repair of aortic dissection of the arch and branches chang shu m.d., phd. dept. of vascular surgery,...
TRANSCRIPT

Repair of Aortic Dissection of
the Arch and Branches
Repair of Aortic Dissection of
the Arch and Branches
Chang Shu M.D., PhD.Chang Shu M.D., PhD.
Dept. of Vascular Surgery,The 2nd Xiang-Ya Hospital, Central-South University
中南大学湘雅二医院血管外科湖南省大血管疾病外科及微创介入诊疗中心
Email : [email protected]
Chang Shu M.D., PhD.Chang Shu M.D., PhD.
Dept. of Vascular Surgery,The 2nd Xiang-Ya Hospital, Central-South University
中南大学湘雅二医院血管外科湖南省大血管疾病外科及微创介入诊疗中心
Email : [email protected]
Clinical Materials
• 2002.7 ~ 2014.2,
• 958 cases with aortic dissection treated with TEVAR• Acute (<2w): 670 cases• Sub-acute and chronic (>2w): 264 cases
• Male: 627 / Female: 331
• age: 20-87; mean age: 51.1
• follow-up: 25.1±7.3 months

Techniques for aortic arch
Hybrid techniques: aorta - supra aortic branches RSA (RCCA) – LCCA RSA (RCCA) – LSA RSA (RCCA) – LCCA – LSA LCCA – LSA
Fenestrated stent-graft
Branched stent-graft
Chimney / double chimney technique

Hybrid technique
aorta - supra aortic branchesRSA (RCCA) – LCCARSA (RCCA) – LSA
RSA (RCCA) – LCCA – LSALCCA – LSA

Extra-anatomic bypass
• needs several operation incisions.
• post-operative anticoagulant treatment is needs.
• reliable/stable/durable outcome
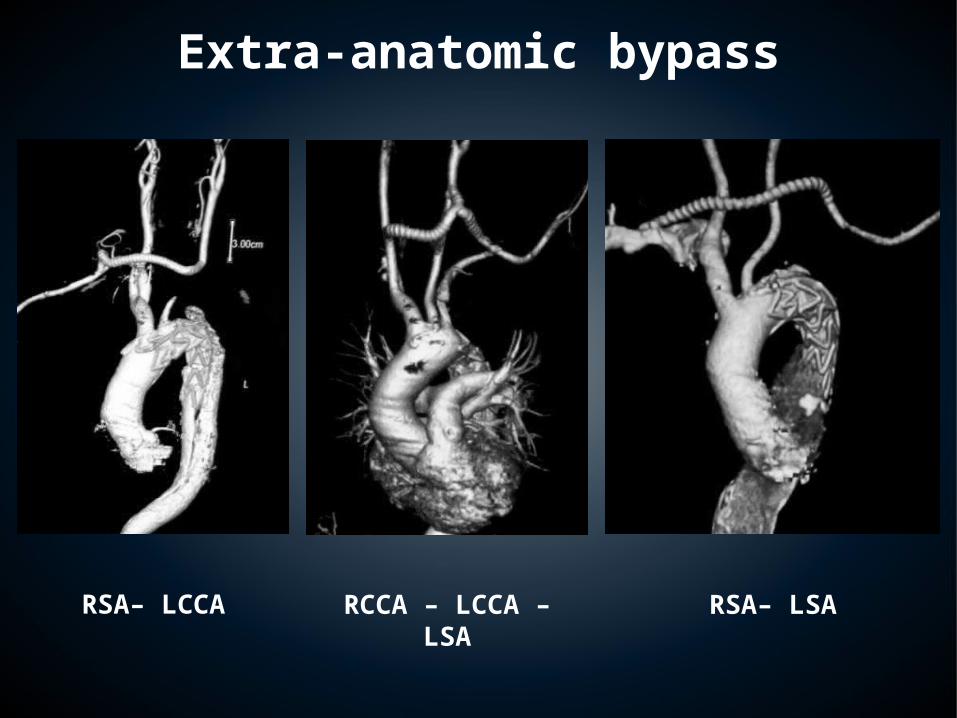
RCCA – LCCA – LSARSA– LCCA RSA– LSA
Extra-anatomic bypass
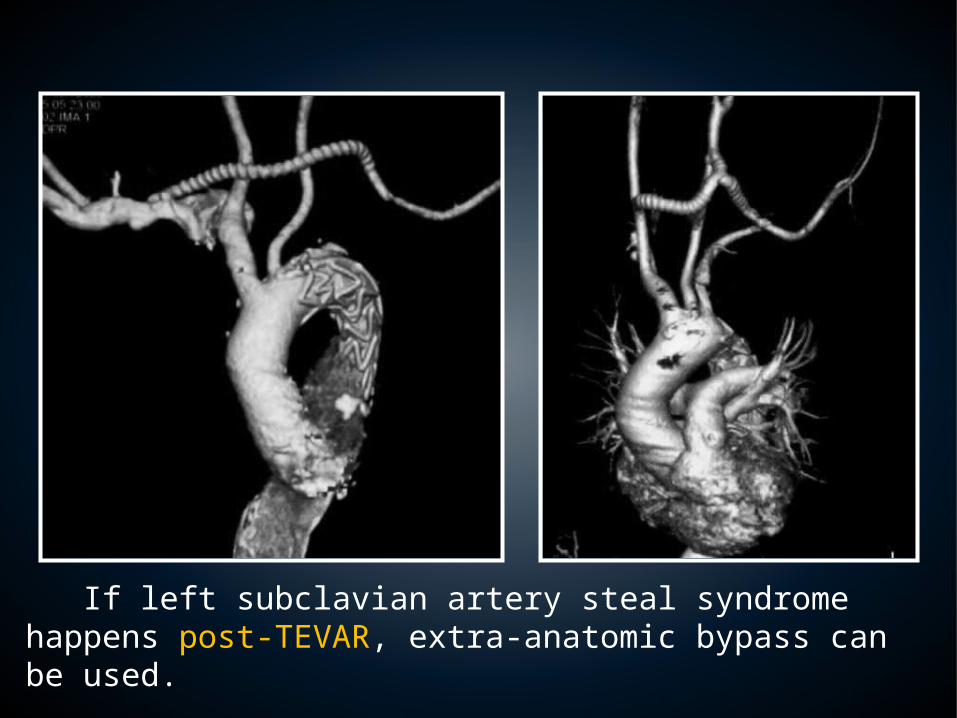
If left subclavian artery steal syndrome happens post-TEVAR, extra-anatomic bypass can be used.
Hybrid technique
aorta - supra aortic branchesRSA (RCCA) – LCCARSA (RCCA) – LSA
RSA (RCCA) – LCCA – LSALCCA – LSA

A man, 36y, suffered from an aortic arch pseudoaneurysm because of a severe traffic accident.

Hybrid technique was adopted.Ascending aorta – innominate artery – left carotid artery – LSA bypass was achieved first.

Hybrid technique was adopted.Then TEVAR was used. The patient recovered unevertfully.
fenestrated SG
Some of the stenting-grafts has been modified to fit the aortic arch area

Fenestration—treatment
• Step 1: CT and DSA for
accurate measurement were performed pre-operation.

Fenestration—treatment
• Step 2: deploy partial of the
proximal stent graft in vitro, and eliminate part of the lateral fabric.

Fenestration—treatmentFenestration—treatment
Step 3Step 3

Fenestration—follow up
The fenestrated stent graft covered the aortic arch dissection completely
With patent supra-aortic branches

Branched stent-graft
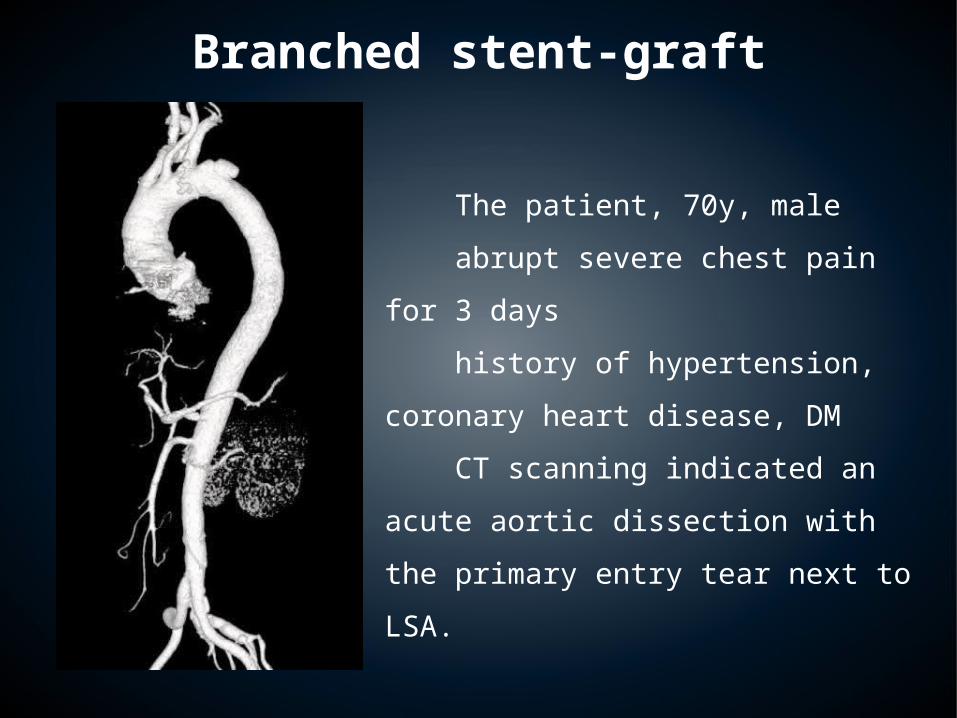
The patient, 70y, male
abrupt severe chest pain for 3
days
history of hypertension, coronary
heart disease, DM
CT scanning indicated an acute
aortic dissection with the primary
entry tear next to LSA.
Branched stent-graft


6 months later, CT
angiography indicated
excellent aortic remodeling
without any complications.
Blood stream of the
reconstructed LSA is fluent.
Branched stent-graft

Chimney technique
Has been applied from 2007.Used to treat the aortic arch disease.
A female, 49 years old, the aortic arch dissection related LSA. There was not enough proximal landing zone.
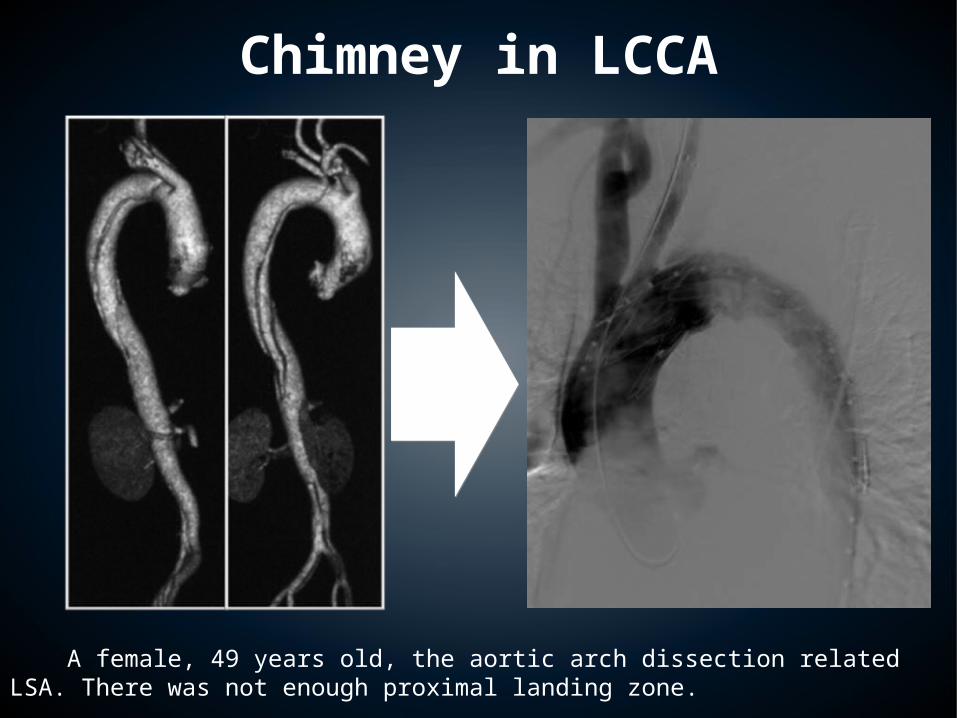
Chimney in LCCA
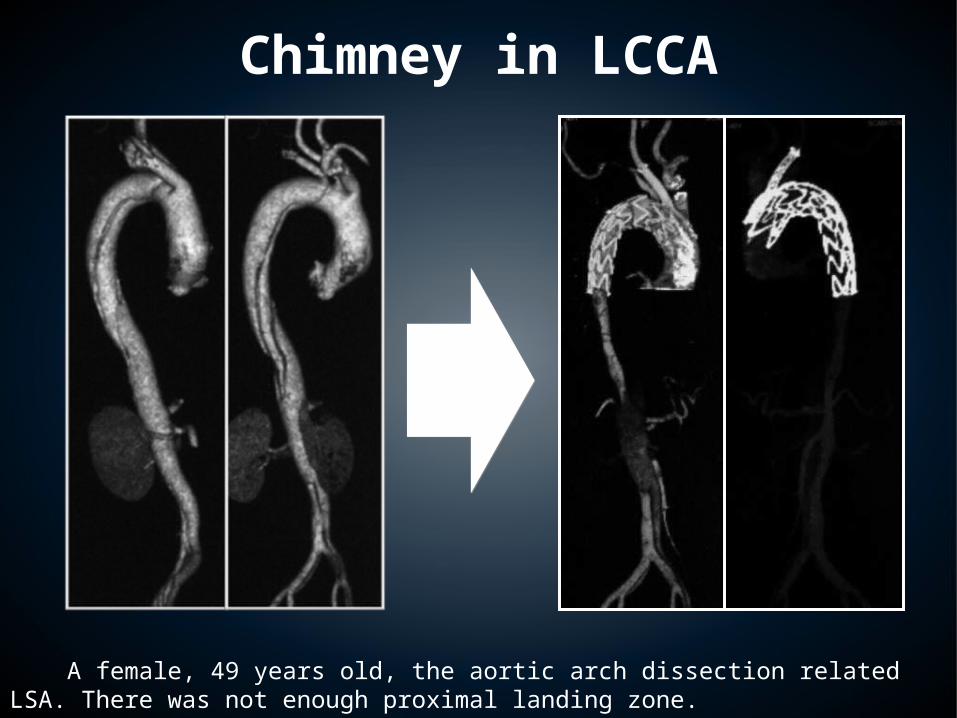
A female, 49 years old, the aortic arch dissection related LSA. There was not enough proximal landing zone.
Chimney in LCCA

the patient, 36y, male
suffered from abrupt chest pain
for 4 days.
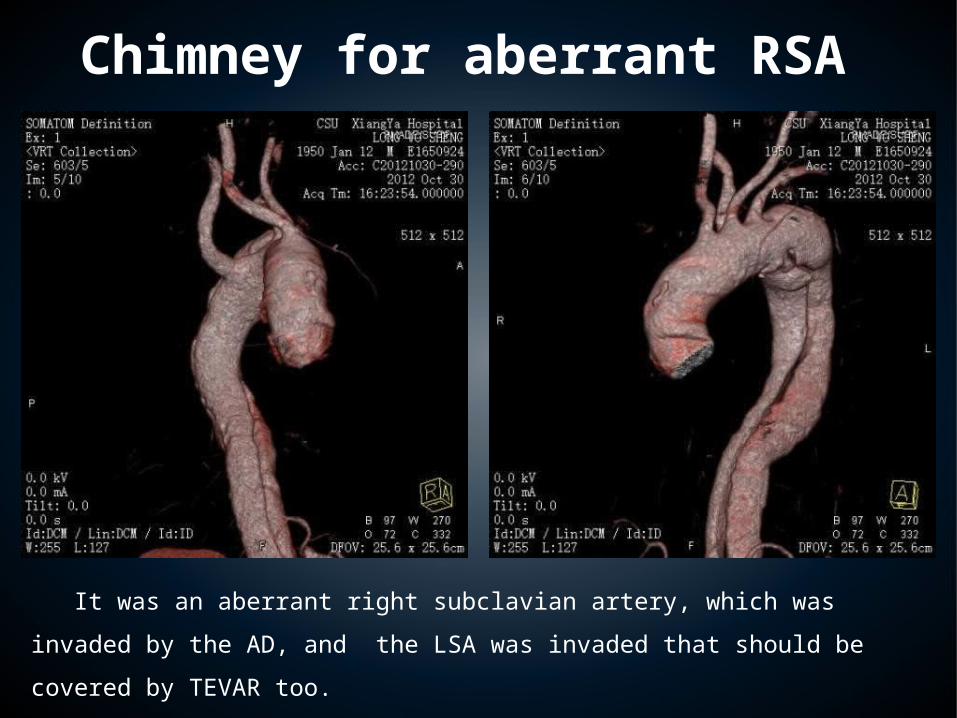
CT angiograph indicated a acute
type B aortic dissection and
aberrant right subclavian artery.
Chimney for aberrant RSA
Chimney for aberrant RSA
It was an aberrant right subclavian artery, which was invaded by the AD, and the
LSA was invaded that should be covered by TEVAR too.
So, chimney technique should be used to reconstruct the invaded LSA.

Chimney for aberrant RSA

Chimney for aberrant RSA

Chimney for aberrant RSA
The aberrant right subclavian
artery was covered. The LSA
reconstructed with a chimney
stent-graft was patent.

Chimney for type Ia endoleak
Chimney for type Ia endoleak

Chimney technique for AD + Marfan syndrome+ pregnancy

A female,29 years old, suffered from abrupt severe back pain 1 week after caesarean section.
The primary entry tear located at the orifice of the LSA ( white arrow ).
MFS associated with puerperal state

One month later, the patient recovered well without any symptoms.
However, CT angiography detected mild contrast in the false lumen, and the patent false lumen
communicated with LSA.
MFS associated with puerperal state

Chimney for MFS + puerperal state
• 13 months later, the patient recovered uneventfully.
• Endoleak disappeared ! • No migration, new entry tear formation.

Chimney technique+ PDA occlude for LSA
If chimney technique is used in the common carotid artery, the covered LSA has the risk of
type II endoleak. PDA occlude technique is a ideal management

• TBAD related LSA• Chimney technique should be used
Chimney technique+ PDA occlude


Chimney technique+ PDA occlude
Chimney technique+ PDA occlude

2 weeks after TEVAR, no type II endoleak lasted.

Double-chimney technique
Double-chimney technique can replace the conventional open surgery, and be used to
reconstruct all supra-aortic branches.

The patient suffer from an acute aortic dissection, which the left common carotid artery was invaded and leaded to severe carotid artery stenosis.
Double-Chimney Technique

Bi-chimney technique was used.
Two Fluency stent-grafts were used to reconstruct IA and LCCA. The LSA was covered.
The patient recovered well, without any complications.
Double Chimney Technique
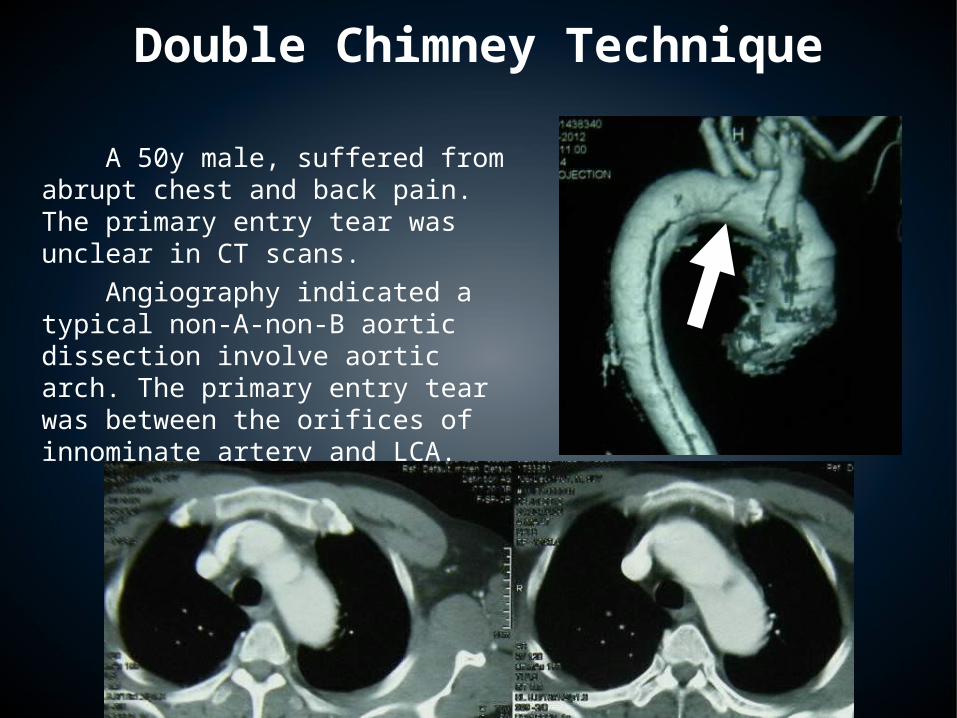
A 50y male, suffered from abrupt chest and back pain. The primary entry tear was unclear in CT scans. Angiography indicated a typical non-A-non-B aortic dissection involve aortic arch. The primary entry tear was between the orifices of innominate artery and LCA.
Double Chimney Technique


Double Chimney Technique

The patient recovered well, without any serious complications
Double Chimney Technique

Double-chimney technique
Double-chimney technique is an experimental technique, with some unclear complications.

Double Chimney Technique
It’s a patient with acute type B aortic dissection. According to the CT scan, it’s hard to distinguish the primary entry tear. So, we need DSA.

Double Chimney Technique

Double Chimney Technique
the primary entry tear is next to the orifice of left subclavian artery. The proximal landing zone is insufficient.

Double Chimney Technique
Double chimney technique could increase the proximal landing zone, extending to ascending aorta. During TEVAR, there was no complications. However, the vital signs during post-anesthesia recovery were unstable~~

Double Chimney Technique
After double chimney stent-graft deployed
30 min later, when we punctured brachial artery
and performed angiography again.
30 minobvious migration
30 minobvious migration

Double Chimney Technique
So, we inserted another two Fluency stent-grafts, overlapped with the previous two, to reconstruct innominate artery and left carotid artery. The patient recovered gradually.

Left subclavian artery dissected post-operation
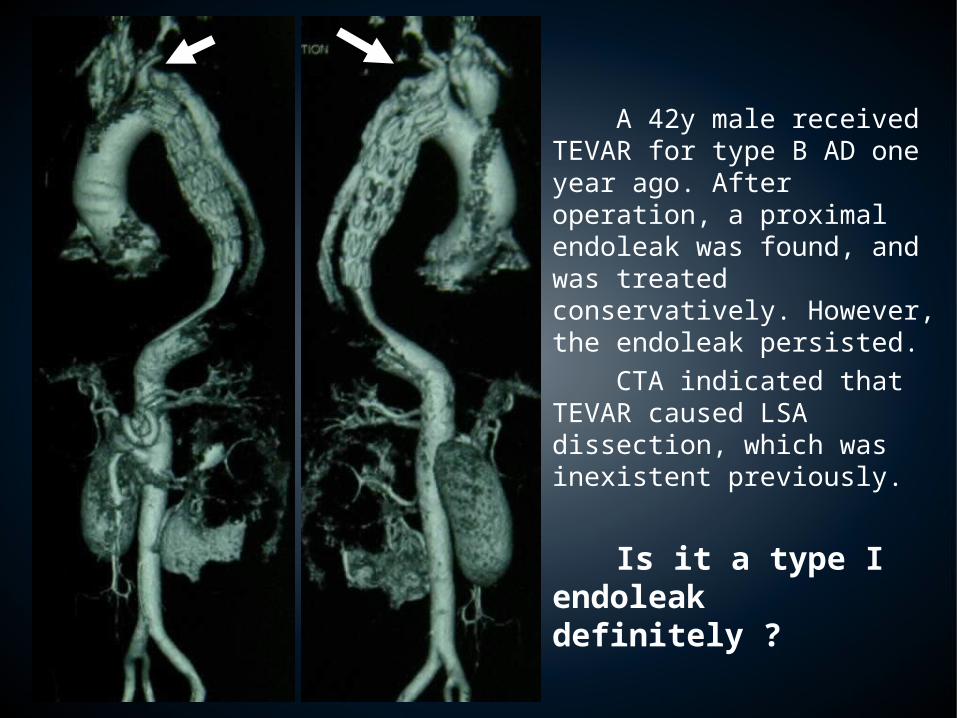
A 42y male received TEVAR for type B AD one year ago. After operation, a proximal endoleak was found, and was treated conservatively. However, the endoleak persisted. CTA indicated that TEVAR caused LSA dissection, which was inexistent previously.
Is it a type I endoleak definitely ?
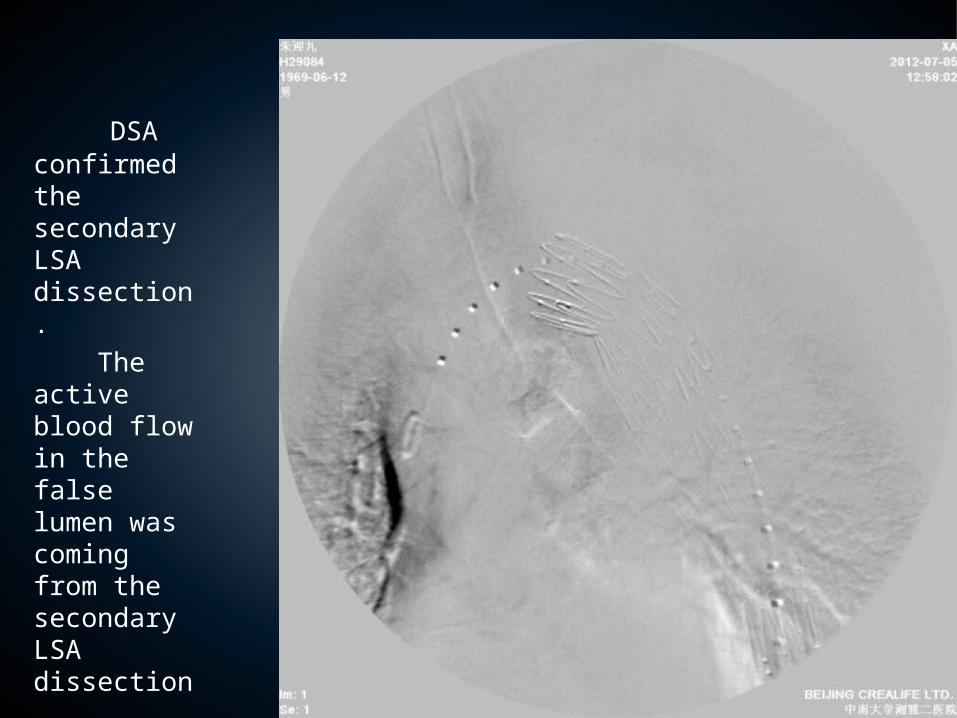
DSA confirmed the secondary LSA dissection. The active blood flow in the false lumen was coming from the secondary LSA dissection.

A balloon was inflated in the LSA and DSA was performed again.
It’s obviously that there is no type I endoleak, the active blood flow in the false lumen was originated from the secondary LSA dissection.
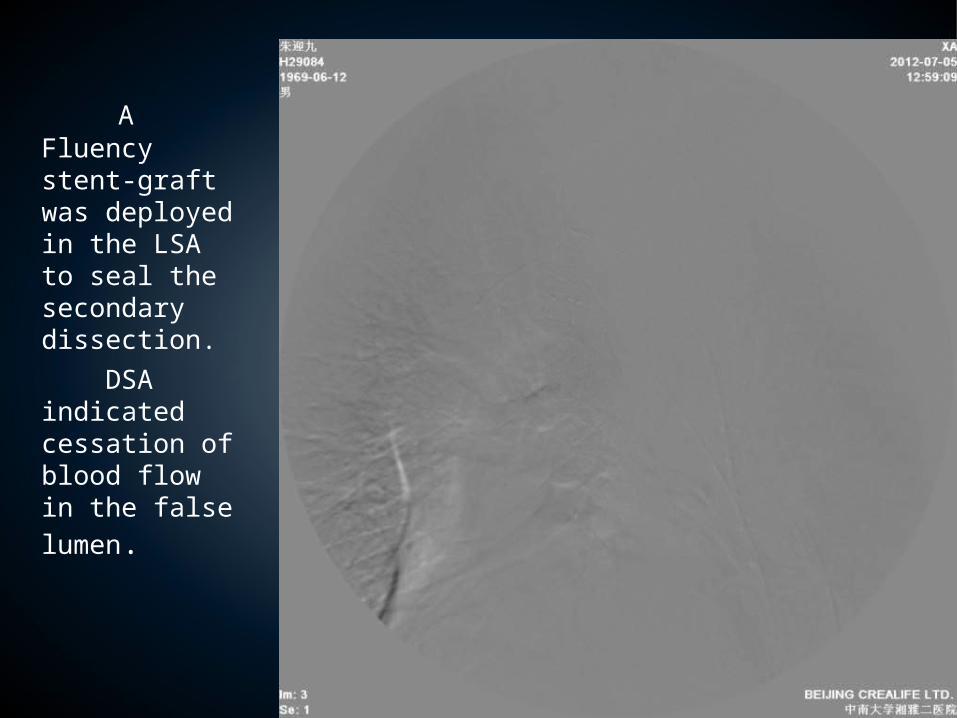
A Fluency stent-graft was deployed in the LSA to seal the secondary dissection.
DSA indicated cessation of blood flow in the false lumen.
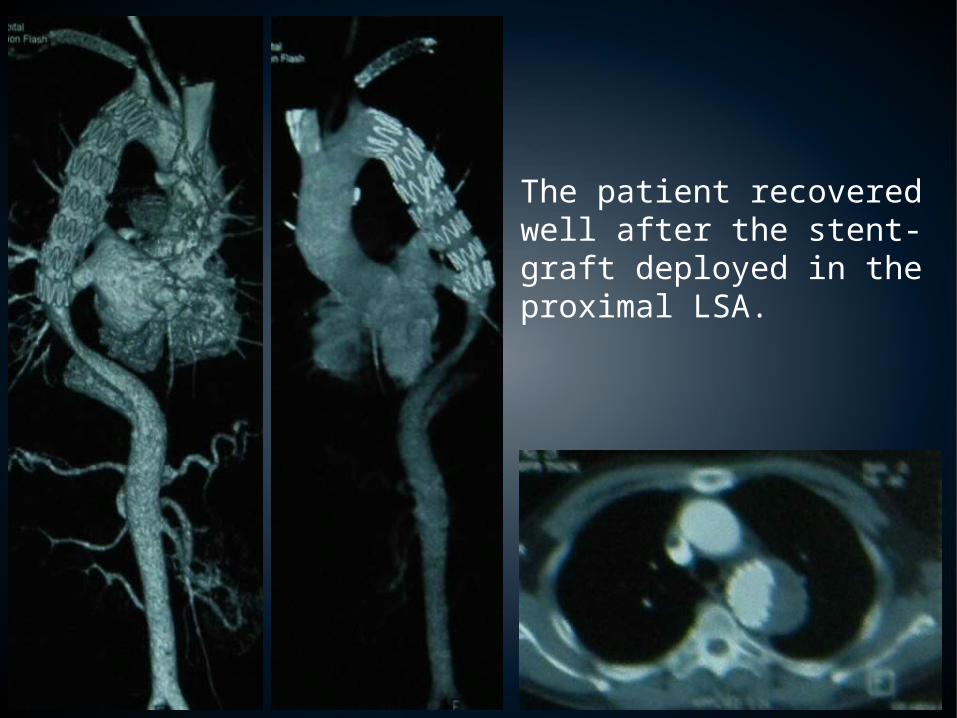
The patient recovered well after the stent-graft deployed in the proximal LSA.

Conclusions
1. The management of aortic arch diseases became popularity now.
2. Hybrid technique/fenestrated stent-graft/ branched stent-graft/ chimney technique are suitable.
3. Extra-anatomic bypass can be replaced by chimney technique.
4. Better technique is to be expected !

Thank u very much!