Download - Disclosures - Biosimilars Nederland

Prof.WojciechJurczakMD,PhD
Disclosures
PROF.WOJCIECHJURCZAK,M.D.,PH.D.
ADVISORYBOARDS:SANDOZNOVARTIS,ROCHE,JANSSEN,ACERTA,ABBVIE,TGTHERAPEUTICS,TEVA,TAKEDA,SPECTRUM,NOVONORDISK,MUNDIPHARMA,RESEARCHFUNDING:CELGENE,ABBVIE,GILEAD,TGTHERAPEUTICS,JANSSEN,ACERTA,,MERCK,BEGENE,PHARMACYCLICS,PFIZER,ROCHE,SANDOZ–NOVARTIS,TAKEDA,TEVA,SERVUIER,EISAI.
DISCLAIMER:Thesenon-promo,onalslidesareintendedtobeusedaseduca,onalmaterialonly.Thedouble-dagger(‡)symbolindicatesthattheseslidesmaycontaininforma,onthatisnotwithinEMAorFDAapprovedproductlabelingandhasnototherwisebeenapprovedbytheEMAorFDA.Informa,onwithinthisslidedeckisrelatedtoinves,ga,onalagentsthatarenotapprovedbytheEMAorFDAandhavenotyetbeendeterminedtobesafeorefficaciousinhumans
Prof.WojciechJurczakMD,PhD
Biosimilar-trialswithRituximab:be6eracceptancethroughbe6erunderstanding
Prof.WojciechJurczak,M.D.,Ph.D.DptofHematology,[email protected],(+48602338290)

Prof.WojciechJurczakMD,PhD
MoAbinNHL:EverythingStartedWithRituximab
Development and registration
of original particle (Roche)
Subcutaneous Rituximab (Roche)
Rituximab biosimilars: • CT-P10 (Celltrion)
• GP2013 (Sandoz Novartis)
Coiffier,Czuczman,Sales,Marcus,Hiddemann
Davies
Coiffier,Jurczak

Prof.WojciechJurczakMD,PhD
RituximabremainsastandardofcareinIlineBcellNHL
WithnewMoAbandsmallparGcles,Rituximabroleinrelapsing/refractoryNHLmaybedisputable
LymphomaSubtype IlineinducGon Ilinemaintenance
AggresiveLymphomas yes NoMCL yes yesIndolentlymphomas yes ?CLL yes yes

Prof.WojciechJurczakMD,PhD
First-LineDLBCLTreatment
60%cure,40%relapsed/refractory
Intensive eligible (70%)
High-risk intensive eligible
(10%)
Intensive ineligible
(20%)
R-CHOP
R-DAEPOCH
R–miniCHOPR-Nodoxorubicin-chemotherapy
R-CHOP:Rituximab+cyclophosphamide,doxorubicin,vincrisdne,prednisone;DA-EPOCH-R:etoposide,vincrisdne,doxorubicin,cyclophosphamide,prednisone,rituximab.Basedon:NCCNguidelines.hfps://www.nccn.org/about/nhl.pdf.Accessed22June2017.
Prof.WojciechJurczakMD,PhD
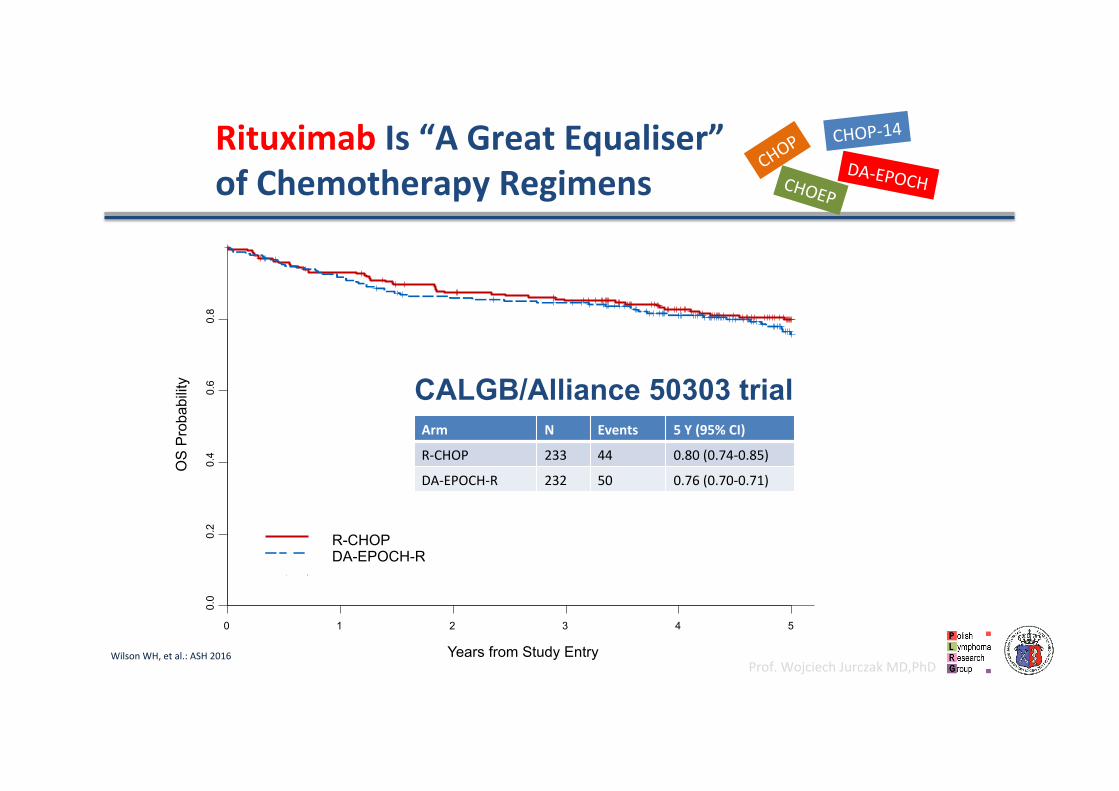
RituximabIs“AGreatEqualiser”ofChemotherapyRegimens
CALGB/Alliance 50303 trialArm N Events 5Y(95%CI)
R-CHOP 233 44 0.80(0.74-0.85)
DA-EPOCH-R 232 50 0.76(0.70-0.71)
Years from Study Entry
OS
Pro
babi
lity
0 1 2 3 4 5
0.0
0.2
0.4
0.6
0.8
R-CHOP DA-EPOCH-R
WilsonWH,etal.:ASH2016
CHOEP
CHOP-14
DA-EPOCH
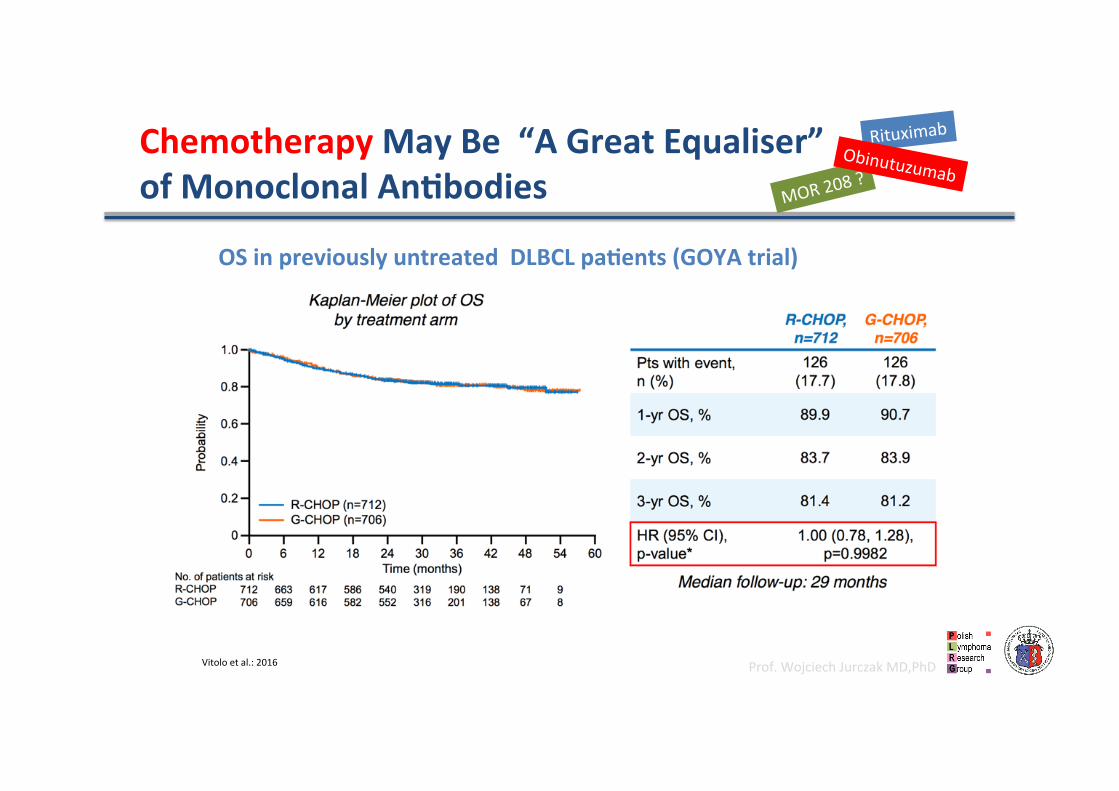
Prof.WojciechJurczakMD,PhDVitoloetal.:2016
ChemotherapyMayBe“AGreatEqualiser”ofMonoclonalAnGbodies MOR208
?
RituximabObinutuzumab
OSinpreviouslyuntreatedDLBCLpaGents(GOYAtrial)

Prof.WojciechJurczakMD,PhD
LenalidomideandIbruGnibinABC-DLBCL:Phase3TrialsAreUnderway(‡)
ABC:acdvatedB-celllike.Figure:1.ShafferAL3rdetal.AnnRevImmunol.2012;30:565-610.
Chronic Active BCR signalling Constitutive
MYD88 signalling
Autocrine cytokine signalling
Akt/mTOR pathway
NF-κB pathway
Interferon pathway
STAT1 STAT3 P P
P P
P P
IFN-β IL-6/IL-10
MYD88 TIR domain
mutation
CARD11 CC domain
mutation
CD79A/B ITAM
mutation SYK
SFK
PI93)K
BTK
PKCβ
A20 loss A20
Survival
CARD11 MALT1 BCL10
IgL
IgH
CD
79A
CD
79B
TYK2 JAK1 MYD88 IRAK4 IRAK1
TRAF6
Lenalidomide downregulates NF-κB and upregulates the
IFN-β pathway 2.ClinicalTrials.govIdendfier:NCT01855750;3.ClinicalTrials.govIdendfier:NCT02285062.
Prof.WojciechJurczakMD,PhD
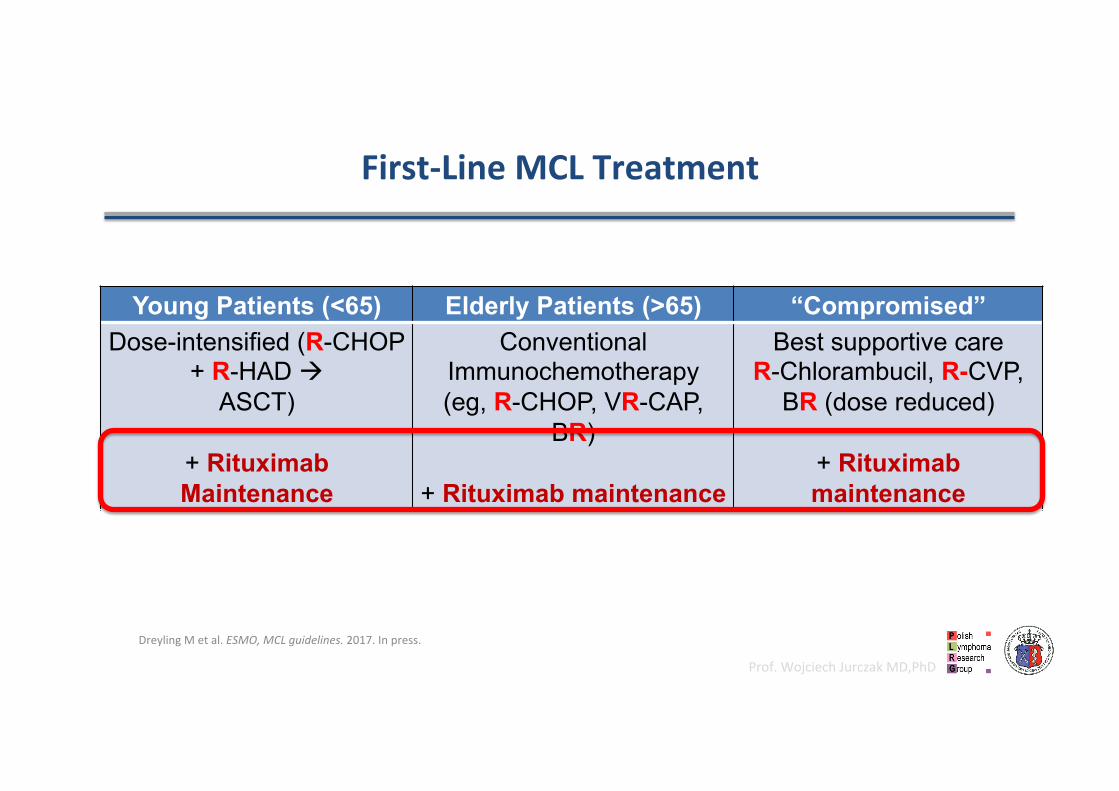
First-LineMCLTreatment
DreylingMetal.ESMO,MCLguidelines.2017.Inpress.
Young Patients (<65) Elderly Patients (>65) “Compromised”Dose-intensified (R-CHOP
+ R-HAD à ASCT)
+ Rituximab Maintenance
Conventional Immunochemotherapy (eg, R-CHOP, VR-CAP,
BR)
+ Rituximab maintenance
Best supportive care R-Chlorambucil, R-CVP,
BR (dose reduced)
+ Rituximab maintenance

Prof.WojciechJurczakMD,PhD
MCL-LYMAtrialin“youngerpaGents”
LEGOUILLetal.:ASH2013/2014/2015/2016

Prof.WojciechJurczakMD,PhD
IndollentLymphomas
R-B
R-CHOP
R-CVP
R
Prof.WojciechJurczakMD,PhD
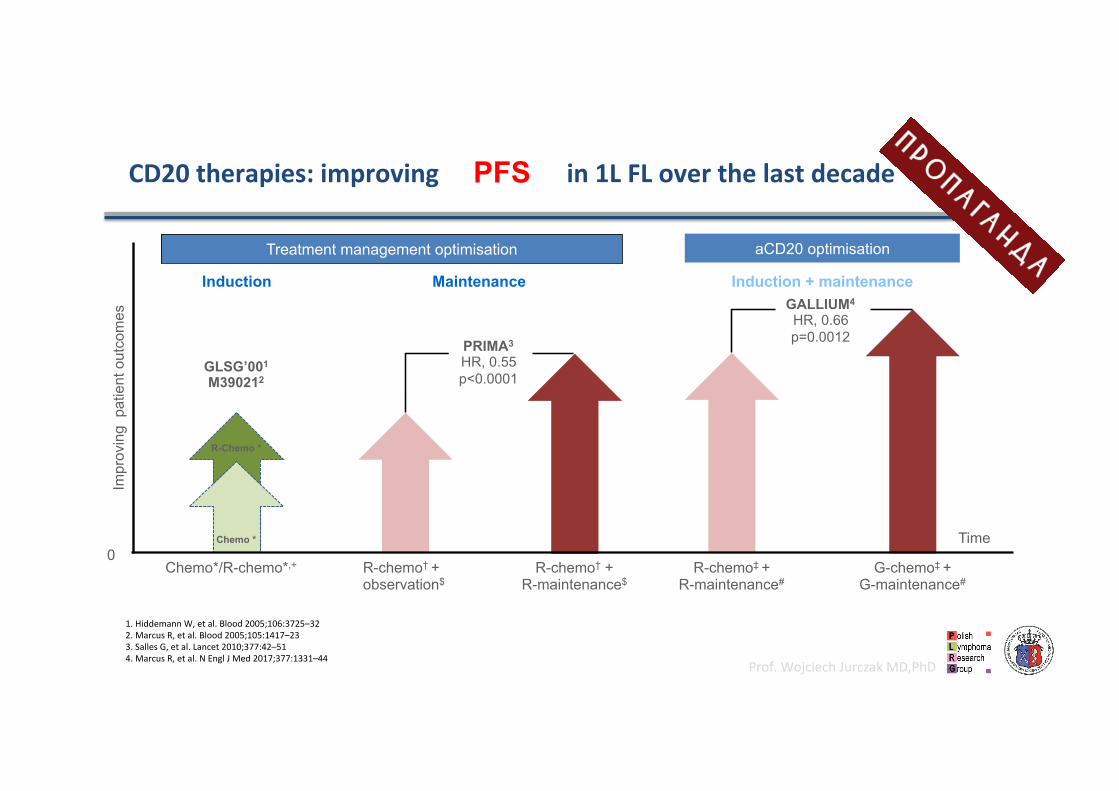
CD20therapies:improvingoutcomesin1LFLoverthelastdecadePFS
Treatment management optimisation
R-chemo‡ + R-maintenance#
G-chemo‡ + G-maintenance#
PRIMA3
HR, 0.55 p<0.0001
GALLIUM4
HR, 0.66 p=0.0012
0 Chemo*/R-chemo*,+ R-chemo† +
R-maintenance$ R-chemo† + observation$
Maintenance
GLSG’001
M390212
Time
Impr
ovin
g p
atie
nt o
utco
mes
aCD20 optimisation
Induction + maintenance Induction
Chemo *
R-Chemo *
1.HiddemannW,etal.Blood2005;106:3725–322.MarcusR,etal.Blood2005;105:1417–233.SallesG,etal.Lancet2010;377:42–514.MarcusR,etal.NEnglJMed2017;377:1331–44

Prof.WojciechJurczakMD,PhD13
Marcusetal.:2016
Chemotherapymaybe“AGreatEqualiser”ofMonoclonalAnGbodies
MOR208?
RituximabObinutuzumab
OSinpreviouslyuntreatedFLpaGents(GALLIUMtrial)

Prof.WojciechJurczakMD,PhD
14
Geodeetal.:2014
ChemotherapyMayBe“AGreatEqualiser”ofMonoclonalAnGbodies
MOR208?
RituximabObinutuzumab
OSinpreviouslyuntreatedelderlyCLLpaGents(CLL-11trial)
OS
StratyfikowanyHR0,7795%CI0,57–1,05p=0,0932
GClbRClb
Czas[miesiące]
ClbAlone
(n=118)
RClb
(n=233) O-Clb
(n=238)
ORR 32% 65% 78% CR 0 7% 21% MedianPFS
11months
16months
27months
Unlessitischlorambucil?

Prof.WojciechJurczakMD,PhD
IsmaintenanceRituximabsGllthestandardofcareiniNHL?
RituximabMaintenance
• DoesnotprolongOS
• MoreAE(infecGons,secondaryneoplasms)
• EfficacyofRituximabretreatment
• Costefficacy?
Prof.WojciechJurczakMD,PhD
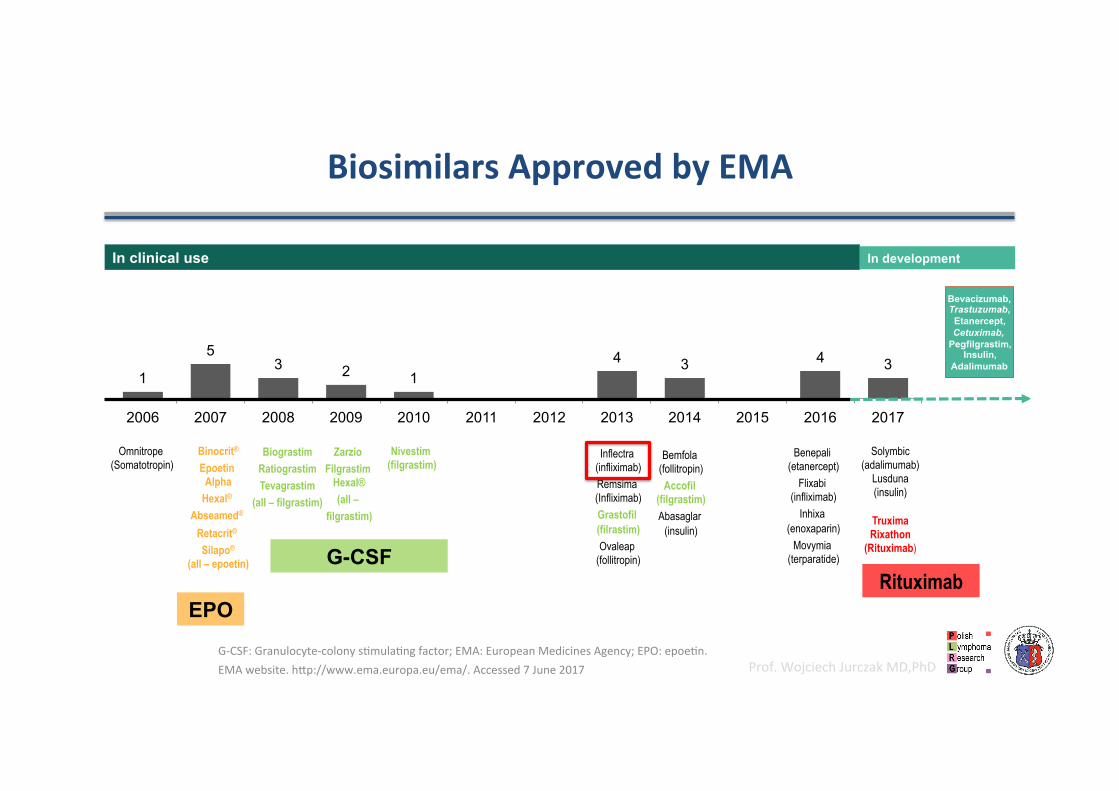
BiosimilarsApprovedbyEMA
Omnitrope (Somatotropin)
Biograstim
Ratiograstim Tevagrastim
(all – filgrastim)
Zarzio Filgrastim
Hexal® (all –
filgrastim)
Nivestim (filgrastim)
Inflectra (infliximab) Remsima (Infliximab) Grastofil (filrastim) Ovaleap
(follitropin)
In clinical use
Bemfola (follitropin) Accofil
(filgrastim) Abasaglar
(insulin)
Solymbic (adalimumab)
Lusduna (insulin)
Truxima Rixathon
(Rituximab)
Benepali (etanercept)
Flixabi (infliximab)
Inhixa (enoxaparin)
Movymia (terparatide)
1
5 3 2 1
4 3 4 3
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
In development
Bevacizumab, Trastuzumab, Etanercept, Cetuximab,
Pegfilgrastim, Insulin,
Adalimumab
Binocrit®
Epoetin Alpha
Hexal® Abseamed®
Retacrit® Silapo®
(all – epoetin)
EPO
G-CSF Rituximab
G-CSF:Granulocyte-colonysdmuladngfactor;EMA:EuropeanMedicinesAgency;EPO:epoedn.EMAwebsite.hfp://www.ema.europa.eu/ema/.Accessed7June2017
Prof.WojciechJurczakMD,PhD
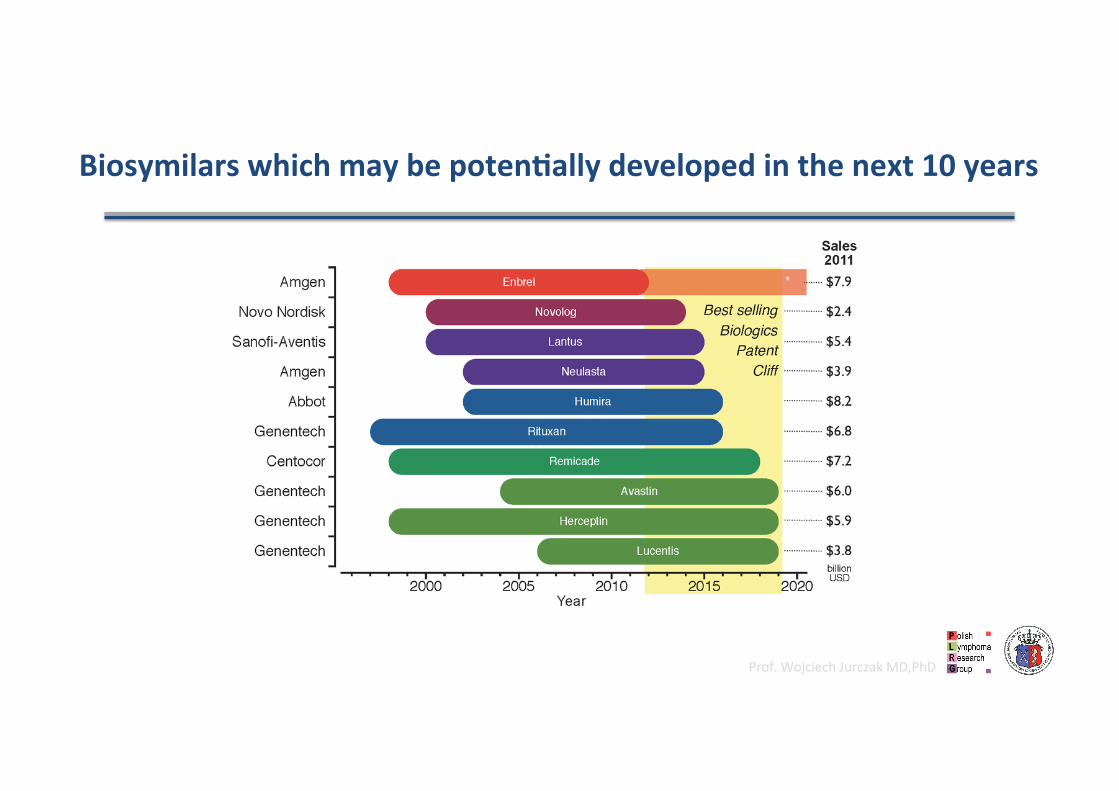
BiosymilarswhichmaybepotenGallydevelopedinthenext10years
Prof.WojciechJurczakMD,PhD
OncebiosymilarisapprovedithassubstanGalfinancialimpact
“Biosymilars– symilarbutnotiden@cal”

Prof.WojciechJurczakMD,PhD
AherintruducingG-CSFbiosymilarit’susagedoubled
WalshK.:BiosimilarMedicines11thEGAInternadonalSymposium,2013

Prof.WojciechJurczakMD,PhD
Analydcal
Preclinical
PK/PD
Clinical
Majorgoalistodeterminetheclinicaleffect
Referencemedicine
Clinical
PK/PD
Preclinical
Analydcal
Majorgoalistodeterminesimilarity;establishmentofthesciendficbridge
totheclinicalexperienceoftheoriginator
Biosimilar
Differentfocusbetweenoriginator&biosimilardevelopment
Intheend,bothapproachesprovidethesamelevelofconfidencewithregardtosafetyandefficacyofthemedicine
Prof.WojciechJurczakMD,PhD
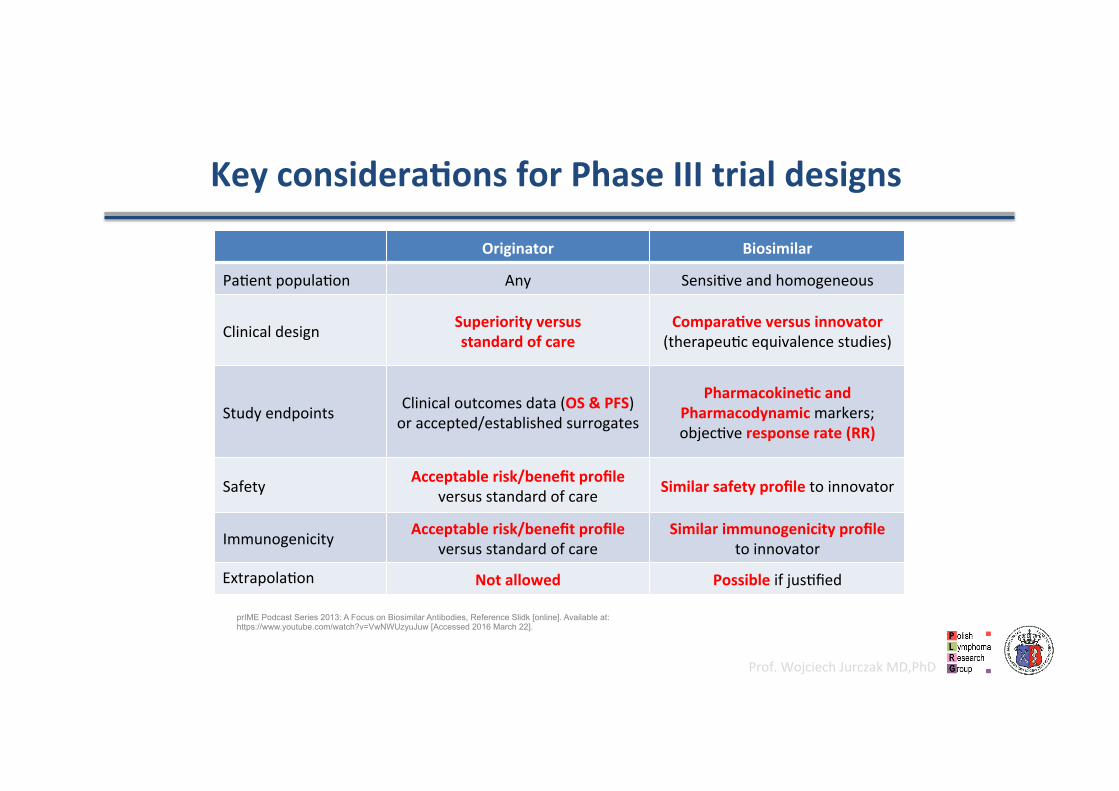
KeyconsideraGonsforPhaseIIItrialdesigns
Originator Biosimilar
Padentpopuladon Any Sensidveandhomogeneous
Clinicaldesign Superiorityversusstandardofcare
ComparaGveversusinnovator(therapeudcequivalencestudies)
Studyendpoints Clinicaloutcomesdata(OS&PFS)oraccepted/establishedsurrogates
PharmacokineGcandPharmacodynamicmarkers;objecdveresponserate(RR)
Safety Acceptablerisk/benefitprofileversusstandardofcare Similarsafetyprofiletoinnovator
Immunogenicity Acceptablerisk/benefitprofileversusstandardofcare
Similarimmunogenicityprofiletoinnovator
Extrapoladon Notallowed Possibleifjusdfied
prIME Podcast Series 2013: A Focus on Biosimilar Antibodies, Reference Slidk [online]. Available at: https://www.youtube.com/watch?v=VwNWUzyuJuw [Accessed 2016 March 22].

Prof.WojciechJurczakMD,PhD
Shihsinqualitya6ributesofRituxan®/Mabthera®betweendifferentbatches
ShieldsetalJBiolChem.2002

Prof.WojciechJurczakMD,PhD
RituximabBiosimilars
GP2013BeingassessedbyEMA
CT-P10RegisteredbyEMA
Prof.WojciechJurczakMD,PhD
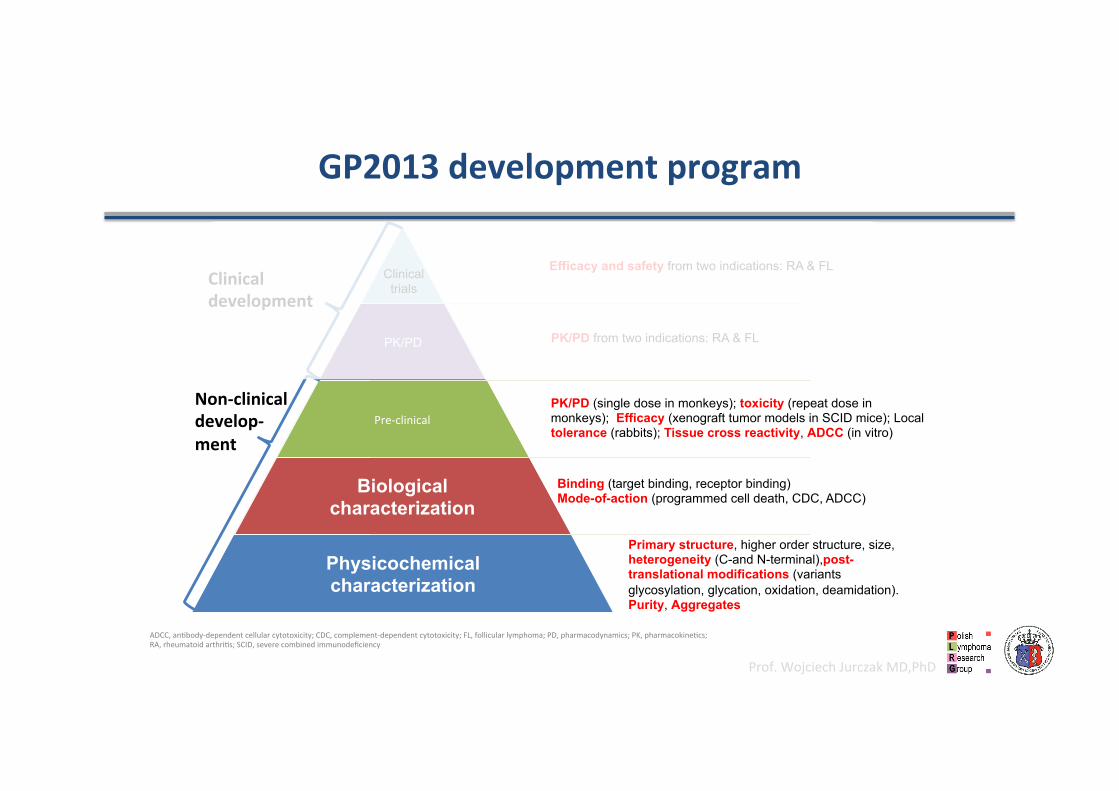
GP2013developmentprogram
PK/PD
Pre-clinical
Biological characterization
Physicochemical characterization
Clinical trials
Binding (target binding, receptor binding) Mode-of-action (programmed cell death, CDC, ADCC)
Primary structure, higher order structure, size, heterogeneity (C-and N-terminal),post-translational modifications (variants glycosylation, glycation, oxidation, deamidation). Purity, Aggregates
PK/PD (single dose in monkeys); toxicity (repeat dose in monkeys); Efficacy (xenograft tumor models in SCID mice); Local tolerance (rabbits); Tissue cross reactivity, ADCC (in vitro)
Efficacy and safety from two indications: RA & FL
PK/PD from two indications: RA & FL
ADCC,andbody-dependentcellularcytotoxicity;CDC,complement-dependentcytotoxicity;FL,follicularlymphoma;PD,pharmacodynamics;PK,pharmacokinedcs;RA,rheumatoidarthrids;SCID,severecombinedimmunodeficiency
Non-clinicaldevelop-ment
Clinicaldevelopment
Prof.WojciechJurczakMD,PhD
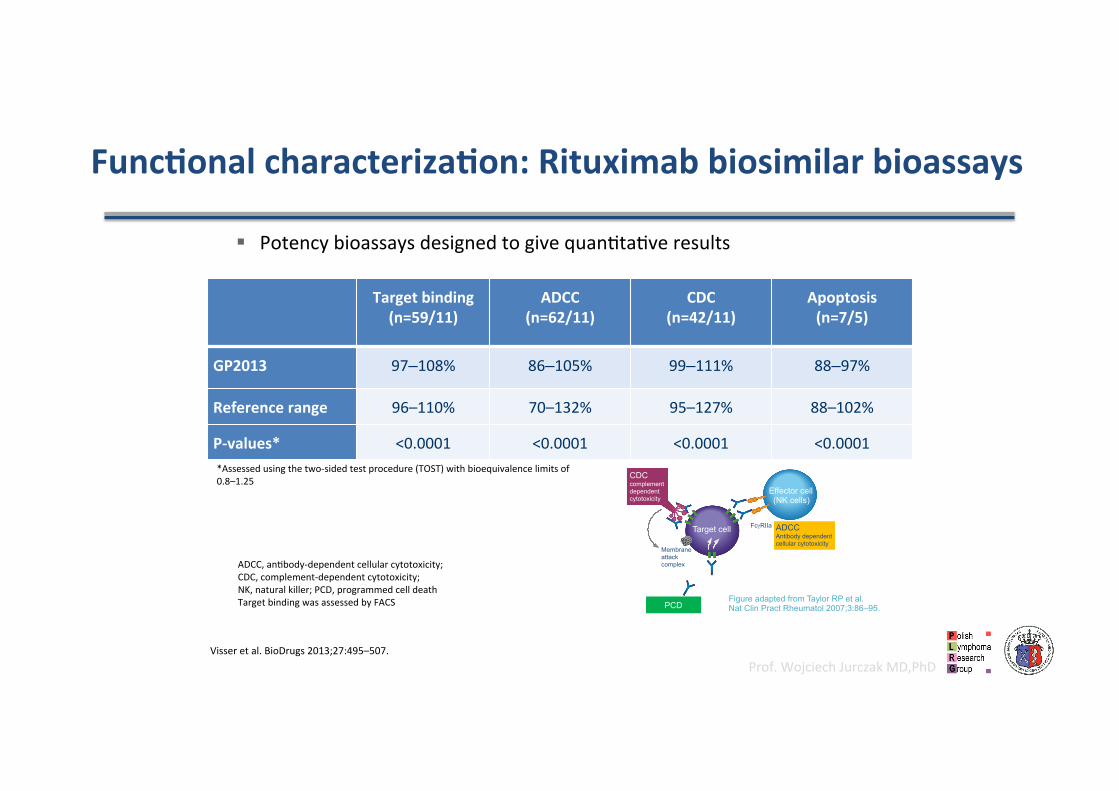
§ Potencybioassaysdesignedtogivequandtadveresults
FuncGonalcharacterizaGon:Rituximabbiosimilarbioassays
Targetbinding(n=59/11)
ADCC(n=62/11)
CDC(n=42/11)
Apoptosis(n=7/5)
GP2013 97–108% 86–105% 99–111% 88–97%
Referencerange 96–110% 70–132% 95–127% 88–102%
P-values* <0.0001 <0.0001 <0.0001 <0.0001*Assessedusingthetwo-sidedtestprocedure(TOST)withbioequivalencelimitsof0.8–1.25
Figure adapted from Taylor RP et al. Nat Clin Pract Rheumatol 2007;3:86–95.
CDC complement dependent cytotoxicity
Effector cell (NK cells)
Target cell
Membrane attack complex
FcγRIIa ADCC Antibody dependent cellular cytotoxicity
PCD
ADCC,andbody-dependentcellularcytotoxicity;CDC,complement-dependentcytotoxicity;NK,naturalkiller;PCD,programmedcelldeathTargetbindingwasassessedbyFACS
Visseretal.BioDrugs2013;27:495–507.

Prof.WojciechJurczakMD,PhD
Pre-clinicalinvitrocomparability:ADCCassayswithNKcells
Further cell lines tested: Raji, Z138
ADCC comparable to EU-sourced reference rituximab
Daudi cell line & fresh effector cells SU-DHL4 & fresh effector cells
EU-rituximab GP2013
80
-3
70
60
50
40
30
20
10
0 -2 -1 0 1 2 3 4
Log[Abs] (ng/ml)
Spec
ific
lysi
s (%
)
EU-rituximab GP2013
80
-3
70 60 50 40 30 20 10
0 -10
-2 -1 0 1 2 3 4 Log[Abs] (ng/ml)
Spec
ific
lysi
s (%
)
da Silva et al. Leuk Lymphoma 2014;55:1609–17.

Prof.WojciechJurczakMD,PhD
Pre-clinicalinvivocomparability(tumorgrowthmodels)
Efficacy is similar
SU-DHL-4 model Jeko-1 model
2000
0
1750
1500
1250
1000
750
500
250
0 7 14 21 28
Time (days)
Tum
or v
olum
e (m
m3 )
IgG-Control (30 mg/kg) GP2013 (3 mg/kg) GP2013 (30 mg/kg) EU-rituximab (3 mg/kg) EU-rituximab (30 mg/kg)
20 25 35 40 Time (days)
30
2400
1600
1200
800
400
0
Tum
or v
olum
e (m
m3 )
2000
IgG-Control (1 mg/kg) GP2013(0.03mg/kg)GP2013 (0.1 mg/kg) GP2013 (0.3 mg/kg) GP2013 (1.0 mg/kg) EU-rituximab(0.03mg/kg)EU-rituximab(0.1 mg/kg) EU-rituximab(0.3 mg/kg) EU-rituximab(1.0 mg/kg)
da Silva et al. Leuk Lymphoma 2014;55:1609–17.

Prof.WojciechJurczakMD,PhD
Pre-clinicalinvivocomparability:PKfollowingIVadministraGonto
primates
PK: AUC and Cmax are similar
da Silva et al. Leuk Lymphoma 2014;55:1609–17.
5 mg/kg 20 mg/kg, repeat dosing 100 mg/kg , repeat dosing
EU-rituximab
Time after administration (days)
Ritu
xim
ab c
once
ntra
tion
(µg/
mL)
180
0
160 140 120 100
80 60 40 20
0 2 4 6 8 10
450 400 350 300 250 200 150 100
50 0
0 2 4 6 8 10 12 14 16 Time after administration
(days)
2000 1800 1600 1400 1200 1000
800 600 400 200
0 0 2 4 6 8 10 12 14 16
Time after administration (days)
GP2013
Seconddose Seconddose
Prof.WojciechJurczakMD,PhD
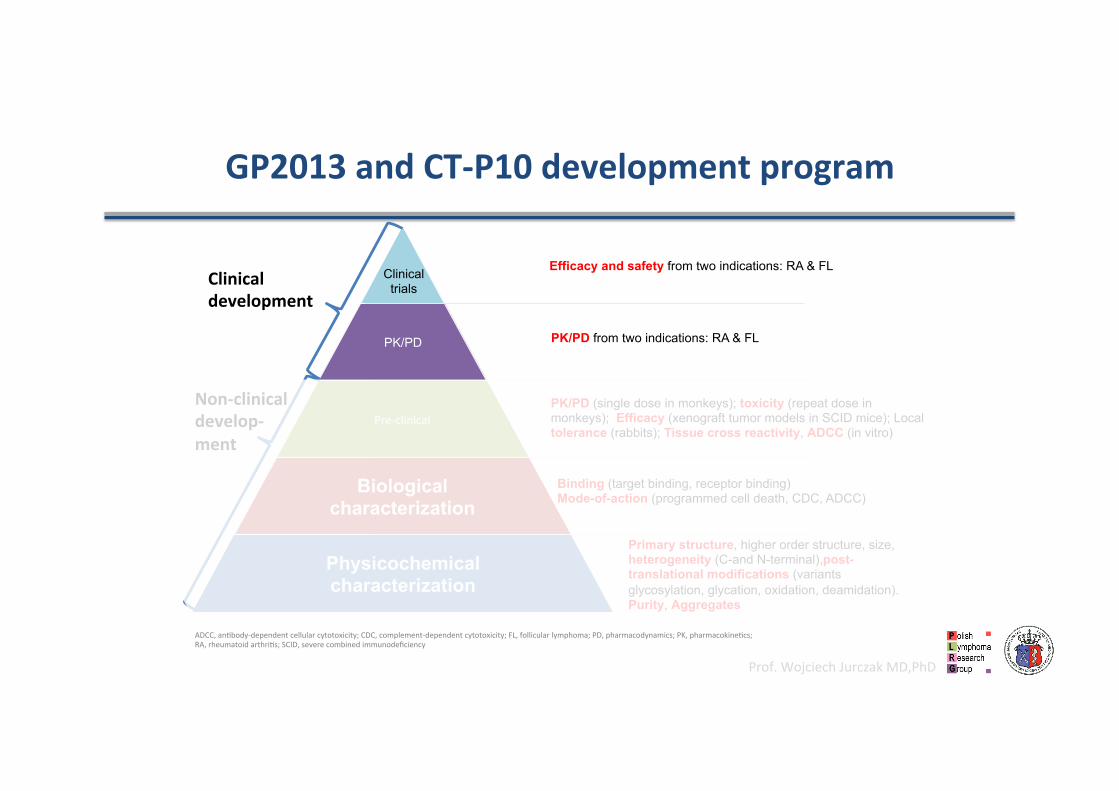
GP2013andCT-P10developmentprogram
PK/PD
Pre-clinical
Biological characterization
Physicochemical characterization
Clinical trials
Binding (target binding, receptor binding) Mode-of-action (programmed cell death, CDC, ADCC)
Primary structure, higher order structure, size, heterogeneity (C-and N-terminal),post-translational modifications (variants glycosylation, glycation, oxidation, deamidation). Purity, Aggregates
PK/PD (single dose in monkeys); toxicity (repeat dose in monkeys); Efficacy (xenograft tumor models in SCID mice); Local tolerance (rabbits); Tissue cross reactivity, ADCC (in vitro)
Efficacy and safety from two indications: RA & FL
PK/PD from two indications: RA & FL
ADCC,andbody-dependentcellularcytotoxicity;CDC,complement-dependentcytotoxicity;FL,follicularlymphoma;PD,pharmacodynamics;PK,pharmacokinedcs;RA,rheumatoidarthrids;SCID,severecombinedimmunodeficiency
Non-clinicaldevelop-ment
Clinicaldevelopment

Prof.WojciechJurczakMD,PhD
ClinicaltrialassessingthesafetyandimmunogenicityoftransiGoningtoGP2013treatmentinpaGentswithRArefractoryorintolerantofstandardDMARDSandanG-TNFswhoreceivedatleastonepriordoseofrituximab1
• N=107(planned)• PrimaryobjecGve:AEs• SecondaryobjecGves:IRRs,immunogenicity
ClinicaltrialassessingthesafetyandPKofGP2013incombinaGonwithMTXinpaGentswithRAwhofailedonatleasttwoanG-TNFs2,3
• N=312(173EU-rituximab,139US-rituximab)• PrimaryobjecGve:PK• SecondaryobjecGves:DAS28atWeek24,PK/PD,safety
ConfirmatoryPhaseIIIclinicaltrialassessingtheefficacyandsafetyofrituximabbiosimilartreatmentinpaGentswithpreviouslyuntreated,
advanced-stageFL5,6• N=629• 8cyclesofR-CVP,followedby2years’maintenance• PrimaryobjecGve:ORRatWeek24• SecondaryobjecGves:CR/PR,PFS,OS,PK/PD,safety
GP2013clinicaldevelopment
AE,adverseevent;CR,completeresponse;CVP,cyclophosphamide,vincrisdne,prednisolone;DAS,diseaseacdvityscore;FL,follicularlymphoma;IRR,infusion-relatedreacdon;JP,Japanesepadents;MTX,methotrexate;NHL,non-Hodgkin’slymphoma;ORR,overallresponserate;OS,overallsurvival;PD,pharmacodynamics;PFS,progression-freesurvival;PK,pharmacokinedcs;PR,pardalresponse;R,rituximab;RA,rheumatoidarthrids;TNF,tumornecrosisfactor1.Clinicaltrials.gov(NCT02514772);2.Clinicaltrials.gov(NCT01274182);3.Smolenetal.AnnRheumDis2017;76:1598–1602;4.Clinicaltrials.gov(NCT01933516);5.Clinicaltrials.gov(NCT01419665);6.JurczakW,etal.LancetHaematol2017Jul13[Epubaheadofprint]
ClinicaltrialassessingthesafetyandPKofGP2013weeklymonotherapyinJapanesepaGentswithindolentNHL4
• N=6
GP13-201ASSIST-RA
GP13-301ASSIST-FL
GP13-302ASSIST-RT
GP13-101JP-trial
Oncologytrials
Totalsafetydata:c.1000paGents(500receivingGP2013),efficacydata:312(RA)+629(FL)paGents
RAtrials
Prof.WojciechJurczakMD,PhD
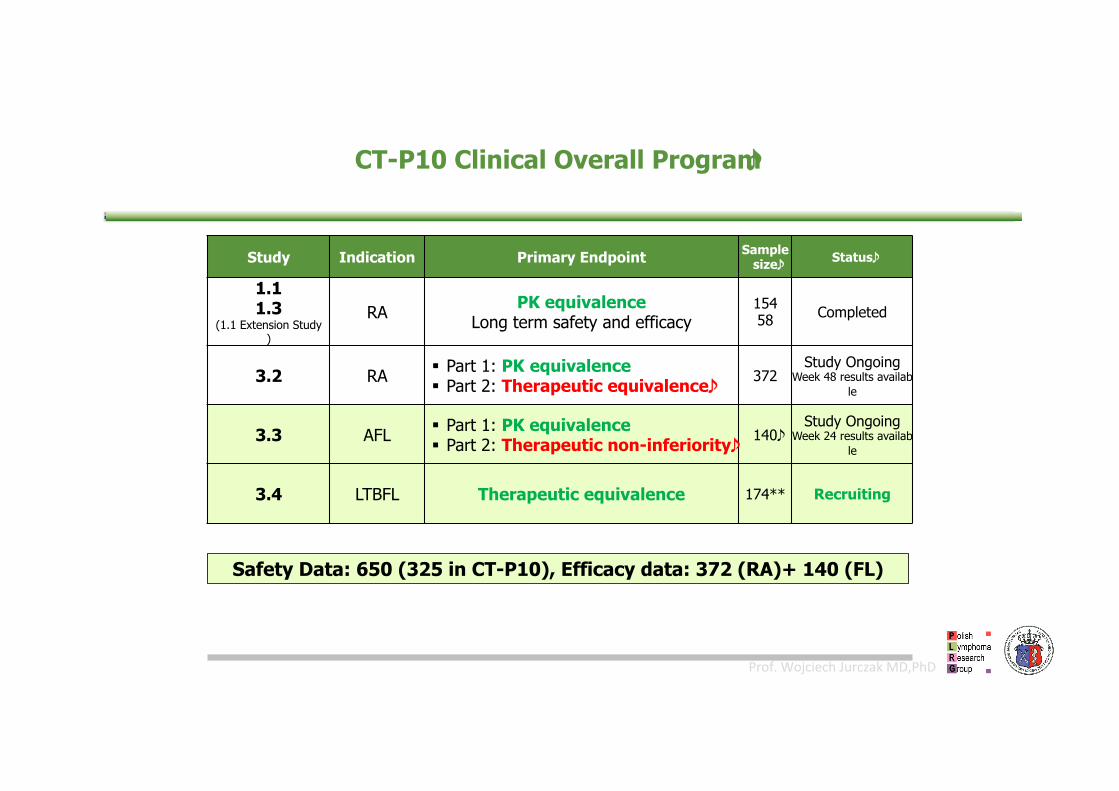
CT-P10 Clinical Overall Program
Study Indication Primary Endpoint Sample size Status
1.1 1.3
(1.1 Extension Study)
RA PK equivalence Long term safety and efficacy
154 58 Completed
3.2 RA § Part 1: PK equivalence § Part 2: Therapeutic equivalence 372
Study Ongoing Week 48 results availab
le
3.3 AFL § Part 1: PK equivalence § Part 2: Therapeutic non-inferiority 140
Study Ongoing Week 24 results availab
le
3.4 LTBFL Therapeutic equivalence 174** Recruiting
Safety Data: 650 (325 in CT-P10), Efficacy data: 372 (RA)+ 140 (FL)

Prof.WojciechJurczakMD,PhD
PharmacokineGcs-(AUC(0-inf))-(PAS)
Serumconcentradon-dmeprofilesforthetwotreatmentsweresimilaruptoweek24AUC(0-inf),Theareaundertheconcentradon-dmecurvefromdmezerotoinfinity;FAS,fullanalysisset;PK,pharmacokinedcs;SD,standarddeviadon*ThePKanalysissetwasasubsetoftheFASandconsistedofpadentswhodidnothaveanymajorprotocoldeviadons
ArithmeGcmean(SD)serumPKconcentraGon-Gmeprofileover24weeksbytreatment(PKanalysisset*)
SmolenJetal.,EULARcongress,8-11June,LondonUK:FRI0222

Prof.WojciechJurczakMD,PhD
Pharmacodynamics-peripheralBcelldepleGonB-cellcoun
t(%)
Time(weeks)GP2013 Time(weeks)CT-P10
GeometricmeanraGoinAUEC0-14d1.019(95%CI:0.997,1.042)
GP2013
Referencerituximab
Median (±SE) B-cell Kinetics (cells/µL)
CT-P10 3.2 RA

Prof.WojciechJurczakMD,PhD
CT-P10 3.2 RA
EfficacyDAS(DisesseAcGvityScore)
Prof.WojciechJurczakMD,PhD
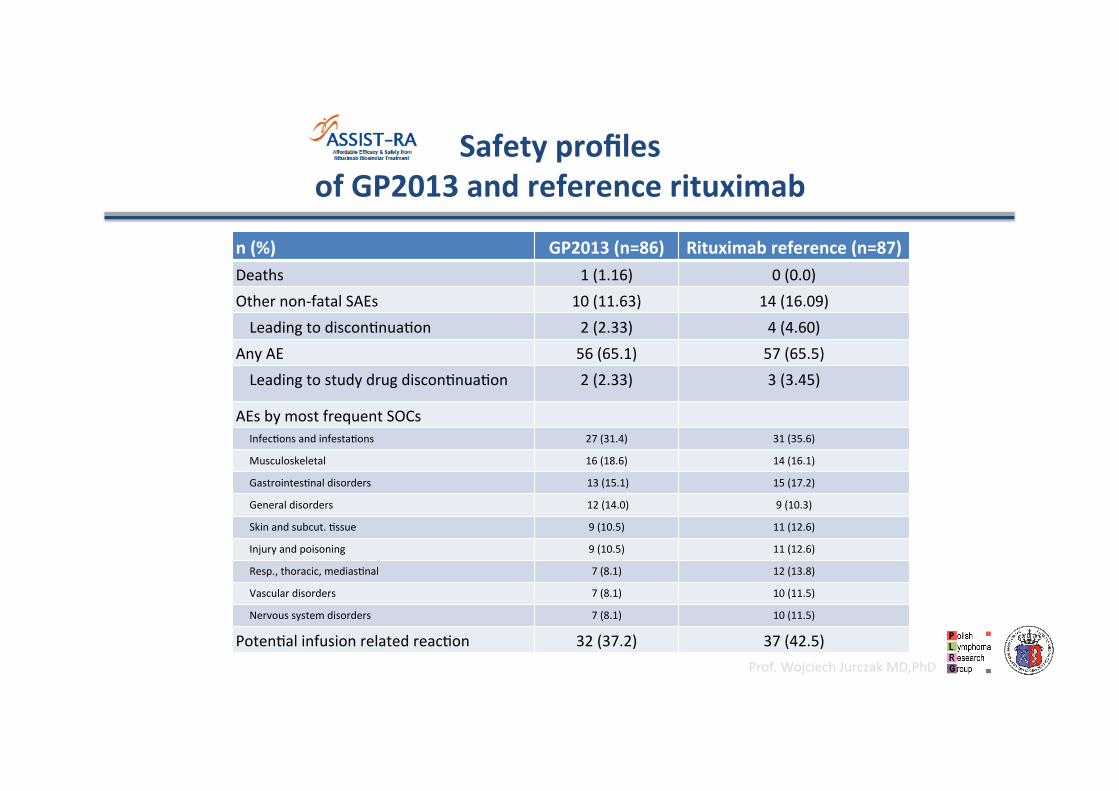
SafetyprofilesofGP2013andreferencerituximab
n(%) GP2013(n=86) Rituximabreference(n=87) Deaths 1(1.16) 0(0.0) Othernon-fatalSAEs 10(11.63) 14(16.09) Leadingtodiscondnuadon 2(2.33) 4(4.60)
AnyAE 56(65.1) 57(65.5) Leadingtostudydrugdiscondnuadon 2(2.33) 3(3.45)
AEsbymostfrequentSOCs Infecdonsandinfestadons 27(31.4) 31(35.6)
Musculoskeletal 16(18.6) 14(16.1)
Gastrointesdnaldisorders 13(15.1) 15(17.2)
Generaldisorders 12(14.0) 9(10.3)
Skinandsubcut.dssue 9(10.5) 11(12.6)
Injuryandpoisoning 9(10.5) 11(12.6)
Resp.,thoracic,mediasdnal 7(8.1) 12(13.8)
Vasculardisorders 7(8.1) 10(11.5)
Nervoussystemdisorders 7(8.1) 10(11.5)
Potendalinfusionrelatedreacdon 32(37.2) 37(42.5)

Prof.WojciechJurczakMD,PhD
Events, n (%) CT-P10
(N=161) US-RTX (N=151)
EU-RTX (N=60)
RTX (N=211)
AE - Related
122 (75.8)
73 (45.3)
96 (63.6)
47 (31.1)
37 (61.7)
25 (41.7)
133 (63.0)
72 (34.1) SAE - Related
13 (8.1) 0
14 (9.3) 5 (3.3)
2 (3.3) 1 (1.7)
16 (7.6) 6 (2.8)
Infection - Related
61 (37.9)
27 (16.8)
53 (35.1)
25 (16.6)
17 (28.3)
6 (10.0)
70 (33.2)
31 (14.7)
IRR 33 (20.5) 12 (7.9) 13 (21.7) 25 (11.8)
Malignancy 0 2 (1.3) 1 (1.7) 3 (1.4) Discontinuation due to AEs - Related
3 (1.9)
2 (1.2)
7 (4.6)
5 (3.3)
2 (3.3)
1 (1.7)
9 (4.3)
6 (2.8)
CT-P10 3.2 RA SafetyprofilesofCTP-10andreferencerituximab
Prof.WojciechJurczakMD,PhD
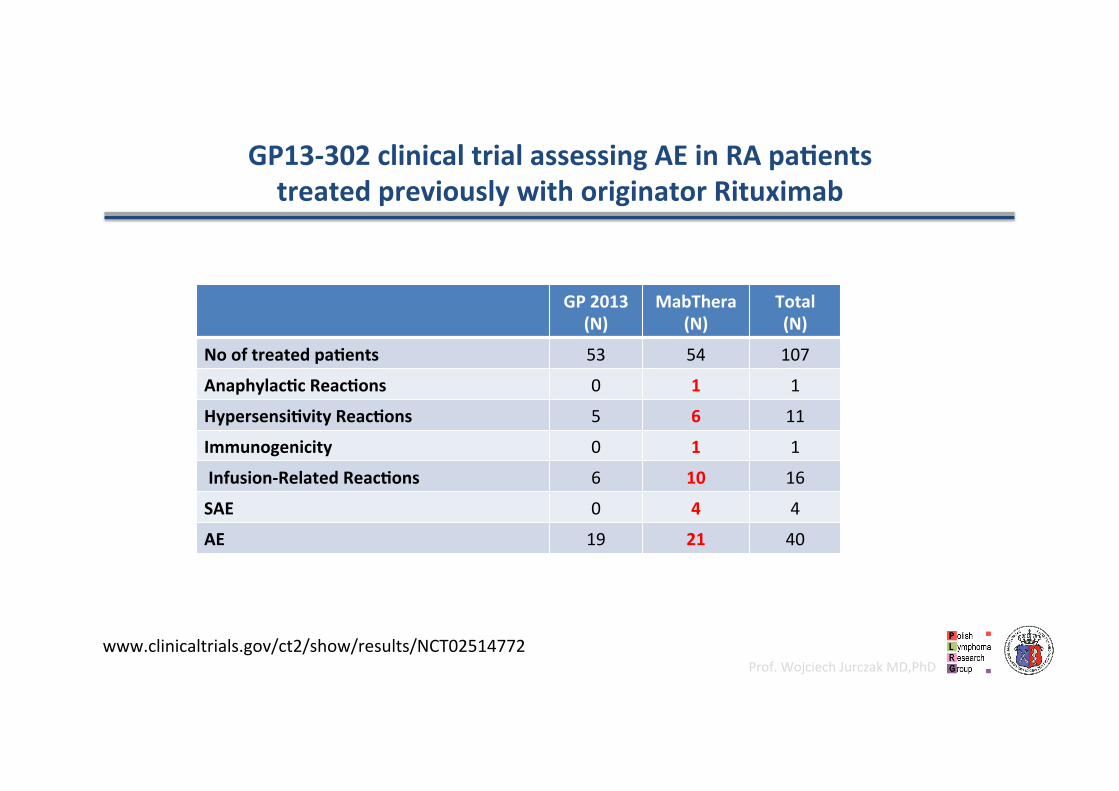
GP13-302clinicaltrialassessingAEinRApaGentstreatedpreviouslywithoriginatorRituximab
GP2013(N)
MabThera(N)
Total(N)
NooftreatedpaGents 53 54 107
AnaphylacGcReacGons 0 1 1
HypersensiGvityReacGons 5 6 11
Immunogenicity 0 1 1
Infusion-RelatedReacGons 6 10 16
SAE 0 4 4
AE 19 21 40
www.clinicaltrials.gov/ct2/show/results/NCT02514772

Prof.WojciechJurczakMD,PhD
:studyraGonale
• ASSIST-FLwasdesignedtoconfirmnon-inferiorclinicaleffecGvenessofGP2013ascomparedtooriginatorrituximabinasensidvepopuladon
• Follicularlymphomawaschosenasthemostappropriateindicadonasthediseasehasamorehomogeneousnatureamongsttheapprovedoncologyindicadonsofrituximab
• Further,thecombinadonR-CVPwasconsideredthemostsensiGvetreatmentopGon,asrituximabhadshownthelargestaddidvetreatmenteffecttoachemotherapybackbonetreatmentinthecombinadonwithCVP
• ImmunochemotherapywithRituximabremainsthecurrentstandardofcareforpreviouslyuntreatedpadents,thecombinadonregimenincreasestheRRandprolongsbothPFSandOS
CT-P10 3.3 AFL
JurczakW,etal.Abstract1809presentedatthe58thASHSanDiego,USA,3–6December2016.CoiffierB,etalAbstract1807presentedatthe58thASH,SanDiego,USA,3–6December2016.

Prof.WojciechJurczakMD,PhD
EquivalentEfficacyofaBiosimilarRituximabandReferenceRituximabinPreviouslyUntreatedAdvancedFollicular
Lymphoma:ExtendedResultsofASSIST-FL,aConfirmatoryPhaseIIIStudy
WojciechJurczak;IlidiaMoreira;KanakaSefyGovindbabu;EduardoMunhoz;Maria-AsuncionEcheveste;PratyushGiri;NelsonCastro;JulianaPereira;LuizaAkria;SergeyAlexeev;DzhalilOsmanov;PeijuanZhu;SiykaAlexandrova;AngelaZubel;OlofHarlin;JufaAmersdorffer
Jurczaketal,ESMO2017,LancetHematol2017

Prof.WojciechJurczakMD,PhD
(GP13-301):629randomizedptsin22countries
India: 95 Japan: 29
Russia: 46
Colombia: 2
Brazil: 102
Ukraine: 21 Poland: 42
Germany: 2 Austria: 6 Netherlands: 17
UK: 1 Ireland: 2
France: 9
Spain: 37 Portugal: 33 Italy: 23
Greece: 9
South Africa: 28
Peru: 9
Argentina: 5
Bulgaria: 15 Romania: 13 Hungary: 14
Australia: 27
Malaysia: 30
Israel: 12
Jurczaketal,ESMO2017,LancetHematol2017

Prof.WojciechJurczakMD,PhD
ASSIST-FL:AprospecGve,mulGcenter,randomized,double-blind,acGve-controlled,parallel-group,confirmatory,PhaseIIItrial
GP2013 375 mg/m2 + CVP (n=312‡) N=629
• ≥18 years of age • Treatment-naïve, advanced-stage, CD20-
positive, stage III/IV FL (Ann Arbor classification)
• WHO histologic grade 1, 2 or 3a FL • At least one measurable lesion • ECOG performance status 0–2
Screening ≤28 days
GP2013 375 mg/m2 every 3 months*
Combination treatment period
Maintenance period (responders only)
2 years
Reference rituximab 375 mg/m2 + CVP (n=315)
24 weeks (8 cycles)
Reference rituximab 375 mg/m2 every 3 months*
R1:1 Stratification: FLIPI risk group and geographical region
‡2padentsweremis-randomized;*ExceptinItaly,wheremaintenancetherapywasadministeredevery2monthsCVP,cyclophosphamide,vincrisdne,prednisone;ECOG,EasternCooperadveOncologyGroup;FL,follicularlymphoma;FLIPI,FollicularLymphomaInternadonalPrognosdcIndex;WHO,WorldHealthOrganizadon
Jurczaketal,ESMO2017,LancetHematol2017

Prof.WojciechJurczakMD,PhD
Studyassessments
Efficacy
• Efficacyassessments:• primaryendpoint:• Overallresponserate(ORR)
• Secondaryendpoints:• Completeresponse(CR)• Pardalresponse(PR)• Progressionfreesurvival(PFS)• Overallsurvival(OS)
Safety(secondaryendpoints)
• Safetyassessments:AEs,SAEs,withtheirseverityandreladonshiptostudydrug,pregnancies,monitoringofhematology,bloodchemistryandurine,vitalsigns,performancestatus,ECG,andbodyweight
• Immunogenicity:ADAformadon
PK/PD
(secondaryendpoints)
• PK:Cmax,Ctrough,AUC(0-t),andAUCall
• PD:peripheralCD19+Bcellcounts(absoluteandreladvetobaseline)andAUEC(0-21)inCycle1
CT-P10 3.3 AFL PK being the primary target, ORR the secondary target
JurczakW,etal.Abstract1809presentedatthe58thASHSanDiego,USA,3–6December2016.CoiffierB,etalAbstract1807presentedatthe58thASH,SanDiego,USA,3–6December2016.
Prof.WojciechJurczakMD,PhD
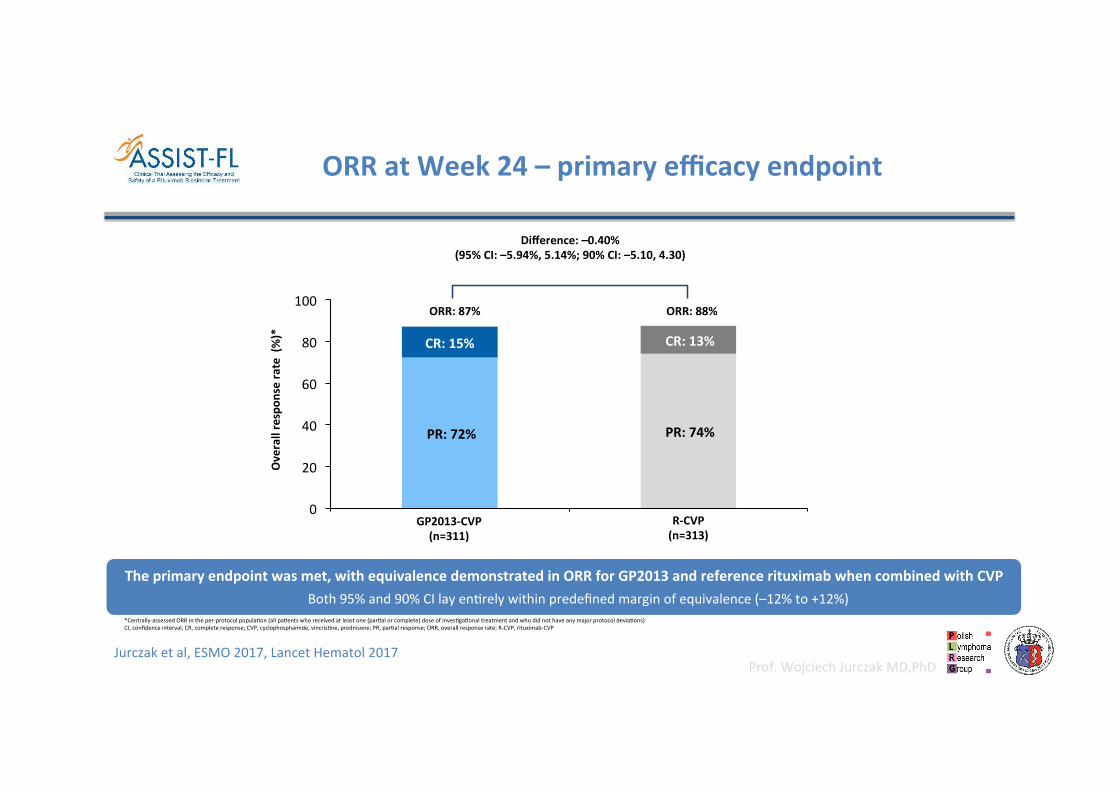
ORRatWeek24–primaryefficacyendpoint
Theprimaryendpointwasmet,withequivalencedemonstratedinORRforGP2013andreferencerituximabwhencombinedwithCVPBoth95%and90%CIlayendrelywithinpredefinedmarginofequivalence(–12%to+12%)
*Centrally-assessedORRintheper-protocolpopuladon(allpadentswhoreceivedatleastone(pardalorcomplete)doseofinvesdgadonaltreatmentandwhodidnothaveanymajorprotocoldeviadons)CI,confidenceinterval;CR,completeresponse;CVP,cyclophosphamide,vincrisdne,prednisone;PR,pardalresponse;ORR,overallresponserate;R-CVP,rituximab-CVP
PR:72% PR:74%
CR:15% CR:13%
0
20
40
60
80
100
Overallrespon
sera
te(%)*
ORR:87% ORR:88%
Difference:–0.40%(95%CI:–5.94%,5.14%;90%CI:–5.10,4.30)
GP2013-CVP(n=311)
R-CVP(n=313)
Jurczaketal,ESMO2017,LancetHematol2017
Prof.WojciechJurczakMD,PhD
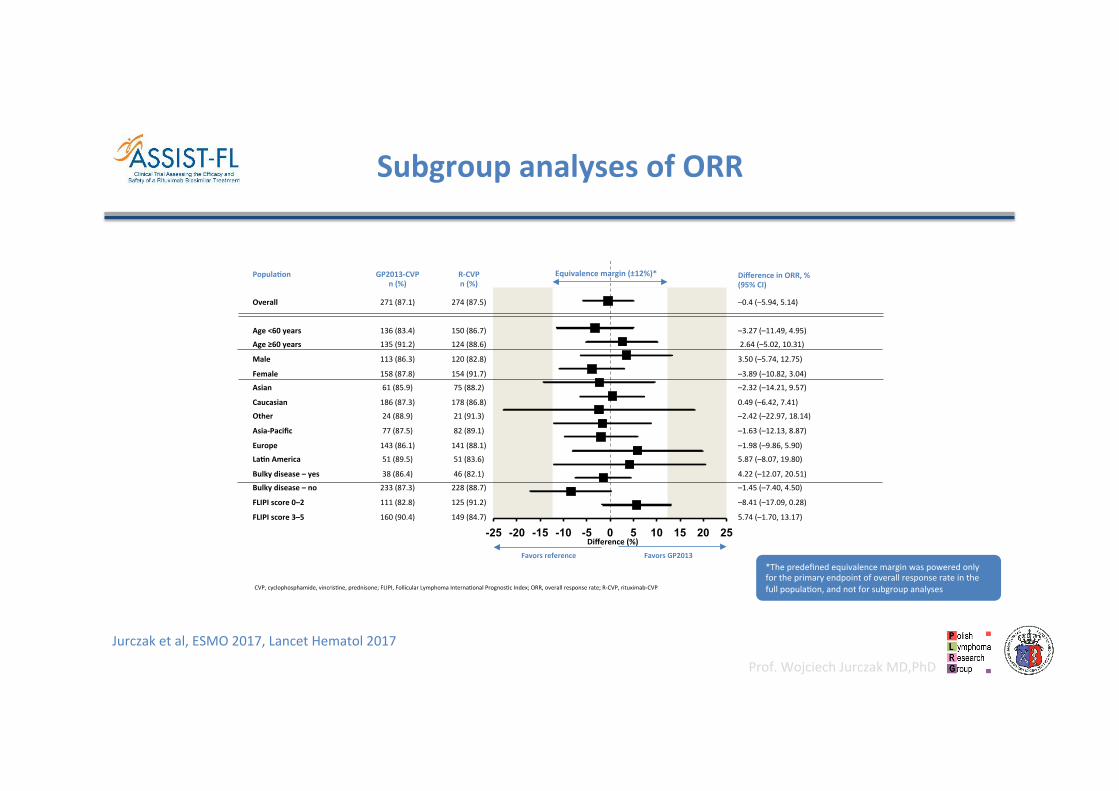
PopulaGon GP2013-CVPn(%)
R-CVPn(%)
DifferenceinORR,%(95%CI)
Overall
Age<60years
Age≥60years
Male
Female
Asian
Caucasian
Other
Asia-Pacific
Europe
LaGnAmerica
Bulkydisease–yes
Bulkydisease–no
FLIPIscore0–2
FLIPIscore3–5
271(87.1)
136(83.4)
135(91.2)
113(86.3)
158(87.8)
61(85.9)
186(87.3)
24(88.9)
77(87.5)
143(86.1)
51(89.5)
38(86.4)
233(87.3)
111(82.8)
160(90.4)
274(87.5)
150(86.7)
124(88.6)
120(82.8)
154(91.7)
75(88.2)
178(86.8)
21(91.3)
82(89.1)
141(88.1)
51(83.6)
46(82.1)
228(88.7)
125(91.2)
149(84.7)
–0.4(–5.94,5.14)
–3.27(–11.49,4.95)
2.64(–5.02,10.31)
3.50(–5.74,12.75)
–3.89(–10.82,3.04)
–2.32(–14.21,9.57)
0.49(–6.42,7.41)
–2.42(–22.97,18.14)
–1.63(–12.13,8.87)
–1.98(–9.86,5.90)
5.87(–8.07,19.80)
4.22(–12.07,20.51)
–1.45(–7.40,4.50)
–8.41(–17.09,0.28)
5.74(–1.70,13.17)
-25 -20 -15 -10 -5 0 5 10 15 20 25
SubgroupanalysesofORR
CVP,cyclophosphamide,vincrisdne,prednisone;FLIPI,FollicularLymphomaInternadonalPrognosdcIndex;ORR,overallresponserate;R-CVP,rituximab-CVP
Equivalencemargin(±12%)*
FavorsGP2013Favorsreference
Difference(%)
*Thepredefinedequivalencemarginwaspoweredonlyfortheprimaryendpointofoverallresponserateinthefullpopuladon,andnotforsubgroupanalyses
Jurczaketal,ESMO2017,LancetHematol2017

Prof.WojciechJurczakMD,PhD
PFS&OS–secondaryefficacyendpoints
• ASSIST-FLwasnotpoweredtoevaluatecomparabilityintermsofPFSandOS–theseendpointsarenotintendedtobeusedtoconfirmbiosimilarity• Dataarecurrentlyimmature,withahighproporGonofpaGentscensored(~70–90%)• TheobservedhazardraGosforPFSandOSareinconsistent,suggesGngthatcurrentresultsarelikelyduetorandomvariaGonandnotactualtreatment
differences
Outcome†GP2013-CVPN=312,n(%)
R-CVPN=315,n(%)
HazardraGo(90%CI)*
PFS
Event,n(%) 94(30) 76(24) 1.31(1.02,1.69)
Censoredevents,n(%) 218(70) 239(76)
Kaplan-Meieresdmate,median Notreached Notreached
OS
Event,n(%) 23(7) 29(9) 0.77(0.49,1.22)
Censoredevents,n(%) 289(93) 286(91)
Kaplan-Meieresdmate,median Notreached Notreached
Jurczaketal,ESMO2017,LancetHematol2017

Prof.WojciechJurczakMD,PhD
46
Patients with CD20+
confirmed FL
Randomization 1:1
(N=134)
Core Study Period
24 weeks
Maintenance Study Period
2 years (for responders; CR, CRu or PR)
Follow-up Period: Up to 3 years from the Day 1 of Cycle 1 of the last patient
EOT1
EOT2
CT-P10² + CVP1
(n=67)
Rituxan² + CVP (n=67)
Rituxan
CT-P10
1. CVP: Cyclophosphamide 750 mg/m2, Vincristine 1.4 mg/m2 [max 2mg], Prednisone or prednisolone 40 mg/m2 2. Rituximab: 375 mg/m2 (Core study: 3-weekly, Maintenance study: every 2 months)
Abbreviations: FL, Follicular Lymphoma; EOT, End of Treatment; FLIPI, Follicular Lymphoma International Prognostic Index
Stratification Factor § Gender: Male vs. Female § FLIPI score: 0-2 vs. 3-5 § Country
StudydesignCT-P10 3.2 RA
CoiffierB,etalASH2017,LancetHematology2017

Prof.WojciechJurczakMD,PhD
ITT Population
Response CT-P10 (N=70)
Rituxan (N=70)
Difference [lower bound of 95%
CI]
ORR1 67 (95.7%) 63 (90.0%) 5.7% [-3.41%]
CR 21 (30.0%) 15 (21.4%) -
CRu 6 (8.6%) 8 (11.4%) -
PR 40 (57.1%) 40 (57.1%) -
The difference between the groups lies on the positive side of -7%. lower bound of 95% CI of differences lies on the positive side of -7%.
Efficacyresults(ORR)–secondaryendpointCT-P10 3.2 RA
CoiffierB,etalASH2017,LancetHematology2017

Prof.WojciechJurczakMD,PhD
ResearchonBiosimilars:pivotaltrialsandprinciplesWojciechJurczak,ArnoldGVulto,JufaAmersdorffer,WonSKim,BertrandCoiffierTheLancetHaematology,Vol.4,No.9,e409–e410Published:September,2017RituximabbiosimilarandreferencerituximabinpaGentswithpreviouslyuntreatedadvancedfollicularlymphoma(ASSIST-FL):primaryresultsfromaconfirmatoryphase3,double-blind,randomised,controlledstudyWojciechJurczak,IlídiaMoreira,GovindBabuKanakasefy,EduardoMunhoz,MariaAsunciónEcheveste,PratyushGiri,andothersTheLancetHaematology,Vol.4,No.8,e350–e361Published:July13,2017Rituximabbiosimilars:introducGonintoclinicalpracGceShinichiMakita,KenseiTobinaiTheLancetHaematology,Vol.4,No.8,e342–e343Published:July13,2017Efficacy,pharmacokineGcs,andsafetyofthebiosimilarCT-P10comparedwithrituximabinpaGentswithpreviouslyuntreatedadvanced-stagefollicularlymphoma:arandomised,double-blind,parallel-group,non-inferiorityphase3trialWonSeogKim,ChrisdanBuske,MichinoriOgura,WojciechJurczak,Juan-ManuelSancho,EdvardZhavrid,andothersTheLancetHaematology,Vol.4,No.8,e362–e373Published:July13,2017
July17wasamilestoneinRituximabbiosimilardeveloppment

Prof.WojciechJurczakMD,PhD
:summary
ORR with GP2013 and CT-P10 equivalent to reference rituximab
PK (Cmax) of GP2013 and CT-P10 equivalent to reference rituximab
1 2
Medians not yet reached for PFS and OS 3 PD (B-cell depletion) with GP2013 and CT-P10 equivalent to reference rituximab 4 No clinical meaningful differences between GP2013 or CT-P10 and reference rituximab in safety, tolerability or immunogenicity 5
CT-P10 3.2 RA
No clinical meaningful differences between GP2013 or CT-P10 and reference rituximab in safety, tolerability or immunogenicity 5 Registered by EMA 6
Jurczaketal,ESMO2017,LancetHematol2017CoiffierB,etalASH2017,LancetHematology2017
Prof.WojciechJurczakMD,PhD
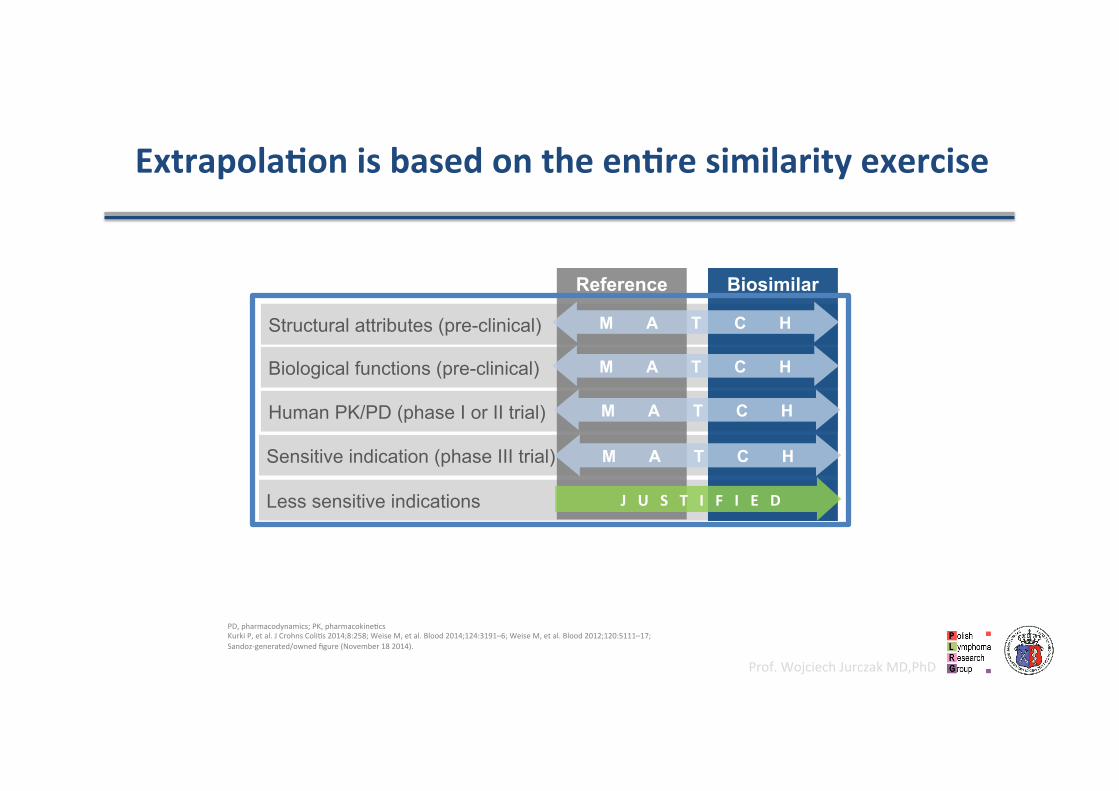
ExtrapolaGonisbasedontheenGresimilarityexercise
Structural attributes (pre-clinical)
Biological functions (pre-clinical)
Human PK/PD (phase I or II trial)
Less sensitive indications
Sensitive indication (phase III trial)
Reference Biosimilar
M A T C H
JUSTIFIED
M A T C H
M A T C H
M A T C H
PD,pharmacodynamics;PK,pharmacokinedcsKurkiP,etal.JCrohnsColids2014;8:258;WeiseM,etal.Blood2014;124:3191–6;WeiseM,etal.Blood2012;120:5111–17;Sandoz-generated/ownedfigure(November182014).

Prof.WojciechJurczakMD,PhD
RrituximabregistraGon&clinicalpracGce
• FL• IlineDLBCL• CLL• RA• GPA(Wegener’sgranulomatosis)
andMPA(microscopicpolyangiids)
MabTheraisamedicineusedtotreatthefollowingbloodcancersandinflammatorycondidons: • FL,MZL,LPL
• IlineDLBCL,R/RDLBCL• CLL• MCL• RA• GPA(Wegener’sgranulomatosis)
andMPA(microscopicpolyangiids)
Prof.WojciechJurczakMD,PhD
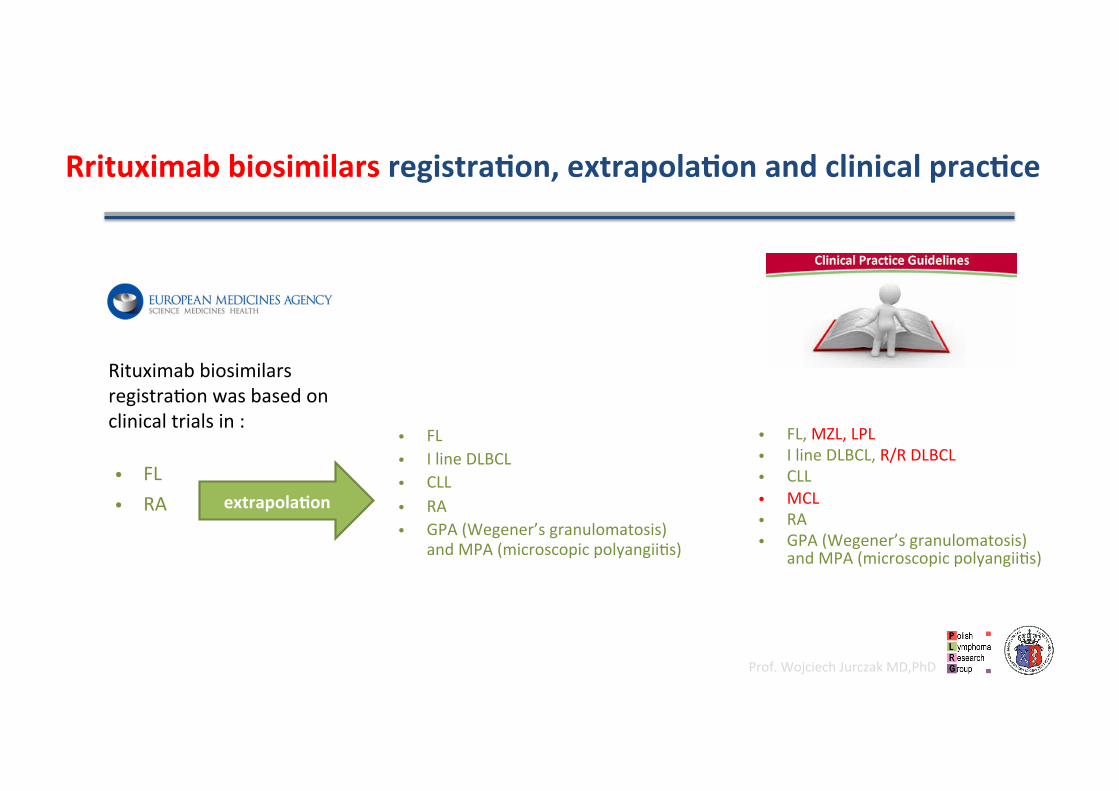
RrituximabbiosimilarsregistraGon,extrapolaGonandclinicalpracGce
• FL• RA
Rituximabbiosimilarsregistradonwasbasedonclinicaltrialsin:
• FL,MZL,LPL• IlineDLBCL,R/RDLBCL• CLL• MCL• RA• GPA(Wegener’sgranulomatosis)
andMPA(microscopicpolyangiids)
• FL• IlineDLBCL• CLL• RA• GPA(Wegener’sgranulomatosis)
andMPA(microscopicpolyangiids)
extrapolaGon
Prof.WojciechJurczakMD,PhD
Conclusions:
• RituximabbiosimilarsaregoodqualityMoAbwithasafetyandefficacyprofileidendcaltotheiroriginator
• TheirsimilaritytoRituximabwasdeterminedbyextensivepre-clinicalanalyses,andfinallyconfirmedbyclinicaltrials,withnearly2000parGcipaGngpaGents
• SubcutaneousRituximabistheonlycompedtortoRituximabbiosimilarsintheIlineBcellNHLtherapy
• Chlorambucil+Obinutuzumabistheonlyprotocol,withnovelandCD20MoAb,befertoRituximabbasedIlineimmuno-chemotherapyregimens

Prof.WojciechJurczakMD,PhD
Prof.WojciechJurczak,M.D.,Ph.D.DptofHematology,[email protected],(+48602338290)







