successes & challenges in development of drugs for children uspesi i izazovi u razvoju lekova za...
TRANSCRIPT
Successes & Challenges In Development Of Drugs For ChildrenUspesi i izazovi u razvoju lekova za decuSmiljana Milosavljević – Ristić MD PhD
Beograd, 28. Oktobar 2011
1
Content
• Historical Examples• Current situation– Modern drug development– Insufficient pediatric drug research– New legislations to stimulate pediatric drug development – Specific challenges in pediatric drug development
• Examples of Current Pediatric Drug Development– Avastin: identification of pediatric indications in oncology– Mircera: paediatric dose finding and long term safety study
• Conclusions
- 2 -
Historical example - Soothing syrup
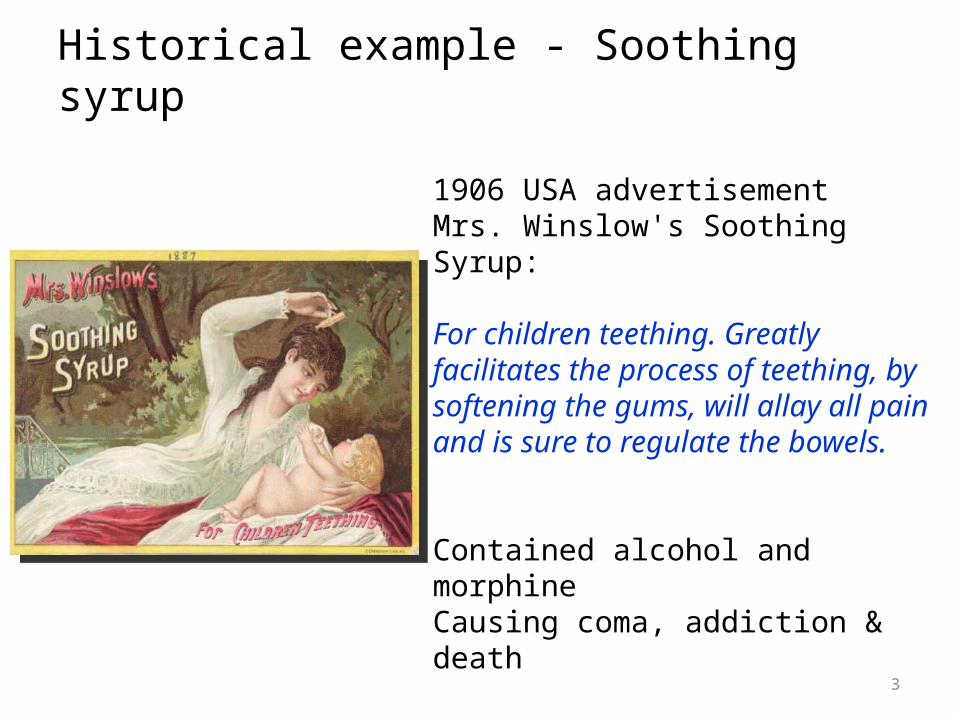
1906 USA advertisementMrs. Winslow's Soothing Syrup:
For children teething. Greatly facilitates the process of teething, by softening the gums, will allay all pain and is sure to regulate the bowels.
Contained alcohol and morphineCausing coma, addiction & death
3

Historical experience - Sulfanilamid
September 1937 in USASulfanilamidcompounded with an solvent, diethylene glycol (chemically related to antifreeze)
107 deaths including many children1938 Food and Drug Act: firms had to prove that any new drug was safe before it could be marketed
4

Historical example - Talidomide
• 1960 a New Drug Application in USA, drug approved in Europe
• FDA felt data were incomplete to support the safety
• 10 000 children in 46 countries born with birth defects (phocomelia)
5

Modern Drug Development and Approval
Pediatric Drug Development:Changing Paradigm
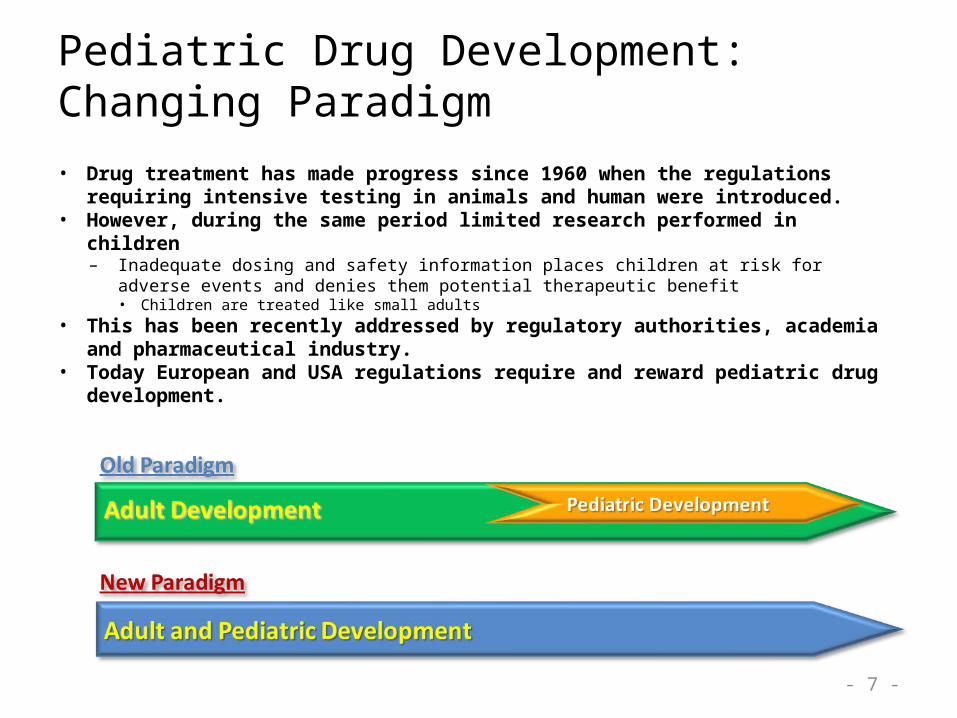
• Drug treatment has made progress since 1960 when the regulations requiring intensive testing in animals and human were introduced.
• However, during the same period limited research performed in children– Inadequate dosing and safety information places children at risk for adverse events and denies
them potential therapeutic benefit • Children are treated like small adults
• This has been recently addressed by regulatory authorities, academia and pharmaceutical industry.
• Today European and USA regulations require and reward pediatric drug development.
- 7 -

EU Pediatric Regulation in 2006
REQUIREMENTS
Pediatric Investigation Plan (PIP) to be approved by EU Pediatric Committee– Condition for the submission of
the new drug dossier–Compliance check at submission
validation
INCENTIVES
For drugs with patent – Six-month patent extension
8
International Recommendations on Timing of Pediatric Drug Development - ICH E 11
• Medicinal products for diseases predominantly affecting children– Development in children only, e.g. lung surfactant
• Drugs for serious or life-threatening diseases, occurring in both adults and children with limited therapeutic options – Pediatric development should begin early with initial
safety/efficacy evidence. e.g. antibiotics, antivirals• Medicinal products for other diseases and conditions – Less urgent in children, start development in phase IIIb/IV, e.g.
osteoporosis, lipid lowering drugs

10
Use Of Pre-clinical (Animal) Research For Pediatric Drug Development
• Adult drug development includes reproductive toxicology and carcinogenicity studies
• Postnatal developmental toxicity can be addressed in juvenile animal studies
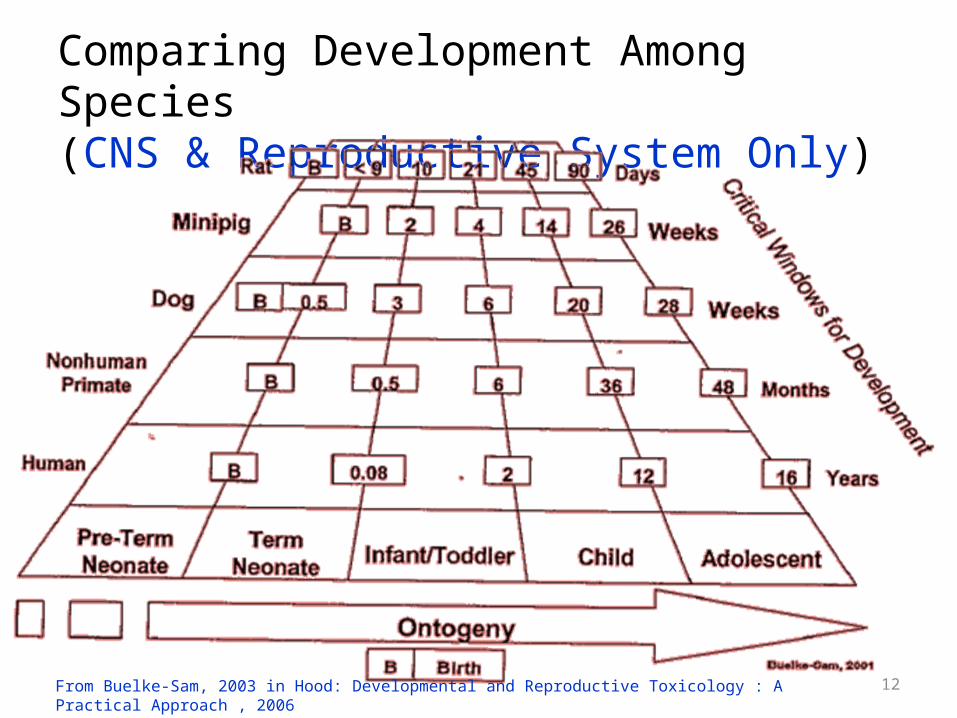
Comparing Development Among Species (CNS & Reproductive System Only)
12From Buelke-Sam, 2003 in Hood: Developmental and Reproductive Toxicology : A Practical Approach , 2006
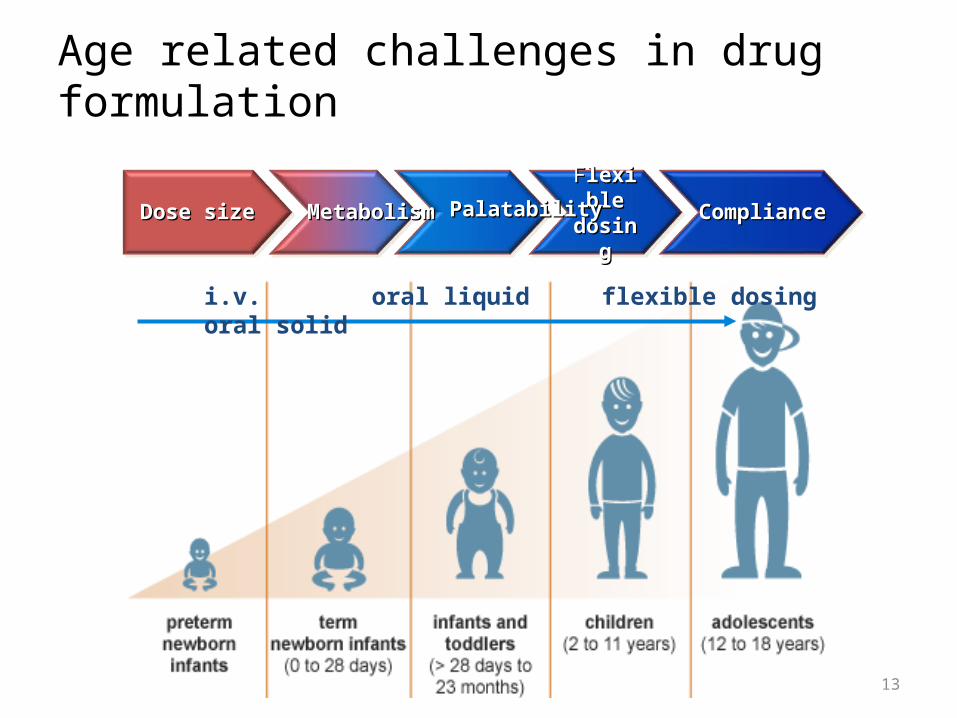
Age related challenges in drug formulation
13
Dose sizeDose size ComplianceComplianceFFlexiblelexibledosingdosing
i.v. oral liquid flexible dosing oral solid
MetabolismMetabolism PalatabilityPalatability

Challenges in pediatric drug formulation
Oral liquid or powder for reconstitution are preferred for children <6 yrs.•may be difficult to develop: stability, taste masking•not preferred for developing countries
14
Clinical trials in children are more difficult and more expensive
• Informed Consent – Assent from children 6-13 years and adolescents– Consent from the legal representative
• Limited use of placebo– Only if no approved therapies
• Limited population – Lower incidence of diseases, need to study different age groups
• Specific efficacy and safety measurements– Children not able to perform (spirometry)
• Minimal invasiveness of examinations – number & volume of blood samples
• Child and family friendly research facilities
Avastin:Pediatric drug development in oncologyBernie & Herby studies
- 16 -
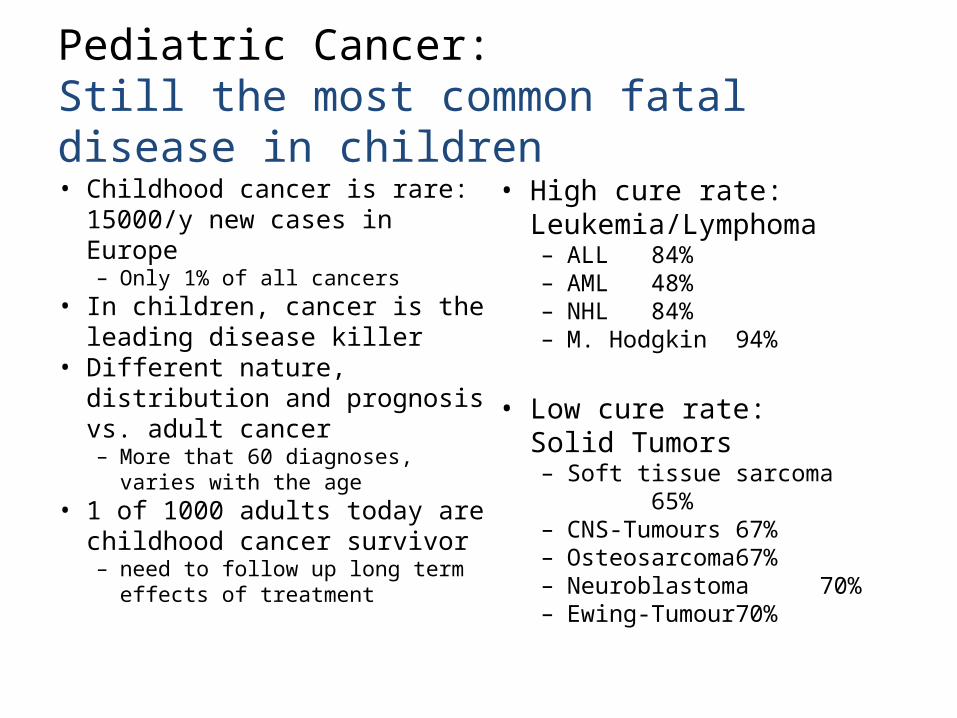
Pediatric Cancer:Still the most common fatal disease in children
• Childhood cancer is rare: 15000/y new cases in Europe – Only 1% of all cancers
• In children, cancer is the leading disease killer
• Different nature, distribution and prognosis vs. adult cancer– More that 60 diagnoses, varies
with the age• 1 of 1000 adults today are
childhood cancer survivor– need to follow up long term
effects of treatment
• High cure rate: Leukemia/Lymphoma– ALL 84%– AML 48%– NHL 84%– M. Hodgkin 94%
• Low cure rate:Solid Tumors– Soft tissue sarcoma 65% – CNS-Tumours 67%– Osteosarcoma 67% – Neuroblastoma 70%– Ewing-Tumour 70%
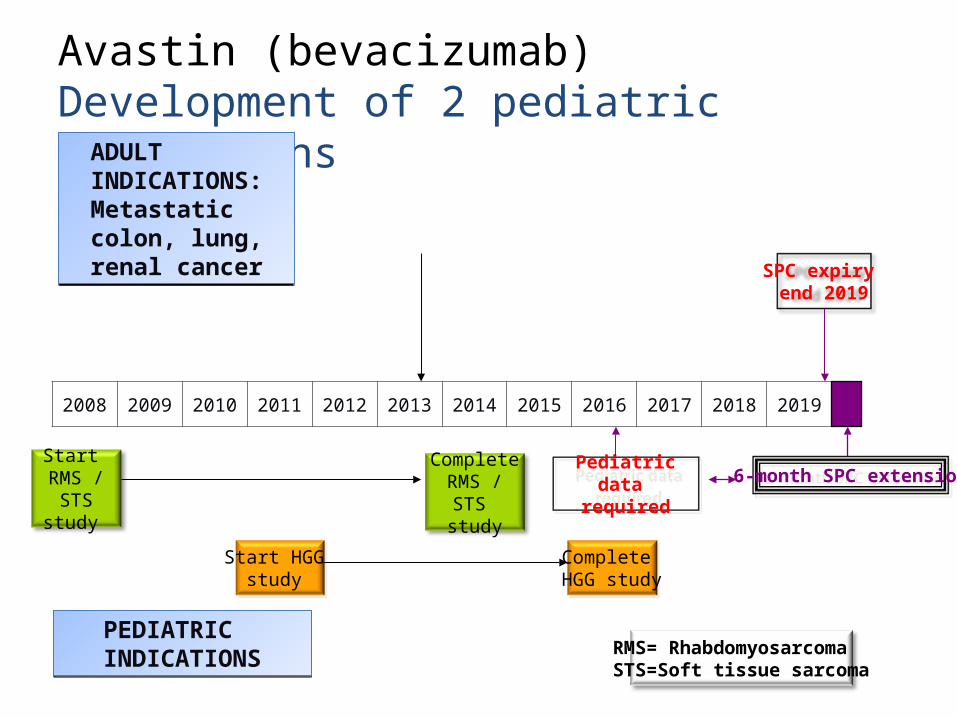
Avastin (bevacizumab)Development of 2 pediatric indications
ADULT INDICATIONS:Metastatic colon, lung, renal cancer
ADULT INDICATIONS:Metastatic colon, lung, renal cancer
RMS= RhabdomyosarcomaSTS=Soft tissue sarcoma
SPC expiry end 2019
Start RMS / STS
study
CompleteRMS / STS
study
PEDIATRIC INDICATIONSPEDIATRIC INDICATIONS
Pediatric data required
2008
20092010
2011 2012 20132014
2015 20162017
20182019
Start HGG study
Complete HGG study
6-month SPC extension
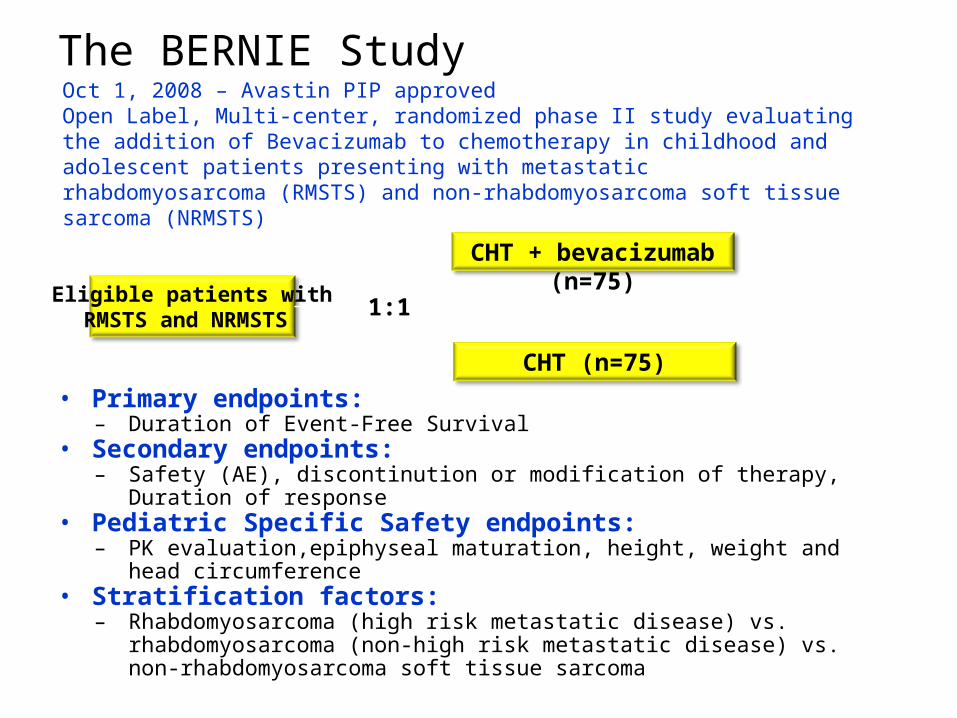
The BERNIE Study
• Primary endpoints: – Duration of Event-Free Survival
• Secondary endpoints: – Safety (AE), discontinution or modification of therapy, Duration of response
• Pediatric Specific Safety endpoints:– PK evaluation,epiphyseal maturation, height, weight and head circumference
• Stratification factors: – Rhabdomyosarcoma (high risk metastatic disease) vs. rhabdomyosarcoma (non-
high risk metastatic disease) vs. non-rhabdomyosarcoma soft tissue sarcoma
Eligible patients withRMSTS and NRMSTS
CHT + bevacizumab (n=75)
CHT (n=75)
1:1
Oct 1, 2008 – Avastin PIP approvedOpen Label, Multi-center, randomized phase II study evaluating the addition of Bevacizumab to chemotherapy in childhood and adolescent patients presenting with metastatic rhabdomyosarcoma (RMSTS) and non-rhabdomyosarcoma soft tissue sarcoma (NRMSTS)
The Herby Study: High Grade Glioma (HGG) Research of Bevacizumab in children&adolescents
• 2009: accelerated approval for the treatment in adults with glioblastoma muliforme (GBM)
• Pediatric unmet medical need • Applicability to pediatric glial tumors?– Differences in biology between pediatric and adult glial tumors?• Molecular and chromosomal characteristics• Lower frequency of EGFR amplification or overexpression
– Effects of bevacizumab on child’s growth/development• Effects on post-natal bone growth and development• Bevacizumab distribution and metabolism
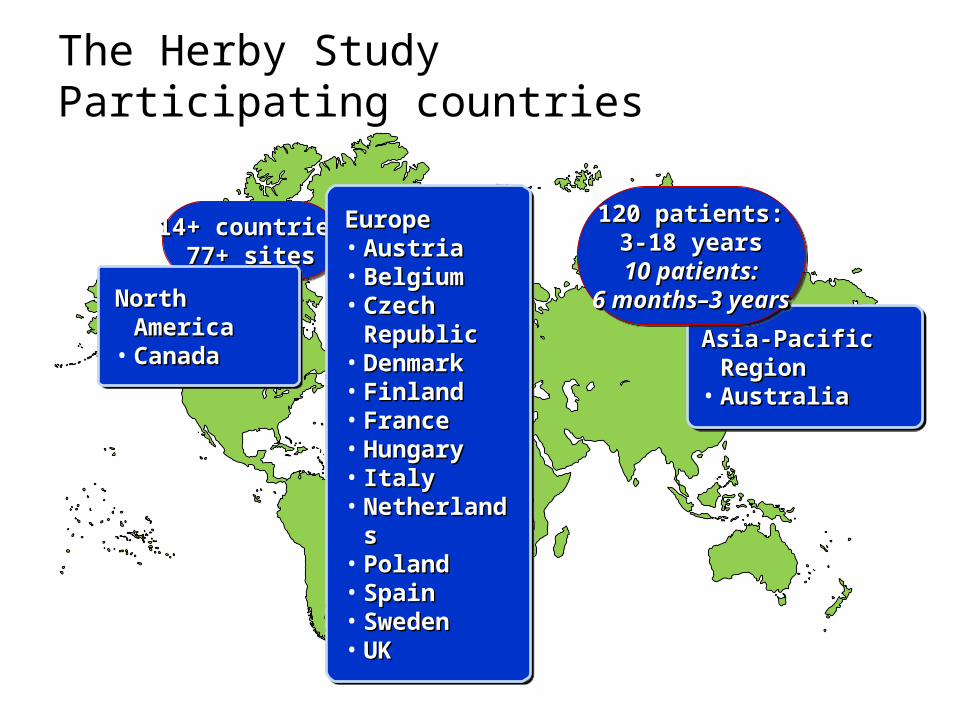
The Herby StudyParticipating countries
14+ countries14+ countries77+ sites77+ sites
14+ countries14+ countries77+ sites77+ sites
North AmericaNorth America• CanadaCanadaNorth AmericaNorth America• CanadaCanada
EuropeEurope• AustriaAustria• BelgiumBelgium• Czech Republic Czech Republic • DenmarkDenmark• FinlandFinland• FranceFrance• HungaryHungary• ItalyItaly• NetherlandsNetherlands• PolandPoland• SpainSpain• SwedenSweden• UKUK
EuropeEurope• AustriaAustria• BelgiumBelgium• Czech Republic Czech Republic • DenmarkDenmark• FinlandFinland• FranceFrance• HungaryHungary• ItalyItaly• NetherlandsNetherlands• PolandPoland• SpainSpain• SwedenSweden• UKUK
Asia-Pacific RegionAsia-Pacific Region• AustraliaAustraliaAsia-Pacific RegionAsia-Pacific Region• AustraliaAustralia
120 patients:120 patients:3-18 years3-18 years
10 patients:10 patients:6 months–3 years6 months–3 years
120 patients:120 patients:3-18 years3-18 years
10 patients:10 patients:6 months–3 years6 months–3 years

The Herby StudyStudy population
• Children…– Between the age of 3 and 18 years – With newly diagnosed histologically documented HGG– Localised supratentorial non-brainstem HGG – WHO Grade III or IV – Confirmed by an independent reference neuro-pathologist• Before randomization, to avoid inclusion of low grade glioma
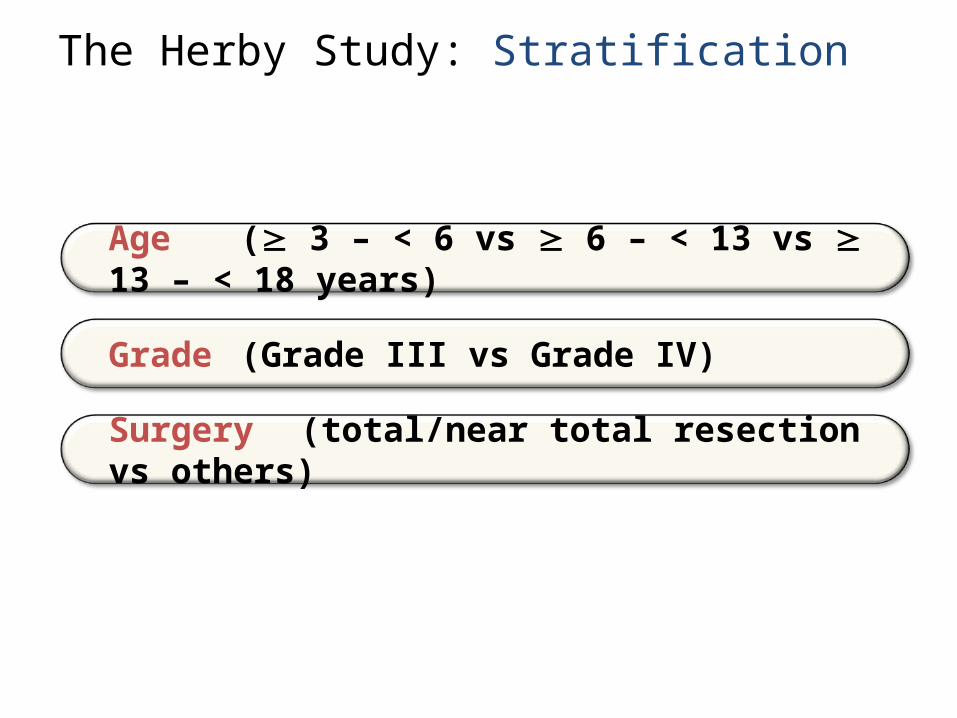
The Herby Study: Stratification
Age ( 3 – < 6 vs 6 – < 13 vs 13 – < 18 years)
Grade (Grade III vs Grade IV)
Surgery (total/near total resection vs others)
The Herby Study Efficacy outcome measures
• Primary Endpoint– Event-Free Survival (EFS)
• Secondary Endpoints– Overall Survival (OS) and 1-year OS– 6-month and 1-year EFS
• Exploratory Endpoints– Health status measured by the health utility index– IQ measured by Wechsler scale adapted to age – Multimodal imaging
- 25 -
Mircera:Development of pediatric indication for maintenance treatment of anemia in chronic kidney disease on hemodialysis with long terms safety extension

Mircera:Pediatric drug development for treatment of anemia in chronic kidney disease on hemodialysis
• Children with end-stage renal disease represent small proportion (1.5%) of total ESRD population– Most 60% treated with peritoneal dialyses at home– 20% below age of 6
• Mircera: chemically synthesized continuous erythropoietin receptor activator– Efficacious in correction anemia in ESRD– Toxicology data suggest good safety and tolerability
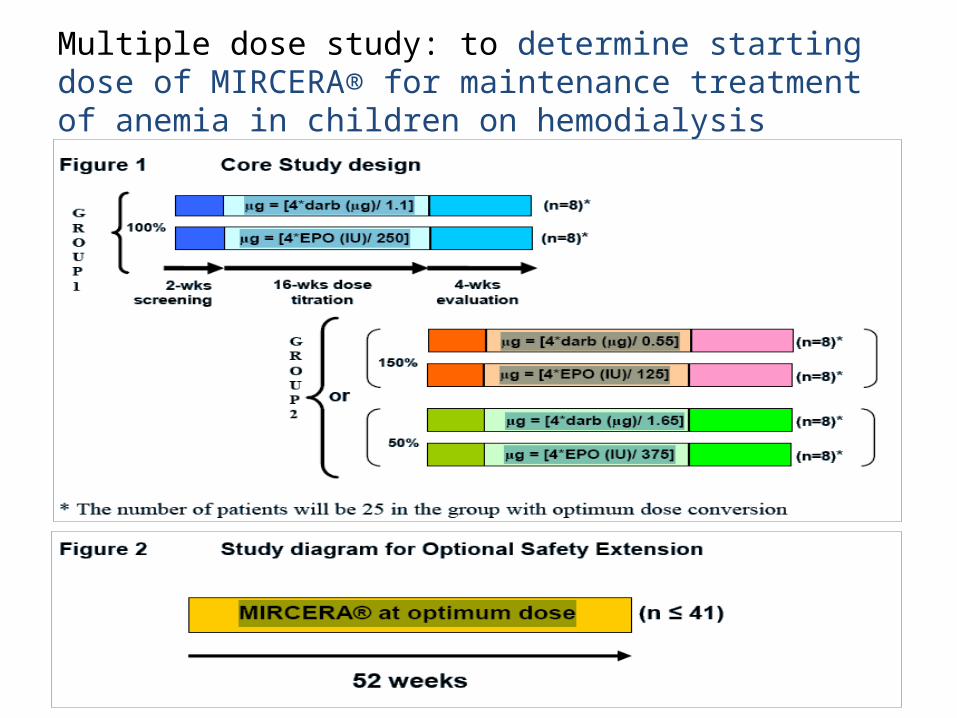
Multiple dose study: to determine starting dose of MIRCERA® for maintenance treatment of anemia in children on hemodialysis
Zaključci
• Lekovi koji se primenjuju kod dece generalno nisu dovoljno rigorozno ispitani u pedijatrijskoj populaciji
• Nove zakonske regulative za odobravanja upotrebe leka zahtevaju da se pedijatrijske studije rade paraleleno sa adultnim studijama
• Razvoj lekova za pedijatrijsku primenu je kompleksan proces jer zahteva razvoj pedijatrijske formulacije, odredjivanje optimalne doze sve starosne grupe i dugotrajno pracenje ispitanika
• Primena novih zakonskih regulative je povecala broj istrazivanja usmerenih na optimalnu primenu modernih lekova kod dece

Best Pharmaceuticals for Children – Oxymoron?
29Da joj čitam pred spavanje? A šta misliš, da joj damo opet jedan benzedinčić?© New Yorker