임상시험이란? - 대한내과학회 · 2016-12-27 · 임상시험에서고려할사항 speed...
TRANSCRIPT

임상시험이란 ?
분과전문의로서의 역할
Young Suk Park, M.D.
Samsung Medical Center

임상시험에서 고려할 사항
Speed : 빠른 심사, 계약, 피험자 등록
Quality : 믿을 수 있는 자료
With ICH-GCP guideline
Speed
• 행정
– 병원 행정 part 의 지원
– IRB 의 체계적인 운영
– 병원 집행부의 의지
• 연구자
• 환자

Speed : 연구자
• 환자와 상담할 시간이 없다.
• 상담과 권유에 익숙치 않다.
• 새로운 임상시험이면 본인도 잘 모른다.
• 상담 기술을 배운다.
• 임상시험의 이익에 대해 확인/확신한다.
• 도와줄 인력을 확보한다.

Speed : 환자
• 암 환자가 임상시험 참여를 결정하는 요인
선호하는 요인 점수(%)
치료에 대한 기대 83
의료진의 관심 80
의학발전에 대한 참여 75
병에 대한 많은 정보 75
새로운 치료를 받음 72

Speed : 환자
• 암 환자가 임상시험 참여를 결정하는 요인
거부하는 요인 점수(%)
환자 스스로 치료를 결정치 못 함 25
의료진이 아닌 시험자체에서 치료의 결정
24
시험적 치료를 받을 가능성 15
Speed : Barriers
PATIENT RELATED• Doctor never discussed or offered• Unaware of trials as option• Concerns about insurance coverage• Fear of receiving placebo PHYSICIAN RELATED
• Burdensome regulatory requirements- Institutional Review Board- Informed consent- Conflict of interest
• Lack of time• Inadequate funding for personnel• Inadequate reimbursement• Resistance by third-party payers
… …
Quality
• 임상시험은 다음에 따라 실시, 기록되어야
한다. 시험계획서(Protocol)표준작업지침서(SOP)임상시험관리기준(GCP) 및 관련규정
• 임상시험과 관련된 모든 자료는 정확, 완전, 검증 가능해야 한다.
• 그 결과로 자료는 신뢰를 받는다.
Major Deficiencies/Deviation
• A variance from protocol-specified
procedures that makes the resulting
data questionable
• Evidence of significant deviation from
protocol treatment, data alteration, data
falsification, or non-reporting of data
that effects protocol eligibility,
treatment or disease status

Major Deficiencies/Deviation
• Informed Consent
• Eligibility
• Treatment
• Disease Outcome/Response
• Toxicity
• General Data Quality

Major Deficiencies/Deviation
• Informed Consent Form– missing
– not signed and dated by the patient
– signed after patient started on treatment
– does not contain all required signatures
– used was not current IRB-approved version at the time of patient registration
– not protocol specific
– does not include updates or information required by IRB.

Major Deficiencies/Deviation
• Eligibility
– Review of documentation available at the
time of the audit confirms patient did not
meet all eligibility criteria as specified by
the protocol
– Documentation missing.
• Unable to confirm eligibility
– Enrollment of ineligible patients

Major Deficiencies/Deviation
• Treatment – Incorrect agent/treatment used
– Additional agent/treatment used which is not permitted by protocol
– Dose deviations incorrect (error greater than +/- 10%)
– Dose modifications not per protocol
– Treatment doses incorrectly administered, calculated or documented
– Unjustified delays in treatment
Major Deficiencies/Deviation
• Disease Outcome/Response Failure to evaluate response according to the
protocol, for example;
– Inaccurate documentation of initial sites of involvement
– Tumor measurements/evaluation of status or disease not performed according to protocol
– Protocol-directed response criteria not being followed

Major Deficiencies/Deviation
• Disease Outcome/Response Failure to evaluate response according to the
protocol, for example;
– Claimed response (PR, CR, etc) cannot be verified
– Failure to detect cancer (as in a prevention study) or failure to identify cancer progression

Major Deficiencies/Deviation
• AE/SAE Failure to assess and report AE and SAE
according to the protocol
– Grades, types, or dates/duration of SAE inaccurately recorded
– Follow-up studies necessary to assess AE/SAE not performed
– Failure to report a toxicity that would require filing an Adverse Event Report (AER)
– Recurrent under- or over-reporting of AE/SAE
Major Deficiencies/Deviation
• General Data Quality – Recurrent missing documentation e.g.,
charts
– Protocol-specified laboratory tests not documented
– Protocol-specified diagnostic studies not documented
– Frequent data inaccuracies
– Errors in submitted data
– Delinquent data submission

Lesser Deficiency/Minor Deviation
• Deficiency that is judged to not have a significant impact on the outcome or interpretation of the study and is not described above as a major deficiency.
• Transcriptional errors
• An unacceptable frequency of lesser deficiencies(exceed 5%) should be treated as a major deficiency in determining the final assessment of a component.
For Speed & Quality
• Monitoring
• 인력
– 전임의/전공의 ?
– 일반 간호사 ?
– 임상시험 관련 전문인력

Clinical Research Coordinator
• Clinical Research Nurse, CRN
• 의뢰자와 시험자 사이에서 조정자– 시험책임자의 감독하에
– 임상시험 관련규정의 원칙에 따라
– 전문적인 지식과 기술
– 환자의 존엄성과 피험자의 권리를 보호
– 신뢰성 있는 자료를 수집, 기록, 보관
– 윤리적이고 과학적인 임상시험을 추구
– 실질적인 조정과 수행에 책임, 건강전문가

환자
Sponsor PI
CRC
Clinical Research Coordinator
CRC의 자격요건
• 지식– 의약학 관련분야 전공
– 임상약리학, 면역학, 생화학 등의 지식
– 임상시험 수행 훈련
– 임상시험 관련 각종 규정, 지침서 및 임상시험계획서
• 기술– 임상간호술 및 임상경험
– 의사소통 및 상담기술
– 기록, 컴퓨터 및 어학능력
• 태도– 임상시험 질 향상에 공헌하려는 마음가짐과 태도

임상시험에서 CRC의 위치
• 교육자
• 피험자의 대변자
• 직접 간호 제공자
• 임상시험 진행자
• 의견의 충돌
– 의사결정, 책임한도의 갈등
– 환자를 위한 윤리적, 도덕적 문제
•피험자 보호

어떠한 임상시험을 할 수 있을까 ?
• Hypothesis
• Know what has been done before
– Systematic review or meta-analysis
– Trials & literatures search
• Safe dose, evidence of activity ?
• Comparative trial, sufficiently strong ?

어떠한 임상시험을 할 수 있을까 ?
• If the difference between treatments in a clinical trial is declared “not statistically
significant”, this does not mean that there
are no clinically important differences
between the two treatments.
– Not enough evidence to draw any conclusions
– Might be due to too low power(too small
sample size)

어떠한 임상시험을 할 수 있을까 ?
• Modified study and new evidence ?
– Not truly randomized study
– Changed gold standard
– Statistically underpowered study
– Lacking important outcome measure
– Highly selected population
– New combination and/or new indication

Has a safe dose or schedule been established in clinical use ?
No Yes
Phase I study may be needed Is there evidence of activity at this dose or schedule?
No Not yet investigated Yes
Abandon or review potentialto enhance activity? Phase Ⅱ trial may be needed
Has the treatment been used in a comparative trial?*
No Yes
Is there sufficient evidence ofpotential improvement over standard tojustify a randomized trial?
Has the trial(s) answered the questions of interest reliably?
No Yes No Yes
Randomized phase Ⅲ trialmay be needed
Could a systematic review ±meta-analysis answer the question?
No Yes
Trial may not be required
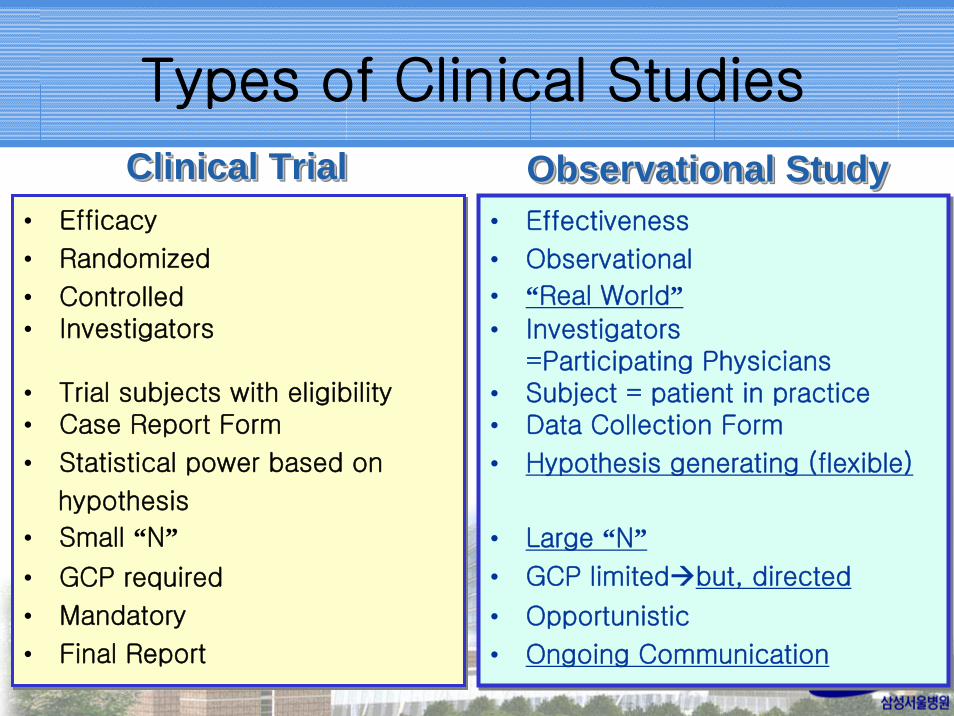
• Efficacy
• Randomized
• Controlled• Investigators
• Trial subjects with eligibility• Case Report Form
• Statistical power based on
hypothesis
• Small “N”• GCP required
• Mandatory
• Final Report
• Efficacy
• Randomized
• Controlled• Investigators
• Trial subjects with eligibility• Case Report Form
• Statistical power based on
hypothesis
• Small “N”• GCP required
• Mandatory
• Final Report
• Effectiveness
• Observational
• “Real World”• Investigators
=Participating Physicians• Subject = patient in practice• Data Collection Form
• Hypothesis generating (flexible)
• Large “N”• GCP limited but, directed
• Opportunistic
• Ongoing Communication
• Effectiveness
• Observational
• “Real World”• Investigators
=Participating Physicians• Subject = patient in practice• Data Collection Form
• Hypothesis generating (flexible)
• Large “N”• GCP limited but, directed
• Opportunistic
• Ongoing Communication
Clinical TrialClinical TrialClinical Trial Observational StudyObservational StudyObservational Study
Types of Clinical Studies

삶의 질 관련
임상시험
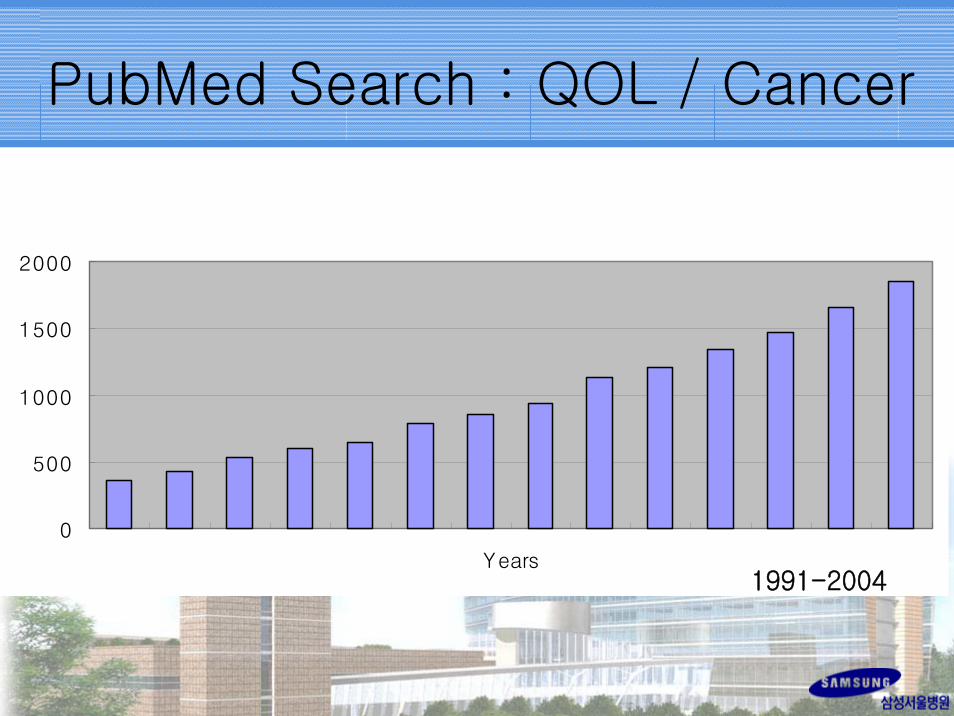
PubMed Search : QOL / Cancer
0
500
1000
1500
2000
Years1991-2004

삶의 질 : Quality of Life
• Assessment of QOL into every new trial
• Decision not to include QOL in a trial
– “We don’t care about patients’ QOL”• Results of many trials with QOL
–Largely irrelevant data
–Use of considerable resources
–Overburdening of patients

암치료와 삶의 질
• Chance of cure– toxicity ↑ & QOL ↓ : reasonable
• No chance of cure– Giving treatment with longer survival but
poorer QOL
– Reducing or stopping treatment with shorter survival but better QOL
• ‘Treatment can be recommended in metastatic cancer even without an improvement of survival, if it improves quality of life’ ASCO guidelines 1995

QOL in Clinical Trials
• Determine your QOL objective
• Choose an instrument
• Select a design (time schedule) linked to your objective
• Develop an analysis plan
• To go or not to go ?
삶의 질 임상시험에서 고려할 사항
• Who should assess QOL ?
• Response shift
• Timepoints
• Compliance– questionnaire, item, patients, center
• How many patients are required ?
• Choosing the questionnaire
• QOL coordinator
• Information sheets
• Quality and analysis of data

0
5
10
15
20
25
Improved Same Worse
Num
ber of
patients
Life quality (patient)
Phy s icalcondition(patient)
Overallcondition(phy s ician)
삶의 질에 대한 평가자의 차이

삶의 질 관련 설문지의 번역
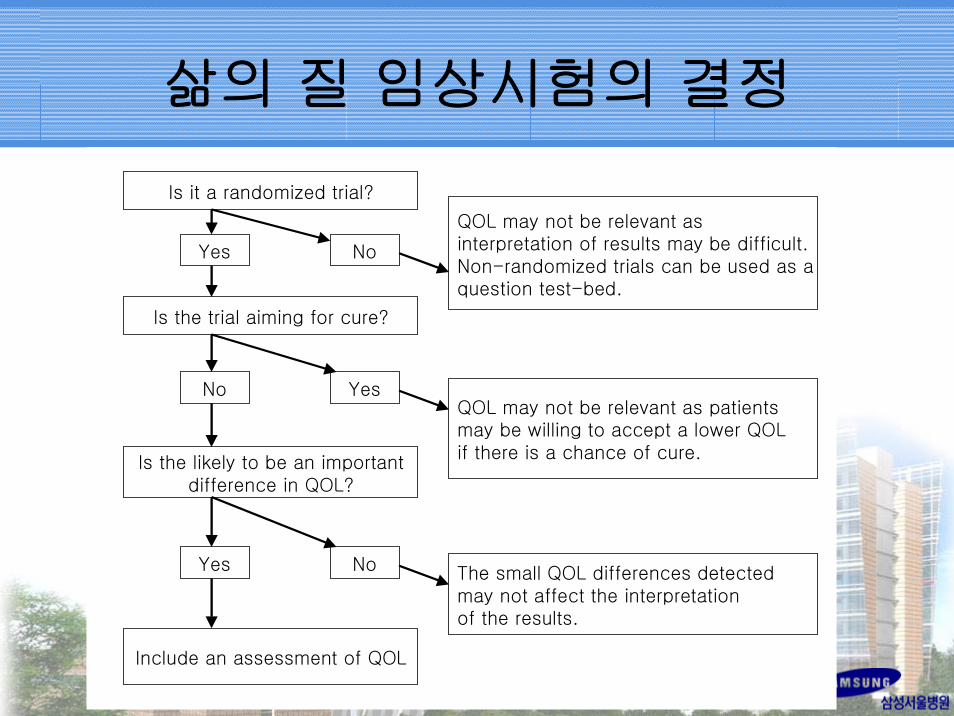
Is it a randomized trial?
Yes
QOL may not be relevant as interpretation of results may be difficult. Non-randomized trials can be used as aquestion test-bed.
Is the trial aiming for cure?
Is the likely to be an importantdifference in QOL?
Include an assessment of QOL
QOL may not be relevant as patientsmay be willing to accept a lower QOLif there is a chance of cure.
The small QOL differences detectedmay not affect the interpretationof the results.
Yes
Yes
No
No
No
삶의 질 임상시험의 결정

임상시험에서
내가 할 수 있는
일은 ?

Differences : Medicines, Medical devices, Surgery
Characteristics MedicinesMedical
devices
Surgical
operations
Patient
protection Usually Sometimes Rarely
Source of
innovation &
developmentCorporation Corporation
Individual or
group of
professionals
Cost of
development Very high Moderate Low
Double-blind
methodsYes Seldom
Almost never
Placebo ?
Trials with Surgical Procedures
1. Evaluation of medicines used during surgical
procedures (e.g., neuromuscular blocking agents)
2. Evaluation of disease treated either by surgery or
medicines(e.g., angina, peptic ulcers)
3. Evaluation of a disease(e.g., cancer) treated either
by surgery or nonmedical modalities(e.g., radiation,
hyperthermia)
4. Comparison of surgical procedures (e.g., new
versus old method, modified versus original
method)

Trials with Surgical Procedures
5. Evaluation of one surgical procedure (usually a novel
technique) compared with historical controls
6. Comparison of a surgical procedure performed with
and without medical adjunct therapy(neoadjuvant or
adjuvant treatment)
7. Evaluation of equipment used in surgery(e.g.,
stereotaxic device, prosthetic heart valves), either
used or implanted during surgical procedures
8. Evaluation of surgical materials (e.g., adhesives,
suture materials, pins, staples) used during surgery

외과 / 타과와의 임상시험
• Comparison of procedures
• new method vs. old method
• modified method vs. original method
• Methods :
– Lumpectomy, TEM, laparoscopic surgery, VATS, EMR
• Modality :
– Neoadjuvant study, Adjuvant study
Considerations in Surgical Trials
1. Preoperative period
• Premedication : doses, time of administration
• Preparation : bowel prep, patient’s diet, exercise
2. During surgery
• Anesthetic(s), neuromuscular blocking agent
• Specific instrumentation and equipment
3. Postoperative period
• Postoperative care and monitoring
• Outpatient or inpatient care

Considerations in Surgical Trials
• Training and technique of personnel
– Surgeons and the rest of the surgical
team(e.g., fellows, residents, PA,
anesthesiologists, pathologists, scrub
team)
– Training of the techniques
– Single surgeon or a group of surgeons
– Single or group of anesthesiologists
– Replacing surgeon with another surgeon

Parameters with Surgery
• During Surgery
– Technical ease or difficulty of procedure
– Amount of practice to perfect technique
– Duration of surgery
– Rate and nature of severe complications
– Number and expertise of staff required

Parameters with Surgery
• After Surgery
– Morbidity and/or mortality rates
– Improvements of endpoints : • Clinical e.g., recurrence, survival
• Cosmetic
• Performance
– Length of hospital stay
– Total Cost
– QOL
• Independent Review

임상시험에서 내과와 외과의 차이
• 내과계
– 치료를 위하여 여러 번 치료
– 진단, 치료법은 같다.
– 같은 약을 투여한다.
– 내과적인 care 에서의 차이가 있다
• 부작용에 대한 supportive care
• 병발하는 질환에 대한 지식과 대처
• 계속 치료할 것이냐 말 것이냐의 결정
임상시험에서 내과와 외과의 차이
• 외과계
– 한 번의 수술로 이루어지며 비가역적이다.
– 새로운 수술법을 기존의 data 와 비교한다(historical control).
– Randomized study ?
• Surgeon Thinks
– Shame vs. Fame

우리의 전략
• 참여할 기회가 있으면 참여한다.
• 본인이 idea 를 제시한다.
• 다른 과를 참여시킨다.
• 다른 과의 임상시험을 도와준다.
• CRC 를 확보한다.
• IRB 에 참여한다.