proximal humerus fractures
TRANSCRIPT

Proximal fracture # of the &
humersfracture of humeral shaft


ANATOMY OF HUMERUS



VASCULAR SUPPLY

NERVE SUPPLY



SITES
Common))-surgical neck
-anatomical neck
-both tubercities

CLINICAL PICTURE:
# History
# Symptoms Upper extremity held closed to the chest by
contra lat.hand.
Pain,swelling,crepitus, painfull
# signs:
look
palpation
moove
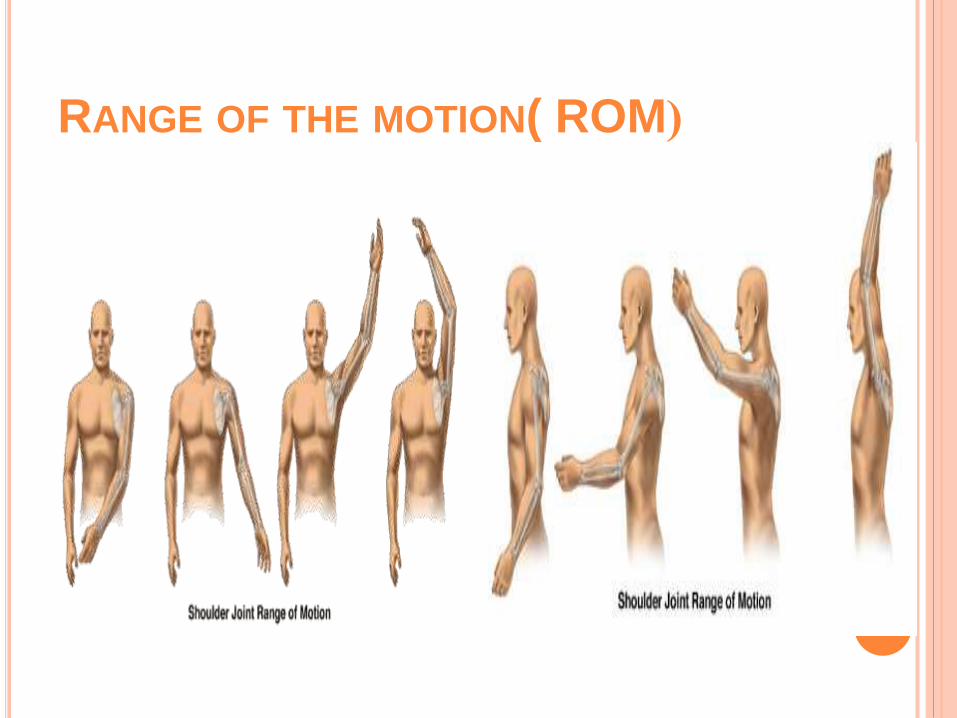
(RANGE OF THE MOTION( ROM

FLEXION 180
ABDUCTION 180
ADDUCTION 75
EXTENTION 50
ETERNAL ROTATION 65
INTERNAL ROTATION 90

CLASSIFICATION
KOCHERS;-based on different anatomic levels.
Anatomic neck
Epiphyseal region
Surgical neck.
Did not included #s at multiple level, degree of displacement, dislocations, mechanism.
Watson Jones-contusion crack #s.
Impacted #s.
Impacted abducted#s.
Codmann”s based on epiphyseal region-identifies four possible #s GT ,LT ,anatomic head, shaft

CLASSIFICATION:
NEER’S CLASSIFICATION
(5-TYPE) THE MOST COMMONLY USED CLASSIFICATION SYSTEM FOR PROXIMAL
HUMERAL
HEAD FRACTURES WAS DEVELOPED IN 1970 BY DR CHARLES NEER.
THE BASIS OF THE SYSTEM ACCORDING TO
1-DISPLACEMENT
2-ANATOMICAL LINES OF EPIPHYSEAL UNION,
INCLUDING THE
HUMERAL HEAD, GREATER TUBEROSITY
, LESSER TUBEROSITY, AND THE SHAFT (SURGICAL NECK).

NEER’S CLASSIFICATION
Displacement defined as greater than 45 degrees of
angulation or 1 cm of separation.
1-One part fracture – No displacement or angulation less than 45 degrees or seperationless than 1cm2-Two part fracture – Displacement of one fragment3-Three part fracture – Displacement of twoindividual fragments from remaining humerus4-Four part fracture – Displacement of all foursegments5-there is dislocation (anterior or posterior ) regardless number of displaced segment








DIAGNOSIS:
CLINICAL PRESENTATION :
> history of trauma
> pain during movement> Large bruise in the upper part of the arm
> Swelling and delayed ecchymosis >Tenderness to palpation> clear deformity
> Signs of axillary nerve or brachial plexus injury
> Crepitus indicative of fracture instability

RADIOLOGY
X-ray1- AP views
2- lat views.
3-axillary views(. Axillary andscapular-lateral views should always be obtained, toexclude dislocation of the shoulder)).
MRI
• CT Scan– articular fractures
• impression
• head split
– glenoid fractures
– assess tuberosity
displacement for
operative decision
making
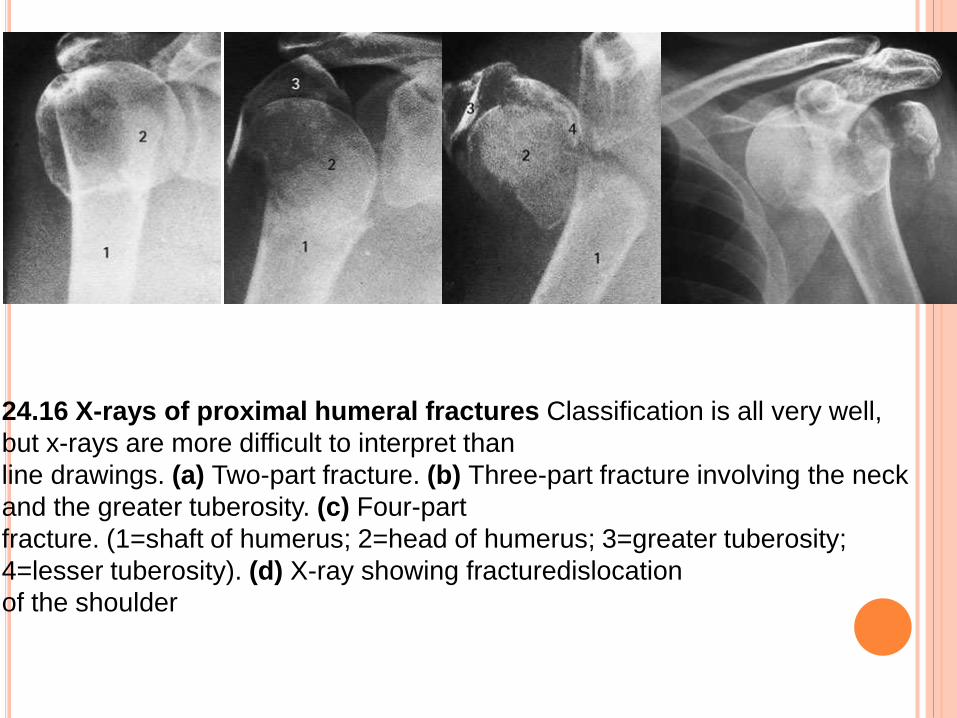
24.16 X-rays of proximal humeral fractures Classification is all very well,
but x-rays are more difficult to interpret than
line drawings. (a) Two-part fracture. (b) Three-part fracture involving the neck
and the greater tuberosity. (c) Four-part
fracture. (1=shaft of humerus; 2=head of humerus; 3=greater tuberosity;
4=lesser tuberosity). (d) X-ray showing fracturedislocation
of the shoulder
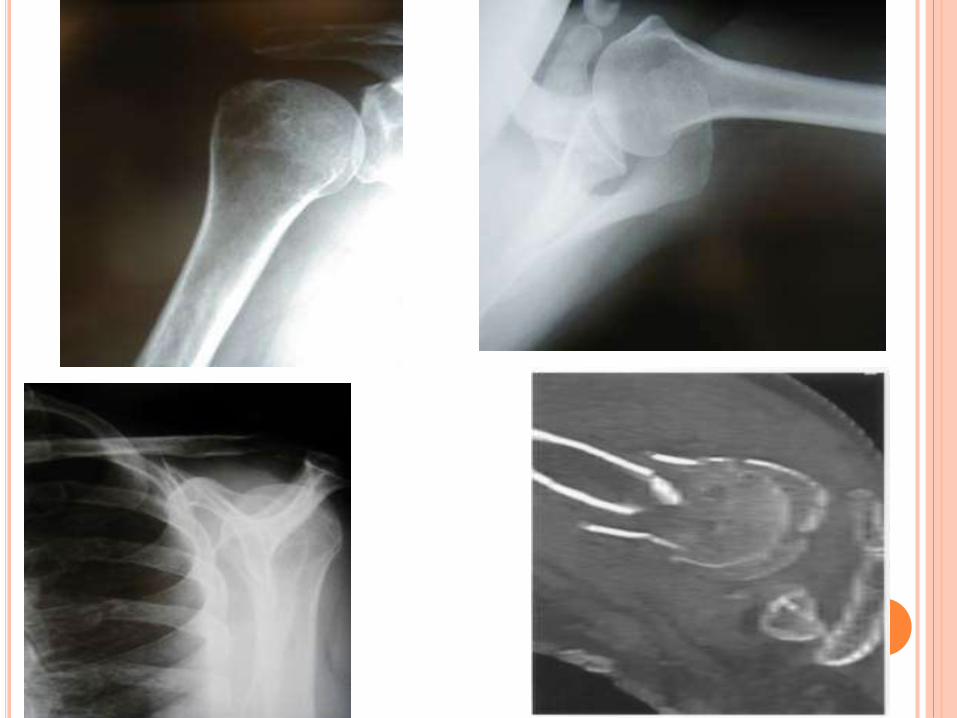

CT SCAN
The advent of 3D CT
reconstruction
has helped to reduce
the degree of inter-
and intra-observer
error, enabling better
planning of treatment
than in the past. CT with three-dimensional reconstruction
Advanced imaging provides a much clearer
picture of the injury, allowing better pre-operative
planning.

TREATMENT
1-One part fracture These comprise the vast
majority. They need no
treatment apart from a week
or two period of rest with the
arm in a sling until the pain
subsides, and then gentle
passive movements of the shoulder. Once the fracture has
united (usually after 6 weeks), active exercises are encouraged;
the hand is, of course, actively exercised from the start.
2-TWO PART FRACTURE
STABLE Closed reduction then sling for about
four weeks or until the fracture feels stable and the
x-ray shows some signs of
healing. Elbow and hand exercises are encouraged
throughout this period; shoulder exercises are
commenced at about four weeks.
if the fracture cannot be reduced closed or if the
fracture is very unstable after closed reduction,
then external fixation is Required Options
.include percutaneous pins, bone sutures,
intramedullary pins

3-THREE PART FRACTURE
4-Four part fracture
5-there is dislocation
they are extremely difficult to reduce closed.
In active individuals this injury is best
managed by open reduction and internal
fixation.


Proximal humerus fractures – treatment
(a) Three-part fracture, treated by
(b) locked nail fixation.
(c) Four-part fracture fixed with a locked plate; the intra-operative
picture
(d) shows how the plate was positioned

INTRA-MEDULLARY K WIRE FIXATION


COMPLICATIONS:
Early complication:
*Rotator cuff syndrom
* Vascular injury .
* Nerve injury.
* Biceps tendon
rupture
* Thoracic injury
late complication:
•* stiffness of the
shoulder.
* malunion.
* infection
* Avascular
necrosis.


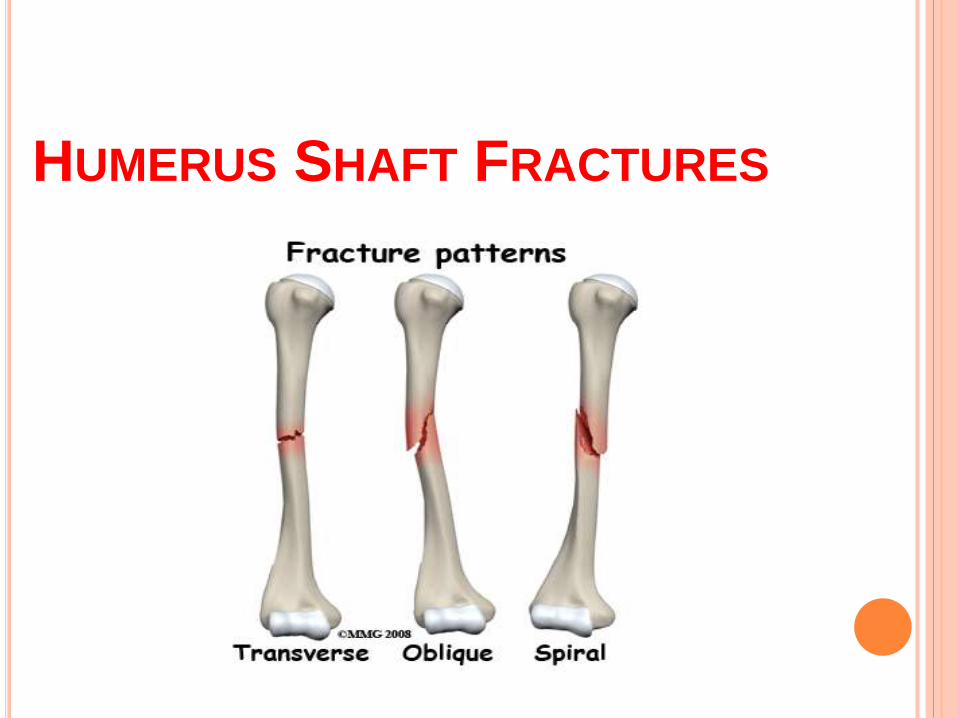
HUMERUS SHAFT FRACTURES

THE HUMERUS IS THE LONG,
TUBULAR BONE THAT MAKES UP THE
UPPER ARM. THE HUMERAL SHAFT IS
THE MIDDLE PORTION OF THE BONE
WITH THE SHOULDER JOINT AT THE
TOP END AND THE ELBOW JOINT AT
THE BOTTOM. ONE OF THE NERVES
THAT TRAVELS FROM THE NECK TO
THE HAND, THE RADIAL NERVE,
SPIRALS AROUND THE HUMERAL
SHAFT LYING VERY CLOSE TO THE
BONE ABOUT TWO THIRDS OF THE
WAY TO THE ELBOW. FRACTURES OF
THE HUMERAL SHAFT ARE IMPORTANT
BECAUSE THEY CAN INJURE THE
RADIAL NERVE RESULTING IN THE
INABILITY TO EXTEND (BEND) THE
WRIST AND FINGERS BACKWARDS

ANATOMY

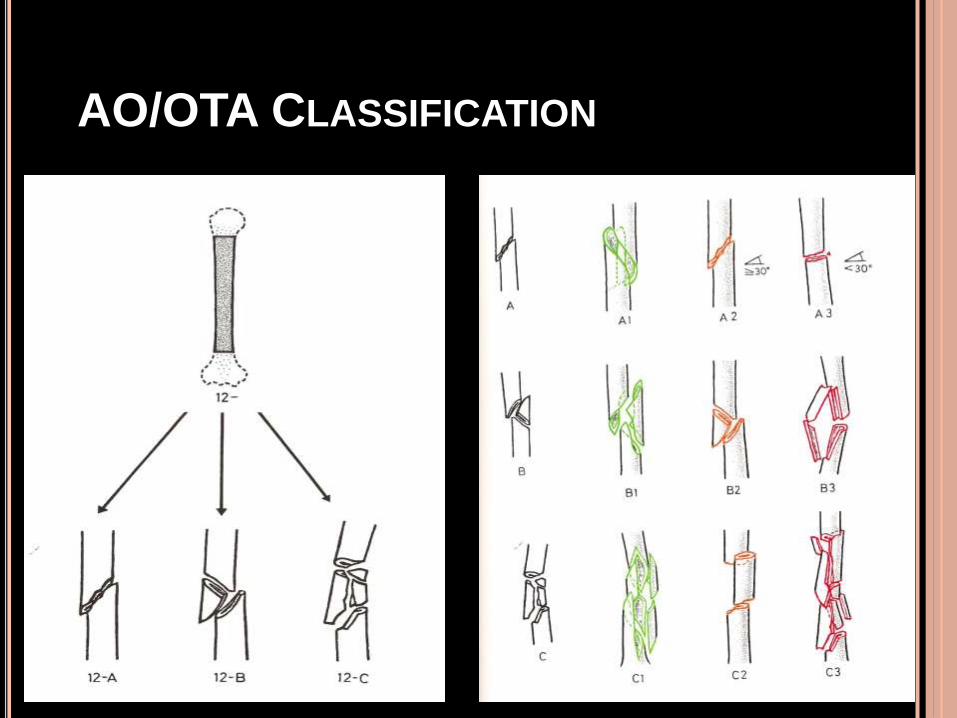
AO/OTA CLASSIFICATION

CLINICAL:

DIAGNOSIS

TETMENT


INDICATIONS FOR ORIF -
INJURY FACTORS
Failed closed treatment
Loss of reduction
Poor patient tolerance/compliance
(Open fractures)
Vascular injury/
Change in neuro exam (radial n.)
Floating elbow





COMPLICATIONS OF HUMERAL
SHAFT FRACTURES
Radial nerve injury
Vascular injury
Nonunion



COMLICATION

