
12
/
28
29 30
1/
1 3 5 7 9 11 13 15 17 19 21
出院帶藥1/22~2/5
Allermin inj 5 mg/ml 1ml
ST IVA
Aprovel FC 300 mg 1tab
QD PO
※
Concor FC 1.25 mg 1tab
QD PO
※
Norvasc tab 5 mg 1tab QD
PO
※
Ciproxin "Bayer*inf 200 mg
Q12H
Targocid inj 400 mg/3ml
QOD IVA
Cubicin inj 500 mg QOD IVA
BID
Q3D
2011/3/25
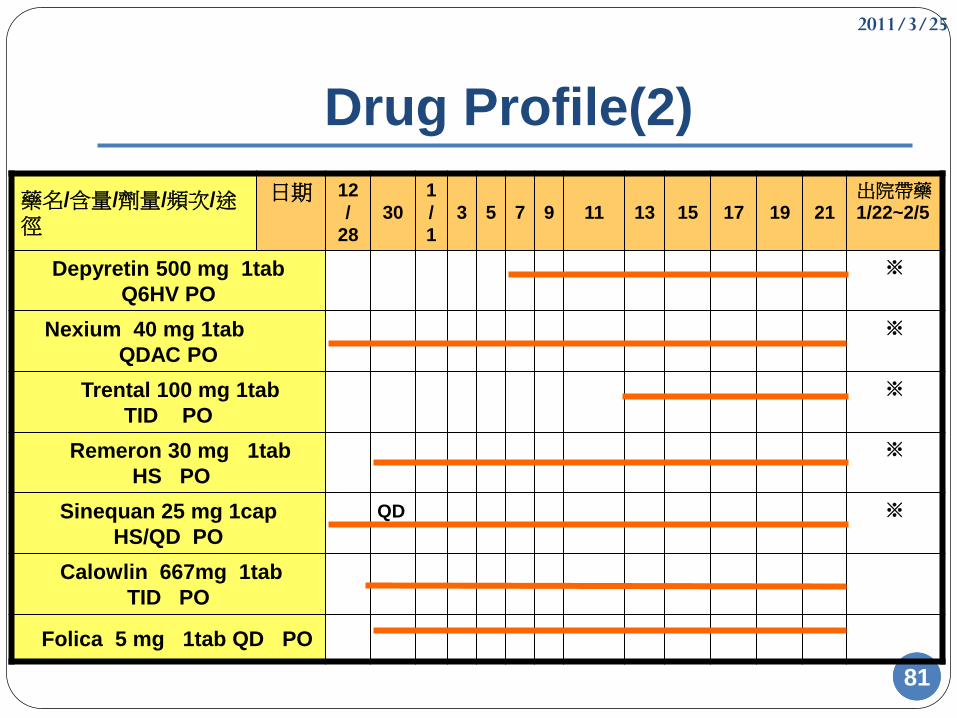
8181
Drug Profile(2)
藥名/含量/劑量/頻次/途徑
日期 12
/
28
30
1
/
1
3 5 7 9 11 13 15 17 19 21
出院帶藥1/22~2/5
Depyretin 500 mg 1tab
Q6HV PO
※
Nexium 40 mg 1tab
QDAC PO
※
Trental 100 mg 1tab
TID PO
※
Remeron 30 mg 1tab
HS PO
※
Sinequan 25 mg 1cap
HS/QD PO
※
Calowlin 667mg 1tab
TID PO
Folica 5 mg 1tab QD PO
QD
2011/3/25
8282
Case Discussion
Catheter related infection
MRSA related infection
Antibiotics dose with hemodialysis patient
2011/3/25
83
Catheter related infection
2011/3/25
84
Catheter-related Bacteremia(1)
Pathogens
1. Staphylococcus epidermidis
2. Staphylococcus aureus (27% to 39%)
3. Enterococcus
4. Gram-negative bacilli
5. Candida spp.
6. Coagulase-negative Staphylococcus (CoNS)
7. Mycobacteria
84
2011/3/25
8585
Catheter-related Bacteremia(2)
Risk factor
1. Diabetes mellitus
2. Prolonged duration of usage catheter
3. Iron overload
4. Staphlococcus aureus nasal colonization
5. Old age
6. Low hemoglobin
7. Low serum albumin
2011/3/25
86
Catheter-related Bacteremia(3)
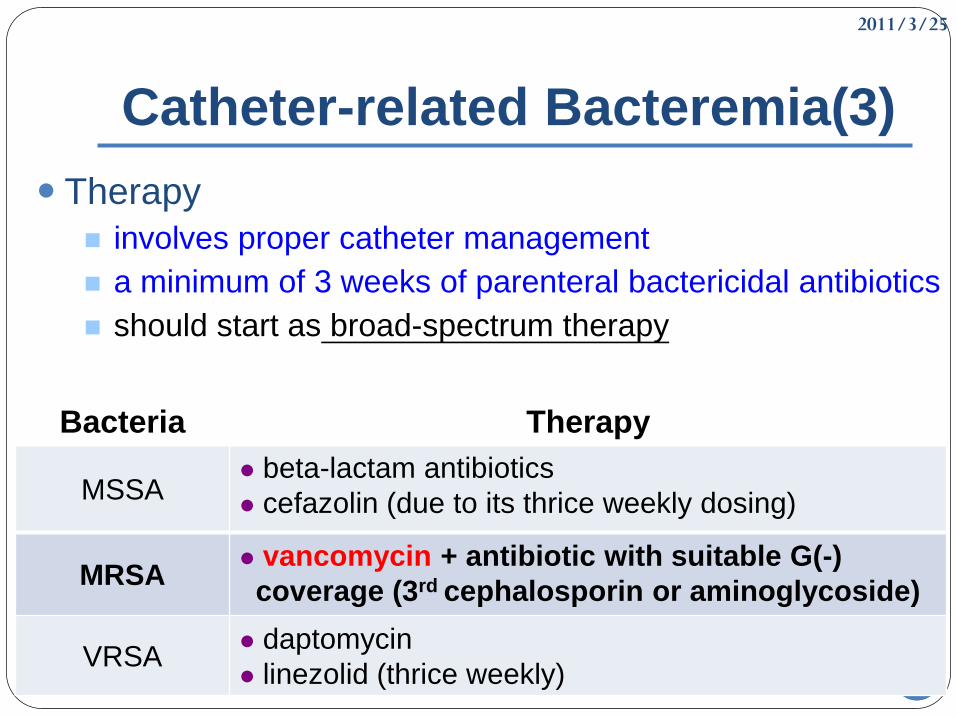
Therapy
involves proper catheter management
a minimum of 3 weeks of parenteral bactericidal antibiotics
should start as broad-spectrum therapy
86
Bacteria Therapy
MSSA beta-lactam antibiotics
cefazolin (due to its thrice weekly dosing)
MRSA vancomycin + antibiotic with suitable G(-)
coverage (3rd cephalosporin or aminoglycoside)
VRSA daptomycin
linezolid (thrice weekly)
2011/3/25
8787
MRSA related infection
2011/3/25
8888
Introduction
Methicillin-resistant Staphylococcus Aureus
(MRSA) is a type of staph bacteria that is
resistant to certain antibiotics called β-lactams.
Methicillin resistance is mediated by PBP-2a, a
penicillin binding protein encoded by the mecA
gene that permits the organism to grow and
divide in the presence of methicillin and other
beta-lactam antibiotics.
2011/3/25
8989
Epidemiology
The prevalence of MRSA has steadily increased since the first clinical isolate was described in 1961, with an estimated 94,360 cases of invasive MRSA disease in the United States in 2005.
Health care-associated MRSA (HA-MRSA)
increased from 22 to 57 percent between 1995 and 2001
Community-associated MRSA (CA-MRSA)
422 patients with skin and soft tissue infections seen in emergency departments in August 2004
- S. aureus :76 %
- CA-MRSA :97%
2011/3/25
90
Risk Factor
Invasive device
MRSA infection
Surgery
Hospitalization or in a long-term care facility
HIV infection
Antibiotic use:particularly cephalosporin and
fluoroquinolone use
Hemodialysis
2011/3/25
91
Antimicrobial therapy(1)
Clindamycin Rifampin
Daptomycin Tetracyclines
Linezolid TMP-SMX
Quinupristin-
DalfopristinVancomycin
2011/3/25
92
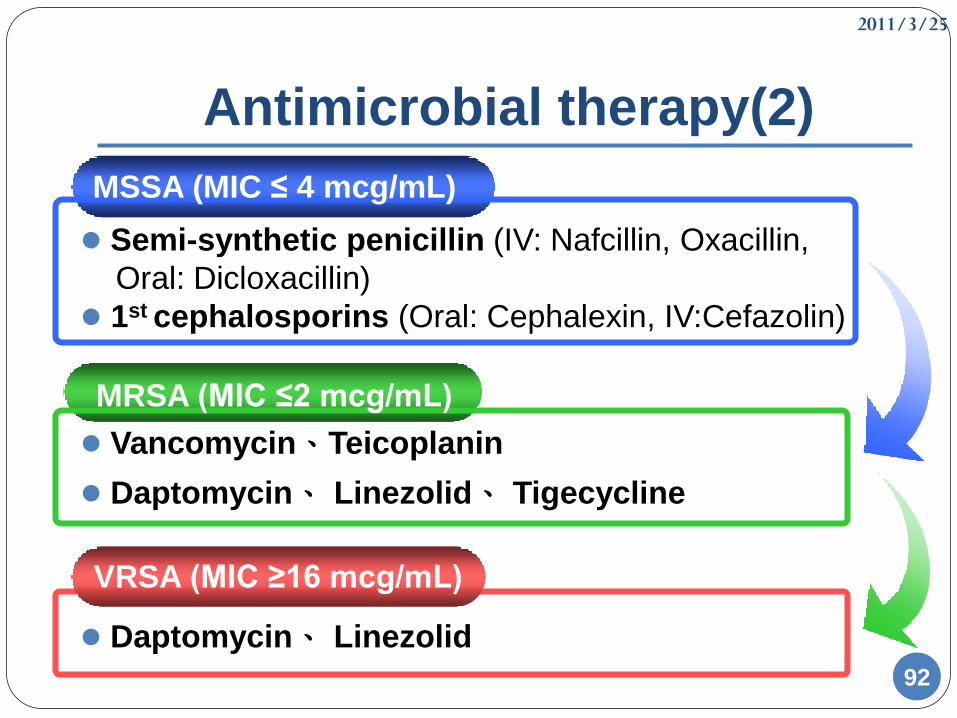
Antimicrobial therapy(2)
Daptomycin、 Linezolid
Vancomycin、Teicoplanin
Daptomycin、 Linezolid、 Tigecycline
MRSA (MIC ≤2 mcg/mL)
VRSA (MIC ≥16 mcg/mL)
Semi-synthetic penicillin (IV: Nafcillin, Oxacillin,
Oral: Dicloxacillin)
1st cephalosporins (Oral: Cephalexin, IV:Cefazolin)
MSSA (MIC ≤ 4 mcg/mL)
2011/3/25
93
Antibiotic dose with
hemodialysis patients
2011/3/25
94
Antibiotic dose with hemodialysis
patients(1)
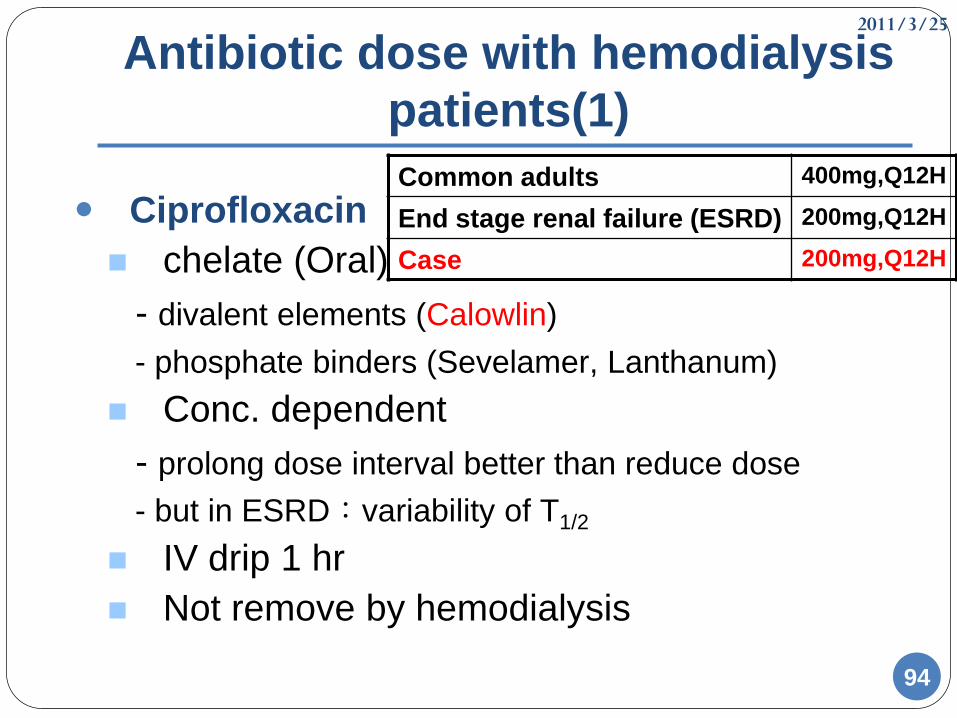
Ciprofloxacin
chelate (Oral)
- divalent elements (Calowlin)
- phosphate binders (Sevelamer, Lanthanum)
Conc. dependent
- prolong dose interval better than reduce dose
- but in ESRD:variability of T1/2
IV drip 1 hr
Not remove by hemodialysis
Common adults 400mg,Q12H
End stage renal failure (ESRD) 200mg,Q12H
Case 200mg,Q12H
2011/3/25
95
Antibiotic dose with hemodialysis
patients(2)
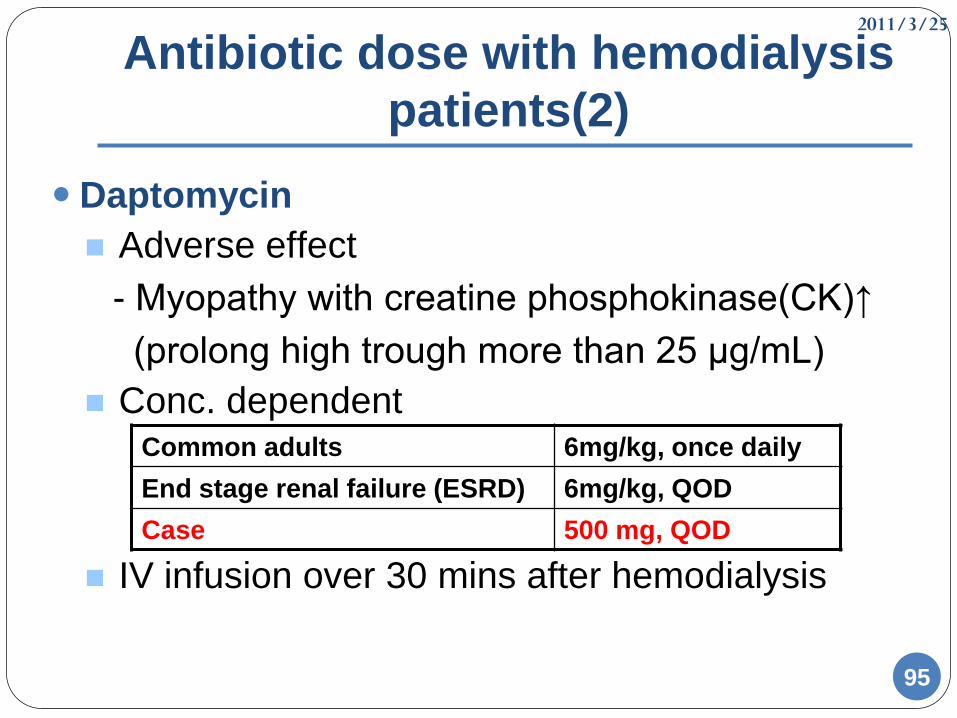
Daptomycin
Adverse effect
- Myopathy with creatine phosphokinase(CK)↑
(prolong high trough more than 25 μg/mL)
Conc. dependent
IV infusion over 30 mins after hemodialysis
Common adults 6mg/kg, once daily
End stage renal failure (ESRD) 6mg/kg, QOD
Case 500 mg, QOD
2011/3/25
96
Antibiotic dose with hemodialysis
patients(3)
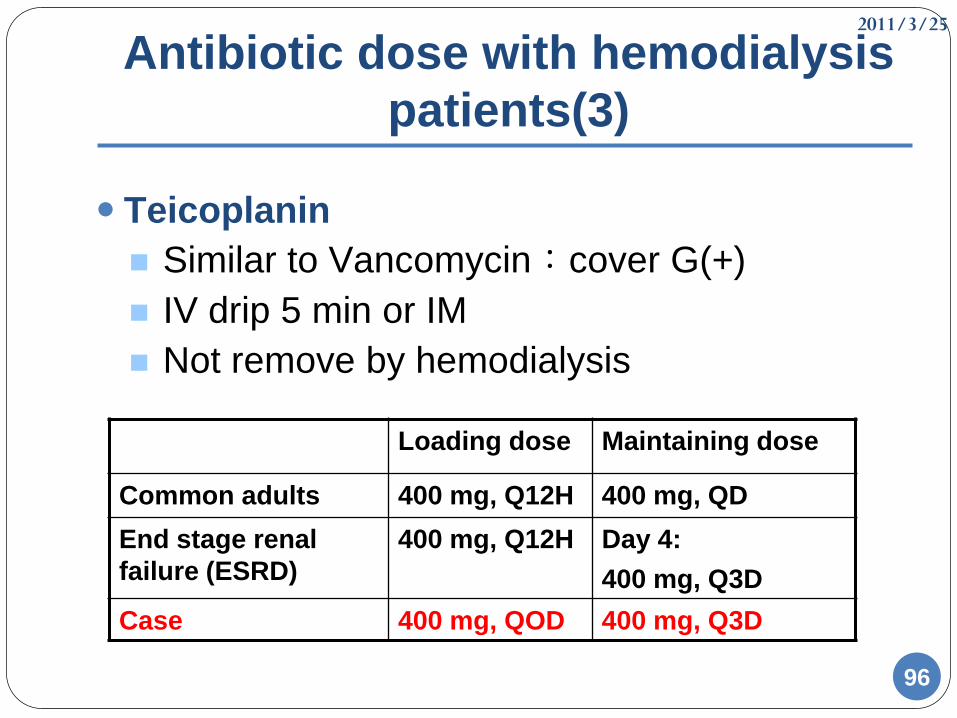
Teicoplanin
Similar to Vancomycin:cover G(+)
IV drip 5 min or IM
Not remove by hemodialysis
Loading dose Maintaining dose
Common adults 400 mg, Q12H 400 mg, QD
End stage renal
failure (ESRD)
400 mg, Q12H Day 4:
400 mg, Q3D
Case 400 mg, QOD 400 mg, Q3D
2011/3/25
97
Antibiotic dose with hemodialysis
patients(4)
Conclusion
Shift dose (standard dose reconsider)
- reach Pharmacodynamic targets
- attain Pharmacokinetic goals
Challenge
- advancing dialysis technology
→remove more drug than studies
Follow up outcome
2011/3/25
9898
References(1)
Applied Therapeutics: The clinical use of drug, 2009, 9th.
Chapter 56
Pharmacotherapy: a pathophysiologic approach, 2008,7th.
Chapter108 &109
Epidemiology of methicillin-resistant Staphylococcus aureus
infection in adults, John M Boyce, Daniel J Sexton, Elinor L Baron, MD,
DTMH, 2010 Form UPTODATE
Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of Methicillin-Resistant Staphylococcus Aureus Infections in Adults and Children
Clinical Infectious Diseases Advance Access published January 4, 2011
References(2)
Antibiotic Pharmacokinetic and Pharmacodynamic
Considerations in Patients With Kidney Disease Rachel F.
Eyler and Bruce A. Mueller, 2010 by the National Kidney Foundation
Treatment of invasive methicillin-resistant
Staphylococcus aureus infections in adults Franklin D Lowy,
Daniel J Sexton, Elinor L Baron, 2010 Form UPTODATE
Tunneled, cuffed hemodialysis catheter-related
bacteremia Michael Allon, Daniel J Sexton, Jeffrey S Berns, Theodore
W Post, 2010 Form UPTODATE
Vancomycin-intermediate and vancomycin-resistant
Staphylococcus aureus infections Franklin D Lowy, Daniel J
Sexton, Elinor L Baron, 2010 Form UPTODATE
2011/3/25
100100
Thanks for your listening !
2011/3/25
101
Bacteremia
Vancomycin (AII)
Adult:15–20 mg/kg/dose IV q8–12 h
Pediatric:15 mg/kg/dose IV every 6 h
The addition of gentamicin (AII) or rifampin (AI) to
vancomycin is not routinely recommended.
Daptomycin (AI/CIII)
Adult:6 mg/kg/dose IV QD
Pediatric:6–10 mg/kg/dose IV QD
For adult patients, some experts recommend higher
dosages of 8–10 mg/kg/dose IV QD (BIII).
2011/3/25
102102
Perm catheter AV fistula