transforming end of life care in acute hospitals pm workshop 3: vital signs ‘making measurement...
TRANSCRIPT

Vital signs – making measures matter
Transforming End of Life Care in Acute HospitalsSean Manning
18th November 2015
The black hole?
“We call our measures board the ‘wall of shame’”
“ Most of what we collect seems meaningless to us. We rarely see the
results of what we submit.”
This paperwork is stopping us doing our job!”

Insights into
• Importance of measurement• Traditions of measurement• Knowing How We are Doing• Pareto principle• Structure ‐ process ‐ outcome measures• Driver diagrams• Model for improvement• Tracking variation• 7 steps to measurement




Hitting the target but missing the point!

Measurement for improvement
UnderstandUnderstand
ImproveImprove
MotivateMotivate
Curiosity

“I can make the last stage of my life as good as possible because everyone works together confidently, honestly and consistently to help me and the people who are important to me, including my carer(s).”

The traditions of measurement
• eg A‐B comparison, average, huge dataset
Research
• eg one‐to‐many benchmarking comparision, average, large dataset
Judgement
• eg continual analysis of single changing process over time
Improvement

Research Judgement Improvement
GoalNew knowledge (not its applicability)
ComparisonReward / punishmentSpur for change
Process understanding
Evaluating a change
Hypothesis Fixed None Multiple and flexible
Measures Many Very few Few
Time period Long, past Long, past Short, current
Sample Large Large Small
Confounders Measure or control Describe and try to measure
Consider but rarely measured
Risks in improvement
settings
Ignores time based variation
Over‐engineers data collection
Ignores time based variation
Over‐reaction to natural variation
Incorrectly perceived as ‘inferior statistics’
Measurement mindsets
Based on L Solberg, G Mosser and S McDonald (1997) The Three Faces of Performance Measurement: Improvement, Accountability and Research, Journal on Quality Improvement, 23 (3): 135 ‐ 147.

What mind sets are at play here?
Research
ImprovementJudgement


What do we collect now?

What does a great team meeting look like?Is that what we do?

SMART goals

Making better decisions about prioritiesFocusing your effort where it matters
Prioritisation - The Pareto Principle

The Principle
We don’t have time to improve everything
A small number of issues account for the majority of the challenge
20% of causes account for 80% of the problem
We should focus on the ‘critical few’, not the ‘trivial many’

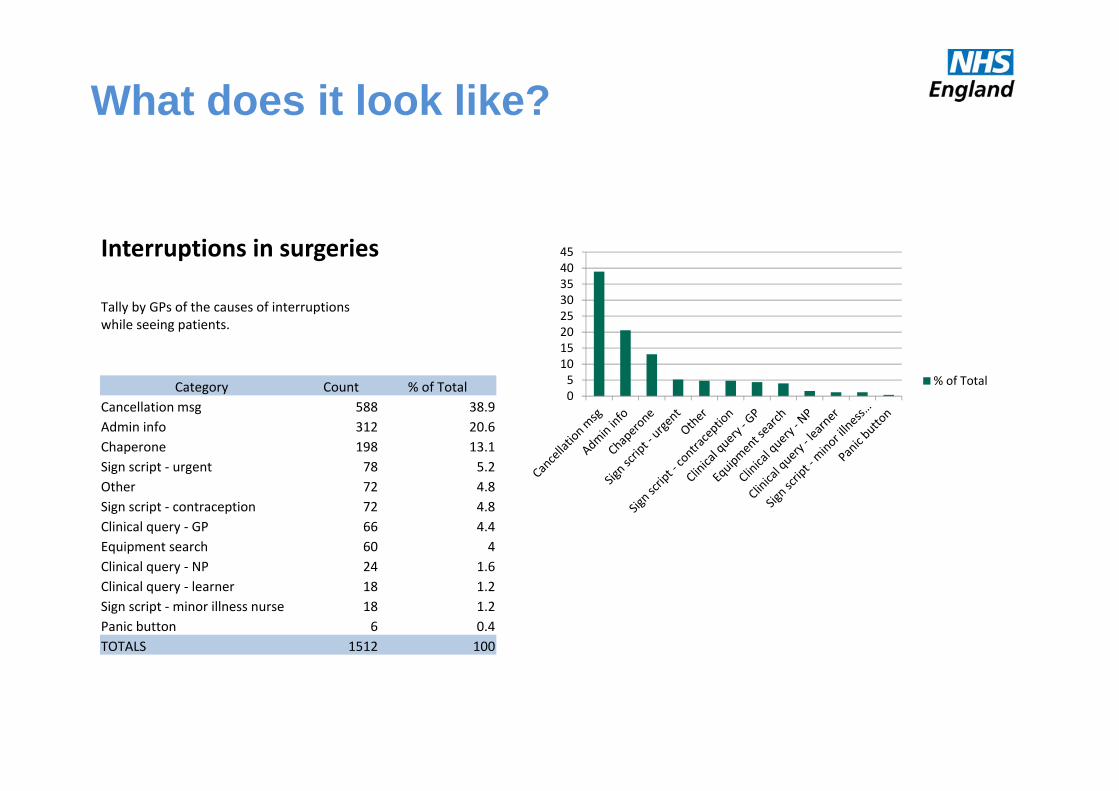
What does it look like?
Interruptions in surgeries
Tally by GPs of the causes of interruptions while with a patient.
Category CountSign script ‐ contraception 72Sign script ‐minor illness nurse 18Clinical query ‐ learner 18Clinical query ‐ NP 24Sign script ‐ urgent 78Chaperone 198Equipment search 60Admin info 312Clinical query ‐ GP 66Panic button 6Cancellation msg 588Other 72TOTALS 1512
0100200300400500600700
Count
What does it look like?
Interruptions in surgeries
Tally by GPs of the causes of interruptions while seeing patients.
Category Count % of TotalCancellation msg 588 38.9Admin info 312 20.6Chaperone 198 13.1Sign script ‐ urgent 78 5.2Other 72 4.8Sign script ‐ contraception 72 4.8Clinical query ‐ GP 66 4.4Equipment search 60 4Clinical query ‐ NP 24 1.6Clinical query ‐ learner 18 1.2Sign script ‐minor illness nurse 18 1.2Panic button 6 0.4TOTALS 1512 100
051015202530354045
% of Total

What does it look like?
0
10
20
30
40
50
60
70
80
90
100
0
5
10
15
20
25
30
35
40
45
% of Total
Cumulative %

What does it look like?
0
10
20
30
40
50
60
70
80
90
100
0
5
10
15
20
25
30
35
40
45
% of Total
Cumulative %
Three categories of interruption (17%) account for 73% of the problem
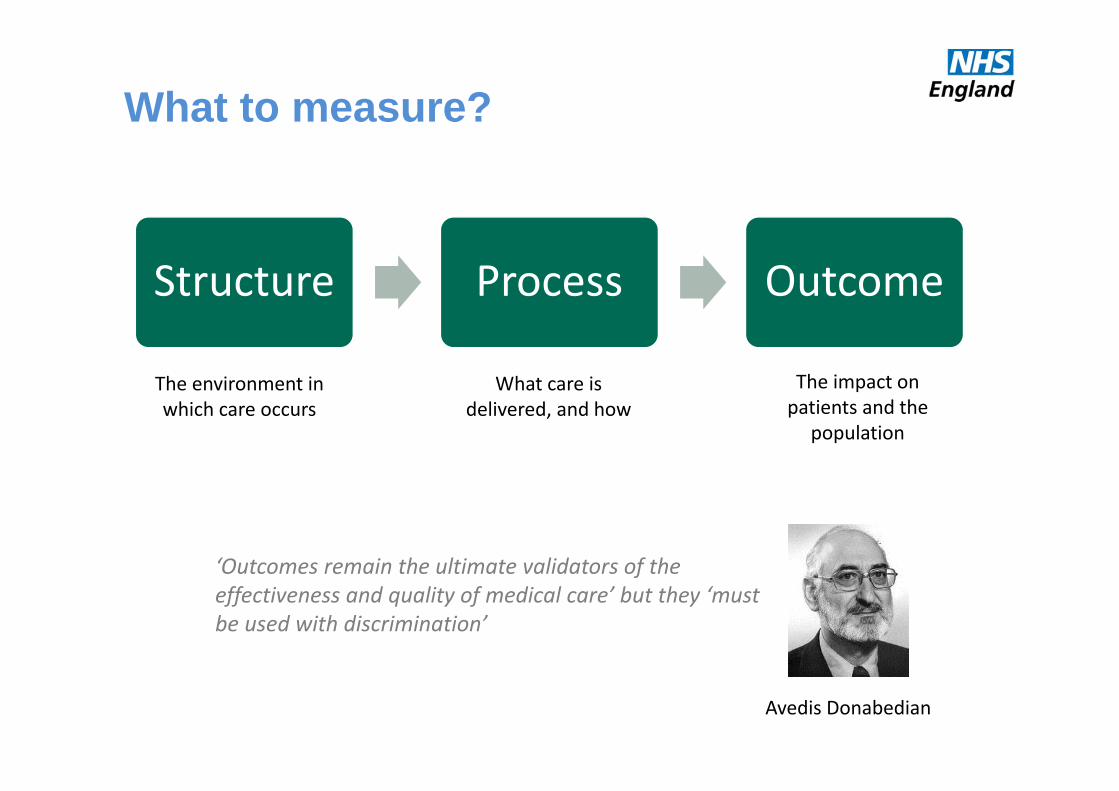
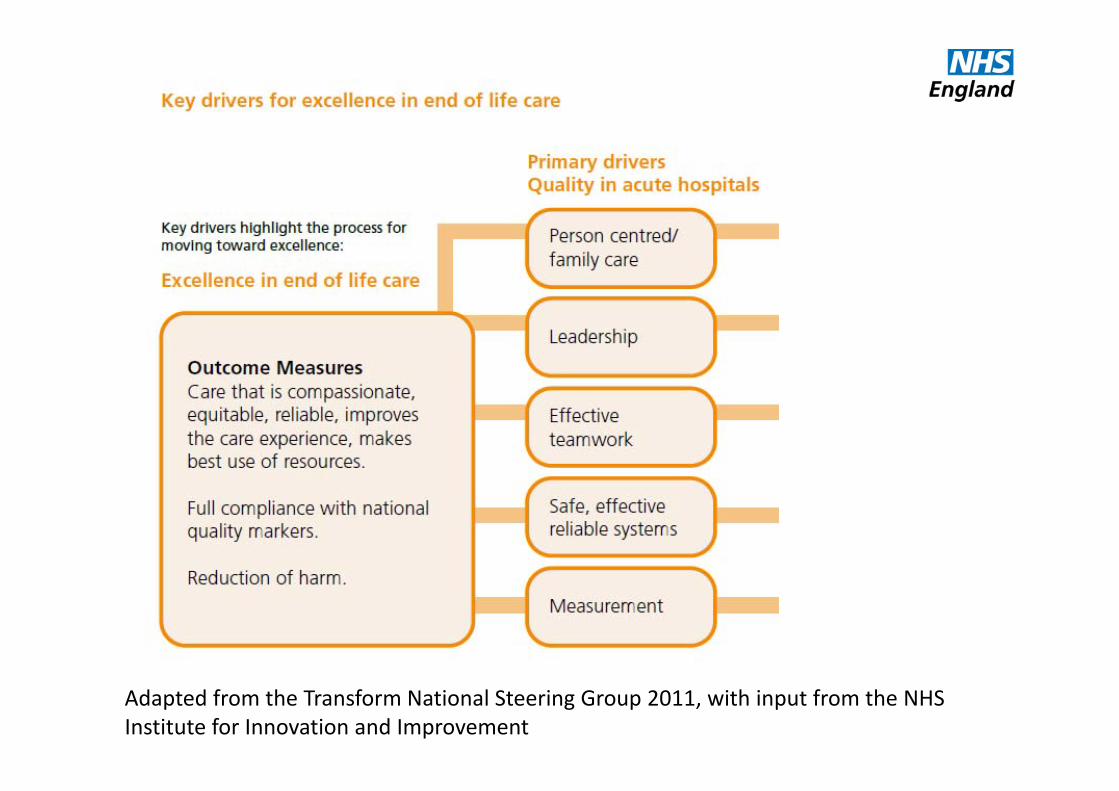
What to measure?
Structure Process Outcome
Avedis Donabedian
‘Outcomes remain the ultimate validators of the effectiveness and quality of medical care’ but they ‘must be used with discrimination’
The environment in which care occurs
What care is delivered, and how
The impact on patients and the
population

What to measure?
Structure Process Outcome
o Outcomes are a worthy goalo All have pros & conso Should measure a selection of all
threeVeena Ralegh

What to measure?
Structure Process Outcome
“Intermediate outcomes”• a common solution• properties of both process & outcome• but be careful to acknowledge it’s not ‘the ultimate outcome’

OUTP
UTS
HUMAN FACTORS
HUMANFACTORS
INTERNAL PROCESSES & PROCECEDURES
INPU
TSEXTERNALFACTORS
Process Measure(s)
Outcome
Measure(s)
Balancing Measure(s)
What to measure?
Is it being done?
Is it working?
Unintended consequences?
Is it in place?
Structure Measure(s)
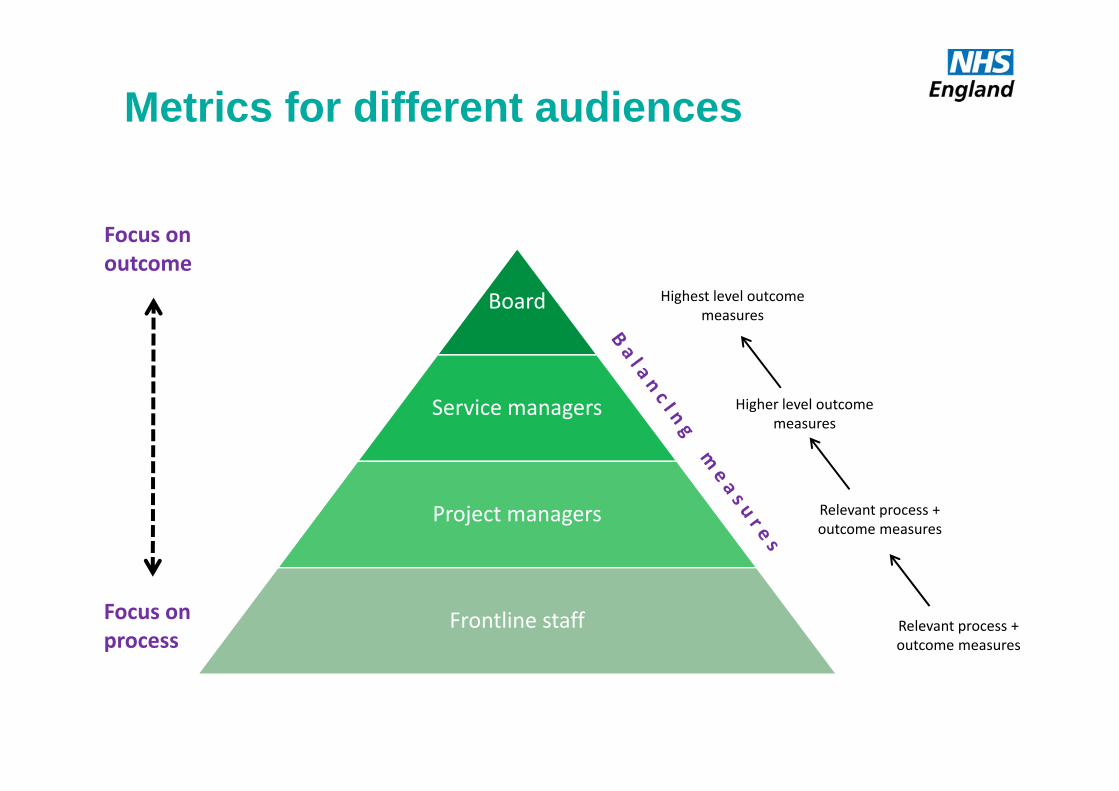
Metrics for different audiences
Board
Service managers
Project managers
Frontline staff
Focus onoutcome
Focus onprocess
Relevant process +outcome measures
Relevant process +outcome measures
Higher level outcomemeasures
Highest level outcomemeasures

Driver Diagrams
Benefits ...build complex strategyimmediatevisual
Different scenarios ...1. Help generate change ideas2. Marshall a mass of change ideas3. Survive failure / the unexpected
avoid “silver bullet” thinkinghighlight overlooked ideas

Aim
Defect FreeSurgery
Avoid Mistakes
AvoidComplications
AvoidDelays
Driver Intervention
Conduct team brief
Conduct team debrief
Conduct time out
Produce accurate lists
Implement SSI bundle
Implement VTE bundle
Have correct kit to hand
Ensure staff adequately trained
O1
O2
O3
O1 Overall glitch countO2 Never eventsO3 Number of surgical site infections
P1 % lists with Team BriefP2 % lists with Team DebriefP3 % compliance with SSI bundle
P2
P1
P3
Driver Diagrams clinical example

AIM –an improved system
Primary driver 1
Primary driver 2How much? By when?
Secondary driver 1
Secondary driver 2
Secondary driver 3
Secondary driver 4
Secondary driver 5
CP1
CP2
CP3
CP4
CP5
CP6
CP7
How much? By when?
How much? By when?
AIM PRIMARYDRIVERS
SECONDARYDRIVERS
CHANGEPROJECTS
Driver DiagramsPlanning & presenting change
CauseEffectDrives

Driver DiagramsWeight loss example
Pedometer
Gym work out 3 days
Squash weekends
No pub weekdays
Take packed lunch
Low fat meals
Buy only 1 sandwich
Water bottle for work bag
Fruit for dessert
Put away the large glasses
Put cycling days in diary
Cycling kit out night before
Get rid of Oyster cardBe more
active during the
day
Do sport
Drink less alcohol
Substitute lower
calorie foods
Eat lessReducecalories in
Increasecalories out
Take stairs
2 stone weight loss
in 6/12
AIM
Improveaccess
Help marshal change ideas
Waiting room info, list clinician interests/languages, web info, Rx access (Feel Better Faster), signpost more (WIC/HV/minor inj/Secs/DNs/A&E), Chronic disease training, care planning, review periods, get it right first time, test results processing, teamworking/multiskilling, results line hours, protocols for test results, widen skill mix, BP machine in watiting room, update rpt Rx, pharmacist planning, streamline processes, streamline recalls, education & reflection, up‐to‐date pt contact details, know what appt is for, pt registration management, Triage, Care planning / pathways, more TelC, emailC, clinical buddies/teams, test results, repeat Rx, forwarding tasks + results, check + update usual GP, results actioned by right person, advance appt booking, reserve list, ask pt who they want, rota in advance, notekeeping w plan + pt info, Consult skills, comp skills, speed reading/typing, forms + equipment, multi‐skilling, longer appts, No emerg appts, Test results, Care planning, High risk processes, Referral chase‐up, results continuity, streamline processes, streamline recalls, clear up alerts, handling of normal results, self‐checkin, fast‐track queue

AIM PRIMARYDRIVERS
SECONDARYDRIVERS
CHANGEPROJECTS
Improveaccess
Doctors (capacity)
Demand
Dealing (efficiency)
Appt system
Supply of GP time
Organisation of GP time
Pt help‐seeking
Deflecting demand
Creating our own workload
Planning care
Appt system project
GP rota change project
Community education
Waiting room TV
PILS & CDs & DVDs
Feel better faster
Student sick notes
Reception signposting
Test results
Consulting skills
Longer appts
Guaranteed interpreters
Help marshal change ideas
Dealing w failed referrals
Chronic disease pathways
Review periods
More TelC’s
Email appts
Continuity
AIM PRIMARYDRIVERS
SECONDARYDRIVERS
CHANGEPROJECTS
Improveaccess
Doctors (capacity)
Demand
Dealing (efficiency)
Appt system
Supply of GP time
Organisation of GP time
Pt help‐seeking
Deflecting demand
Creating our own workload
Planning care
Appt system project
GP rota change project
Community education
Waiting room TV
PILS & CDs & DVDs
Feel better faster
Student sick notes
Reception signposting
Test results
Consulting skills
Longer appts
Guaranteed interpreters
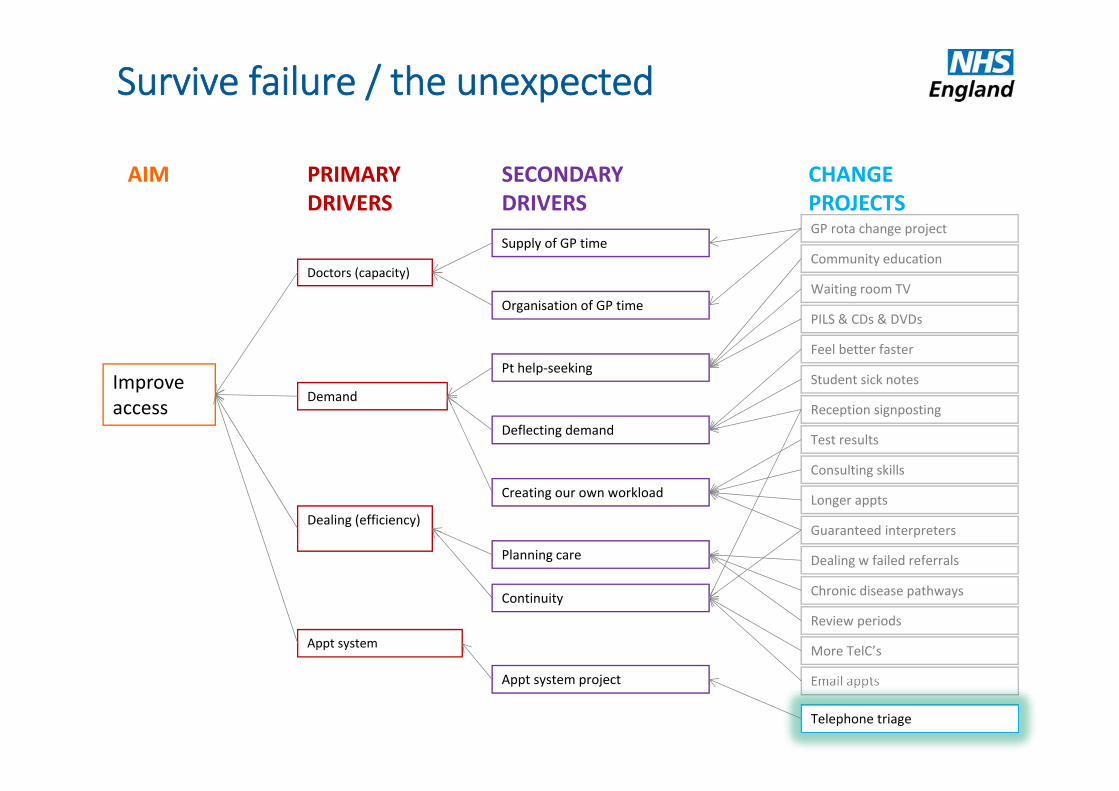
Survive failure / the unexpected
Dealing w failed referrals
Chronic disease pathways
Review periods
More TelC’s
Email appts
Continuity
Telephone triage
Adapted from the Transform National Steering Group 2011, with input from the NHS Institute for Innovation and Improvement

How much?By when?

Different audiences
Board
Service managers
Project managers
Frontline staff

What to measure?
AIM –an improved system
Primary driver 1
Primary driver 2
Secondary driver 1
Secondary driver 2
Secondary driver 3
Secondary driver 4
Secondary driver 5
CP1
CP2
CP3
CP4
CP5
CP6
CP7
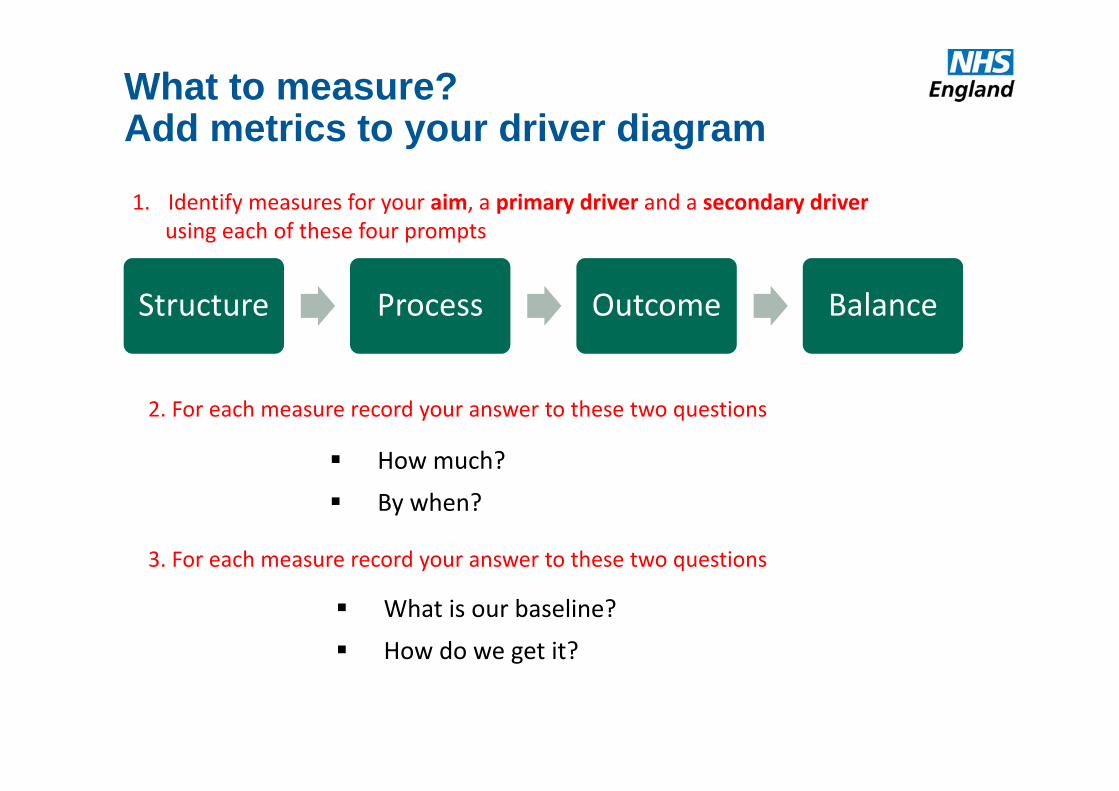
What to measure?Add metrics to your driver diagram
Structure Process Outcome Balance
How much?
By when?
What is our baseline?
How do we get it?
1. Identify measures for your aim, a primary driver and a secondary driver using each of these four prompts
2. For each measure record your answer to these two questions
3. For each measure record your answer to these two questions

How much & how often?
There is no precise science to guide decisions about how many metrics to use, or how often…
How many different thingsare you monitoring consciously?
How frequently?
Straight motorwayReversing round a corner

The usual approach

Meeting rooms
Real world
Approve
Design Design Design Design
Implement !
Courtesy of Patient Safety First
Opinion

Meeting rooms
Real world
Courtesy of Patient Safety First
Implement
Approve
Test & refine
Test & refine
Test & refine
Design
Measurement
Change through small steps
Change ...• with a clear purpose• you can learn from (without fear of failure)• which is less exhausting• with fewer unintended consequences• which builds engagement and optimism

What are we trying to accomplish?
How will we know that change is an improvement?
What change can we make that will result in improvement?
The Model for Improvement
Langley, G., Nolan, K., and Nolan, T., 1994. The Foundation of Improvement, Quality Progress, June 1994

Plan-Do-Study-Act
disciplined framework ensures every part is done every time
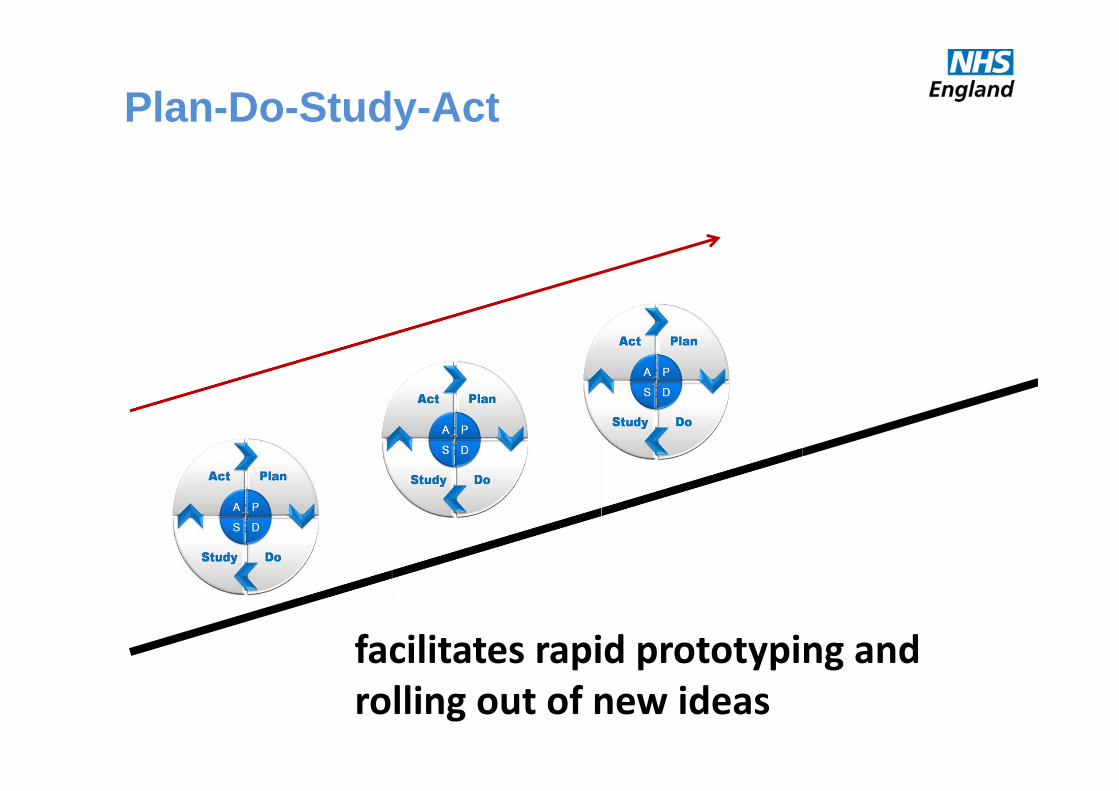
Plan-Do-Study-Act
facilitates rapid prototyping and rolling out of new ideas

Plan-Do-Study-Act

“We’re pressed for time, so we’ll be jumping to conclusions”
We’re pressed for time, so we’ll be jumping to conclusions


The Manager’s Dilemma
In order to manage a system, we are required to make predictionsabout its future.
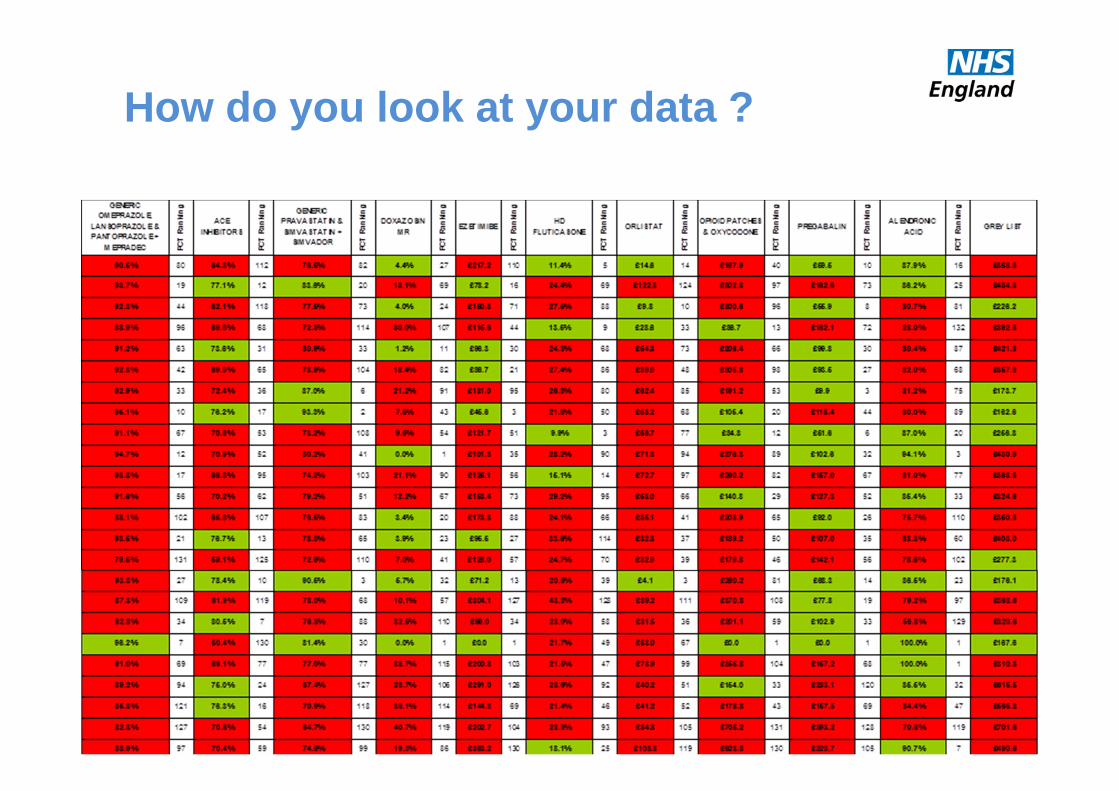
How do you look at your data ?

“If I stick my right foot in a bucket of boiling water and my left foot in
a bucket of ice water, on the average, I’m pretty comfortable.”
The Problem with Averages
The Problem
Aggregated data presented in tabular formats or with summary
statistics, will not help you measure the impact of improvement efforts. Aggregated data can only lead to judgment, not to improvement.

Enumerative Dynamic
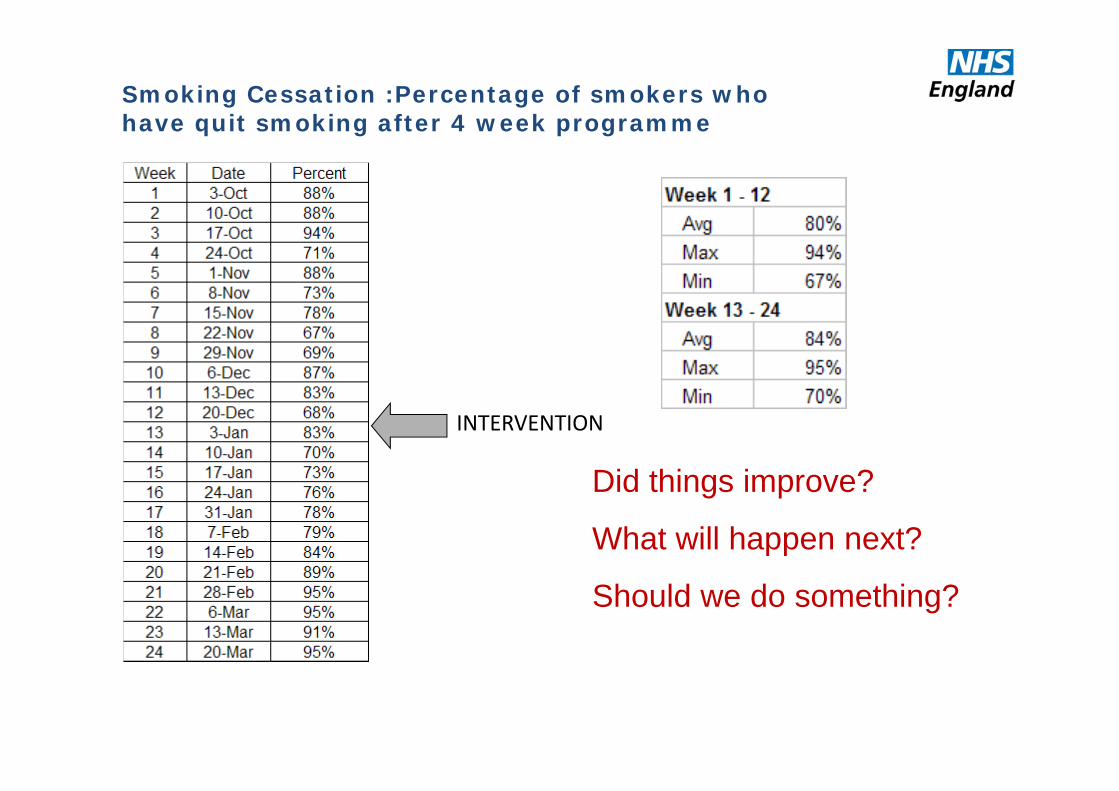
Did things improve?
What will happen next?
Should we do something?
Smoking Cessation :Percentage of smokers who have quit smoking after 4 week programme
INTERVENTION

1C-58
50%
55%
60%
65%
70%
75%
80%
85%
90%
95%
100%
10/3
/200
7
10/1
7/20
07
10/3
1/20
07
11/1
4/20
07
11/2
8/20
07
12/1
2/20
07
12/2
6/20
07
1/9/
2008
1/23
/200
8
2/6/
2008
2/20
/200
8
3/5/
2008
3/19
/200
8
Change made here
Did things improve?
What will happen next?
Should we do something?
Smoking Cessation :Percentage of smokers who have quit smoking after 4 week programme
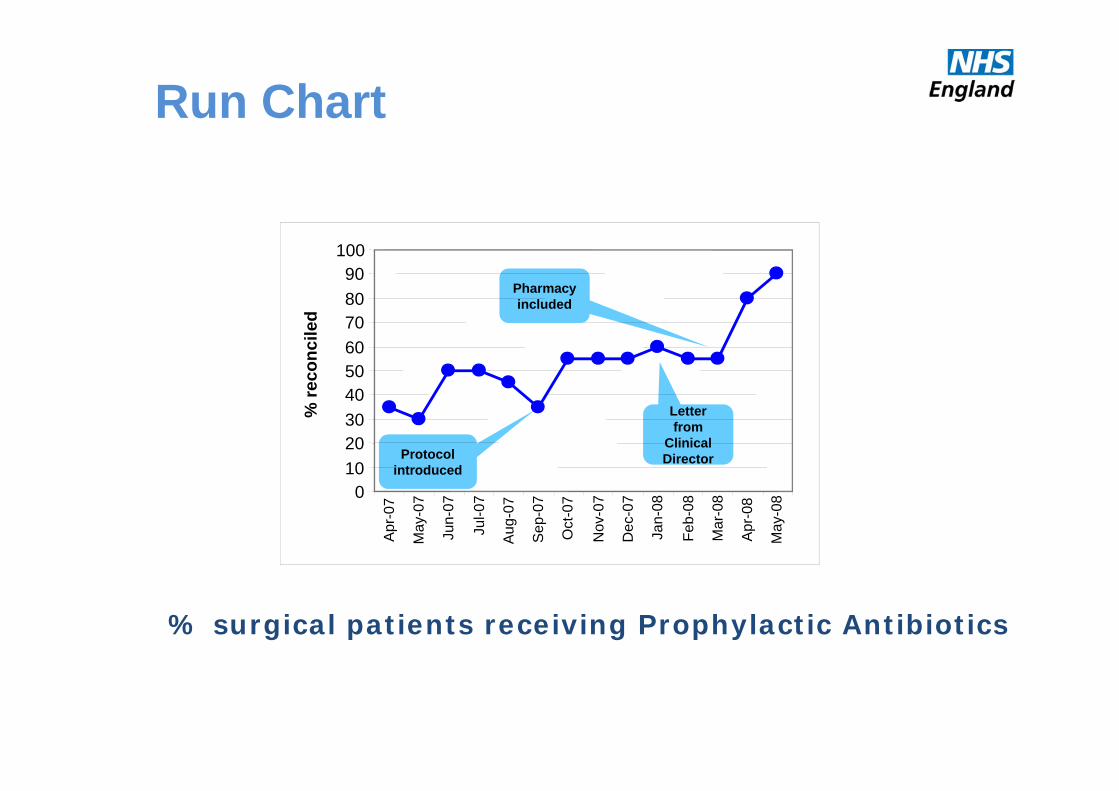
Protocol introduced
Letter from
Clinical Director
Pharmacy included
% surgical patients receiving Prophylactic Antibiotics
0102030405060708090
100
Apr
-07
May
-07
Jun-
07
Jul-0
7
Aug
-07
Sep
-07
Oct
-07
Nov
-07
Dec
-07
Jan-
08
Feb-
08
Mar
-08
Apr
-08
May
-08
% re
conc
iled
Run Chart

Waiting time results
70
35
01020304050607080
AvgBeforeChange
Avg AfterChange
Wai
t Ti
me
(min
.)

Waiting time results0
102030405060708090
100
date
Jan
Feb
Mar
Apr
May Jun
Jul
Aug Sep
Oct
Nov
Dec
Change MadeC
ycle T
ime (m
in.)
0102030405060708090
100
date
Jan
Feb
Mar
Apr
May Jun
Jul
Aug Sep
Oct
Nov
Dec
Change Made
Cyc
le T
ime
(min
.)
Unit 1
Unit 3
0102030405060708090
100
date
Jan
Feb
Mar
Apr
May Jun
Jul
Aug Sep
Oct
Nov
Dec
Change MadeC
ycle
Tim
e (m
in.)
Unit 270
35
01020304050607080
AvgBeforeChange
Avg AfterChange
Wai
t Ti
me
(min
.)

If We Have 3 Numbers in Sequence:How Do You Report These?
Downward Trend
Upward Trend
Some Recovery
Setback
Collapse
Dramatic Recovery
Each pattern has an equal 1:6 chance
Lets Get Scientific!
Data has no meaning without a
Context

Run ChartsPlot the dots
0102030405060708090
100
date
Jan
Feb
Mar
Apr
May Ju
n
Jul
Aug Se
p
Oct
Nov
Dec
Change Made
Cyc
le T
ime
(min
.)

0
20
40
60
80
100
120
Consecutive trips
Min.
My Trip To Work
Mean
Common Cause
Special Cause
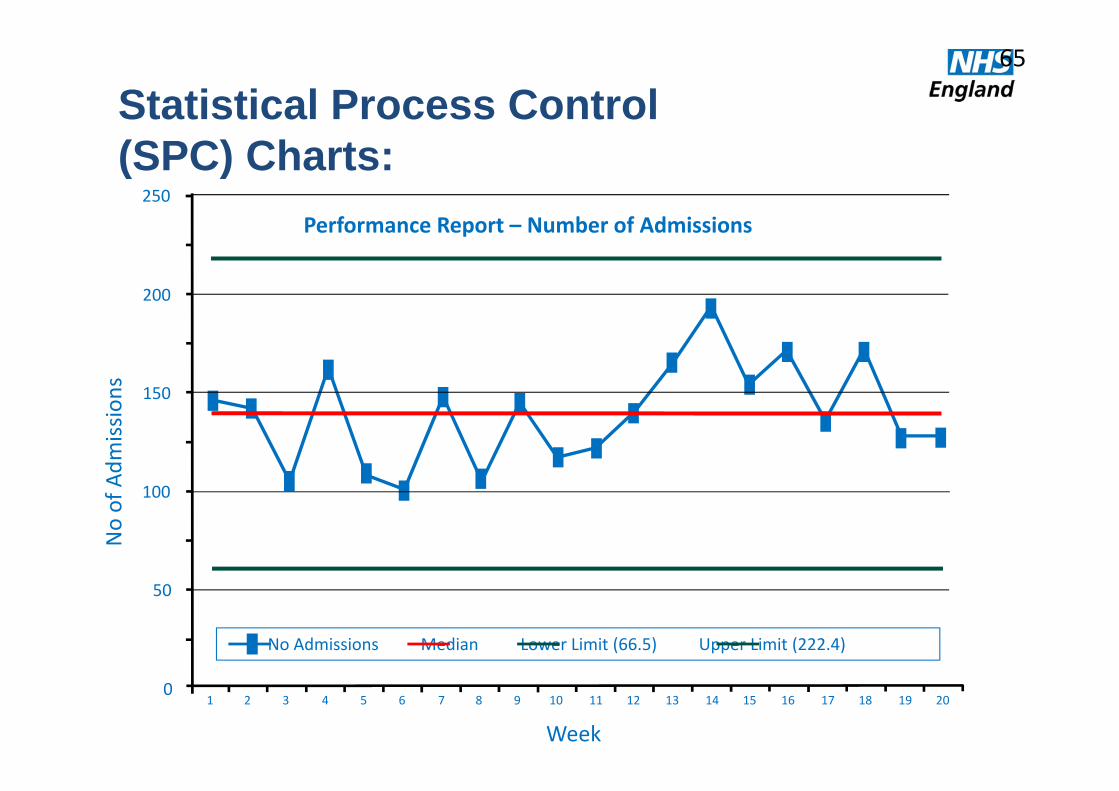
Statistical Process Control(SPC) Charts:
No of Adm
issions
0
200
150
100
50
250
Performance Report – Number of Admissions
Week1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
No Admissions Median Lower Limit (66.5) Upper Limit (222.4)
65

It is normalto have some variation
But some may be‘special’
Control charts

2 Ways To Improve A Process
If controlled variation (Common Cause)• process is stable
• variation is inherent to process
• therefore, process must be changed i.e. Redesign
If uncontrolled variation (Special Cause)• process is unstable
• variation is extrinsic to process
• cause should be identified and “treated”

7 steps to measurement
https://www.youtube.com/watch?v=Za1o77jAnbw&list=PL_V1d0Y94nv4u2yCCDnApxa9ykKmSG1oE

Insights into
• Importance of measurement• Traditions of measurement• Knowing How We are Doing• Pareto principle• Structure ‐ process ‐ outcome measures• Driver diagrams• Model for improvement• Tracking variation• 7 steps to measurement

What do you need from your data?