case presentation ethan
TRANSCRIPT
Controversies in
Hypertrophic Cardiomyopathy:
Case Presentation
Ethan Rowin, MD
Associate Director, Hypertrophic Cardiomyopathy Center
Tufts Medical Center, Boston MA
Chanin T. Mast Center for Hypertrophic Cardiomyopathy
Morristown Medical Center, Morristown NJ
HCM Case Presentation
• 40-year-old male with HCM referred for management of progressive heart failure symptoms over the past 3 years.
• Limiting exertional dyspnea (stairs and gradual inclines; NYHA Class II) and atypical chest pain despite Toprol XL 150mg.
• In addition, severe post-prandial SOB resulting in significant limitation, even walking on level ground (class III); and 30 pound weight loss
• One syncopal episode, 1 year prior, occurred with exertion, 30 minutes after ingestion of a large meal

Past Medical History
• Atypical chest pain prompted cardiac catheterization
which demonstrated no CAD
• No other significant medical history
• Employed as a transporter of raw materials
• No family history of HCM or unexplained sudden death
• 14 year-old asymptomatic daughter underwent a recent
screening echocardiogram without LV hypertrophy
• No NSVT on 24 hour Holter monitoring

Exercise
Echocardiogram…

Echocardiogram at Rest
Parasternal Long-Axis Apical 4-Chamber
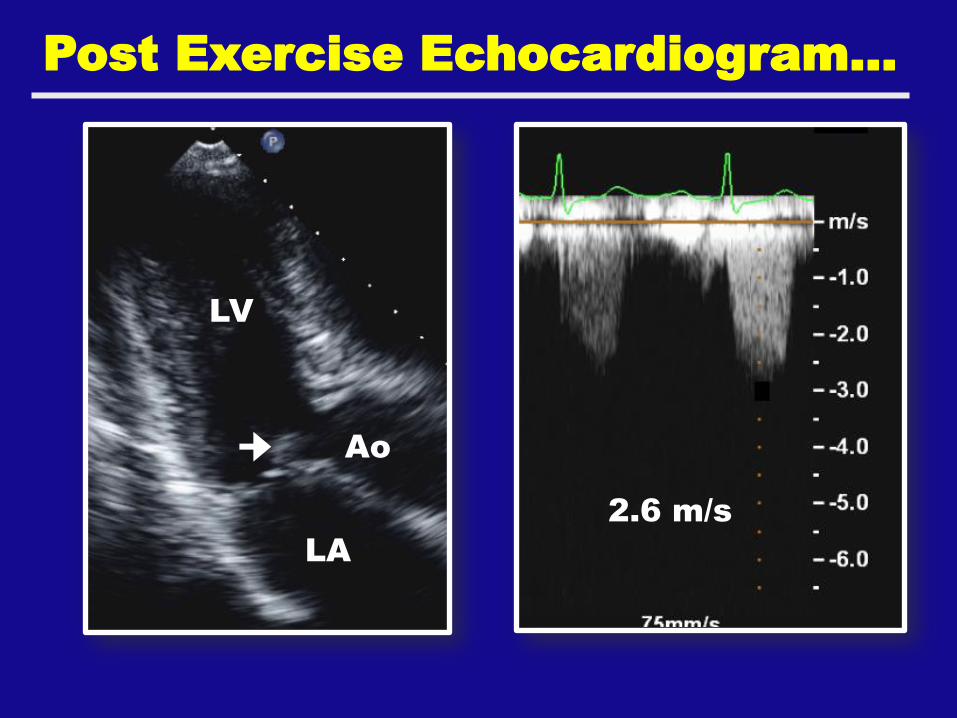
Post Exercise Echocardiogram…
LV
LA
Ao
2.6 m/s

Cardiac MRI…
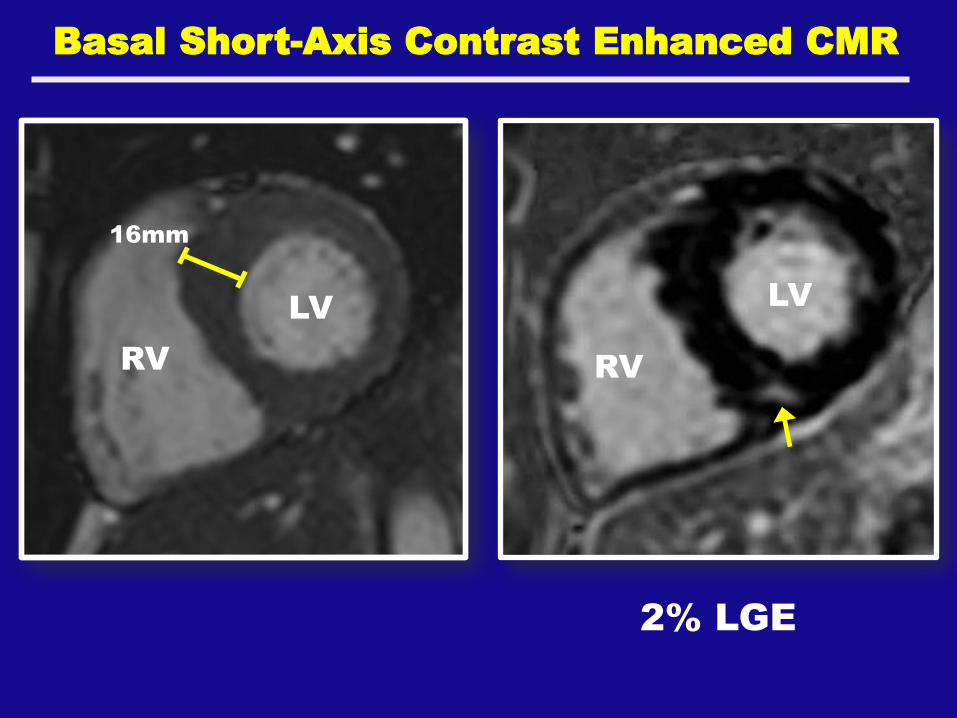
16mm
LV
RV
LV
RV
2% LGE
Basal Short-Axis Contrast Enhanced CMR

HCM Case
• Maximum LV wall thickness of 16mm
• Ejection Fraction of 60%
• SAM at rest and with exercise but no LVOT
obstruction
• Trace mitral regurgitation
• Normal BP response to exercise
• Minimal LGE on CMR (2% of LV myocardium)
• MYPC3 Arg502Trp positive pathogenic mutation
What is the next step?
1. Evaluation/ management of his
symptoms
2. Risk stratification
3. Family Screening

Exercise echo was
repeated several days
later off medications for
24 hours and one hour
after a small meal…

6:00 minutes on Bruce Protocol…
Mild MR 130 mmHg
LV
LA
Ao

Management
• Initially not interested in moving forward with invasive option
• Started on Disopyramide…
• Limiting symptoms improved for several months before eventually recurred
• An exercise echocardiogram was repeated which confirmed prior findings
• At this point patient elected to move forward with invasive option…

Management
• Alcohol Septal Ablation
• Surgical Myectomy
• Mitral valve replacement
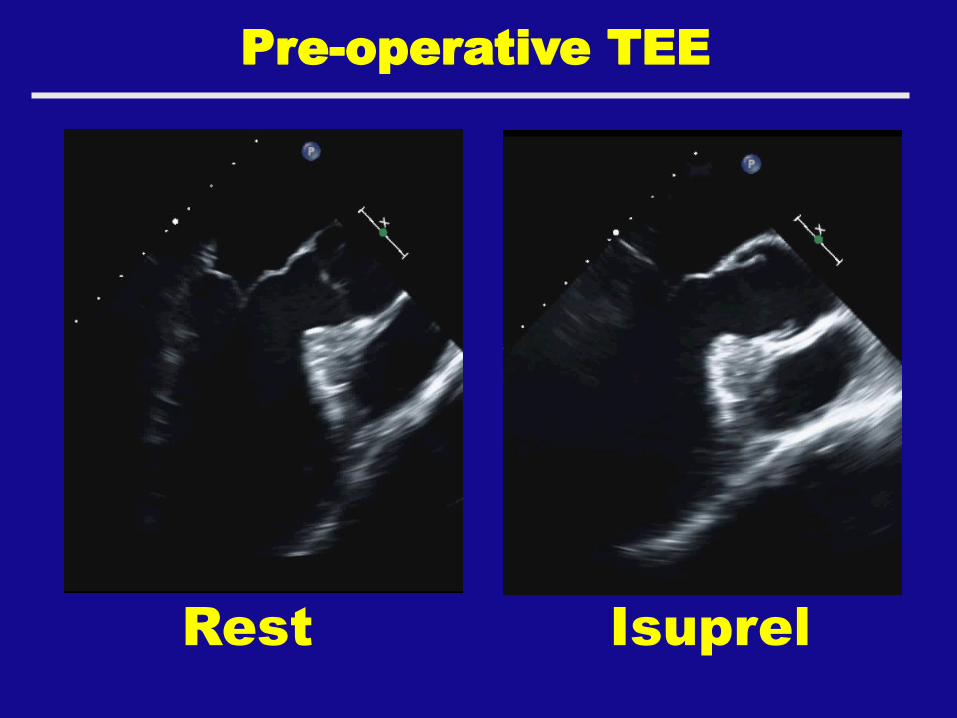
Pre-operative TEE
Rest Isuprel

Pre-operative TEE
Isuprel Isuprel
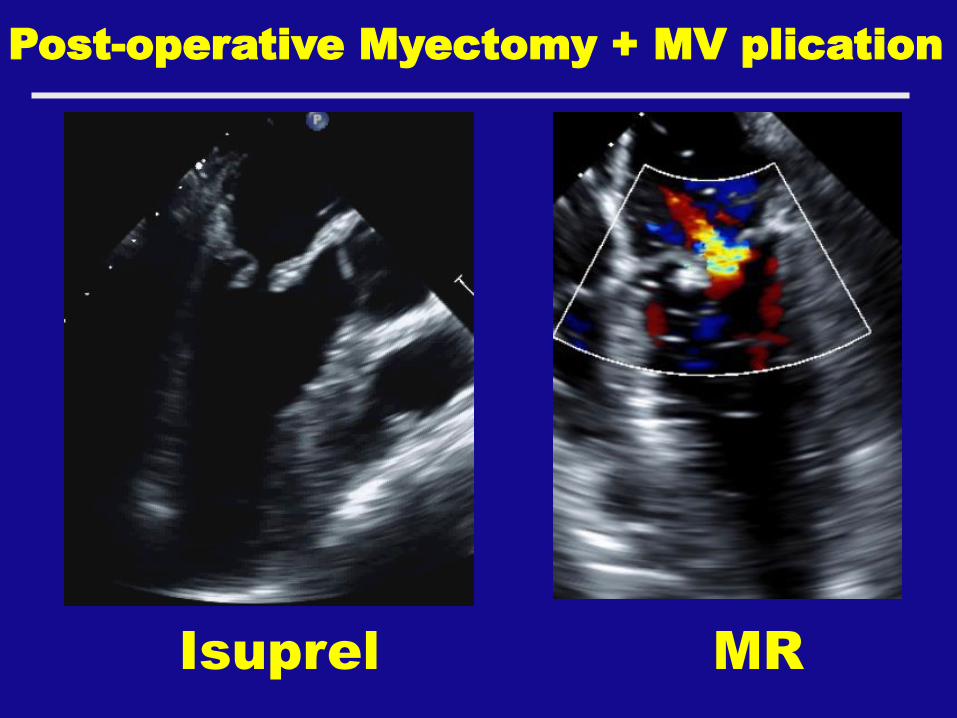
Post-operative Myectomy + MV plication
Isuprel MR

One Year Later…
Asymptomatic… Able to eat all
foods without symptoms. Very
happy with his improved quality
of life.
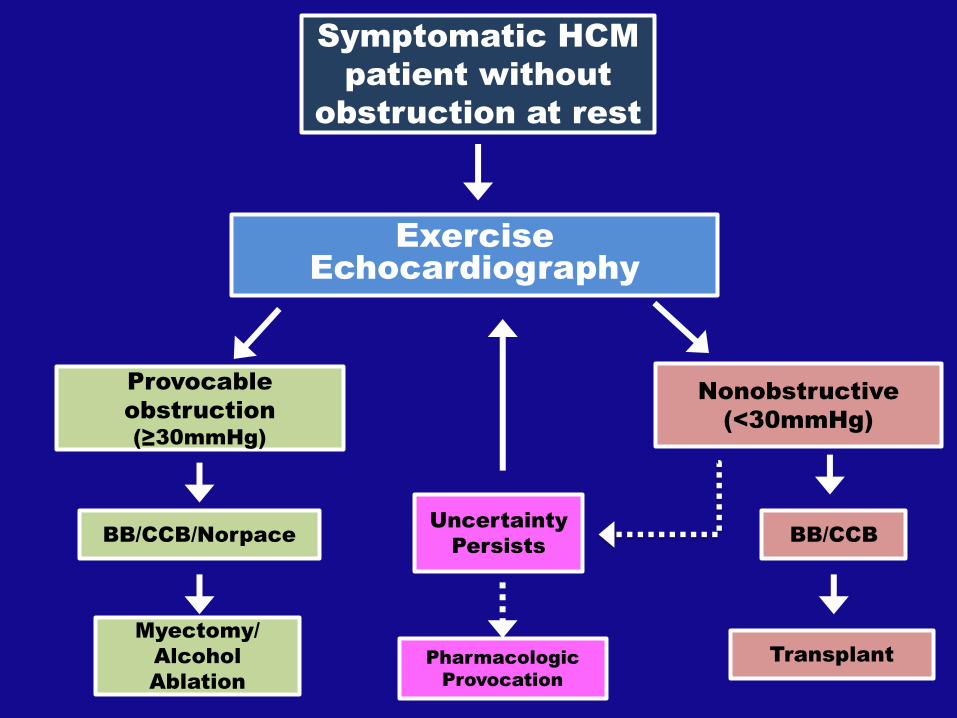
Symptomatic HCM
patient without
obstruction at rest
Exercise
Echocardiography
Provocable
obstruction
(≥30mmHg)
Nonobstructive
(<30mmHg)
Myectomy/
Alcohol
Ablation
Uncertainty
Persists BB/CCB/Norpace
Pharmacologic
Provocation
Transplant
BB/CCB
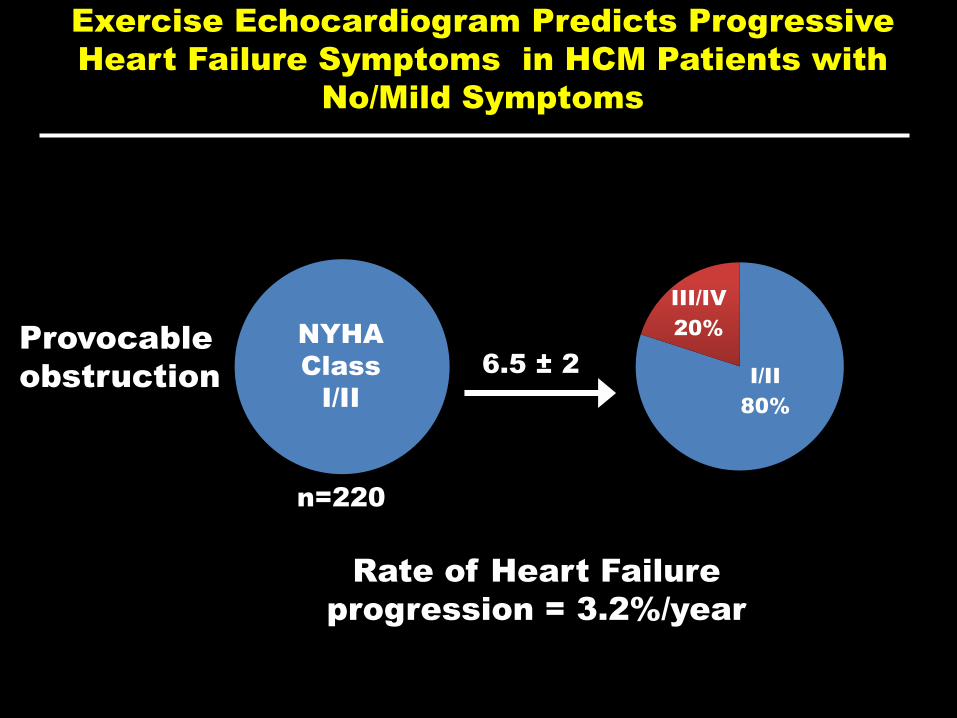
Provocable
obstruction
n=220
I/II
80%
III/IV
20% NYHA
Class
I/II
6.5 ± 2
Rate of Heart Failure
progression = 3.2%/year
Exercise Echocardiogram Predicts Progressive
Heart Failure Symptoms in HCM Patients with
No/Mild Symptoms

What is the next step?
1. Evaluation/ management of his
symptoms
2. Risk stratification
3. Family Screening

Sudden Death Risk Assessment
• Maximum LV wall thickness = 16mm
• Ejection Fraction of 60%
• Unexplained Syncope 2 years ago
• Normal BP response to exercise
• No FH of SD due to HCM
• No NSVT on Holter
• MYPC3 Arg502Trp positive pathogenic mutation
• CMR with 2% LGE
Family evaluation
• Underwent genetic testing which returned positive for MYPC3 Arg502Trp positive pathogenic mutation
• He has an asymptomatic 14 year old daughter who has had a recent echocardiogram without LV hypertrophy
• Next step in the approach to screening his family?


0.50
0.60
0.70
0.80
0.90
1.00
Free
do
m f
rom
Pro
gres
sio
n t
o
NYH
A C
lass
III/
IV
0 2 4 6 8 10
Time from Initial Visit (years)
p=.003
Nonobstructive
Provocable Obstruction
1.5%/yr
3.2%/yr
0.40
Exercise Echocardiogram Predicts Progressive
Heart Failure Symptoms in HCM Patients with
No/Mild Symptoms
Family evaluation
• Underwent genetic testing which
returned positive for MYPC3 Arg502Trp
positive pathogenic mutation
• He has a 14 year old daughter who has
had a recent echocardiogram without
LV hypertrophy
• Next step in the approach to
screening his family?

Non-
obstructive
Provocable
obstruction
n=220
I/II
90%
III/IV
10%
I/II
80%
III/IV
20%
NYHA Class
n=249
NYHA
Class
I/II
NYHA
Class
I/II
6.5 ± 2
6.5 ± 2
1.5%/year
3.2%/year
p=0.003
Exercise Echocardiogram Predicts Progressive
Heart Failure Symptoms in HCM Patients with
No/Mild Symptoms
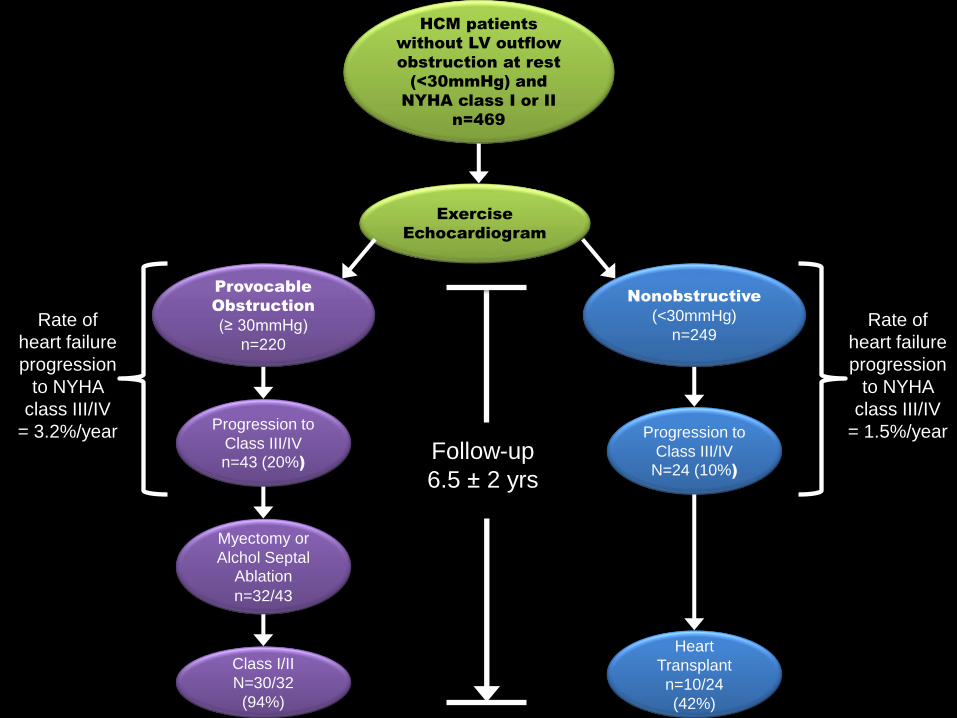
HCM patients
without LV outflow
obstruction at rest
(<30mmHg) and
NYHA class I or II
n=469
Exercise
Echocardiogram
Provocable
Obstruction
(≥ 30mmHg)
n=220
Progression to
Class III/IV
n=43 (20%)
Myectomy or
Alchol Septal Ablation
n=32/43
Class I/II
N=30/32
(94%)
Nonobstructive
(<30mmHg)
n=249
Progression to
Class III/IV
N=24 (10%)
Heart
Transplant
n=10/24
(42%)
Follow-up
6.5 ± 2 yrs
Rate of
heart failure
progression
to NYHA
class III/IV
= 1.5%/year
Rate of
heart failure
progression
to NYHA
class III/IV
= 3.2%/year

Outflow obstruction can be effectively relieved with
myectomy even in HCM patients with minimal hypertrophy
without need for MV replacement…
Table 1. Demographic and Clinical Variables of 22 HCM Patients with Minimally
Increased Left Ventricular Wall Thickness who Underwent Surgery
Age at myectomy, yrs 56 ± 10
Male, n (%) 13 (59%)
Time between diagnosis and surgery, months 23 ± 31
Family history of HCM, n (%) 7 (32%)
NYHA class at time of surgery:
Class III
Class IV
19 (86%)
3 (14%)
Max basal septal thickness (mm) 13.7 ± 1.7
LA size (mm) 40 ± 5.2
LVED (mm) 42 ± 4.9
Ejection Fraction (%) 64 ± 4
LVOT gradient at rest or provocation:
Rest LVOT gradient, mm Hg 91 ± 34
Range LVOT gradient, mm Hg 50-160
Mitral regurgitation: n (%)
Trace-Mild 17 (77%)
Moderate-Severe 5 (23%)
Pre-Op
Gradient/MR
100±35 mmHg
Mild MR (n=9)
Post-Op
Complications
Post-Op
Gradient/MR
Complete Heart Block
(n=3*)
6±2 mmHg
Mild MR (n=9)
*1 patient with pre-op right bundle branch block
93±34 mmHg
Mild-Mod MR (n=10)
Severe MR (n=2) Complete Heart Block (n=1)
Tamponade (n=2)
6±1 mmHg
Mild MR (n=12)
60 mmHg
Mild MR
None
9 mmHg
Mild MR

Should this patient be
considered for primary
prevention ICD
placement?
Surgical Approach?
• Extended Myectomy
• Myectomy plus MV repair (plication)
• Mitral valve replacement