access to medical care depending on the employment … · welfare regimes and healthcare systems...
TRANSCRIPT

Access to Medical Care Depending on the Employment
Status and History of Unemployment in different
welfare regimes and healthcare systems
First draft June 2016
Ave Roots
University of Tartu
First draft prepared for session “Health, labour markets & (un)employment II”
in the European Social Survey Conference “Understanding key challenges for
European societies in the 21st century“ in Lausanne 13-15th July 2016.
Please do not quote or cite without permission of the authors.
Contact:
Ave Roots, University of Tartu, [email protected]

2
Abstract
Health inequalities between employed and unemployed have been widely studied and found
that unemployed have systematically lower health status. Inequalities in access to health care
depending on the employment status have not been studied that much. Different welfare
regimes and health care systems both play their role as mediators between employment status
and access to health care. Using the gradual approach of employment status between
employed and unemployed, the group of employed was divided into those with the experience
of unemployment and those without it.
In 2014 European Social had the special health inequalities block and it has been utilised in
current study. European Social Survey data shows that employed with the experience of
unemployment are in several countries more likely not to get medical consultation or
treatment in case of need compared to the employed who have never been unemployed,
whereas the last group often does not differ from unemployed. The worse access to medical
care of the employed with unemployment history is associated with worse working conditions
compared to those who have not been unemployed in Estonia, Great Britain, Ireland, Poland
and Portugal. These countries have strict access restrictions on the primary level of health care
and the Anglo-Saxon and the Eastern-European countries also have more liberal labour
markets and that amplifies the differences between mentioned groups on the labour market.
Keywords: access to health care, impact of unemployment, health care systems, welfare state

3
Introduction
Unequal access to medical care is one of the factors that influence socioeconomic inequality
in health. If people who have a disadvantaged position on the labour market, have also worse
access to medical care, it leads to multidimensional accumulation of disadvantages.
Virtanen et al. (2006) have found that there is rather gradual and not strict difference between
employed and unemployed in terms of health care utilization, the marginal groups on the
labour market (employees with fixed term contracts) are doing worse than employees with
permanent contracts and the health care utilization is the lowest among unemployed. This
article compares the access to medical care based on unmet need between different groups
according to their unemployment experience (currently unemployed, employed with the
experience of unemployment as a more marginal group on the labour market and employed
with no previous unemployment experience).
The purpose of this article is to study how the position on the labour market is associated with
the access to the medical care in case of need and how health care systems and welfare state
types moderate this association.
Unemployment and health
The association between unemployment and worse health outcomes compared to the
employed has been well documented. For example Bambra and Eikemo (2008) study the
impact of unemployment in different welfare regimes. Unemployment had the most negative
effect on women in Anglo-Saxon and Scandinavian regimes. Inequality between employed
and unemployed was the greatest in Anglo-Saxon regime, but also for men in Bismarkian and
women in Scandinavian regime, the smallest difference between employed and unemployed
was among Southern women. In Anglo-Saxon countries there is the greatest income
deprivation and stigmatisation (means tested benefits). In Bismarkian familial approach men

4
are more treated as breadwinners. The authors claim that in Scandinavia many women work
part time and do not meet the benefits criteria and therefore there is much income inequality
between working and not working women. The small differences in Southern regime can be
explained by traditional family model and additional resources by the family.
Long term unemployment has become a stronger predictor of healthy life years at the age of
50 in European countries between 2005 and 2010 (Fouweather et al. 2015).
Unemployment and the access to health care
Access to health care be measured based on health care utilisation as it is done very often or
based on unmet need, which is individuals’ subjective assessment that they did not receive the
needed health care (Allin, Grignon, and Le Grand 2010:465). EU-SILC 2004 data show that
of the surveyd countries the highest unmet need was perceived in Sweden (13%), followed by
Estonia (11%) and Italy (%) and the lowest proportion of people with unmet need was in
Denmark (1%), Belgium and Austria (2% in both) (Koolman 2007:188). The same study
shows that in the majority of surveyed countries the cost of the services has been hindrance
for access (in Belgium, Greece, Estonia, France, Ireland, Italy and Portugal), waiting list has
been the greatest problem in Spain, Finland and Sweden, having no time in Austria and care
being too far in Norway (Koolman 2007:188).
There is plenty of articles that establish the relationship between unemployment and worse
access to health care in US. In US unemployed are often also uninsured and therefore have
less access to healthcare (Driscoll and Bernstein 2012). There is only some research that
studies the relationship between unemployment and access to healthcare in Europe. In macro

5
level increase of unemployment is connected to worse health outcomes in European Union
countries and the reasons assumed to be worse access to health care for the unemployed
(Maruthappu et al. 2016). In Greece, in 2013, the unemployed with chronic illness were more
likely to experience the economic, but also waiting lists access barrier to health care
(Kyriopoulos et al. 2014). A Swedish study shows that non-employed (people with no
employment income) have lower access to ACE Inhibitors (that reduce mortality and
morbidity from heart failure), even when other factors, including medical literacy are
controlled for (Ohlsson et al. 2016). The same study found that the impact of non-
employment to the choice of medical treatment is more important than material resources and
ability to access and understand medical information. Different treatment of the non-
employed might be associated with their lower status. It has also been found about underclass
in Canada, that they are stereotyped and treated differently than others in medical system
(Tang et al. 2015).
In terms of the utilisation of the mental care there are different results. Alonso et al. (2007)
and Gouwy, Christiaens, and Bracke (2008) have fount that in case of mental health
problems, unemployed seek less often medical care than the employed. However, Buffel, van
de Straat, and Bracke (2015) have found that the unemployed use medical care more than
employed, even regardless of their mental health status.
A Finnish study (Virtanen et al. 2006) shows that the border between employed and
unemployed is not clear-cut. People at margins of the labour market differ from the people at
the core. Permanently employed differ from both, fixed term employed and unemployed in
terms of using dental care and primary care in case of cardiovascular, respiratory and
skeletomuscular disease, permanently employed visit the healthcare specialists most often,
followed by fixed term employed and the least amount of visits are made by unemployed and
the differences between these groups widened after controlling for need (Virtanen et al. 2006).

6
People have unemployment in their work history are not vulnerable only during that moment
of unemployment, but unemployment has a “scarring” effect on their work career later and
can have a negative cumulative outcome during their life course (Layte et al. 2000;
Vandecasteele 2011). The long term negative effects of unemployment during the working
career are lower salaries, more downwards mobility, less upwards mobility compared to the
employed who have not experienced unemployment and also reoccurring unemployment
episodes (Gangl 2006; Layte et al. 2000; McManus and DiPrete 2000; Vandecasteele 2011).
Context: welfare state and health care system
There is a very important mediator between the access to health care and employment status.
It is the institutional context of the state. In this study, the 2 concepts have been chosen to
explain the mediating role of the institutional context. These concepts are welfare state, labour
market type and healthcare system type.
Welfare state has a direct effect to health outcomes but is also a mediator between labour
market status, access to healthcare and health outcomes (Beckfield et al. 2015).
Studying social inequalities in health, several authors cluster countries in 5 welfare regime
types: Scandinavian (Denmark, Finland, Norway, Sweden), Anglo-Saxon (UK and Ireland),
Bismarckian (Germany, France, Austria, Belgium, the Netherlands), Southern (Greece, Italy,
Portugal, Spain) and Eastern-European (Czech Republic, Estonia, Hungary, Poland, Slovenia,
Slovakkia) (Bambra 2009; Bambra and Eikemo 2008; Bambra, Netuveli, and Eikemo 2010;
Eikemo, Bambra, Joyce, et al. 2008; Eikemo, Bambra, Judge, et al. 2008; Eikemo, Huisman,
et al. 2008). Scandinavian regime can be described by universalism, generous transfers, strong
interventionist state and promotion of social equality through social security system; Anglo-
7
Saxon regime has modest social transfers and minimal level of provision and dominance of
the market; Bismarckian regime is characterized by often earnings related benefits,
administration through employer, the role of the family is emphasized and the role of the
market marginalized; Southern welfare regime has strong reliance on family and only
fragmented provision, health care system provides only limited and partial coverage; Eastern-
European system includes post-socialist countries where there have been great reforms with
direction of decentralization and liberalization since the beginning of 90s (Eikemo, Bambra,
Joyce, et al. 2008).
Wendt (2014) divides European countries between 4 main types of healthcare systems. First
type is described by high share of public financing, moderate level of out-of-pocket payments
and very high access regulation. Australia, Denmark, Ireland, Italy, the UK, Czech Republic,
Estonia, Hungary, Poland, the Slovak Republic, Slovenia and the Netherlands can be
described by this type. The second type of healthcare systems have high share of public
financing as well as out-of-pocket payments and high access regulation. The countries in this
type are Finland, Iceland, Portugal, Spain and Sweden. The third type with Greece, Israel and
Turkey can be described by low level of public financing and no control over patients accsess
to medical care. The medical systems in the last group, Austria, Belgium, France, Germany,
Luxembourg, have the highest share of public financing, the lowest share of out-of-pocket
payments and free choice of medical doctors.
Based on this context, it can be hypothesised that first unemployment as a status might play a
greater role in a system with strict gate keeping (like healthcare system types 1 and 2 by
Wendt 2014), because might make their decisions based on the status of the patient and labour
market status makes a contribution in general status. Second, it can be hypothesized, that
unemployment in the past which leads to cumulative disadvantage on the labour market, plays
a greater role in the Anglosaxon and Eastern-European welfare regimes, because less state

8
intervention leads to greater inequality on the labour market (for example less flexible
working conditions, more job insecurity, working contract with no entitlement to health
insurance coverage), which can be a hindrance accessing health care.
Data and methods
European Social Survey (ESS) where the sample are non-institutionalized persons 15 years
old and older. In current study there is only active population (working and unemployed) and
in the regression analysis only those who had need for medical treatment or consultation
during last 12 months. In 2014 there was the special block on health inequalities in ESS.
There was all together 15054 individuals in the analysis. The countries in the analysis were
Austria (781 individuals), Belgium (728), Switzerland (671), Czech Republic (664), Germany
(1429), Denmark (625), Estonia (785), Spain (855), Finland (851), France (840), Great Britain
(829), Hungary (420), Ireland (617), Lithuania (696), The Netherlands (662), Norway (627),
Poland (571), Portugal (517), Sweden (616), Slovenia (405).
The dependent variable in the regression analysis measures whether the respondent was able
to get or was not able to get medical consultation or treatment in case of need.
The central independent variable of interest was labour market status connected to
unemployment (unemployed, currently employed, who have been unemployed and as a
reference category, employed who have never been unemployed).
To further study the wider relationship with labour market, there are some characteristics of
the working conditions in the analysis: the type of the contract (permanent as reference,
compared to fixed and no contract), total working hours normally per week and work
autonomy (to what extent allowed to decide, how daily work is organized, on the scale 0-10).
9
The control variables on the regression models were age, gender, marital status, children at
home, place of residence, ethnic minority, migration background, citizen of country (except in
Czech Republic, Hungary and Poland due to lack of variation), life satisfaction, subjective
health, hampered in daily life, assessment of current household income.
Results
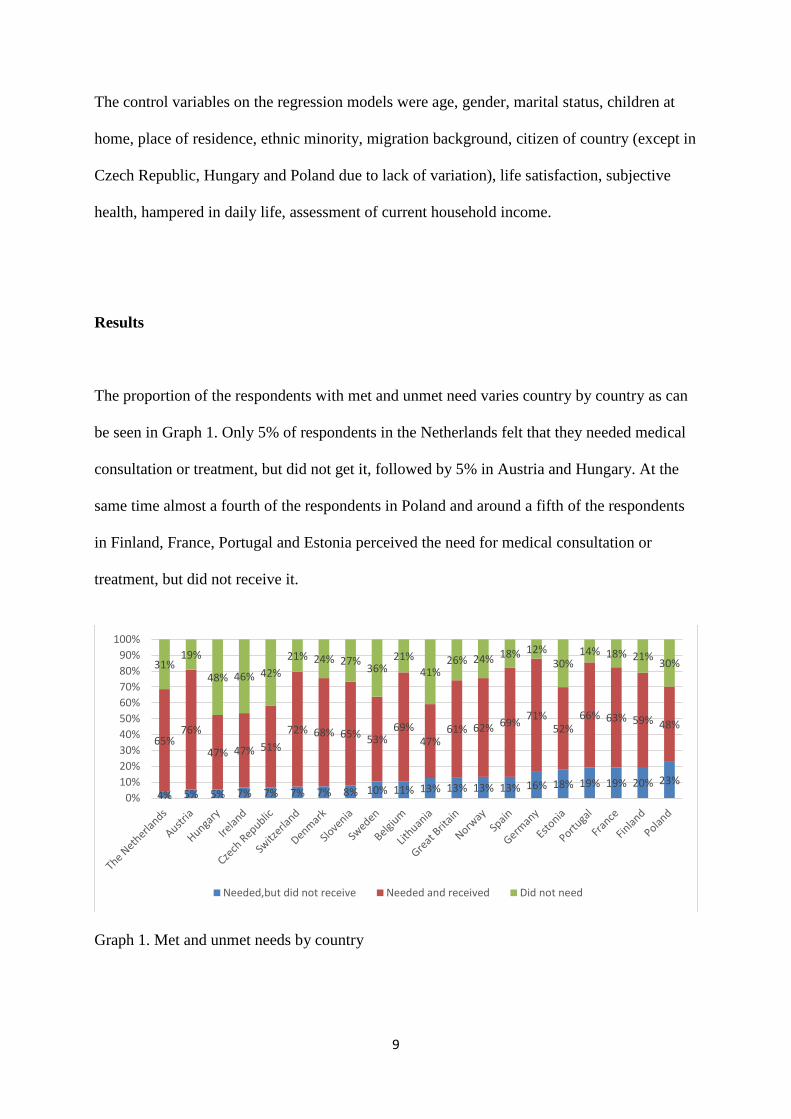
The proportion of the respondents with met and unmet need varies country by country as can
be seen in Graph 1. Only 5% of respondents in the Netherlands felt that they needed medical
consultation or treatment, but did not get it, followed by 5% in Austria and Hungary. At the
same time almost a fourth of the respondents in Poland and around a fifth of the respondents
in Finland, France, Portugal and Estonia perceived the need for medical consultation or
treatment, but did not receive it.
Graph 1. Met and unmet needs by country
4% 5% 5% 7% 7% 7% 7% 8% 10% 11% 13% 13% 13% 13% 16% 18% 19% 19% 20% 23%
65%76%
47% 47% 51%
72% 68% 65% 53%69%
47%61% 62% 69%
71%52%
66% 63% 59% 48%
31%19%
48% 46% 42%
21% 24% 27%36%
21%
41%26% 24% 18% 12%
30%14% 18% 21%
30%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Needed,but did not receive Needed and received Did not need

10
The proportion of respondents with unmet need is broken down by the position on the labour
market on the graph 2.
Graph 2. Proportion of those who needed, but did not get medical consultation or treatment by
employment status.
In France clearly unemployed are the most disadvantaged in terms of getting medical
consultation or treatment, when needed, half of them did not receive it. Also in Finland, like
in France, the unemployed are the most disadvantaged. However in several countries (like
Great Britain, Portugal, Poland, Norway, Lithuania etc) working people with the history of
unemployment are the most disadvantaged one in terms of the access to the health care.
Table 1 presents the results of the regression analysis.
4%6% 6% 6% 7% 7% 8% 9% 10% 10% 11%
15% 16%18%
20% 21% 21%25% 25%
49%
6%
11% 10%
15%
10%
6%
20%
9%
15%
9%11%
19%
18% 19%
26%
21% 21%
20%
30%
23%
3% 5% 6% 12% 5% 3% 12% 8% 4% 4% 10% 12% 15% 9% 21% 18% 15% 16% 14% 20%0%
10%
20%
30%
40%
50%
60%
Currently unemployed Employed, been unemployed Employed, never been unemployed

11
Table 1. Logistic regression predicting not getting medical consultation or treatment in case of
need.
Employment status Working conditions
Country
Unem-
ployed
Employed,
been
unem-
ployed
Fixed-term
contract No contract
Working
hours
Auto-
nomy
B Sig B Sig B Sig B Sig B Sig B Sig
Austria -0.02 0.28
-0.48 0.14 1.59 *** 1.25 0.01 0.01
Belgium 0.29 0.57 *
0.24 0.50 0.49 0.63 -0.01 0.04
Switzer- 0.35 1.37 ***
land -0.07 1.34 *** -0.13 0.62 0.00 -0.06
Czech -0.33 0.42
Republic -0.91 0.21 -0.37 -1.70 0.02 0.08
Germany -0.48 0.08
-0.39 0.08 0.08 -0.56 0.00 0.03
Denmark -0.42 0.24
-0.70 0.19 -0.13 0.1 0.01 -0.07
Estonia 0.32 0.39 *
0.05 0.41 0.34 1.34 0.00 0.07 *
Spain -0.21 0.04
-0.17 -0.03 0.02 -2.83 ** 0.02 * 0.06
Finland 0.14 0.05
0.15 0.05 -0.04 2.56 ** 0.03 * -0.06
France 0.79 ** -0.03
0.82 ** -0.14 -0.13 -0.55 0.02 0.01
Great -0.95 * 0.47 *
Britain -0.91 0.4 0.89 ** 0.42 0.00 -0.08 *
Hungary 0.28 0.26
0.25 -0.14 -1.24 -0.27 -0.03 -0.03
Ireland -0.34 0.81 **
-0.08 0.64 0.30 0.6 0.00 0.07
Lithuania -1.40 * 0.00
-3.03 ** -0.26 0.64 0.27 0.02 -0.11 **
The -0.78 0.52
Netherlands -0.88 0.26 0.64 -1.48 -0.01 -0.08
Norway -0.6 0.39
-0.6 0.31 0.71 0.06 0.03 * 0.00
Poland -0.04 0.39 *
0.05 0.24 -0.49 * 0.48 0.00 0.06
Portugal 0.65 * 1.23 ***
0.96 * 1.08 *** -0.49 0.01 -0.01 0.15 **

12
Sweden -0.16 -0.02
0.12 0.10 -0.13 2.07 * 0.00 0.13 *
Slovenia -0.34 0.34
0.65 0.82 -0.10 2.07 0.05 * 0.03 *** p<0.001; ** p<0.01; * p<0.05
Dependent variable: not receiving or receiving (reference category) medical consultation or treatment in case of
need.
Controls: age, gender, marital status, children at home, place of residence, ethnic minority, migration
background, citizen of country (except in Czech Republic, Hungary and Poland due to lack of variation), life
satisfaction, subjective health, hampered in daily life, assessment of current household income
Table 1 shows that in France and Portugal, unemployed have better access to medical care
than employed who have never been unemployed, but in Lithuania unemployed are
disadvantaged in terms of access to the health care. In Belgium, Estonia, Great Britain,
Ireland, Poland and Portugal, employed with unemployment history were more likely not
getting medical consultation or treatment in case of need, but this association looses statistical
significance after adding working conditions to the model. In case of Portugal having been
unemployed still significantly predicts no access to medical care in case of need, but the
coefficient is somewhat reduced. Adding working conditions to the model does not influence
the association between unmet need and unemployment background in Switzerland. The
concrete working conditions seem to have different influence on the relationship between
access and employment status in different countries.
Discussion and conclusions
Although in the Bismarkian system, the labour market based entitlement to heal care
insurance is more expected, the analysis shows that of the Bismarkian countries, only in
France the unemployed are much more likely to get no medical consultation or treatment in
case of need.

13
Following Virtanen et al. (2006) and dividing the employed into groups, has showd some
important differences between the employed with and without the experience of
unemployment. The employed with the history of unemployment differed in terms of access
to the health care from the employed who had never been unemployed in Belgium,
Switzerland, Estonia, Great Britain, Ireland, Poland and Portugal. In all of these countries
other than Switzerland, difference in working conditions was behind the difference between
employed with and without the experience of unemployment. Going back to the healthcare
system types described by Wendt (2014), all these countries other than Belgium are in types
1(Estonia, Great Britain, Ireland, Portugal, Poland) and 2 (Portugal) according to Wendt 2014
in both of these clusters there is high access regulation.
Gatekeepers can play a role in two ways. First they can be influenced by the unemployment
as a status. The research of Ohlsson et al. (2016) and Buffel et al. (2015) has shown that
unemployment works in medical system as low status compared to employed. Second, people
with the history of unemployment might also possess different characteristics than people
without that experience and these characteristics might play an important role getting through
and around the gatekeepers.
Working conditions play also a role in enabling or disabling access to needed medical care.
First people with less autonomy, higher work strain and longer working hours may encounter
more difficulties to get time off for doctor’s appointment. Also people with the history of
unemployment and temporary or no contract might feel less job security and therefore are
more hesitant to take time off of work for the doctor’s appointment and they also might be
more reluctant to indicate their health problems, not to be seen as less productive due to
health issues. The more liberal and less regulated labour markets in Eastern European and
Anglo-Saxon countries is likely to amplify the inequality of working conditions between the
workers with and without the experience of unemployment.

14
References
Allin, Sara, Michel Grignon, and Julian Le Grand. 2010. ‘Subjective Unmet Need and
Utilization of Health Care Services in Canada: What Are the Equity Implications?’
Social Science & Medicine 70:465–472.
Alonso, Jordi et al. 2007. ‘Population Level of Unmet Need for Mental Healthcare in Europe’.
The British journal of psychiatry 190(4):299–306.
Bambra, Clare. 2009. ‘Welfare State Regimes and the Political Economy of Health’.
Humanity & Society 33(1–2):99–117.
Bambra, Clare and Terje Andreas Eikemo. 2008. ‘Welfare State Regimes, Unemployment
and Health: A Comparative Study of the Relationship between Unemployment and
Self-Reported Health in 23 European Countries.’ Journal of epidemiology and
community health jech–2008.
Bambra, Clare, Gopalakrishnan Netuveli, and Terje Andreas Eikemo. 2010. ‘Welfare State
Regime Life Courses: The Development of Western European Welfare State Regimes
and Age-Related Patterns of Educational Inequalities in Self-Reported Health’.
International Journal of Health Services 40(3):399–420.
Beckfield, Jason et al. 2015. ‘An Institutional Theory of Welfare State Effects on the
Distribution of Population Health’. Social Theory & Health 227–244.
Buffel, Veerle, Vera van de Straat, and Piet Bracke. 2015. ‘Employment Status and Mental
Health Care Use in Times of Economic Contraction: A Repeated Cross-Sectional
Study in Europe, Using a Three-Level Model’. Int J Equity Health 14(1):29.
Driscoll, Anne K. and Amy B. Bernstein. 2012. Health and Access to Care among Employed
and Unemployed Adults: United States, 2009-2010. US Department of Health and
Human Services, Centers for Disease Control and Prevention, National Center for
Health Statistics. Retrieved 4 March 2016
(http://198.246.124.22/nchs/data/databriefs/db83.pdf).
Eikemo, Terje Andreas, Clare Bambra, Ken Joyce, and Espen Dahl. 2008. ‘Welfare State
Regimes and Income-Related Health Inequalities: A Comparison of 23 European
Countries’. The European Journal of Public Health 18(6):593–599.
Eikemo, Terje Andreas, Clare Bambra, Ken Judge, and Kristen Ringdal. 2008. ‘Welfare State
Regimes and Differences in Self-Perceived Health in Europe: A Multilevel Analysis’.
Social Science and Medicine 66(11):2281–95.
Eikemo, Terje Andreas, Martijn Huisman, Clare Bambra, and Anton E. Kunst. 2008. ‘Health
Inequalities according to Educational Level in Different Welfare Regimes: A
Comparison of 23 European Countries’. Sociology of health & illness 30(4):565–582.
Fouweather, Tony et al. 2015. ‘Comparison of Socio-Economic Indicators Explaining
Inequalities in Healthy Life Years at Age 50 in Europe: 2005 and 2010’. The
European Journal of Public Health ckv070.
15
Gangl, Markus. 2006. ‘Scar Effects of Unemployment: An Assessment of Institutional
Complementarities’. American Sociological Review 71(6):986–1013.
Gouwy, Anneleen, Wendy Christiaens, and Piet Bracke. 2008. ‘Mental Health Service Use in
the General Belgian Population: Estimating the Impact of Mental Health and Social
Determinants’. Arch Public Health 66(2):50–68.
Koolman, Xander. 2007. ‘Unmeet Need for Health Care in Europe’. Pp. 181–19 in
Proceedings of the EU-SILC conference, Comparative EU statistics on Income and
Living Conditions: Issues and Challenges. Retrieved 28 June 2016
(https://www.researchgate.net/profile/Paul_Van_Der_Laan2/publication/269649087_
The_Income_Concept_in_EU-
SILC_Relevance_Feasibility_Challenges/links/54cb51c10cf2517b75617fe5.pdf#page
=181).
Kyriopoulos, Ilias-Ioannis et al. 2014. ‘Barriers in Access to Healthcare Services for Chronic
Patients in Times of Austerity: An Empirical Approach in Greece’. Int. J. Equity
Health 13. Retrieved 13 June 2016 (http://www.biomedcentral.com/content/pdf/1475-
9276-13-54.pdf).
Layte, Richard, Hendrik Levin, John Kendrickx, and Ivano Bison. 2000. ‘Unemployment and
Cumulative Disadvantage in the Labour Market’. Pp. 153–74 in Welfare Regimes and
the Experience of Unemployment in Europe, edited by D. Gallie and S. Paugam.
Oxford: Oxford University Press.
Maruthappu, Mahiben et al. 2016. ‘Unemployment, Public-Sector Healthcare Expenditure
and Colorectal Cancer Mortality in the European Union: 1990–2009’. International
journal of public health 61(1):119–130.
McManus, Patricia A. and Thomas A. DiPrete. 2000. ‘Market, Family, and State Sources of
Income Instability in Germany and the United States’. Social Science Research
29:405–440.
Ohlsson, Anna, Bertil Lindahl, Marianne Hanning, and Ragnar Westerling. 2016. ‘Inequity of
Access to ACE Inhibitors in Swedish Heart Failure Patients: A Register-Based Study’.
Journal of epidemiology and community health 70(1):97–103.
Tang, Sannie Y., Annette J. Browne, Bill Mussell, Victoria L. Smye, and Patricia Rodney.
2015. ‘“Underclassism”and Access to Healthcare in Urban Centres’. Sociology of
health & illness 37(5):698–714.
Vandecasteele, Leen. 2011. ‘Life Course Risks or Cumulative Disadvantage? The Structuring
Effect of Social Stratification Determinants and Life Course Events on Poverty
Transitions in Europe’. European Sociological Review 27(2):246–263.
Virtanen, Pekka, Mika Kivimäki, Jussi Vahtera, and Markku Koskenvuo. 2006. ‘Employment
Status and Differences in the One-Year Coverage of Physician Visits: Different Needs
or Unequal Access to Services?’ BMC Health Services Research 6(1):1.
Wendt, Claus. 2014. ‘Changing Healthcare System Types’. Social Policy & Administration
48(7):864–82.

16