利用電腦導引植入四支植體合併立即負載重建 上顎:兩年追蹤病例報告與...
TRANSCRIPT
- 28 -
Taiwan J Oral Maxillofac Surg 台灣口外誌Taiwan J Oral Maxillofac Surg29: 28-42, March 2018 台灣口外誌
引 言
上顎全口無牙患者,植體支持固定贋復物
所需最佳的植體數目至今仍無共識。在1980年
代,Branemark認為重建下顎無牙患者六支植體
為黃金準則,可支撐跨弓固定贋復物1,但近年
仍有學者提倡需要6-12支植體支持上顎跨弓固
定贋復物2–4。
然而自1990年來,已被證實減少植體數目
來支撐固定贋復物是可行的5。Agliardi利用六支
植體立即負載上顎跨弓固定贋復物,3年追蹤
成功率高且臨床結果穩定,是一個可預測性高
且節省花費和縮短時間的治療選擇6。自2003年
Malò團隊7, 8 先後提出“all-on-4 concept"僅利
用4支植體並立即負載,重建上下顎全口無牙患
者。“All-on-4 concept"運用傾斜植體來減少
懸臂程度,和閃避上顎竇及下齒槽神經,縮短
治療時程,植體和贋復物在長期追蹤中皆有相
當高的成功率9, 10。
近年來,電腦輔助植體植入系統已發展更
為精良,讓術前計畫更有效率且植體植入更安
全,亦可同時考量到未來贋復物製作。治療概
利用電腦導引植入四支植體合併立即負載重建
上顎:兩年追蹤病例報告與文獻回顧
黃健瑜 龍萱 歐陽玲 吳友仁
高雄長庚醫院牙周病科
摘 要
上顎無牙患者若藉由傳統的植牙手術,到最終贋復物完成,需要等待補
骨與植體骨整合時間。這段時間內,病人通常沒有任何贋復物或是需要配
戴活動義齒。且因術後傷口照護及在不影響補骨結果前提下,贋復物常需
要調整,因此會增加病人咀嚼功能和社交上的許多不便。利用“all-on-4
concept”可以免除補骨步驟,手術立即提供患者一個美觀的、具功能的全顎
固定式贋復物。
本次文獻回顧藉由上顎全部缺牙的患者之病例討論開始,其接受電腦輔助
不翻瓣植牙手術並立即負載,透過電腦斷層掃描、電腦輔助治療計畫訂定、
以及兩次掃描方式,讓醫師在術前可以透過3D影像了解軟組織與硬組織的關
係,精確的計畫出植牙的位置,並且在術前藉由電腦設計出的植牙位置,來
翻製以植體支持的臨時全壓克力樹脂義齒。經過三個月骨整合,印模製作正
式鈦金屬基底固定式義齒。術後每三個月回診維護清潔植體周圍;目前追蹤
二年,植體周圍軟組織健康穩定。文中並回顧電腦導引式植牙手術相關研究
文獻,了解目前電腦輔助系統發展程度與探討臨床的實用性。
關鍵詞:上顎骨,電腦導引式,立即負載。

- 29 -
台灣口外誌 利用電腦導引植入四支植體合併立即負載重建上顎:兩年追蹤病例報告與文獻回顧
念是藉由電腦斷層攝影掃描同時取得預先排列
的牙齒位置和患者的齒槽骨結構11,電腦整合
後輸出製成手術模板。此模板可以精準引導鑽
頭和植體植入,且可預先製作手術後的立即臨
時固定贋復物。
本病例報告利用“all-on-4 concept"電腦
導引植入二支傾斜植體與二支軸向植體(axially
oriented implant)支持上顎贋復物並立即負載,
提出討論並探討相關文獻。
病例報告
81歲男性有置放冠狀動脈血管支架病史,
平日有定時服用口服抗凝血劑,但經血液測
試,無凝血功能異常;患者上顎全口無牙,抱
怨上顎活動假牙易鬆脫且咀嚼食物咬不爛至本
院求診,患者要求為上顎植牙重建。患者下顎
配戴局部活動義齒,左下犬齒和右下犬齒為析
量牙冠(survey crown),左下側門齒為根管治
療後的殘根。左下犬齒為未完全根管治療,在
左下側門齒犬齒根尖有根尖病灶,但患者並未
抱怨下顎義齒有任何不適,且沒有意願重建下
顎。
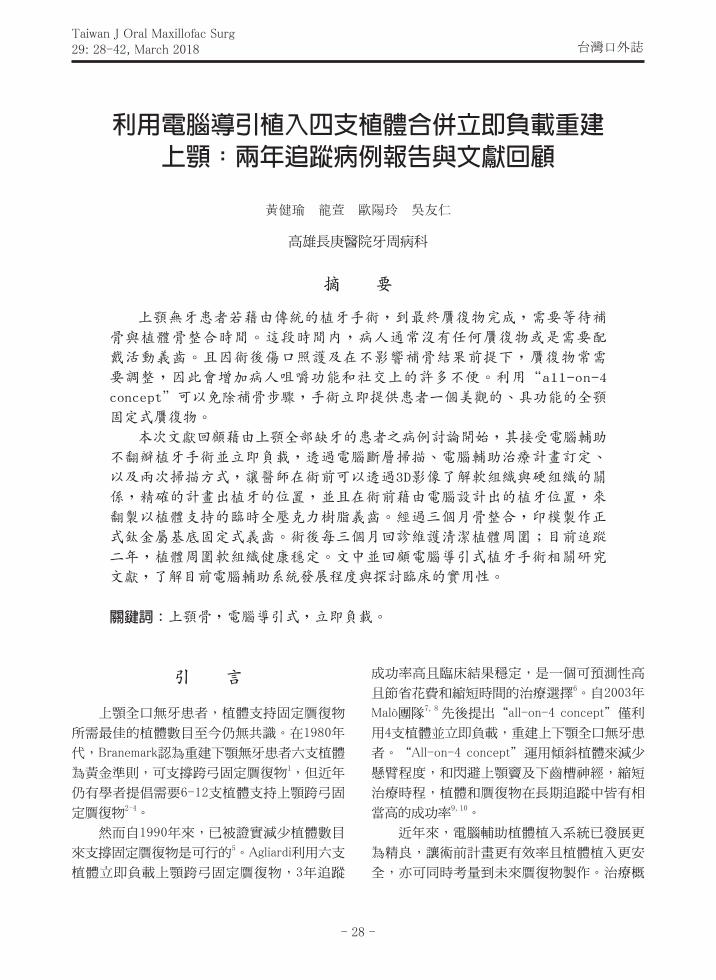
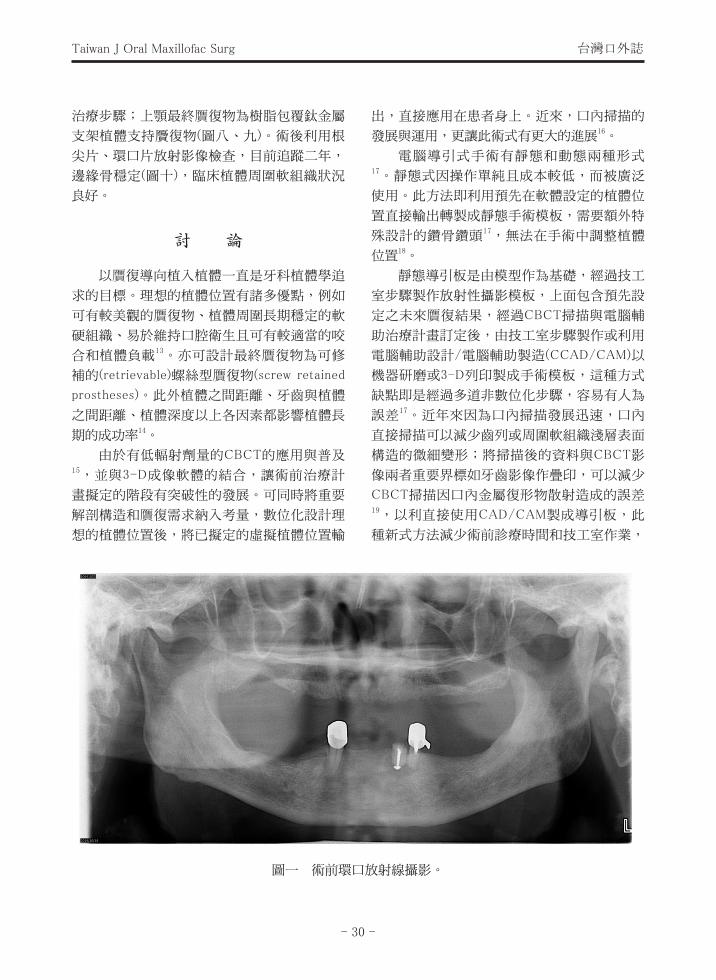
放射影像檢查包括環口片(圖一)及電腦斷
層掃描(圖二)顯示上顎嚴重吸收齒槽骨脊,前
牙區殘存骨脊垂直高度約為12至13 mm,臼齒
區高度不足10 mm。
上顎贋復治療計畫為植體固位覆蓋式義齒
(implant-retained overdenture)或植體支持贋復
物(implant-supported fixed prosthesis),患者選
擇製作植體支持贋復物。根據Bedrossian12 上
顎骨分類及相對應治療計畫,前牙區和小臼齒
區有足夠骨頭。考慮患者年事已高且其不考慮
接受鼻竇增高術與全身麻醉進行手術,遂運用
All-on-4 concept利用傾斜植體和電腦導引不翻
瓣植入植體,省去補骨步驟並立即負載。
將患者舊有上顎活動義齒利用彈性底墊重
新換底墊,並翻製成透明樹脂義齒做為放射線
攝影模板,至少填入6個馬來牙膠球(1 mm)於
透明義齒表面,利用兩次掃描法(double scan
protocol),分別做透明義齒及患者配戴透明
義齒的錐束電腦斷層(cone-beam computerized
tomography, CBCT)的兩次掃描。
經過CBCT掃描後,運用電腦軟體(Nobel
Clinician)依據3-D (three dimensional)解剖結構
和贋復設計數位化設計植體位置和治療計畫,
接著電腦輸出製成依照治療計畫所設計的手術
模板。
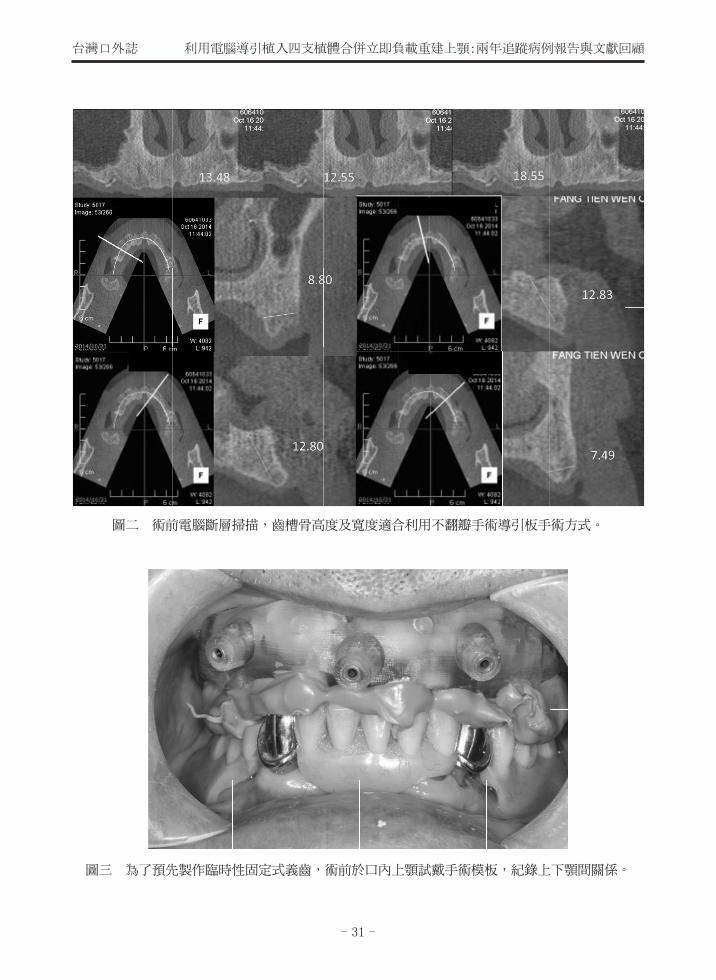
手術前請患者試戴手術模板並和下顎舊有
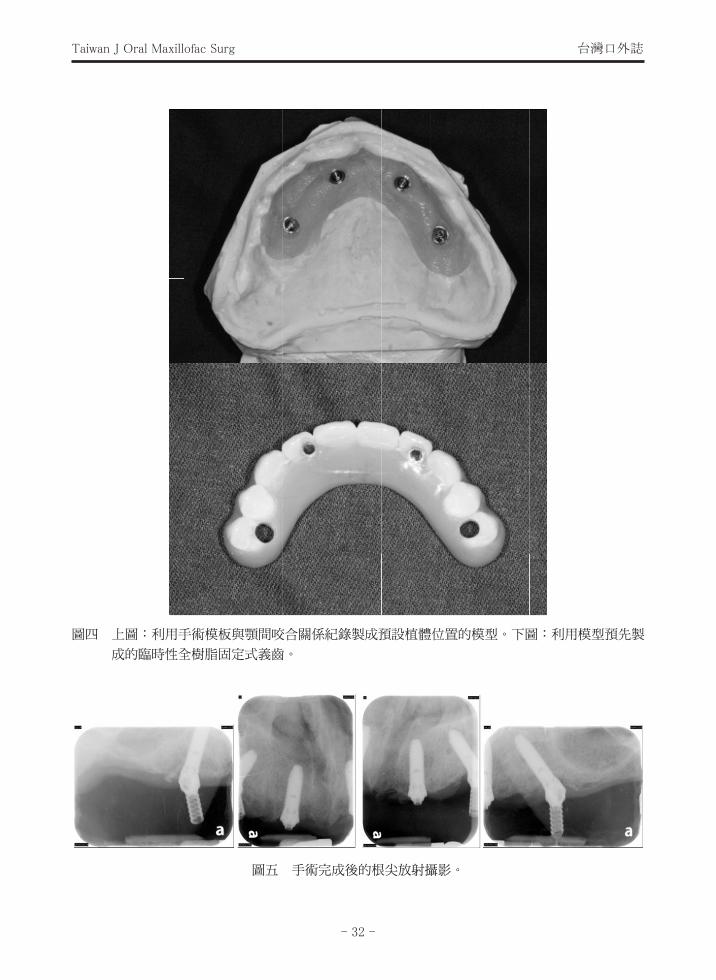
局部活動義齒做咬合紀錄(圖三)。在技工端,
利用手術模板與此咬合紀錄可製成預設植體位
置的模型,並預先製作臨時性全樹脂固定式義
齒(圖四)。為了在植體骨整合期間減少遠心端
懸臂力量,臨時義齒人工牙只排列到第二小臼
齒。
手術在局部麻醉下,將手術導引板利用
咬合指標定位後,於患者咬緊的狀態下植入三
支定位釘,按照術前計畫位置不翻瓣依序於右
上第二小臼齒左上第二小臼齒植入兩支傾斜植
體(4.0 × 15 mm, NobelSpeedy Groovy RP; Nobel
Biocare),於右上側門齒、左上側門齒植入兩隻
軸向植體(4.0 × 15 mm, NobelSpeedy Groovy RP;
Nobel Biocare)四支植體植入初期穩定度扭矩皆
為50 Ncm (圖五)。植體植入後移除手術模板,
依序於右上側門齒、左上側門齒鎖入支台齒
(Multi-Unit abutments; Nobel Biocare AB),接著
利用技工室預先製作的定位篩板(jig)來鎖入右
上第二小臼齒、左上第二小臼齒的30度支台齒
(30-degree Multi-unit non-engaging abutments;
Nobel Biocare AB)。預防原先電腦設定植體位
置與實際臨床位置有誤差,於右上第二小臼
齒、左上第二小臼齒區域利用樹脂臨床將臨時
薄蓋冠(temporary coping)取出,來得到支台齒
最終正確位置。隨即鎖上臨時固定式義齒,並
調整咬合,使其右上犬齒至左上犬齒共6顆牙齒
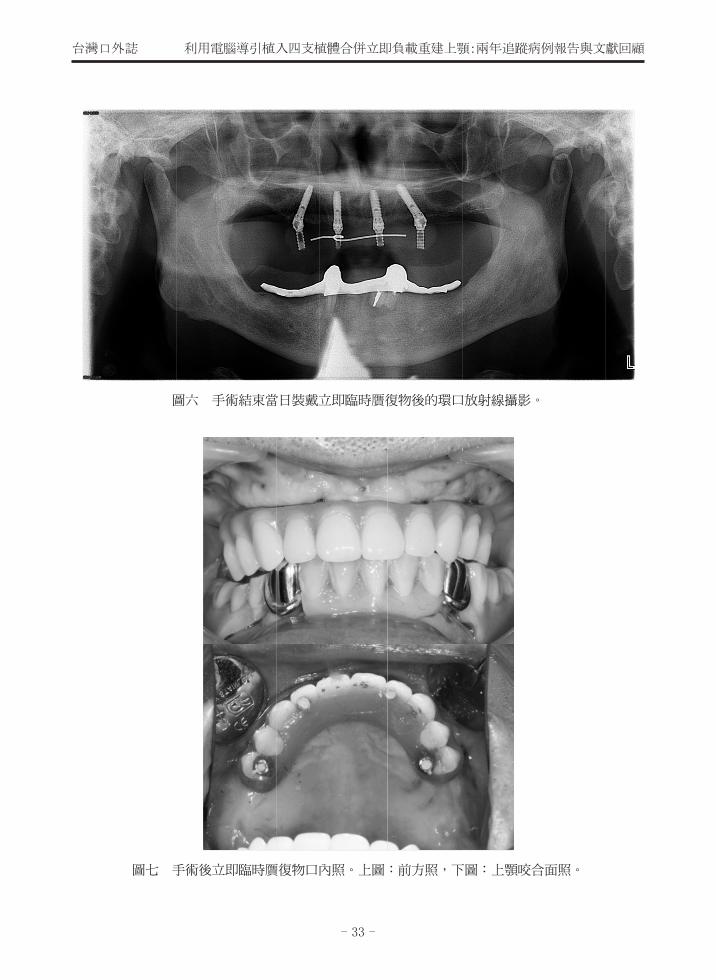
有咬合接觸(圖六、七)。建議病人吃軟質食物
三個月,並定期回診檢查。
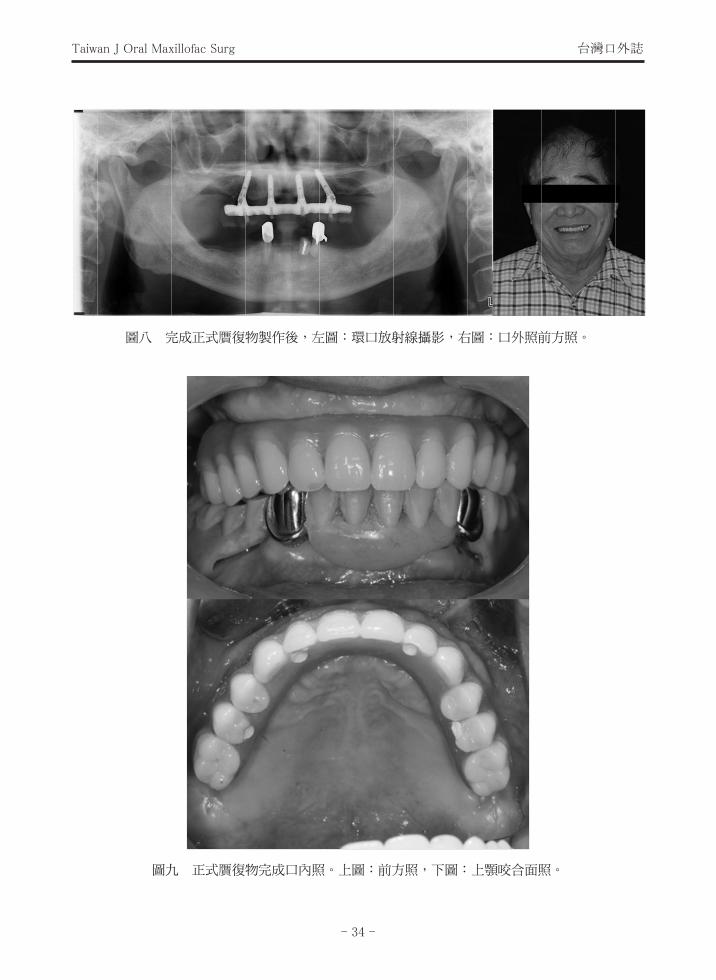
術後等待三個月骨整合後,完成後續贋復
- 30 -
Taiwan J Oral Maxillofac Surg 台灣口外誌
治療步驟;上顎最終贋復物為樹脂包覆鈦金屬
支架植體支持贗復物(圖八、九)。術後利用根
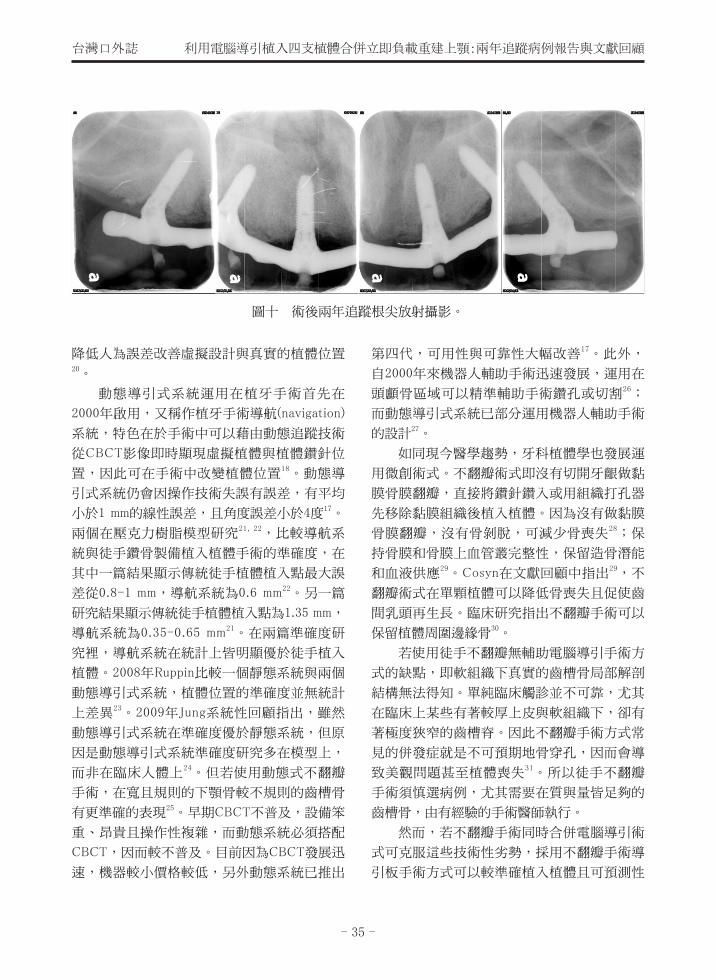
尖片、環口片放射影像檢查,目前追蹤二年,
邊緣骨穩定(圖十),臨床植體周圍軟組織狀況
良好。
討 論
以贋復導向植入植體一直是牙科植體學追
求的目標。理想的植體位置有諸多優點,例如
可有較美觀的贋復物、植體周圍長期穩定的軟
硬組織、易於維持口腔衛生且可有較適當的咬
合和植體負載13。亦可設計最終贋復物為可修
補的(retrievable)螺絲型贋復物(screw retained
prostheses)。此外植體之間距離、牙齒與植體
之間距離、植體深度以上各因素都影響植體長
期的成功率14。
由於有低輻射劑量的CBCT的應用與普及15,並與3-D成像軟體的結合,讓術前治療計
畫擬定的階段有突破性的發展。可同時將重要
解剖構造和贋復需求納入考量,數位化設計理
想的植體位置後,將已擬定的虛擬植體位置輸
出,直接應用在患者身上。近來,口內掃描的
發展與運用,更讓此術式有更大的進展16。
電腦導引式手術有靜態和動態兩種形式17。靜態式因操作單純且成本較低,而被廣泛
使用。此方法即利用預先在軟體設定的植體位
置直接輸出轉製成靜態手術模板,需要額外特
殊設計的鑽骨鑽頭17,無法在手術中調整植體
位置18。
靜態導引板是由模型作為基礎,經過技工
室步驟製作放射性攝影模板,上面包含預先設
定之未來贋復結果,經過CBCT掃描與電腦輔
助治療計畫訂定後,由技工室步驟製作或利用
電腦輔助設計/電腦輔助製造(CCAD/CAM)以
機器研磨或3-D列印製成手術模板,這種方式
缺點即是經過多道非數位化步驟,容易有人為
誤差17。近年來因為口內掃描發展迅速,口內
直接掃描可以減少齒列或周圍軟組織淺層表面
構造的微細變形;將掃描後的資料與CBCT影
像兩者重要界標如牙齒影像作疊印,可以減少
CBCT掃描因口內金屬復形物散射造成的誤差19,以利直接使用CAD/CAM製成導引板,此
種新式方法減少術前診療時間和技工室作業,
圖一 術前環口放射線攝影。
- 31 -
台灣口外誌 利用電腦導引植入四支植體合併立即負載重建上顎:兩年追蹤病例報告與文獻回顧
圖三 為了預先製作臨時性固定式義齒,術前於口內上顎試戴手術模板,紀錄上下顎間關係。
圖二 術前電腦斷層掃描,齒槽骨高度及寬度適合利用不翻瓣手術導引板手術方式。
- 32 -
Taiwan J Oral Maxillofac Surg 台灣口外誌
圖四 上圖:利用手術模板與顎間咬合關係紀錄製成預設植體位置的模型。下圖:利用模型預先製
成的臨時性全樹脂固定式義齒。
圖五 手術完成後的根尖放射攝影。
- 33 -
台灣口外誌 利用電腦導引植入四支植體合併立即負載重建上顎:兩年追蹤病例報告與文獻回顧
圖七 手術後立即臨時贋復物口內照。上圖:前方照,下圖:上顎咬合面照。
圖六 手術結束當日裝戴立即臨時贋復物後的環口放射線攝影。
- 34 -
Taiwan J Oral Maxillofac Surg 台灣口外誌
圖八 完成正式贋復物製作後,左圖:環口放射線攝影,右圖:口外照前方照。
圖九 正式贋復物完成口內照。上圖:前方照,下圖:上顎咬合面照。
- 35 -
台灣口外誌 利用電腦導引植入四支植體合併立即負載重建上顎:兩年追蹤病例報告與文獻回顧
降低人為誤差改善虛擬設計與真實的植體位置20。
動態導引式系統運用在植牙手術首先在
2000年啟用,又稱作植牙手術導航(navigation)
系統,特色在於手術中可以藉由動態追蹤技術
從CBCT影像即時顯現虛擬植體與植體鑽針位
置,因此可在手術中改變植體位置18。動態導
引式系統仍會因操作技術失誤有誤差,有平均
小於1 mm的線性誤差,且角度誤差小於4度17。
兩個在壓克力樹脂模型研究21, 22,比較導航系
統與徒手鑽骨製備植入植體手術的準確度,在
其中一篇結果顯示傳統徒手植體植入點最大誤
差從0.8-1 mm,導航系統為0.6 mm22。另一篇
研究結果顯示傳統徒手植體植入點為1.35 mm,
導航系統為0.35-0.65 mm21。在兩篇準確度研
究裡,導航系統在統計上皆明顯優於徒手植入
植體。2008年Ruppin比較一個靜態系統與兩個
動態導引式系統,植體位置的準確度並無統計
上差異23。2009年Jung系統性回顧指出,雖然
動態導引式系統在準確度優於靜態系統,但原
因是動態導引式系統準確度研究多在模型上,
而非在臨床人體上24。但若使用動態式不翻瓣
手術,在寬且規則的下顎骨較不規則的齒槽骨
有更準確的表現25。早期CBCT不普及,設備笨
重、昂貴且操作性複雜,而動態系統必須搭配
CBCT,因而較不普及。目前因為CBCT發展迅
速,機器較小價格較低,另外動態系統已推出
第四代,可用性與可靠性大幅改善17。此外,
自2000年來機器人輔助手術迅速發展,運用在
頭顱骨區域可以精準輔助手術鑽孔或切割26;
而動態導引式系統已部分運用機器人輔助手術
的設計27。
如同現今醫學趨勢,牙科植體學也發展運
用微創術式。不翻瓣術式即沒有切開牙齦做黏
膜骨膜翻瓣,直接將鑽針鑽入或用組織打孔器
先移除黏膜組織後植入植體。因為沒有做黏膜
骨膜翻瓣,沒有骨剝脫,可減少骨喪失28;保
持骨膜和骨膜上血管叢完整性,保留造骨潛能
和血液供應29。Cosyn在文獻回顧中指出29,不
翻瓣術式在單顆植體可以降低骨喪失且促使齒
間乳頭再生長。臨床研究指出不翻瓣手術可以
保留植體周圍邊緣骨30。
若使用徒手不翻瓣無輔助電腦導引手術方
式的缺點,即軟組織下真實的齒槽骨局部解剖
結構無法得知。單純臨床觸診並不可靠,尤其
在臨床上某些有著較厚上皮與軟組織下,卻有
著極度狹窄的齒槽脊。因此不翻瓣手術方式常
見的併發症就是不可預期地骨穿孔,因而會導
致美觀問題甚至植體喪失31。所以徒手不翻瓣
手術須慎選病例,尤其需要在質與量皆足夠的
齒槽骨,由有經驗的手術醫師執行。
然而,若不翻瓣手術同時合併電腦導引術
式可克服這些技術性劣勢,採用不翻瓣手術導
引板手術方式可以較準確植入植體且可預測性
圖十 術後兩年追蹤根尖放射攝影。
- 36 -
Taiwan J Oral Maxillofac Surg 台灣口外誌
高32, 33,減少術中出血,保存軟硬組織血流供
應,患者術後不適大幅降低,這種手術技巧被
認為可作為傳統翻瓣植體植入的替代方案34。
但利用此術式仍有禁忌症,例如:骨量不足、
殘留牙齒影響術前設計、張口度不足50 mm、
患者有高微笑線(high smile line)或贋復空間不足
需要做截骨術和骨成形術、不規則或過薄的齒
槽脊35,都會增加設計上的困難度而導致事倍
功半。
Tahmaseb在2014年的系統性回顧分析,
14篇關於靜態式電腦導引系統的植體存活率研
究,其中有13篇研究使用不翻瓣手術,12篇合
併立即負載,總數共1,941支植體一年存活率為
97.3%25。Moraschini在2015年的統合分析共分
析14篇研究,在無牙患者使用不翻瓣電腦導引
式植入植體,平均追蹤1-4年,植體存活率為
97.2%,平均邊緣骨喪失為1.45 mm。36
D'haese等學者在2012年的文獻回顧中37,
共收入31篇研究,其中有10篇研究關於電腦導
引式的準確率,結論顯示導引式手術植入植體
較徒手植入更準確。Tahmaseb的系統性回顧
分析中25,24篇是靜態式電腦導引系統準確率
研究,14篇為臨床研究,其餘為模型或大體研
究,其中13篇完全為不翻瓣手術,靜態導引式
手術植入植體較徒手植入準確;不翻瓣手術較
翻瓣來的準確;植體齒槽冠部植入點誤差偏移
為平均為1.12 mm,最大誤差為4.5 mm,根尖處
偏移平均1.39 mm,最大達到7.1 mm;但其中
發現兩篇臨床研究植體位置有過大的誤差偏移31, 38,Di Giacomo等學者31 認為較大的誤差偏移
來自於在植體鑽骨製備時手術模板發生位移。
另外CAD/CAM製成的導引板較技工室製作來
的準確25;而導引板的支持對準確度亦有重大
影響;在臨床研究中,與其他形式支持的導引
相比,骨支持式的手術導引有最大的誤差25,
此因手術模板由電腦斷層掃描成像來製作,而
較細小的齒槽骨脊在掃描成像時被忽略,因而
使手術模板定位有誤差,有時須要將尖銳的骨
移除39,才能使手術模板貼合。當比較上下顎
時,目前尚無定論,有一些研究認為結果無差
異40, 41。Ozan研究結果提出下顎較上顎準確42,
而Di Giacomo等學者發現在上顎有較大偏移43。
然而,Pettersson44 發現在下顎有較大誤差。此
外,證據顯示一些導引系統同時提供鑽骨製備
與放置植體,又稱全導引系統較只提供鑽骨製
備,但須拿掉手術導引板徒手放置植體的部分
導引系統來的準確25。長度較長的植體會有較
大的根尖偏移36,兩篇關於顴骨植體和翼骨植
體使用靜態骨支持式導引的準確度研究45, 46,平
均冠部偏移2.56 mm,根尖偏移3.7 mm,角度誤
差3.92度37。而比較在完全無牙牙脊與局部無牙
牙脊的準確度,在Tahmaseb的系統性回顧分析
中顯示並無顯著差異25;但在2009年Valente多
中心回溯研究中,在完全無牙牙脊較局部無牙
牙脊有較小的根尖偏移47。
電腦導引式常見的手術併發症25, 36 是植體
植入時扭矩過大,導致術中手術導引板斷裂、
植體缺乏初期穩定度、無法準確置入手術模
板、植體斷裂、植體頰側骨開窗。而機械性併
發症36 常見於立即置入術前預先製成臨時固定
贋復物,包括螺絲鬆脫、植體/支台齒與支台齒
/贋復物連結處的錯位、贋復物斷裂、大規模的
咬合調整、中線偏移;這些併發症與植體植入
位置與術前設計位置不符有關。Schneider報告
中48 指出手術中併發症發生率為9.1%,而贋復
物機械性併發症為18.8%。此外,若植體發生較
大偏移,易導致贋復物併發症或重大解剖結構
的傷害,如神經障礙或誤植入鼻竇或鼻腔,因
此建議距離預設植體位置的根尖處在應該要有2
mm安全區37 或使用長度較短植體以減小根尖偏
移36,避免侵犯重要解剖結構。
2015年Moraschini統合分析單顎或雙顎無
牙患者使用不翻瓣電腦導引式手術植入植體後
提出,儘管植體有高的存活率和低的邊緣骨喪
失,但手術和贋復物併發症種類類仍似於徒手
翻瓣手術,且常發生;故施術者仍需要有一定
的學習曲線才能達到成功的治療36。而至目前
為止,沒有足夠證據顯示電腦輔助導引式植入
- 37 -
台灣口外誌 利用電腦導引植入四支植體合併立即負載重建上顎:兩年追蹤病例報告與文獻回顧
植體手術在安全、治療結果、或效率優於傳統
徒手手術17, 24, 25。
病例討論
牙齒喪失後,齒槽骨萎縮程度隨著時間增
加而變嚴重。有幾種贋復治療可選擇,包括活
動義齒,植體固持活動式贋復物,或植體支撐
固定式贋復物49。而植體固持活動式義齒和植
體支撐固定式贋復物比活動義齒有較高的患者
滿意度50,且植體支撐撐固定式贋復物有很高
的存活率51。
在後牙區無牙脊,若需要植入傳統軸向植
體,常需要大範圍補骨手術。補骨手術需要額
外費用和較長治療時間,且伴隨可能的手術後
併發症。傾斜植體植入原有的齒槽骨減少補骨
步驟,是有效的替代方案。且在臨床成功率與
軸向植體並無差異52。
Paulo Malo在上下顎骨前牙區利用兩支軸
向植體,後牙區兩支傾斜植體,四支植體支撐
固定式贋復物並立即負載,稱之為“All on four
concept"7。即使在骨質密度較低的上顎骨,利
用此做法在3年到5年追蹤中,植體存活率仍高
達98%,贋復物存活率100%10。然而,若要在上
顎完全無牙牙脊的後牙區徒手植入傾斜植體,
為了閃避上顎竇,常需要在上顎竇開窗來決定
植體植入路徑8,因此也容易造成病患術後不適
與手術併發症。
利用電腦導引式手術有多項優點,可以依
照齒槽骨外型,精準地閃避重要解剖結構且利
用贋復導向植體植入方式植入植體,改善美觀
增加病患舒適度和滿意度53。在無牙脊使用電
腦導引式不翻瓣植體植入並立即給予贋復物首
先是由2005年Steenberghe提出53,術前若有準
確設計的放射線攝影模板,並製作成手術導引
板就能在理想位置處植入植體,若植入扭矩足
夠,術後即可有固定式贋復物並立即負載54,
因此就不需要臨時活動贋復物;若在植體骨整
合期間,配戴活動贋復物可能給予植體非軸向
力量55。
黏膜支持手術模板因為是軟組織支撐,在
診斷階段的電腦斷層掃描及手術階段的手術模
板放置,可能會因為軟組織的位移及旋轉而偏
移56,尤其是上顎黏膜較下顎厚,產生的誤差
更大。因此Van Assche建議黏膜支持手術模板
要使用咬合指標及固定螺絲定位來減少擺放位
置的誤差57。
2007年Malo發表不翻瓣使用手術導引板植
入4支植體合併立即負載術式的研究,共23位
患者(18 上顎骨,5下顎骨),一年後平均邊緣骨
頭喪失為1.9 mm35,符合2008年Misch等學者擬
定植體臨床成功標準所建議低於2.0 mm的邊緣
骨喪失14;本病例利用同Malo術式,目前追蹤
二年,植體周圍軟組織健康穩定,植體周圍骨
喪失穩定;正式贋復物完成後半年曾發生樹脂
義齒斷裂的機械性併發症,經過技工室修復並
咬合調整後,目前狀況穩定且患者咀嚼功能改
善,提高其生活品質,滿意其治療結果。
參考文獻
1. Branemark PI, Svensson B, van Steenberghe
D. Ten-year survival rates of fixed prostheses
on four or six implants ad modum Branemark
in full edentulism. Clin Oral Implants Res
1995; 6: 227–31.
2. Chung S,McCullagh A, Irinakis T. Immediate
loading in the maxillary arch: evidence-based
guidelines to improve success rates: a review.
J Oral Implantol 2011; 37: 610–21.
3. Papaspyridakos P, Chen CJ, Chuang SK,
Weber HP. Implant loading protocols for
edentulous patients with fixed rostheses: a
systematic review and meta-analysis. Int J
Oral Maxillofac Implants 2014; 29(Suppl):
256–70.
4. Gallucci GO, Morton D, Weber HP. Loading
protocols for dental implants in edentulous
- 38 -
Taiwan J Oral Maxillofac Surg 台灣口外誌
patients. Int J Oral Maxillofac Implants 2009;
24(Suppl ): 132–46.
5. Mericske-Stern R, Worni A. Optimal number
of oral implants for fixed reconstructions: a
review of the literature. Eur J Oral Implantol
2014; 7(Suppl 2S): 133–53.
6. Agliardi EL, Pozzi A, Stappert CFJ, Benzi
R, Romeo D, Gherlone E. Immediate fixed
rehabilitation of the edentulous maxilla: a
prospective clinical and radiological study
after 3 years of loading. Clin Implant Dent
Relat Res 2012; 16: 292–302.
7. Malò P, Rangert B, Nobre M. “All-on-Four”
immediate function concept with Brånemark
System implants for completely edentulous
mandibles: a retrospective clinical study. Clin
Implant Dent Relat Res 2003; 5(Suppl 1): 2–9.
8. Malò P, Rangert B, Nobre M. All-on-4
immediate-function concept with Brånemark
System implants for completely edentulous
maxillae: a 1-year retrospective clinical
study. Clin Implant Dent Relat Res 2005;
7(Suppl 1): S88–94.
9. Malò P, de Araújo Nobre M, Lopes A, Moss
SM, Molina GJ. A longitudinal study of the
survival of All-on-4 implants in the mandible
with up to 10 years of follow-up. J Am Dent
Assoc 2011; 142: 310–20.
10. Malò P, de Araújo Nobre M, Lopes A,
Francischone C, Rigolizzo M. “All-on-4”
immediate-function concept for completely
edentulous maxillae: a clinical report on the
medium (3 years) and long-term (5 years)
outcomes. Clin Implant Dent Relat Res 2012;
14(Suppl 1): e139–50.
11. Vasak C, Kohal RJ, Lettner S, Rohner
D, Zechner W. Clinical and radiological
evaluation of a template-guided (Nobel
Guide™) treatment concept. Clin Oral
Implants Res. 2014; 25: 116-23.
12. Bedrossian E. Rehabilitation of the edentulous
maxilla with the zygoma concept: a 7-year
prospective study. Int J Oral Maxillofac
Implants 2010; 25: 1213-21.
13. Buser D, Bornstein MM, Weber HP, Grutter
L, Schmid B, Belser UC. Early implant
placement with simultaneous guided bone
regeneration following single-tooth extraction
in the esthetic zone: a cross-sectional,
retrospective study in 45 subjects with a 2-
to 4-year follow-up. J Periodontol 2008; 79:
1773–81.
14. Misch CE, Perel ML, Wang HL, Sammartino
G, Galindo-Moreno P, Trisi P. Implant
success, survival and failure: The International
Congress of Oral Implantologists (ICOI) Pisa
Consensus Conference. Implant Dent 2008;
17: 5–15.
15. Loubele M, Bogaerts R, Van Dijck E, et
al. Comparison between effective radiation
dose of CBCT and MSCT scanners for
dentomaxillofacial applications. Eur J Radiol
2009; 71: 461–8.
16. Joda T, Gallucci GO. The virtual patient in
dental medicine. Clin Oral Implant Res 2014;
26: 725–6.
17. D'haese J, Ackhurst J, Wismeijer D. Current
state of the art of computer-guided implant
surgery Periodontol 2000. 2017; 73: 121-33.
18. Vercruyssen M, Fortin T, Widmann G,
Jacobs R, Quirynen M. Different techniques
of static/dynamic guided implant surgery:
modalities and indications. Periodontol 2000.
2014; 66: 214-7.
19. Lan is A, Á lvarez De l Canto O. The
Combination of digital surface scanners and
cone beam computed tomography technology
for guided implant surgery using 3 shape
- 39 -
台灣口外誌 利用電腦導引植入四支植體合併立即負載重建上顎:兩年追蹤病例報告與文獻回顧
implant studio software: A case history report
2015; 28: 169-78.
20. Geng W, Liu C, Su Y, Li J, Zhou Y. Accuracy
of different types of computer-aided design/
computer-aided manufacturing surgical guides
for dental implant placement. Int J Clin Exp
Med 2015; 8: 8442–9.
21. Brief J, Edinger D, Hassfeld S, Eggers G.
Accuracy of image guided implantology. Clin
Oral Implants Res 2005; 16: 495–501.
22. Kramer FJ, Baethge C, Swennen G, Rosahl S.
Navigated vs. conventional implant insertion
for maxillary single tooth replacement. Clin
Oral Implants Res 2005; 16: 60–8.
23. Ruppin J, Popovic A, Strauss M, Spuntrup E,
Steiner A, Stoll C. Evaluation of the accuracy
of three different computer- aided surgery
systems in dental implantology: optical
tracking vs. stereolithographic splint systems.
Clin Oral Implants Res 2008; 19: 709–16.
24. Jung R, Schneider D, Ganeles J, et al.
Computer technology applications in surgical
implant dentistry: a systematic review. Int J
Oral Maxillofac Implants 2009; 24: 92–109.
25. Tahmaseb A , W i sme i j e r D , Coucke
W, Derksen W. Computer technology
applications in surgical implant dentistry:
a systematic review. Int J Oral Maxillofac
Implants 2014; 29: 25-42.
26. Gulati M, Anand V, Salaria SK. Computerized
implant-dentistry: Advances toward automation.
J Indian Soc Periodontol. 2015; 19: 5-10.
27. Lorsakul A, Suthakorn J. Toward robot-
assisted dental surgery: Path generation
and navigation system using optical tracking
Proceedings of the 2008 IEEE. International
Conference on Robotics and Biomimetics
2009; 21: 1212-6.
28. Staffileno H. Significant differences and
advantages between the full thickness and
split thickness flaps. J Periodontol 1974; 45:
421–5.
29. Cosyn J, Hoogde N, De Bruyn H. A systematic
review on the frequency of advanced recession
following single immediate implant treatment.
J Clin Periodontol 2012; 39: 582–9.
30. Becker W, Goldstein M, Becker BE, Sennerby
L. Minimally invasive flapless implant surgery:
a prospective multicenter study. Clin Implant
Dent Relat Res 2005; 7: 21–7.
31. Di Giacomo GA, Cury PR, de Araujo NS,
Sendyk WR, Sendyk CL. Clinical application
of stereolithographic surgical guides for
implant placement: Preliminary results. J
Periodontol 2005; 76: 503–7.
32. Puig CP. A retrospective study of edentulous
patients rehabilitated according to the ‘all-
on-four’ or the ‘all-on-six’ immediate
function concept using flapless computer-
guided implant surgery. Eur J Oral Implantol
2010; 3: 155–63.
33. Hahn J. Single-stage, immediate loading, and
flapless surgery. J Oral Implantol 2000; 26:
193–8.
34. Brodala N. Flapless surgery and its effect on
dental implant outcomes. International J Oral
Maxillofac Implants 2009; 24(Suppl): 118–25.
35. Malo P, de Araujo Nobre M, Lopes A. The
use of computer-guided flapless implant
surgery and four implants placed in immediate
funct ion to support a f ixed denture:
preliminary results after a mean follow-up
period of thirteen months. J Prosthet Dent
2007; 97(6 Suppl): S26-34.
36. Moraschini V, Velloso G, Luz D, Porto Barboza
E. Implant survival rates, marginal bone level
changes, and complications in full-mouth
rehabilitation with flapless computerguided
- 40 -
Taiwan J Oral Maxillofac Surg 台灣口外誌
surgery: a systematic review and meta-
analysis. Int J Oral Maxillofac Surg 2015; 44:
892–901.
37. D’haese J, Van de Velde T, Komiyama
A, Hultin M, De Bruyn H. Accuracy and
complications using computer designed
stereolithographic surgical guides for oral
rehabilitation by means of dental implants:
a review of the literature. Clin Implant Dent
Relat Res 2012; 14: 321–35.
38. Cassetta M, Giansanti M, Di Mambro A,
Calasso S, Barbato E. Accuracy of Two
Stereolithographic Surgical Templates: A
Retrospective Study. Clinical Implant Dent
Relat Res 2013; 15: 448–59.
39. Yong LT, Moy PK. Compl icat ions o f
computer-aided-design/ computer- aided-
machining- guided (NobelGuide) surgical
implant placement: an evaluation of early
clinical results. Clin Implant Dent Relat Res
2008; 10: 123-7.
40. Ersoy AE, Turkyilmaz I, Ozan O, McGlumphy
EA. Reliability of implant placement with
stereolithographic surgical guides generated
from computed tomography: Clinical data
from 94 implants. J Periodontol 2008; 79:
1339–45.
41. Arisan V, Karabuda ZC, Piskin B, Ozdemir
T. Conventional multi-sl ice computed
tomography (CT) and cone-beam CT (CBCT)
for computer-aided implant placement.
Part II: Reliability of mucosa-supported
stereolithographic guides. Clin Implant Dent
Relat Res 2013; 15: 907-17.
42. Ozan O, Orhan K, Turkyilmaz I. Correlation
between bone density and angular deviation of
implants placed using CT-generated surgical
guides. J Craniofac Surg 2011; 22: 1755–61.
43. Di Giacomo GA, da Silva JV, da Silva AM,
Paschoal GH, Cury PR, Szarf G. Accuracy
and complications of computer-designed
selective laser sintering surgical guides
for flapless dental implant placement and
immediate definitive prosthesis installation. J
Periodontol 2012; 83: 410–9.
44. Pettersson A, Kero T, Gillot L, et al.
Accuracy of CAD/CAM-guided surgical
template implant surgery on human cadavers:
Part I. J Prosthet Dent 2010; 103: 334–42.
45. van Steenberghe D, Malevez C, Van
Cleynenbreugel J, et al. Accuracy of drilling
guides for transfer from three dimensional
CT-based planning to placement of zygoma
implants in human cadavers. Clin Oral
Implants Res 2003; 14: 131–6.
46. Vrielinck L, Politis C, Schepers S, PauwelsM,
Naert I. Image based planning and clinical
validation of zygoma and pterygoid implant
placement in patients with severe bone
atrophy using customized dril l guides.
Preliminary results from a prospective clinical
follow-up study. Int J Oral Maxillofac Surg
2003; 32: 7–14.
47. Valente F, Schiroli G, Sbrenna A. Accuracy
of computer aided oral implant surgery: a
clinical and radiographic study. Int J Oral
Maxillofac Implants 2009; 24: 234–44.
48. Schneider D, Marquardt P, Zwahlen M, Jung
RE. A systematic review on the accuracy
and the clinical outcome of computer-guided
template-based implant dentistry. Clin Oral
Implants Res 2009; 4: 73–86.
49. A t tW, Be rnha r t J , S t r ub JR . F i xed
rehabilitation of the edentulous maxilla:
possibilities and clinical outcome. J Oral
Maxillofac Surg 2009; 67: 60–73.
50. Att W, Stappert C. Implant therapy to
improve quality of life. Quintessence Int
- 41 -
台灣口外誌 利用電腦導引植入四支植體合併立即負載重建上顎:兩年追蹤病例報告與文獻回顧
2003; 34: 573–81.
51. Bergendal T, Engquist B. Implant-supported
overdentures: A longitudinal prospective
study. Int J Oral Maxillofac Implants 1998;
13: 253–62.
52. Ata-Ali J, Penarrocha-Oltra D, Candel-Marti
E, Penarrocha-Diago M. Oral rehabilitation
with tilted dental implants: A meta-analysis.
Med Oral Patol Oral Cir Bucal. 2012; 17:
582-7.
53. van Steenberghe D, Glauser R, Blomback U,
et al. A computed tomographic scan-derived
customized surgical template and fixed
prosthesis for flapless surgery and immediate
loading of implants in fully edentulous
maxillae: a prospective multicenter study.
Clin Implant Dent Relat Res 2005; 7(suppl 1):
S111–20.
54. Sanna AM, Molly L, van Steenberghe D.
Immediately loaded CAD-CAM manufactured
fixed complete dentures using flapless implant
placement procedures: a cohort study of
consecutive patients. J Prosthet Dent 2007;
97: 331–9.
55. Gillot L, Noharet R, Cannas B. Guided
su rge ry and p resurg i ca l p ros thes i s :
preliminary results of 33 fully edentulous
maxillae treated in accordance with the
NobelGuide protocol. Clin Implant Dent Relat
Res 2010; 12 (Suppl 1): e104–13.
56. Cassetta M, Di Mambro A, Giansanti M,
Stefanelli LV, Barbato E. How does an
error in positioning the template affect the
accuracy of implants inserted using a single
fixed mucosa-supported stereolithographic
surgical guide? Int J Oral Maxillofac Surg
2014; 43: 85-92.
57. Van Assche N, Vercruyssen M, Coucke W,
Teughels W, Jacobs R, Quirynen M. Accuracy
of computer-aided implant placement. Clin
Oral Implants Res 2012; 23 Suppl 6: 112-23.
- 42 -
Taiwan J Oral Maxillofac Surg 台灣口外誌
Maxillary Rehabilitation with Immediately Loaded Protocol by Four Implants Using the Guided Surgery―A Two-year
Follow-up Case Report and Literature Review
Huang JY, Lung H, Auyeung L and Aaron Yu-Jen Wu
Division of Periodontics, Department of Dentistry, Kaohsiung Chang Gung Memorial Hospital,
Kaohsiung, Taiwan, R.O.C.
Abstract
Maxillary rehabilitation with dental implants in the atrophic maxilla using traditional implant surgery necessitates the wait for wait for the bone augmentation procedures and osseointegration of the implants. The patient usually does not have any prostheses or needs to wear a removable denture during this time. The prosthesis often requires adjustment to avoid interference with the post-wound healing and the outcome of bone augmentation procedure, and thus affect the patient's chewing function and social contact. "All-on-4 concept" provides the patient with an immediate, high-quality, esthetic, and functional complete fixed prosthesis and eliminates the need for bone augmentation procedures.
This literature review begins with a case discussion of a maxillary edentulism. An edentulous maxilla was rehabilitated by placement of four implants using the tilted treatment concept and immediate loading using computer-assisted flapless surgery. Physicians determined the relationship between soft tissue and hard tissue through 3D images before surgery and accurately planned the positioning of the implant through digital tomography scans, computer-aided treatment planning, and two-scan protocol. By utilizing the preoperative computer-aided design of the implants, a cast was made to fabricate the temporary implant-supported all-acrylic resin denture. After a three –month period to achieve osseointegration, impressions were taken for fabricating the final metal-based prostheses. The patient was recalled every three months for maintenance. At the two-year follow-up examination, the peri-implant mucosal soft tissues remained in good condition. In this paper, we reviewed the literature of computer-guided implant surgery to explore its development and assess its clinical practicability.
Key words: Maxilla, Computer guided, Immediate loading.
Received: January 21, 2018Accepted: March 13, 2018Reprint requests to: Dr. Aaron Yu-Jen Wu, Department of Dentistry, Kaohsiung Chang Gung
Memorial Hospital, No.123, Dapi Rd., Niaosong Dist., Kaohsiung City 833, Taiwan, R.O.C.