Interim Analysis of SARC022, A Phase II study of Linsitinib in Pediatric and Adult Wild Type (WT) Gastrointestinal
Stromal Tumors (GIST)M von Mehren, M Heinrich, S Schuetze,
K Ganjoo, J Yu, J Yap, AD Van den Abbeele,
J Wright, S George

Background
WT GIST in adults and children are less responsive to tyrosine kinase inhibitors compared to GIST tumors with KIT/PDGFRA mutations
Insulin-like growth factor-1 receptor (IGF-1R), a member
of the insulin receptor family (IR), has been demonstrated to be highly expressed on WT GIST
We hypothesized that growth and proliferation in these tumors may be IGF-1R-dependent, and therefore, linsitinib, a dual inhibitor of IGF-1R and IR, might demonstrate clinical benefit in this patient population

Study Schema
N=40
Linsitinib(150 mg PO BID on days 1-28, courses
repeat every 28 days in the absence of
disease progression or unacceptable
toxicity)
Pediatric WT Eligibility Criteria:• Diagnosis ≤18 years of age or
diagnosis of Carney Triad or Carney-Stratakis Dyad
• Progressed on or intolerant to at least sunitinib
Adult WT Eligibility Criteria:• Diagnosis >18 years of age and no
diagnosis of Carney Triad or Carney-Stratakis Dyad
• Progressed on or intolerant to at least imatinib Primary end point: ORR
Secondary end points: SD ≥9 months, PFS, OS, time to progression, metablic responses
http://clinicaltrials.gov/ct2/show/NCT01560260

Patient Demographics, n=20Gender Female Male
12 8
Age 18-62, average 41
Pediatric type Carney Triad
62
Performance Status 0/1/2 12/7/1
Primary Site Stomach (Gastroesophageal) Small bowel Peritoneum
16 (1)21
Metastatic Sites Liver Peritoneum Lymph Nodes
17114
Prior Therapies Imatinib Sunitinib Sorafenib
1-7, median 319197

Toxicities
Hyperglycemia: One grade 2 episode in a patient on steroids
for Iodine IV contrast allergy prophylaxis No increases in HgbA1c levels
No evidence of drug induced: Hepatotoxicity QTc prolongation
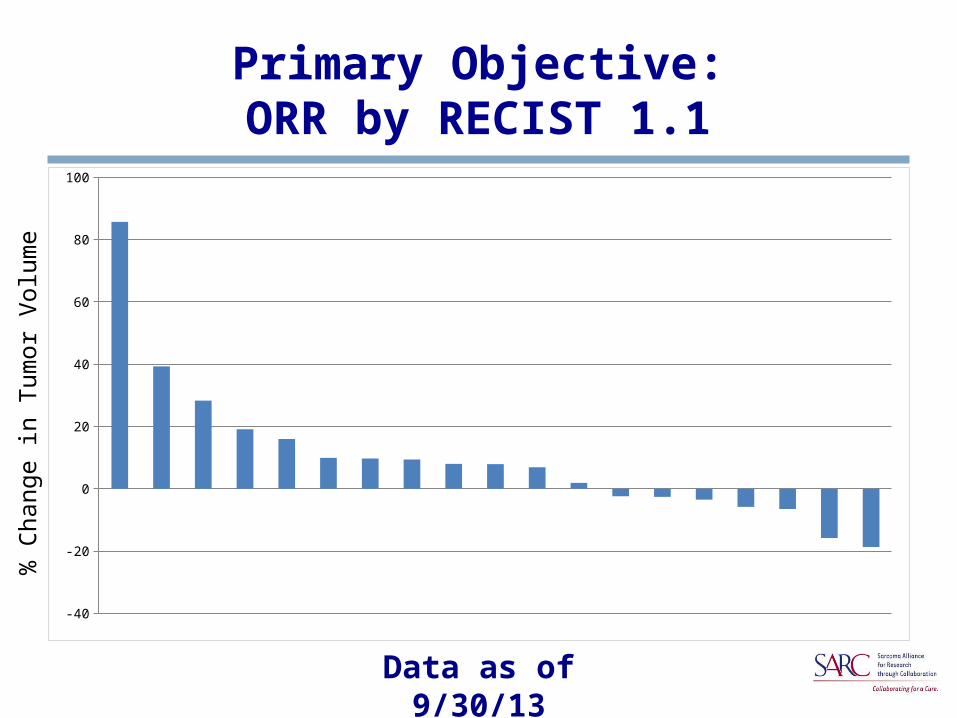
Primary Objective:ORR by RECIST 1.1
Data as of 9/30/13
-40
-20
0
20
40
60
80
100
% C
hang
e in
Tum
or V
olum
e

Metabolic Responder
Baseline
Week-8 Follow-up

Metabolic Progressor
Baseline
Week 8 Follow-up

-100%
-75%
-50%
-25%
0%
25%
50%
EORTC Metabolic Response, N=13
Ranked Patients
Per
cen
t ch
ang
e in
su
mm
ed S
UV
max PMR
SMDPMD
**
*Progression due to new lesions

Clinical Benefit Rate (CR, PR and SD > 9 months)
As of last data cut off of 9/30/13: 15% (3/20 patients) have remained on study
for greater than 9 months 55% (11/20 patients) have had stable disease
for at least 6 months, with 10 remaining on study
1 additional patients remains on study for greater than 4 months
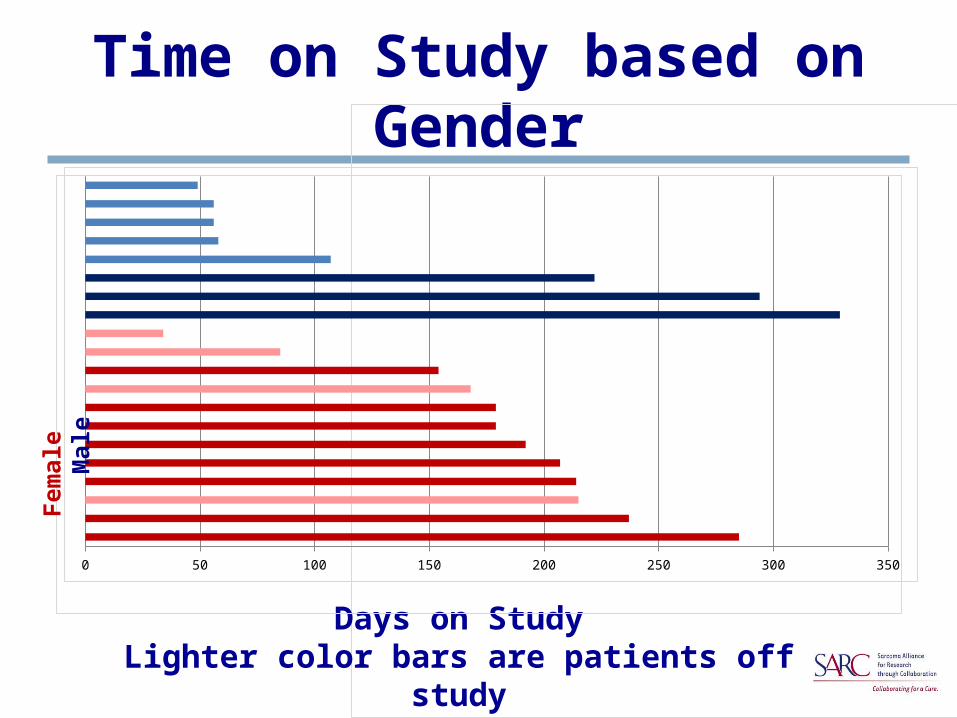
Time on Study based on Gender
Days on StudyLighter color bars are patients off study
0 50 100 150 200 250 300 350
Fem
ale
Mal
e

Time on Study by Primary Site
Time on Study in DaysBlack boxed patients are off study
0 50 100 150 200 250 300 350
GE junc-tion
Stomach
Small Bowel

PFS and OS
Progression-Free Survival, SARC022
0%
20%
40%
60%
80%
100%
0 2 4 6 8 10 12Months from enrollment
SARC022Events / N
6 / 20
6-MonthEstimate
70% (46, 94)
Overall Survival, SARC022
0%
20%
40%
60%
80%
100%
0 2 4 6 8 10 12Months from enrollment
SARC022Deaths / N
3 / 20
6-MonthEstimate
85% (69, 100)
6-Month PFS Estimate: 70%Events/N: 6/20
6-Month OS Estimate: 85%Events/N: 3/20

Conclusions
Clinical trials in WT GIST are feasible Linsitinib is well tolerated without any
unanticipated toxicities We have not seen Recist 1.1 ORR to date 55% of patients have had stable disease for six
months or longer Of the patients reviewed, 15% have had EORTC
metabolic response by FDG-PET Additional correlative studies are being
completed
Acknowledgements
The Patients and their families
Correlative Science: Funding:
Martin Belinsky NCI R21 CA150381
Katherine Janeway NCI R01 CA106588
FCCC Molecular Diagnostics SARC
Laboratory
SARC Clinical Trials Office: Ann Johnson, Brenda Steltzriede, Denise Reinke
CRAB.org: John Crowley, Antje Hoering
CTEP: John Wright, MD, PhD







