
INMUNOSENESCENCIA AUTOINMUNIDAD/INFLAMACION Y
ENVEJECIMIENTO(INFLAMM-AGING THEORY)
2012-UpdatedJ. Alijotas-Reig M.D, PhD. Consultor. Servicio Enfermedades Autoinmunes Sistémicas -
Medicina Interna I. Hospital Universitario Vall d’Hebron. Laboratorio de Biologia, Oncología Molecular y Envejecimiento. CIBBIM-F. Investigación Vall d’Hebron. Departamento de Medicina. Facultad de Medicina. U.A.B
CURSO DE MEDICINA DEL ENVEJECIMIENTO
FISIOLOGICO
Curso 2012-13
TEORIAS MOLECULARES Y GENETICAS
Mutaciones somáticas y alteraciones en la reparación del ADN
Erroes catastróficos de transcripción o de translocación
Alteraciones o diversidad de gerontogenes (LAG-1)
Telómeros
Presencia de apoE4
Mutación del precursor de la beta amiloide
TEORIAS CELULARES
T. de Hayflick
T. de los radicales libres
T. mitocondrial
T. de la glicosilación proteica
TEORIAS DE SISTEMAS
T. Neuroendocrina
T. Inmune-autoinmune (inflamatoria, INFLAMM-AGEING THEORY)
PRINCIPALES TEORIAS SOBRE EL ENVEJECIMIENTO

INMUNOLOGIA Y ENVEJECIMEINTO
• CONCEPTOS BÁSICOS DE INMUNOLOGÍA
• MODIFICACIONES FISIOLÓGICAS DEL SISTEMA INMUNE RELACIONADAS CON LA EDAD
• ENVEJECIMIENTO Y ENFERMEDADES AUTOINMUNES ORGANOESPECÍFICAS Y NO ORGANOESPECÍFICAS
• RELACIÓN ENTRE AUTOINMUNIDAD, INFLAMACION Y ENVEJECIMIENTO: LA ARTERIOSCLEROSIS COMO MODELO
• MODELO EXPERIMENTAL: SENESCENCIA CELS HUVEC
Sistema Inmune Fisiológico


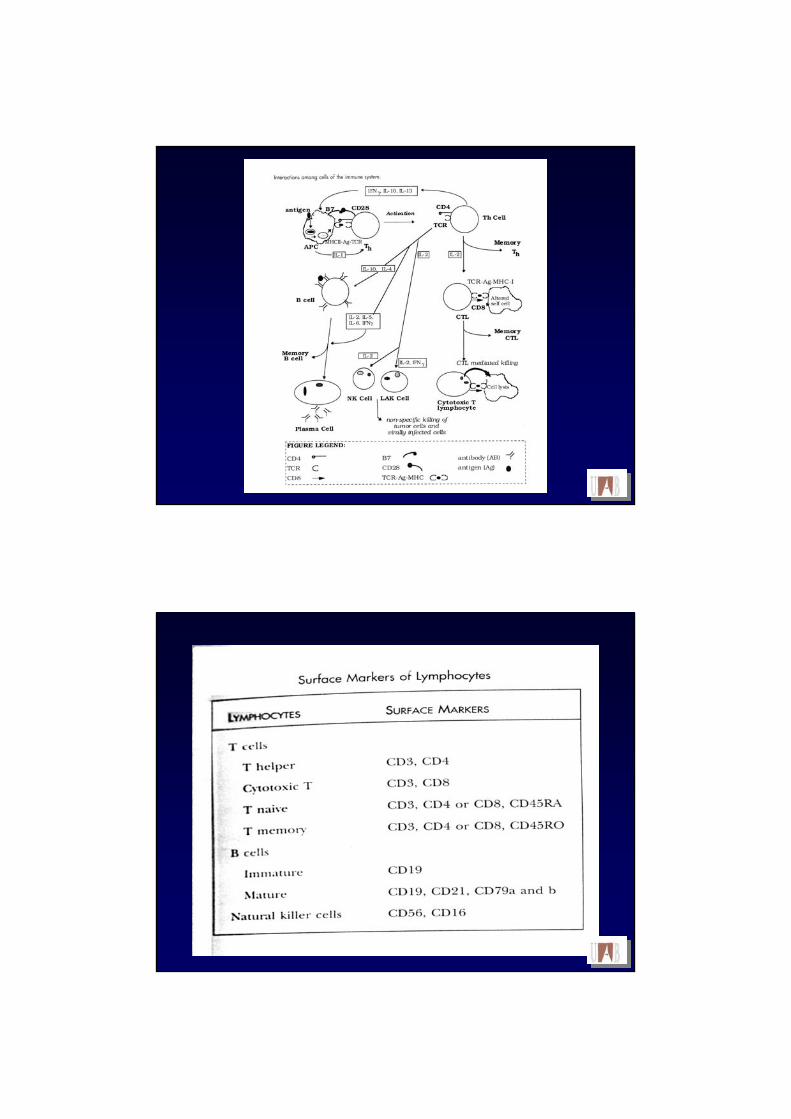
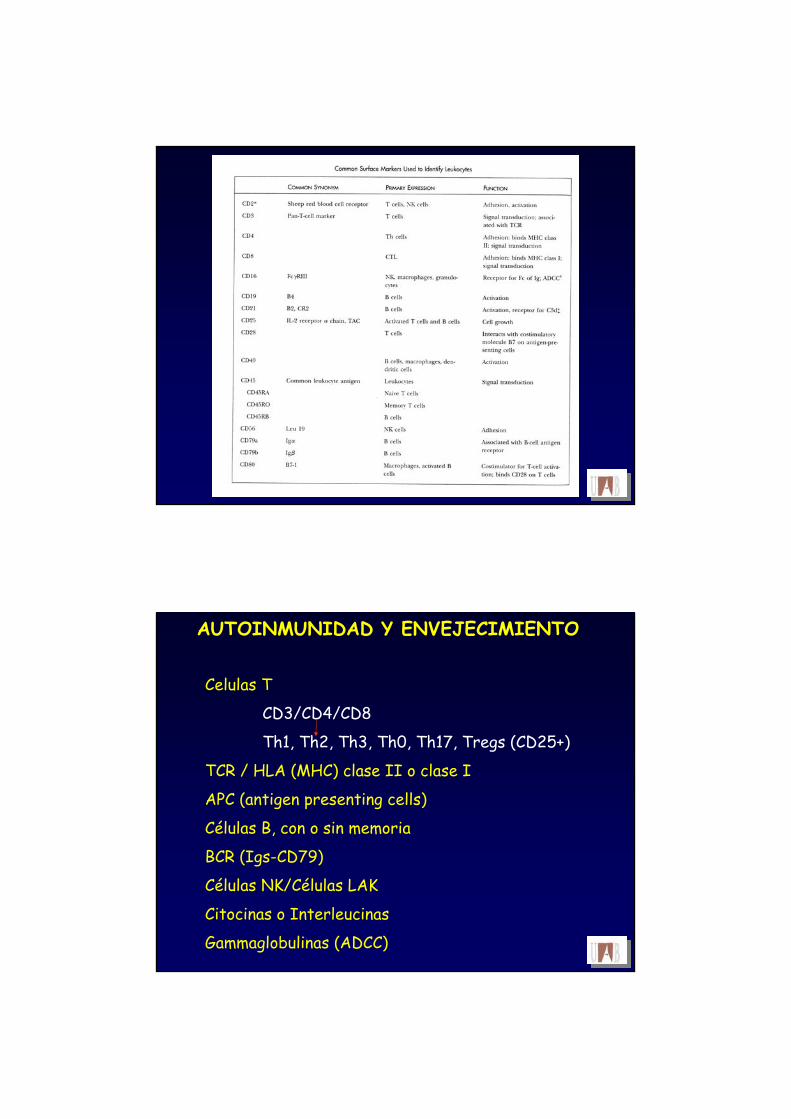
AUTOINMUNIDAD Y ENVEJECIMIENTO
Celulas T
CD3/CD4/CD8
Th1, Th2, Th3, Th0, Th17, Tregs (CD25+)
TCR / HLA (MHC) clase II o clase I
APC (antigen presenting cells)
Células B, con o sin memoria
BCR (Igs-CD79)
Células NK/Células LAK
Citocinas o Interleucinas
Gammaglobulinas (ADCC)

AUTOINMUNIDAD Y ENVEJECIMIENTO
Celulas T
CD4:
Th1: IL-2 , IL-3, gamma-IFN, TNF-alfa, GM-CSF
Th2: IL-3, IL-4, IL-5, IL-6,IL-10, IL-13
Th0: Th1 + Th2
Th3: TGF-beta, IL-10
(acción parecida a LT supresor)
T-regs (CD25+ / Foxp3+)
Th17: IL-17, IL-23

AUTOINMUNIDAD Y ENVEJECIMIENTO
Celulas T
CD3/CD4/CD8
Th1, Th2, Th3, Th0, Th17, Tregs
TCR / HLA (MHC) clase II o clase I
APC (antigen presenting cells)
Células B, con o sin memoria
BCR (Igs-CD79)
Células NK/Células LAK
Citocinas o Interleucinas
Gammaglobulinas (ADCC)
Linfocitos Thelper/inducer (CD4+)supresores/citotoxicos (CD8+)
Linfocitos Tsubtipo Th1subtipo Th2
Linfoctios Tcitocinas específicas fenotipo Th1citocinas específicas fenotipo Th2
citocinas tipo Th17 (hipotesis Th17)
Linfocitos TregTh12 /Th23 /Th3?

THE TH17 HYPOTHESIS
The Th1/Th2 hypothesis can not explain all immune reactions !There are flaws in the Th1/Th2 hypothesisie: EAE / RA / ME
Th17 hypothesis could explain cell mediated tissue damage in both:- autoimmunity - immunity triggered by microbial infection.
T-suppressor concept has never been demonstrated (gene-protein)New roles for IL-23.
IL-17 / IL-6 / TNF
Synergies, antogonists and fine tuning of Th17Th17 pathway has many of the features of Th1/Th2, with synergies as well as antagonistic interactionsamong cytocines.
IL-4 + ϒ-IFN ↓ IL-17
IL-6 + TGF-β ↑ IL-17
TGF-β alone no IL-17 response
TNF + IL-23 (IL-12) ↑ IL-17
ϒ-IFN IL-17
TNF IL-17
IL-27* ↓ IL-17
*member of IL-12 family
Preliminary suggestion:More than the action of a single cytokine to provoke cell-mediated tissue damage is required

Green arrows indiacate upregualtion, while red lines indicate inhibition. It has been identificated the transcription factors, specially for Th17
T-helper cell differentiation and regulation
CD25+ IL-2
Regulatory T cells (Tregs)5-10% of peripheral CD4+ T cells are CD25+CD25+ is the high affinity α-chain of the IL-2RThese cells included a subpopulation of Tregs that are
CD45RB and express:CD5, OX40, 4-1BB, CTLA-4, GINF-R
CD103+CD4+, CD25-, Foxp3-

Regulatory T cells (Tregs)CD4+, CD25+, Foxp3+ (forkhead box protein-3)CD4+/CD25+ T cells are heterogeneous T-cell population (CD25high)Treg are anergic but also suppressive T cellsControlling the host immune response to prevent collateral host damageCritical for protecting the host from self-reactive lymphocytes……Controlling the host alloimmune responses (grafts..)
Two different type CD4+ Tregs.
nTregs thymusiTregs peripheral CD4+ become suppressive capabilities if
low antigen dose, oral toleranceimmunotherapychronic antigen exposure
Both are inducible !!
NATURAL AND INDUCED REGULATORY T CELLS: ROLE OF FOXP3
• Foxp3 is a gene
• Foxp3 encodes a member of the forkhead/winged-helix family of transcripttionregalators, termed scurfin.
• Foxp3 has 3 functional domains
•IPEX syndrome, mutation of foxp3+ have been identified
• Mutation of Foxp3 scurfin alteration DNA modifications
• CD4+CD25+ are high levels of foxp3
• Overexpression of Foxp3 induced a suppressor and expansion of CED4CD25+ T cell
• Foxp3 is a key transcription factor in the development of natural CD4+CD25+ Tregs

NATURAL AND INDUCED REGULATORY T CELLS: ROLE OF FOXP3
• Mutation in the forkhead domain affect its ability to bind DNA
• Some mutation of the Foxp3 may do it non-functional
•Foxp3 bind to ARRE site promoter for IL-2 Inhibit IL-2 synthesis
• Foxp3 may also inhibit trnascriptional activation of Nuclear factor Activated T cells (NFAT)
• Foxp3 could function as a transcriptional activator and repressor
• Foxp3 and TCR signalling in Treg cells (see figure)
FoxP3 is the most specific and functional marker of CD4+CD25+ Tregs
FoxP3 blockade
FoxP3 blockade

Regulatory T cells in the elderly• Ageing modify nTregs• Babies: 3-10% of CD4+ are also CD25+• Healthy adults (up to 60 years): 0,5-7% are CD25+• Healthy elderly >65 years: % of CD4+CD25+ is unclear
• Is advanced age associated with a decline functional capacity ofTregs? nTregs or iTregs?
Controversial
• Non-healthy people had more Tregs than their healthy counterparts• Are Foxp3 the definitive marker for Tregs ?• Is it necessary to CD127 to identify live Tregs?

AUTOINMUNIDAD Y ENVEJECIMIENTO




VIA DE LEPTINA
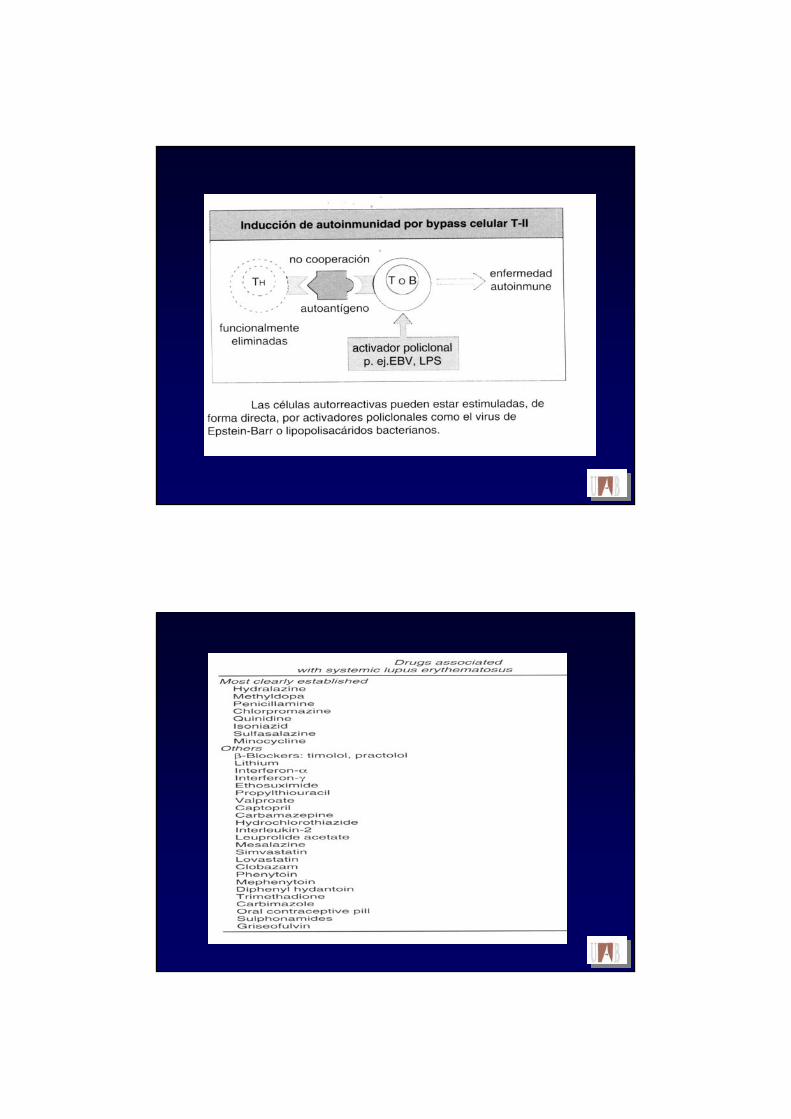
AUTOINMUNIDAD. TOLERANCIA INMUNOLÓGICA
MECANISMOS RESPONSABLES DE LA TOLERANCIA “A LO PROPIO” :
DELECCION CLONAL: apoptósis LT/LB inmaduros órganos linfoides 1ºs
ANERGIA CLONAL: falta de respuesta funcional:TCR / BCR – MHC-II
mol co-estimuladoras CD80-B7+/CD28+ CD 40/40-L
IGNORANCIA CLONALREGULACION ACTIVA: CITOCINAS: Th1 Th2
aumento actividad CD8 –supresoraRol de T-reg (CD4+,CD25+)
AUTOANTICUERPOS PROTECTORES

AUTOINMUNIDAD
AUTOINMUNIDAD:
ORGANO ESPECIFICA
NO ORGANO ESPECIFICA
AUTOANTICUERPO
DISFUNCION INMUNE
ENFERMEDAD AUTOINMUNE


AUTOINMUNIDAD Y ENVEJECIMIENTO
AUTOINMUNIDAD Y ENVEJECIMIENTO


AUTOINMUNIDAD Y ENVEJECIMIENTO
INMUNOSENESCENCIA
ALTERACION CELS. T? ? INVOLUCIÓN TIMICA
La restauracion de la función T en ancianos, conllevará la corrección de otros factores inmunes y ↓ las respuestas oxidativas y los reactantes de fase aguda. Esto mejoraría el envejecimiento.
Médula ósea?
INMUNOSENESCENCIA
Disminución de las células hematopoyéticas medularesAumento del tejido adiposoAlteración de las hormonas y citocinas del estroma medular
↑macrofagos pero ↓ síntesis y ecreción de IL-1 y TNF
-ve↓ 2ª de citocinas del estroma: IL-6/IL-11/M-CSF/GM-CSF/IL-7
No información contrastada sobre las células madre hematopoyéticas
Médula ósea:

INMUNOSENESCENCIA
HSCs se diferencian en CLP (common lymphoid progenitors)
B cell precursor pro-B pre-B LB
INMUNOSENESCENCIA:↓CLP ↓ pro-B ↓pre-B ↓LB
↓ IL-7 ?
Cuantitatia / cualitativa
Baja sensibilidad a IL-7)
INMUNOSENESCENCIAProgenitores de LT migran al timo: Pueden derivar de :• CLP-2 identificadas en el timo IL-7 sensibles
(Lin-, CD19- , B220+, c-Kitneg/lo, CD44hi, hCD25+,IL-7Rα+)• ETP (early T lineage progenitors)
(Lin-, CD44+, c-Kithi, , IL-7Rαneg/lo) IL-7 no sensibles
En la senescencia:
• No parece haber cambios en las CLP-2• Si parece haber disminución de las ETP
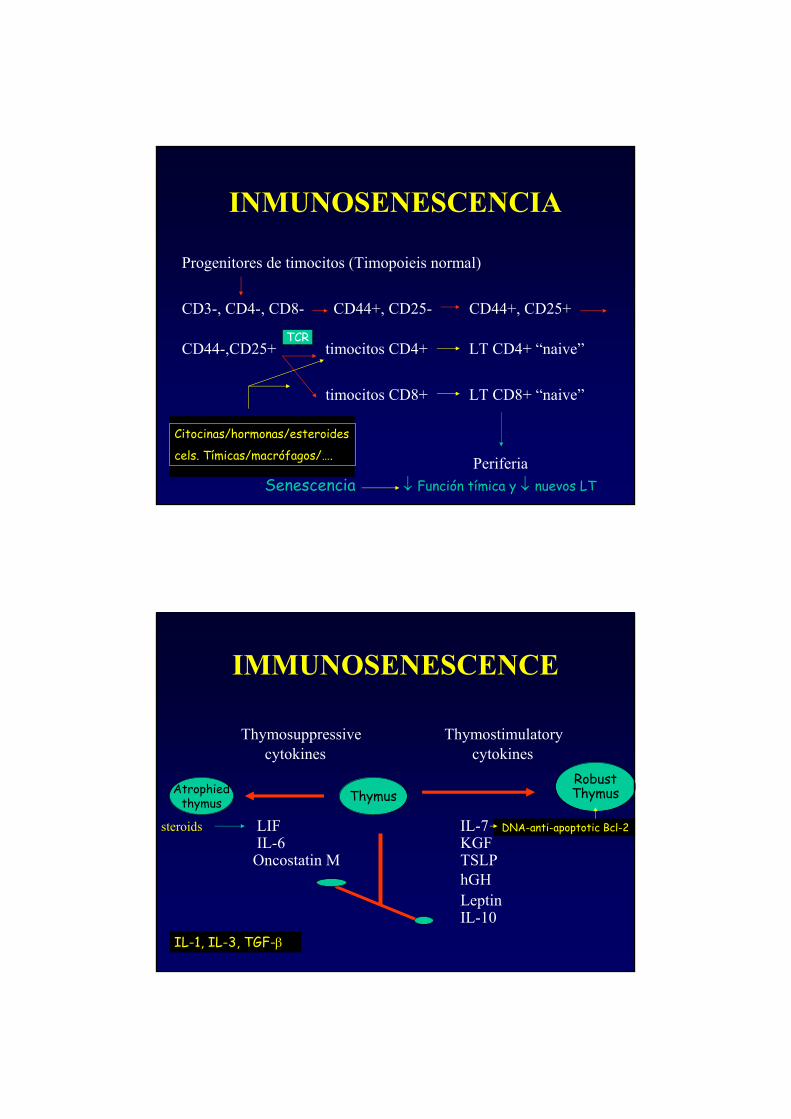
INMUNOSENESCENCIA
Progenitores de timocitos (Timopoieis normal)
CD3-, CD4-, CD8- CD44+, CD25- CD44+, CD25+
CD44-,CD25+ timocitos CD4+ LT CD4+ “naive”
timocitos CD8+ LT CD8+ “naive”
Periferia
TCR
Citocinas/hormonas/esteroides
cels. Tímicas/macrófagos/….
Senescencia ↓ Función tímica y ↓ nuevos LT
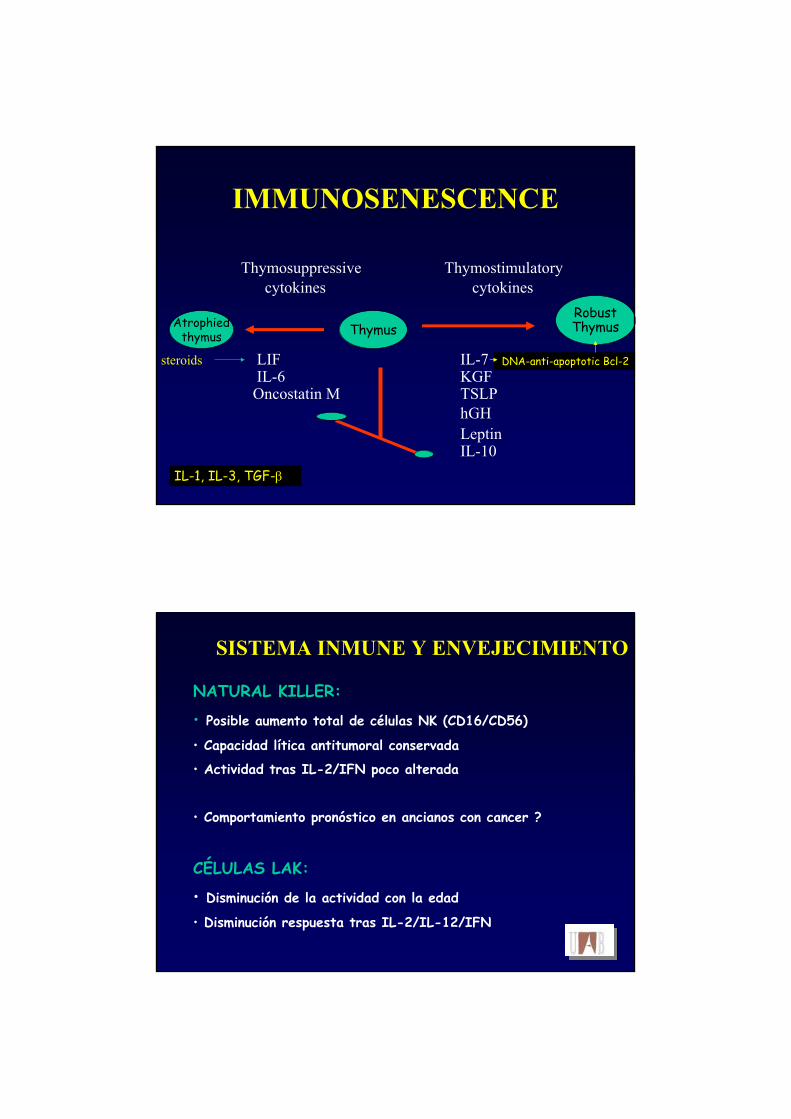
IMMUNOSENESCENCE
Thymosuppressive Thymostimulatorycytokines cytokines
steroids LIF IL-7IL-6 KGFOncostatin M TSLP
hGHLeptinIL-10
ThymusRobustThymusAtrophied
thymus
IL-1, IL-3, TGF-β
DNA-anti-apoptotic Bcl-2


ALTERACION MARCADA DEL COMPARTIMENTO T
• Pocos cambios cuantitativos• ↓ funcionalismo células T
• ↓ funcionalismo APC
• ↓ respuesta a inmunización activa
• ↓ reactividad a las pruebas cutáneas
• ↑ riesgo de infecciones y tumores
• ↑ riesgo de fenómenos autoinmunes (autoreactividad)
SISTEMA INMUNOLOGICO Y ENVEJECIMIENTO

AUTOINMUNIDAD Y ENVEJECIMIENTO
INMUNOLOGIA Y ENVEJECIMIENTO
• Compartimento T alterado: TCD4 y TCD8 (↓ linfocitotoxicidad)
• Alteración LT mas funcional que cuantitativa:
↑ CD29+/CD45R0+, ↓ CD45RA+
• Relación con estado de salud y nutricional del sujeto
• ↓ moleculas coestimuladoras: CD28
Predisposición a INFECCIONES, CANCER y AUTOINMUNIDAD

SISTEMA INMUNE Y ENVEJECIMIENTO
Altreraciones en la producción de citocinas:
predominio de Th1 sobre Th2
IL-2 ? / IL-2R IL-3?
IL-6 IL-4
α-TNF IL-5
IFN-γ IL-10
APCs IL-1

INMUNOLOGIA Y ENVEJECIMIENTO
Parámetro PJ PV Hombre/Mujer (p)
Leucocitos totales ND 0.003
Linfocitos ND 0.014
Neutrófilos ND <0.001
Monocitos ND 0.91 (↑ H )
Linfocitos B ND 0.003 (↑ M)
LT-CD4 + ND <0.001
LT-CD8 + ND <0.001 (↓ M)
CD4 / CD8 ND <0.001
Céls. NK ND 0.01 (↑ H )
IgG/ IgM / IgA ND 0.14
C3 /C4 ND 0.4 /0.75
Lázaro M, et al. Rev Clin Esp 2003;203:417-422
INMUNOLOGIA Y ENVEJECIMIENTOPruebas de hipersensibilidad retardada en función del sexo
(Multitest IMC 7+1)
Hombres Mujeres
Anergia 1 3
Positivos (>2mm) 77 99
Media Ags positivos 1.8 1.4
Ags positivos: 1 11 22
Ags positivos: 2 28 37
Ags positivos: 3 26 25
Ags positivos: 4 11 5
Ags positivos: 5 1 2Lázaro M, et al. Rev Ciln Esp 2003;203:417-422

INMUNOLOGIA Y ENVEJECIMIENTO
SITUACIONES ESPECIALES: Fumadores:
↑ CD8 (sangre, BAL, tejido pulmonar)
↑ CD8 si además de fumador, sufre una EPOC
↓ de linfocitos B
Alcohol:
↓ de linfocitos B (p<0.01)
Anérgia a pruebas cutaneas
Cancer:
↓de linfocitos B y linfocitos T
Aumento de células NK y ↓ de funcionalidad de NKLázaro M, et al. Rev Ciln Esp 2003;203:417-422
ENVEJECIMIENTO E INMUNIDAD•Compartimento B poco afectado cuantitativamente (CD19CD21)
•↑ respuesta policlonal antigeno-inespecífica
•↓ respuesta B antígeno-específica
•↓ síntesis de Ab con Ag conocidos (independiente de IL-3/4/5/10)
•Alteración de la maduración de linfocitos B.
•Alteración en la funcionalidad de los linfocitos B
•↑IgG/IgA y ↓IgM/IgD
•↑de los ac. Antiidiotipo (antiFab) ↓ booster
Predisposición a INFECCIONES, I AUTOINMUNIDAD
Regulatory T cells (Tregs) in the elderly
Ageing modify nTregsBabies: 3-10% of CD4+ are also CD25+Healthy adults (up to 60 years): 0,5-7% are CD25+Healthy elderly >65 years: % of CD4+CD25+ is unclear
Is advanced age associated with a decline functional capacity of Tregs? nTregs or iTregs?
Controversial
SISTEMA INMUNE Y ENVEJECIMIENTO
ALTERACION EN LAS “SEÑALES DE ACTIVACIÓN”
• No alteración TCR-CD3 en número
• ↑ Colesterol/fosfolípidos en TCR-CD3 ↑viscosidad
• Alteración actina-citoesqueleto TCR
• ↓ actividad proteincinasa C ↓ Ca F. Transcripción
• ↓ F. Transcripción nuclear ↓ expresión genes (c-Fos)

INMUNOSENESCENCIAmicroambiente: niveles de Zn y Zn-metalotioneinas
Involución tímica ↓timulina ↓ F/c LT
Mayor descenso de CD4+ que de CD8+
> CD4/CD8+CD45RO+ y < CD4/CD8+CD45RA+
Ojo: a > edad menos pérdida de CD4+CD45RA+
↓ expresió de la molécula CD28 (CD8+)
Alteración del repertorio TCR (CD8)
INMUNOSENESCENCIAPor que se produce la senescencia del compartimento T ?
Alteraciones en la hematopoyesis: ↓ factores de crecimiento↑ factores inhibidores (IL-6,..)
Alteraciones en diferenciación de linfocitos Tligado a la involució tímica
Agotamiento post-tímico: LT naive (senescencia post-mitótica Ag-independiente)LT memoria (senescencia replicativa Ag-dependiente)
Alteración de las moleculas co-estimuladoras: ↓CD28 ↓CD40
Alteración de citocinas: ↓ IL-2 / IL-4 / ↑ IL-6 / ↓ TNF / ↓ IL-8
IMMUNOSENESCENCE
Thymosuppressive Thymostimulatorycytokines cytokines
steroids LIF IL-7IL-6 KGFOncostatin M TSLP
hGHLeptinIL-10
ThymusRobustThymusAtrophied
thymus
IL-1, IL-3, TGF-β
DNA-anti-apoptotic Bcl-2
SISTEMA INMUNE Y ENVEJECIMIENTO
NATURAL KILLER:
• Posible aumento total de células NK (CD16/CD56)
• Capacidad lítica antitumoral conservada
• Actividad tras IL-2/IFN poco alterada
• Comportamiento pronóstico en ancianos con cancer ?
CÉLULAS LAK:
• Disminución de la actividad con la edad
• Disminución respuesta tras IL-2/IL-12/IFN

ENVEJECIMIENTO Y AUTOINMUNIDADAUTOANTICUERPOS EN LA SENESCENCIA
Relativamente frecuentes en > 65 años
Autoanticuerpo PrevalenciaANAs 14% (8-30%)
FR 22% (10-30%)
aPL 28% (0-40%)
PCA 9% (1-13%)
SMA 8% (1-13%)
AMA 5% (0-10%)
ANCA 1% (0-2%)
Lázaro M, et al. Rev Ciln Esp 2003;203:417-422
INMUNOLOGIA Y ENVEJECIMIENTO
AUTOANTICUERPOS EN FUNCIÓN DEL GÉNERO
Autoanticuerpo Hombre Mujer p
Antitiroglobulina 2 7 0.15
Antimicrosomales 3 12 0.05
Anticardiolipina G 3 3 0.5
Anticardiolipina M 3 3
Anti-DNAn 11 10 0.70
Anti-histona 11 10 0.90Lázaro M, et al. Rev Ciln Esp 2003;203:417-422
INMUNOLOGIA Y ENVEJECIMIENTO
Las alteraciones cuantitativas y/o cualitativas del sistema inmunitario predisponen a:
• Aumento de la patología infecciosa
• Aumento de la prevalencia de neoplasias
• Aumento de la frecuencia de aparición de autoanticuerpos y de enfermedades autoinmunes
•↑DETERIORO ORGANICO ↑ENVEJECIMIENTO
ENVEJECIMIENTO Y AUTOINMUNIDADANTICUERPOS ANTINUCLEARES EN LA VEJEZ:
Frecuentes (8-30%)
En general < 1:160
Patrones: homogeneo, moteado, nuclealar
Titulo y patrón cambiantes
Especificidad: anticromatina nuclear
Complejo ANA-nucleocromatina: favorecen autoinmunidad
ANAs anti-nucleosomas: sistema de protección tumoral?
Incrementan envejecimiento ??Ramos M. Lupus 2003;12:341-355
ENVEJECIMIENTO Y AUTOINMUNIDADANAs / Cancer / Autoinmunidad
Naschiztz et al: ANA + 30% de ancianos con cáncer inmunopatía
Tumor apoptosis nucleosomas ANAs
ANAs con especificidad solo antinucleosomas (tumor)
ANAs con especificidad antinucleosomas (tumor)/antiDNAss/antiDNA-histonas
ANAs citotóxicos frente a nucleocromatina tumoral
INMUNOVIGILANCIA ANTITUMORAL ?
MARCADOR DE RIESGO DE AUTOINMUNIDAD ENVEJECIMIENTO
ENVEJECIMIENTO Y AUTOINMUNIDADFACTOR REUMATOIDE
Frecuente: 10-40%
Correlación entre FR y ↑ gammaglobulinas
FR-IgM “primera linea” de actividad anti-infecciosa?
Mecanismos involucrados en la + de FR:
actividad policlonal de LB
mimetismo antigénico
disfunción LT
disfunción red idiotípica
Ramos M. Lupus 2003;12:341-355

ENVEJECIMIENTO Y AUTOINMUNIDADANTICUERPOS ANTIFOSFOLIPIDO
Presentes hasta en un 40% de personas ancianas
Hasta en un 20% de casos coexisten con ANAs+
Significado?
Factor de riesgo trombótico (SAF)
Factor de riesgo de demencia multiinfartica?
Marcador paraneoplásico? (antiB2-GP1-IgM)
Reactividad cruzada ox-LDL/oxLpa/B2GP1...
Factor favorecedor de envejecimiento ?Ramos M. Lupus 2003;12:341-355
Mosek et al, Fields et al,. Alijotas et al......
ENVEJECIMIENTO Y AUTOINMUNIDADOTROS AUTOANTICUERPOS “ESPECIFICOS:
Anti-DNAn: LES
Anti-Sm: LES
Anti-histonas: LES inducido por fármacos
Anti-Ro: Síndrome de Sontheimer (LCSA)
Anti-Ro /Anti-La: Sde. de Sjögren
Anti-SCl70: Esclerosis sistémica
Anti-centromero: Síndrome CREST
Anti PM-SCl/AantiPM-1: PM/Dernmatomiositis
ANCA: vasculitis necrotizantes sistémicas
Antigliadina, anti-LKM, anti.......

ENVEJECIMIENTO Y AUTOINMUNIDAD
VALOR CLINICO DE LOS AUTOANTICUERPOS
Autoanticuerpos aislados SIN clínica compatible
DISFUNCION AUTOINMUNE
Autoanticuerpos CON clínica compatible
ENFERMEDAD AUTOINMUNE
ENVEJECIMIENTO Y AUTOINMUNIDAD
Enfermedades autoinmunes sistémicas más prevalentes:
•Artritis reumatoide
•Síndrome de Sjögren
•Arteritis de células gigantes
•Polimialgia reumática
•Lupus eritematoso sistémico
•Síndrome de Hughes (SAF)
•Miopatía inflamatoria idiopática
•Vasculitis
•Esclerosis sistémica (Esclerodermia)

AUTOINMUNIDAD Y ENVEJECIMIENTO
ESTADO GENERAL DE SALUD DEL SUJETO:
1. Enfermedades crónicas
2. Nutrición
3. Cancer
4. Autoinmunidad
5. Fármacos

AUTOINMUNIDAD Y ENVEJECIMIENTO



INFLAMMAGEING THEORY
Coined by Claudio Franceschi * in 2000
Ageing is accompained by a low-grade, systemic up-regulationof the inflammatory response.
Chronic low-grade inflammatory status
Senescence age-associated diseases
Franceschi et al, Ann NY Acad Sci, 2000
INFLAMMAGEING THEORY
This inflammatory state is characterised by:
1. Low grade
2. Controlled
3. Asymptomatic
4. Chronic
5. systemic

INFLAMMAGEING THEORY
Internal and environmental inflammatory stimuli
individual background
Pro-inflammatory cytokines
cytokine polymorphisms
Reactive Oxigen Species (ROS) oxidative damage
Autoantibodies
pro-inflamm cytokines
INFLAMMAGEING THEORY
Clasical autoimmune diseases adaptive immunity
New “innate” autoimmune syndrome innate immunity
“Inflammaging may constitute the subclinical paradigm of new type of autoimmunity, namely that arising from anauto-immune inflammatory response of the innate immune-syndrome an old actor of immunity and yet a new actor of autoimmunity”*
*Giunta S. Immunity&Ageing 2006

INFLAMMAGEING THEORYChronic low-grade inflammation
Pro-inflammatory cytokines Frailty
Atherosclerosis
Parkinson disease
Alzheimer disease
Osteoarthritis
Osteoporosis
Insulin resistence / diabetes mellitus
Sarcopenia
AUTOINMUNIDAD Y ENVEJECIMIENTO
AUTOINMUNIDAD
NECROSIS
APOPTOSIS
ENVEJECIMIENTO Y NEURODEGENERACION

Inflammation, autoimmunity and ageingAPOPTOSIS, mediated by two major pathways:
Extrinsic Intrinsic
death receptor-mediated (TNFRs) mitchondria mediated
(CD95)
trimerization of DD poor studied in elderly
pro-caspases
caspases

Inflammation, autoimmunity and ageing
APOPTOSIS IN AGING
Increased apoptosis in T cells, CD4+ and CD8+
↑ sensitivity CD95-CD95L ↑ activation caspase-8 /3
↑ FADD
↑sensitivity to TNF-œ -induced apoptosis
(to analise the proposed mechanism, see figure 3)

Inflammation, autoimmunity and ageingRole of apoptotic cells in the regulation of inflammation
and changes in aging (I)
Apoptotic cell death and clearance of dead cells is essential to homeosta
Clearance of apoptotic cells have and anti-inflammatory effects
Ie: co-cocultures between apoptotic cells and APCs
Apoptosis regulates the cytokine profile
Slow apoptotic cell clearence undergo secondary necrosis
Dendritic cells (APCs) are basic in large scale phagocytosis apoptotic cells

Inflammation, autoimmunity and ageingRole of apoptotic cells in the regulation of inflammation
and changes in aging (II)
Apoptotic cell death and clearance of dead cells is decresed in elderly
Phagocytosis of apoptotic T-cells by dendritic cells is decreased
TNF and IL-6 of apoptotic cells is increased (old/young)
Co-cultures failed to inhibid the production of pro-inflammatory cytokines
Accumulation of apoptotic cells, inducing secondary necrosis and inflammation
DCs may uptake self-Ag derived of apoptotic cells or 2 necrosis to induce
Autoimmunity.
Failure in apoptotic regulation: INFLAMMATION AND AUTOIMMUNITY
AUTOINMUNIDAD Y ENVEJECIMIENTO
Alteracion del ADN alt. proteina membrana Ag
APOPTOSIS AUTOINMUNIDAD
ENVEJECIMIENTO
AUTOINMUNIDAD Y ENVEJECIMIENTO
Brain Reactive-Ag (BRA) ↑ with aging
Ag-Ab complexes
Autoimmunity
ALZHEIMER’S DISEASE
Lai et al. Neurobiol Aging 1988;9:733-42
AUTOINMUNIDAD Y ENVEJECIMIENTO
Prolactina / HGF modificación sist. Inmune
En ancianos, ↑ prolactina o HGF o GH-insulin-GF
↓Tolerancia inmunológica
AUTOAGRESIONVolkenien B, et al. 1998;54:1102-8

Inflamación y Envejcimiento:La arteriosclerosis como modelo
AUTOINMUNIDAD, LIPOPROTEINAS ARTERIOSCLEROSIS Y ENVEJECIMIENTO
Anticuerpos anti-colesterol-liposomas
Anticuerpos anti Ox-LDL
Ox-LDL pequeñas muy inmunógenos
Reactividad entre Ox-LDL y Ac-antifosfolipido
Se detectan en plasma y en placa de ateroma
Isotipo IgG e IgM
Se puede asociar a CD4+ (en placa de ateroma)
Casi nunca en personas jovenes (4%)
Siempre en ancianos (100%)Szondi etal, 1985, Parum et al, 1990
Critical Rev Immunol, 1991

AUTOINMUNIDAD, LIPOPROTEINAS, ATEROMATOSIS Y ENVEJECIMIENTO
•LDL poca afinidad por macrófago no células espumosas
•OxLDL gran afinidad por macrófagos si células espumosas
•OxLDL/aPL: reactividad cruzada (crossroad autoimmunity and atherosclerosis sdme)
•A nivel subendotelial LDL pueden oxidarse, glicarse o agregarse
•OxLDL actuan como “neoantígenos”
•Estas Ox-LDL antigénicas pueden ser inmunogénicas (OxLDL-ApoB
•Lesión endotelial inflamación placa daño endotelial
•LT reactivos Ag específicos (HLA-DR-II) y LB es placas
AUTOINMUNIDAD, LIPOPROTEINAS ARTERIOSCLEROSIS Y ENVEJECIMIENTO
En general, a mayor edad, mas OxLDL y ac-anti-OxLDL
Anti-OxLDL + en: diabetes, HTA, EC, SAF, LES.....
Relación entre oxidació y Anti-OxLDL
Detección de IC OxLDL/anti-OxLDL
A > cantidad de IC, menores niveles de anti-OxLDL
Controversia: título de anti-OxLDL factor de riesgo?
No siempre (IC: OxLDL/anti-OxLDL)

AUTOINMUNIDAD Y ENVEJECIMIENTO
Ac-anti OxLDL mas frecuentes en :
HTA, DM
Coronariopatía
Lupus Eritematoso
Sde. Antifosfolípido
Lesión endotelial
Arteriosclerosis
ENVEJECIMIENTO PRECOZ/ACELERADO
AUTOINMUNIDAD, LIPOPROTEINAS ARTERIOSCLEROSIS Y ENVEJECIMIENTO
LDL Ox-LDL MDA MDA+ApoB Inmunógeno
Ac-antiOx-LDL macrófao
CD4 /CD8
Ox-LDL/antiOx-LDL INFLAMACION Radicales libres
AUTOINMUNIDAD
Ateroesclerosis Isquémia Lesión
ENVEJECIMIENTO

AUTOINMUNIDAD, LIPOPROTEINAS ARTERIOSCLEROSIS Y ENVEJECIMIENTO
LDL Ox-LDL MDA MDA+ApoB Inmunógeno
Ac-antiOx-LDL macrófao APC/LT/LB
Ox-LDL/antiOx-LDL INFLAMACION Radicales libres
AUTOINMUNIDAD
Ateroesclerosis Isquémia Lesión
Alijotas J, 2004 ENVEJECIMIENTO
LDL OxLDL Macrófagp-OxLDL (neoantígeno)
IL-1/IFN APC-OxLDL
LT-CD4+ LB
IL-2/IL-4,5,10, ac-antiOxLDL aPL
↑VCAM/ICAM activación complemento
daño endotelial daño endotelial
ateromatosis / trombosis ↑ placa ateroma G-INF/ILs
MCSF
↑ ENVEJECIMIENTO trombosis

AUTOINMUNIDAD, LIPOPROTEINAS ARTERIOSCLEROSIS Y ENVEJECIMIENTO
AUTOINMUNIDAD, LIPOPROTEINAS ARTERIOSCLEROSIS Y ENVEJECIMIENTO

En ocasiones, ↑ ac-anti Ox-LDL ↑ ENVEJECIMIENTO
Otras veces, ↓ ac-anti Ox-LDL ↑ ENVEJECIMIENTO
Ac-anti-OxLDL en relación con el estrés oxidativo:
•Ox-LDL aldehidos, ac. grasos oxidados
MDA, cardiolipina
reacción cruzada con epitopes de membranas de
células apoptósicas
↑ ENVEJECIMIENTO
AUTOINMUNIDAD, LIPOPROTEINAS ARTERIOSCLEROSIS Y ENVEJECIMIENTO
AUTOINMUNIDAD, LIPOPROTEINAS, ATEROMATOSIS Y NVEJECIMIENTO
Lp(a)
Lp(a)Ox
Lp(a)Ox / APC CD4+
Neoantígenos Th1-IL2/6/IFN
aPL(antiB2-GP-1) Ac.-antiLp(a)Ox Th2-IL4/5/10
Lesión endotelial
Ateromatosis / Trombosis
ENVEJECIMIENTO

AUTOINMUNIDAD, LIPOPROTEINAS, ATEROMATOSIS, ENVEJECIMIENTO
• Proteina C reactiva (PCR)-Ox-LDL y PCR-céls apoptóticas placa
• PCR-fosfocolina externalizada-Ox-LDL
• PCR es mas que un marcador de riesgo de inflamación arterial
• Si LDL y Ox-LDL bajos PCR tiene efecto protector ?
• Si LDL y/o Ox-LDL elevadas PCR efector y marcador de riesgo
• Relación entre PCR y anticuerpo T15 ?? Reactivodad cruzada ?Mi-Kyung CH, et al. Proceedings Nat Acad Sci 2002
Lipoproteinas, inmunidad, ateromatosis, envejecimiento
Relación entre fosfocolina –epitope- de:
Ox-LDL / pared bacteriana / céls apoptóticas ?
Reacción inmnune cruzada
Lesión / necrosis

AUTOINMUNIDAD Y ENVEJECIMIENTO
TIROIDES: ↑ autoanticuerpos antitiroideos con la edad
• No aumento de enfermedad clínica, exceptuando hipot.
• Si aumentan las formas subclínicas
• Alteraciones varias ligadas al hipotiroidismo subclínico:
↑lipoproteinas arteriosclerosis E. Coronaria
ENVEJECIMIENTO PRECOZ / ACELERADO
Mariotti S. Exp Gerontol 1998;33:535-541
Ramos M. Lupus 2003:12:341-355
AUTOINMUNIDAD Y ENVEJECIMIENTOAlgunas situaciones clínicas pueden inducir alteraciones del endotelio con posterior trombosis o microtrombosis.
Algunas situaciones clínicas pueden producir directamente trombosis.
Ambas situaciones puede ser congénitas o adquiridas
Algunas son autoinmunes o provocan respuesta autoreactiva
Las alteraciones trombóticas pueden acelerar el envejecimiento
por ellas mismas o, por provocar “segundas” alteraciones
ALTERACION BASE TROMBOSIS
ENVEJECIMIENTO
AUTOINMUNIDAD Y ENVEJECIMIENTO• VASCULITIS• DESHIDRATACION• HORMONAS• OBESIDAD • DIABETES• CANCER• S. ANTIFOSFOLIPIDO• S. MIELODISPLASICOS• ↑ FACTOR VII / I• ↓ PROSTACICLINA
• DEF. DE PROTEINA C• RESISTENCIA PCactivada• DEF. DE PROTEINA S• DEF. DE AT III o AT II• DISPLASMINOGENEMA• DISFIBRINOGENEMIAS• MUTACION FACTOR II• AL. SIST. FIBRINOLITICO• HOMOCISTEINEMIA• ↑GLUCOPROTEINA-HISTIDINA
En negro: enfermedades autoinmunes “primarias”
En rojo: alteraciones inducidas por las autoinmunes “primarias”
AUTOINMUNIDAD Y ENVEJECIMIENTO
SINDROME ANTIFOSFOLIPIDO I:
Los anticuerpos antifosfolípido son inmunoglobulinas de isotipo IgG/IgM/IgA dirigídas contra fosfolípidos de carga negativa de las membranas
Se detectan mediante la denominada serología luética falsamnete positiva, el anticoagulante lúpico, los anticuerpos anticardiolipina y los anticuerpos anticofactor (antiβ2-glicoproteina-1, antiprotrombina).
Lejos de provocar hemorragias, provocan trombosis en cualquier parte de la economía.

AUTOINMUNIDAD Y ENVEJECIMIENTO
SINDROME ANTIFOSFOLIPIDO II:
Mecanismos de acción:
↓producción de prostaciclina
↓fibrinolisis
↓niveles proteina C y trombomodulina
Incremento de la agregación plaquetar
↓niveles de proteina S
↓niveles de antitrombina III
Reactividad con Ox-LDL/Ox-Lpa
Ateromatosis
Trombosis
Envejecimiento
Exitus
AUTOINMUNIDAD, LIPOPROTEINAS, ATEROMATOSIS Y ENVEJECIMIENTO
•Endotelio tiene receptores para OxLDL
•Beta2-GP-1: inhibe captación endotelial y macrofágica de OxLDL
•Ac-antiBeta2-GP-1 ↑captación OxLDL Céls. espumosasN
Ateroma /Senectud
Neoantígenos
OxLDL/anti-OxLDL aPL(antiB2-GP-1)
LT-CD4+ I. Humoral (LB)
Endotelio (VCAM-1/ICAM) lesión endotelio
↑ Ateroma TROMBOSIS

AUTOINMUNIDAD Y ENVEJECIMIENTO: METILACION-DNA
Metilación DNA básica para mantener función celular (LT)
Metilación disminuye con la edad (entre otros factores)
↓ Metiltransferasas ↓ metilación ↓ metilcitosina
Hipometilación DNA induce autoreactividad y autoinmunidad
Hipometilación induce sobreexpresión de LAF-1 (CD11a/CD18)
LFA-1 (lymphocyte function associated antigen-1) induce autoinmunidad
Richardson BC. J Nutr 2002;132(suppl 8):2401S-2405S
AUTOINMUNIDAD Y ENVEJECIMIENTO: METILACION DNA
Senescencia ↓ DNA-metiltransferasa (1, 3a, 3b)
↓ metilación DNA ↑ LFA-1*
↑proto-oncogenes ↑Autoinmunidad
↑transloc. Cromosómicas ↑ Lesión / Apoptósis
↓Imprinting
↑CARCINOGENESIS ↑ ENVEJECIMIENTO*lymphocyte fucntion associated antigen-1

Heat shock proteins: HSP 60/65
Proteinas mitocondriales inducibles por estrés
físico: calor
infección
citocinas: alfa-INF
radicales libres
Normalidad: HSP 60 proteina intracelular (Ag no expuesto)
Epitopes de HSP presentes en membranas lesionadas
HSP 60/65 50% homología con HSP bacteriano
clamidias
micobacterias
H. Pylori
CMV
AUTOINMUNIDAD, ATEROMATOSIS Y ENVEJECIMIENTO
AUTOINMUNIDAD Y ENVEJECIMIENTO
Heat shock proteins (HSP 60) HSP 60 endotelio dañado
Heat shock proteins (HSP 60) (Ag mod) oxLDL antioxLDL
AGRESION AUTOINMUNE ATEROMATOSIS

Célula
estrés bacteria
reactividad cruzada
inmunorespuesta
CD4/CD8 LB
citocinas complemento
lesión LDL/OxLDL lesión endotelio
“upregulation HSP”
ENVEJECIMIENTO anti-HSP 65-ab ENVEJECIMIENTO
Célula
estrés bacteria
reactividad cruzada PCR-fosfocolina
inmunorespuesta
CD4/CD8 LB
citocinas complemento
lesión LDL/OxLDL lesión endotelio
“upregulation HSP”
ENVEJECIMIENTO anti-HSP 65-ab ENVEJECIMIENTO

AUTOINMUNIDAD Y ENVEJECIMIENTO
FENOTIPO DE RIESGO INMUNE PARA ENVEJECER?
ESTUDIOS HLA (ALELOS Y HAPLOTIPOS)
NO FENOTIPO DE RIESGO
Naumova E. Exp Gerontol 2004;39:637-44
AUTOINMUNIDAD Y ENVEJECIMIENTODISFUNCION LINTOCITOS T
↓número y funcionalidad LT-CD8+
ALTERACION PERFIL CITOCINAS: IL-10/IL-6/IFN
Genotipos 1082G/A, 819C/C y 592C/C ↑ producciónIL-10 se asocian a ↑ longevidad
Genotipos 1082A/A, 819C/T y 592C/A ↓ producciónIL-10 se asocian a ↓ longevidad
Naumova E. Exp Gerontol 2004;39:637-44

AUTOINMUNIDAD, LIPOPROTEINAS, ATEROMATOSIS Y ENVEJECIMIENTO
Ac-antiBeta2-GP-1 ↑captación OxLDL Céls Espumosas-APCN
aPL/LDL/Lpa ↑captación OxLpa
Endotelio Ateroma
Neoantígenos autoinmunidad
Estrés/oxidación ateromatosis
OxLDL/anti-OxLDL aPL(antiB2-GP-1)
HSP 60/65 OxLpa/anti-OxLpa HLA-DR-II
LT-CD4+ IL-Th1 I. Humoral (LB)
C1-C9
Endotelio (VCAM-1/ICAM) lesión endotelio
↑ Ateroma TROMBOSIS
Deterioro celular/tisular/sistema/organismo VEJEZAlijotas J, 2004
AUTOINMUNIDAD, LIPOPROTEINAS, ATEROMATOSIS Y ENVEJECIMIENTO
Ac-antiBeta2-GP-1 ↑captación OxLDL Céls Espumosas-APC
aPL/LDL/Lpa ↑captación OxLpa IL1 CD4/CD8/CD19
Endotelio Ateroma
Neoantígenos ANAs
Estrés/oxidación Nucleosomas
OxLDL/anti-OxLDL aPL(antiB2-GP-1)
HSP 60/65 OxLpa/anti-OxLpa
LT-CD4+ IL/GF/IFN CD19 (LB)
Endotelio (VCAM-1/ICAM) lesión endotelio
↑ Ateroma TROMBOSIS
Deterioro celular/tisular/sistema/organismo VEJEZAlijotas J, 2004

AUTOINMUNIDAD Y ENVEJECIMIENTOINMUNOSENESCENCIA
INVOLUCION TIMICA
↓ FUNCIONALISMO CELULAS T
DISFUNCION INMUNE
↑ ESTRÉS OXIDATIVO
APOPTOSIS ENVEJECIMIENTO

PROPUESTAS TERAPEUTICAS ANTI-AGINGTerapia hormonal sustitutiva
Andrógenos
HCG
Melatonina
Actividad física (work-out)
Ozonoterapia
Antioxidantes
Omega-3 / Omega-6
Restricción calórica
Acido acetilsalicílico-estatinas-ezetimibe
Antidopaminérgicos
Inhibidores del CETP: torcetrapib
Inmunomoduladores: AM3, pentoxifilina, estatinas, Mo-abs
Terapia génica
Immunological polymorphismsprofiles and ageing
• ↑ IL-2• ↑ IL-7 +Zn• ↑ IL-4• ↑ IL-10• ↓ TNF• ↑ CD45RA+ y ↓ CD45RO+• ↓ IL-6• ↓ IFN-gamma• ↑nTreg (CD4+,CD25, Foxp3+)
↓ Th1 / ↑ Th2 / ↑ nTreg







