
PENYAKIT JANTUNG KORONER:
PENCEGAHAN DAN
DETEKSI DINI
Dr. Emanoel Oepangat SpJP, FIHA, FAPSIC
Tangerang, 10 February 2018 – inconjunction with PIT IDI TANGERANG 2018

Penyakit Jantung
Penyakit Jantung Koroner
Penyakit Jantung Rematik
Infeksi
Hipertensi
Katup Jantung
Irama Jantung
Penyakit Jantung Bawaan
Gagal Jantung

10 Penyakit Penyebab Kematianutama di Indonesia
Data KEMENKES 20141. Cerebrovaskular atau pembuluh darah di otak
seperti pada pasien stroke.2. Penyakit jantung iskemik.3. Diabetes Melitus dengan komplikasi.4. Tubercolusis pernapasan.5. Hipertensi atau tekanan darah tinggi dengan
komplikasi.6. Penyakit pernapasan khususnya Penyakit Paru
Obstruktif Kronis (PPOK).7. Penyakit liver atau hati.8. Akibat kecelakaan lalu lintas.9. Pneumonia atau radang paru-paru.10.Diare atau gastro-enteritis yang berasal dari
infeksi

PENYAKIT
JANTUNG
KORONER

Arteri Koroner

DEFINISI :
Athero : Lemak,
Sclerosis : Pengerasan /
Penebalan
Proses aterosklerosis dimulai dari metabolisme lipidabnormal dan terpaparnya dengan berbagai faktorrisiko al; Hipertensi, Diabetes mellitus, terutama biladisertai gangguan genetik
Aterosklerosis

NormalFattystreak
Fibrousplaque
Athero-scleroticplaque
Plaquerupture/fissure &
thrombosis MI
Ischemic
stroke/TIA
Critical leg
ischemia
Cardiovascular
death
Stable angina
Intermittent claudication
Unstable
angina
}ACS
ACS, acute coronary syndrome; TIA, transient ischemic
attack
Atherothrombosis: a Generalized and Progressive Process

ACUTE CORONARY SYNDROMES
No ST elevation ST elevation
Unstableangina
NSTEMI STEMIStableangina
Source (Photos): Davies MJ. Heart. 2000;83:361-366.
CAD = coronary artery disease; NSTEMI = non-ST-segment elevation myocardial infarction;
STEMI = ST-segment elevation myocardial infarction.
Spectrum of CAD/ACS
PENCEGAHAN PENYAKIT
JANTUNG KORONER

Non-Modifiable
Risk Factors
Increasing age
Male Gender
Family Hx
Ethnic Origin
Modifiable
Risk Factors
Smoking
Hypertension
Dyslipidemia
Diabetes Mellitus
Obesity
High Calorie Diet
Physical Activity

SCORE chart: 10-year risk of fatal CVD in populations at high and low CVD risk based on the following risk factors: age, sex, smoking, SBP, and
total cholesterol (TC). Note that the risk of total (fatal + non-fatal) CVD events will be approximately three times higher than the figures given.
Chapter: How to assess risk
From: The ESC Handbook of Preventive Cardiology: Putting Prevention into Practice
Editor(s): Catriona Jennings, Ian Graham and Stephan Gielen
Downloaded from Oxford Medicine Online.Reproduced from The ESC Textbook of Preventive Cardiology, Gielen et al. with permission of Oxford University Press.

Risk Stratification
Identifies risks
Important as IHD risks are SYNERGISTIC
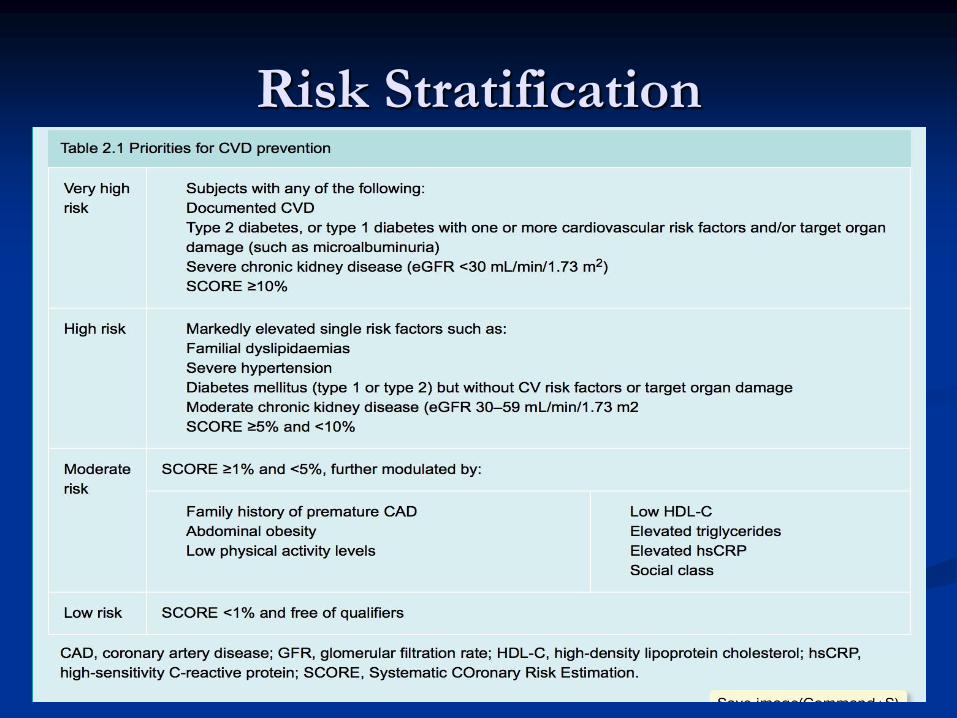
Risk Stratification
Calculates ABSOLUTE risk of CVD event in 10 years
1) Age
2) Sex
3) Cholesterol
4) BP
5) Smoking

Multiple independent
risk factors (silo approach)Integrated identification and management of risk
factors contributing to CVD risk
(global approach)
HT
N
Hyp
erc
ho
lest
ero
lem
ia
Dia
bete
s
Traditional CVD perspective
New CVD risk perspective
Age
GenderDM
Hyper-
cholesterol-
emia
HTN
New targets andgoals for therapy
Reduction of
total CVD risk
is the primary
goal
Smoking
Organ
damage
New Paradigm: Multi-Risk Factor
Approach
CVD: Cardiovascular disease;
DM: Diabetes mellitus; HTN: Hypertension
Volpe M, et al. J Human Hypertens. 2008;22:154–157.

1. Kelebihan berat badan dan Obesitas
Kelebihan berat badan ( BMI > 25/23 kg/m2 ) atau
obesitas ( BMI > 30/27.5 kg/m2 ),
Obesitas sentral : risikolebih tinggi
Mengurangi berat badandengan diet yang benar danmeningkatkan aktivitas fisik
Penurunan berat badan menurunkan tekanan darah, kadarkolesterol, glukosa darah

Obesity, BMI, Waist circumference

Subcutaneous Fat
Abdominal Muscle
Layer
Intra-abdominal
Fat
Visceral Adiposity:
The Critical Adipose Depot

2. Tekanan darah
Target tekanan darah < 140/90
mmHg
Mengubah pola hidup
Olah raga teratur
Diet rendah garam
(<2 g/hari)
Menurunkan BB
Penurunan 2mmHg
TDS, risiko PJK 7%,
Stroke 10%
Terapi obat

ACC Guidelines ESC Guidelines

Figure 13.2 Initiation of lifestyle changes and antihypertensive drug treatment.
Chapter: Managing blood pressure
From: The ESC Handbook of Preventive Cardiology: Putting Prevention into Practice
Editor(s): Catriona Jennings, Ian Graham and Stephan Gielen
Downloaded from Oxford Medicine Online.G. Mancia, R. Fagard, K. Narkiewicz, 2013 ESH/ESC Guidelines for the management of arterial hypertension, European Heart Journal, 2013; 34(28):2159–219 by permission of Oxford University Press.

Partners in Healthcare Education, LLC 2009
Lifestyle Modifications to Manage
HypertensionModification Recommendation Systolic Diastolic Chgs
Weight Reduction BMI 18.5-24.9 5-20mm/10 kg wt loss
Adopt DASH eating Diet rich in fruits 8-14 mm Hg
vegetables and low
fat with reduced
saturated and total fat
Dietary Sodium 2.4g Na 2-8 mm Hg
Physical Inactivity Brisk exercise 30” day 4-9 mm Hg
most days of week
Moderation of
Alcohol intake 2 drinks day max 2-4 mm Hg
24 oz beer; 10 oz wine
2 oz 100 proof whiskey
JAMA. 2003:289:2560-2577.

Target kontrol glukosa darah pada diabetes tipe 2 yakni :
kadar glukosa darah puasa 110 mg/dL,
post prandial 140 mg/dL,
HbA1C < 6.5 % dan menghidari hipoglikemia (ADA)
Pada pasien diabetes tipe II target yang lebih rendah bisa dicapai
dengan aman
Terapi obat profilaksis
Skrining keluarga dekat (Check-Up)
Keluarga dekat pasien dengan PJK prematur
(pria < 45 tahun dan wanita < 55 tahun) harus diskrining
untuk risiko koroner karena tingginya risiko PJK
3. Glukosa darah
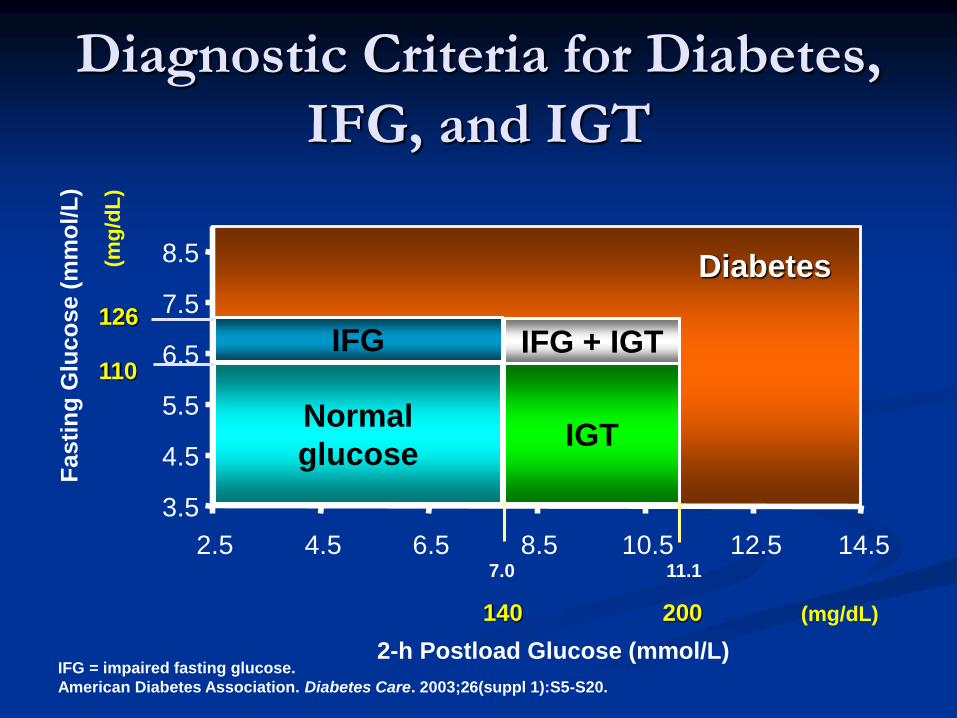
(mg/dL)
Diagnostic Criteria for Diabetes,
IFG, and IGT
3.5
4.5
5.5
6.5
7.5
8.5
2.5 4.5 6.5 8.5 10.5 12.5 14.5
Normal
glucoseIGT
IFG + IGTIFG
2-h Postload Glucose (mmol/L)
Fasti
ng
Glu
co
se (
mm
ol/
L)
(mg
/dL
)
140 200
126
110
Diabetes
IFG = impaired fasting glucose.
American Diabetes Association. Diabetes Care. 2003;26(suppl 1):S5-S20.
7.0 11.1

Figure 15.1 Scottish Intercollegiate Guidelines Network (SIGN) Guideline 116: Management of Diabetes.
Chapter: Managing blood glucose
From: The ESC Handbook of Preventive Cardiology: Putting Prevention into Practice
Editor(s): Catriona Jennings, Ian Graham and Stephan Gielen
Downloaded from Oxford Medicine Online.Scottish Intercollegiate Guidelines Network (SIGN). Management of Diabetes. Edinburgh: SIGN; 2010. (SIGN publication no. 116).
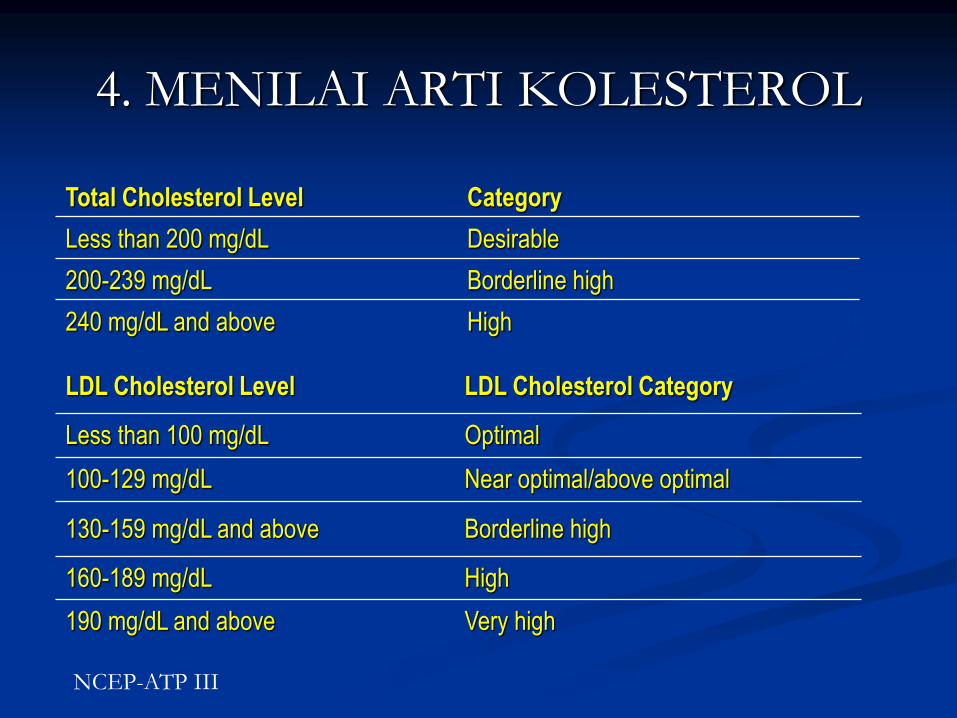
4. MENILAI ARTI KOLESTEROL
Total Cholesterol Level Category
Less than 200 mg/dL Desirable
200-239 mg/dL Borderline high
240 mg/dL and above High
LDL Cholesterol Level LDL Cholesterol Category
Less than 100 mg/dL Optimal
100-129 mg/dL Near optimal/above optimal
130-159 mg/dL and above Borderline high
160-189 mg/dL High
190 mg/dL and above Very high
NCEP-ATP III

HDL 40 mg/dL resiko tinggi PJK
HDL 40 mg/dL resiko rendah PJK
TG 150-199 mg/dL Borderline high
TG 200 mg/dL High
HDL dan Triglyserid
LDL Cholesterol
is
The Primary Target
in Dyslipidemia Treatment
NCEP ATP III 2003/ NCEP ATP III Update 2004
ADA/ACC Guideline Update for Secondary Prevention 2006
ESC/EAS Guidelines for the management of Dyslipidemias 20112013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce
Atherosclerotic Cardiovascular Risk in Adults
ADA Standards of Medical Care in Diabetes 2015

Adapted from Rosensen RS. Exp Opin Emerg Drugs 2004; 9(2): 269-279
LDL-C achieved mg/dL (mmol/L)
WOSCOPS – Placebo
AFCAPS - Placebo
ASCOT - Placebo
AFCAPS - Rx WOSCOPS - Rx
ASCOT - Rx
4S - Rx
HPS - Placebo
LIPID - Rx
4S - Placebo
CARE - Rx
LIPID - Placebo
CARE - Placebo
HPS - Rx
0
5
10
15
20
25
30
40(1.0)
60(1.6)
80(2.1)
100(2.6)
120(3.1)
140(3.6)
160(4.1)
180(4.7)
6
Secondary Prevention
Primary Prevention
Rx - Statin therapyPRA – pravastatinATV - atorvastatin
200(5.2)
PROVE-IT - PRA
PROVE-IT – ATV
TNT – ATV10
TNT – ATV80
On-Treatment LDL-C is Closely Related to
CHD Events in Statin Trials – Lower is Better
CORONA - RxCORONA - Placebo

Recommendation for treatment target LDL-C
(ESC/EAS 2011)
Recommendation Class Level
VERY HIGH CV risk (established CVD, DM type 1
&2 with target organ damage, severe CKD or SCORE
level > 10%) the LDL-C goal is < 70 mg/dl and or
> 50% reduction when target level cannot be
reached
I A
HIGH CV risk (markedly elevated single risk factor, a
SCORE level > 5 to < 10%), an LDL-C goal < 100
mg/dl
II a A
MODERATE risk (SCORE level >1 to< 5), an
LDL-C goal < 115 mg/dl
II a C
European Guidelines on cardiovascular disease prevention in clinical practice (version 2012). Eur Heart J. 2012;33:1635–1701
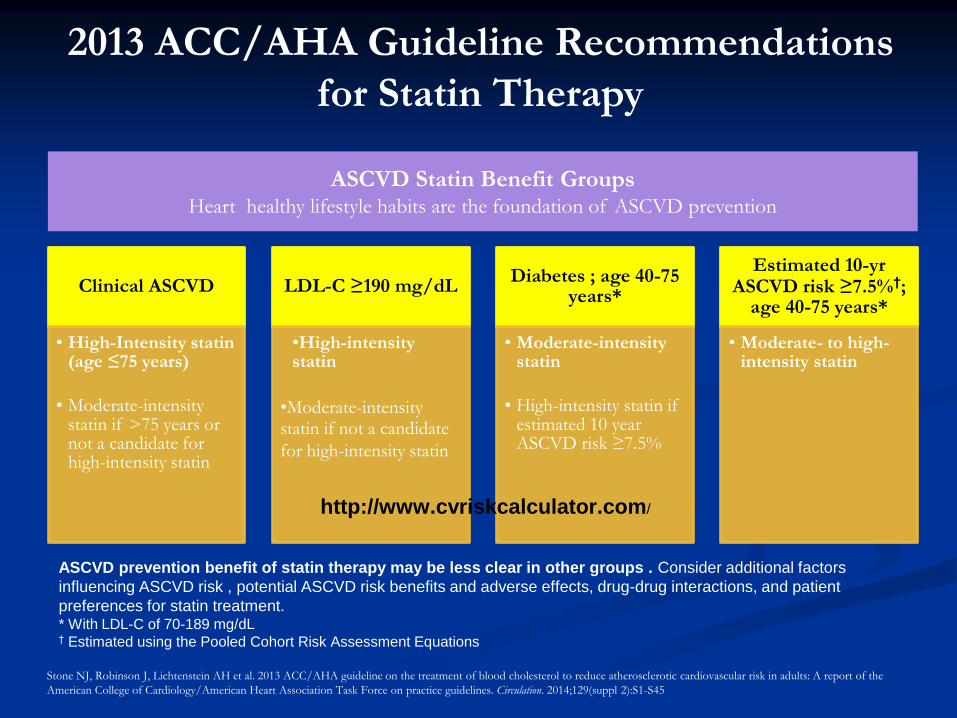
Clinical ASCVD
• High-Intensity statin (age ≤75 years)
• Moderate-intensity statin if >75 years or not a candidate for high-intensity statin
LDL-C ≥190 mg/dL
•High-intensity statin
•Moderate-intensity statin if not a candidate
for high-intensity statin
Diabetes ; age 40-75 years*
• Moderate-intensity statin
• High-intensity statin if estimated 10 year ASCVD risk ≥7.5%
Estimated 10-yr ASCVD risk ≥7.5%†;
age 40-75 years*
• Moderate- to high-intensity statin
ASCVD Statin Benefit GroupsHeart healthy lifestyle habits are the foundation of ASCVD prevention
2013 ACC/AHA Guideline Recommendations
for Statin Therapy
ASCVD prevention benefit of statin therapy may be less clear in other groups . Consider additional factors
influencing ASCVD risk , potential ASCVD risk benefits and adverse effects, drug-drug interactions, and patient
preferences for statin treatment.* With LDL-C of 70-189 mg/dL† Estimated using the Pooled Cohort Risk Assessment Equations
Stone NJ, Robinson J, Lichtenstein AH et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the
American College of Cardiology/American Heart Association Task Force on practice guidelines. Circulation. 2014;129(suppl 2):S1-S45
http://www.cvriskcalculator.com/

High-Intensity Statin
Therapy
Moderate-Intensity Stain
Therapy
Low-Intensity Statin
Therapy
LDL–C ↓ ≥50% LDL–C ↓ 30% to <50% LDL–C ↓ <30%
Atorvastatin (40†)–80 mg
Rosuvastatin 20 (40) mg
Atorvastatin 10 (20) mg Rosuvastatin (5) 10 mg Simvastatin 20–40 mg‡
Pravastatin 40 (80) mg Lovastatin 40 mg
Fluvastatin XL 80 mg
Fluvastatin 40 mg bid
Pitavastatin 2–4 mg
Simvastatin 10 mg
Pravastatin 10–20 mg
Lovastatin 20 mg
Fluvastatin 20–40 mg
Pitavastatin 1 mg
Lifestyle modification remains a critical component of ASCVD risk reduction, both prior to and in concert with the use of cholesterol
lowering drug therapies.
Statins/doses that were not tested in randomized controlled trials (RCTs) reviewed are listed in italics
†Evidence from 1 RCT only: down-titration if unable to tolerate atorvastatin 80 mg in IDEAL
‡Initiation of or titration to simvastatin 80 mg not recommended by the FDA due to the increased risk of myopathy, including rhabdomyolysis.
Intensity of Statin Therapy
Stone NJ, Robinson J, Lichtenstein AH et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the
American College of Cardiology/American Heart Association Task Force on practice guidelines. Circulation. 2014;129(suppl 2):S1-S45


ContinuousRhytmicalIntervalProgressiveEndurance
30 minutes: 3 - 4 times / week
5. EXERCISE
Target nadi: 60-80% nadi max (220-umur)

6. SMOKING KILLS...

Diagnosis dan Tata laksana
Diagnosis :
Anamnesa dan Pemeriksaan Fisik
Elektrokardiogram (EKG)
Uji latih jantung (Treadmill test)
Ekokardiographi (resting and stress)
Szintigrafi Miokard / PET Scan (Kardiologi Nuklir)
CT Scan jantung
Angiografi Koroner (non operatif)

• Angina klasikRasa tidak enak di daerah substernal, sifatnya tumpul, seperti ditekan / diperas, menjalar ke lengan kiri / leher, dapat disertai kesulitan bernapas, berdebar-debar, keringat, mual atau muntah
• Angina EquivalentTidak ada nyeri / rasa tidak enakdi dada yang khas, namun pasien menunjukkangejala gagal jantung mendadak(sesak napas), atau gangguan irama jantung(palpitasi, presinkop, sinkop)
Gejala Penyakit Jantung Koroner

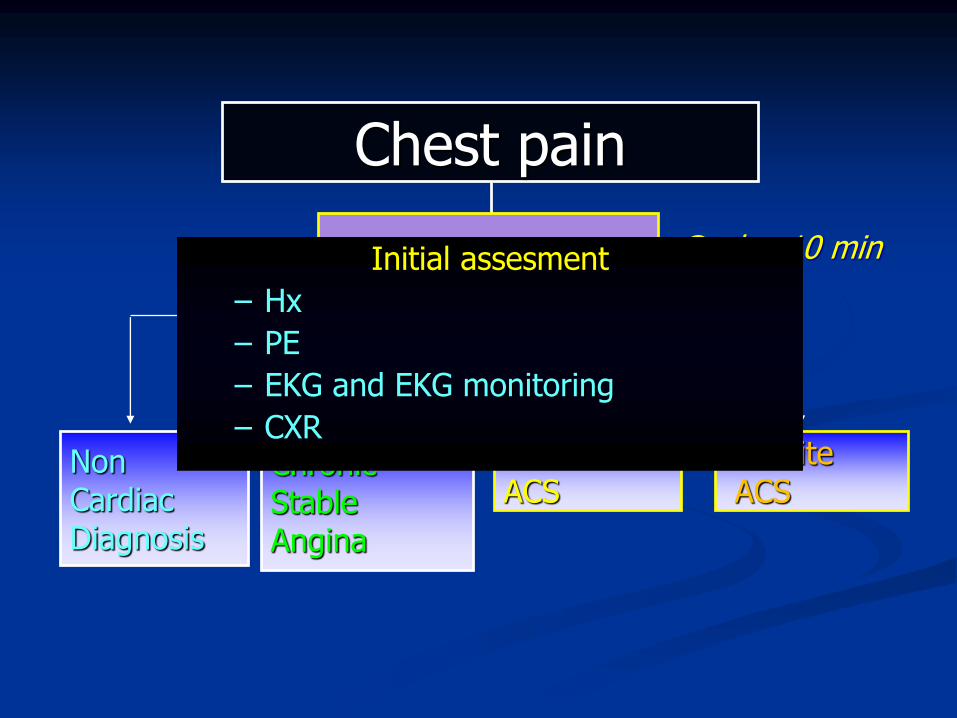
Chest pain
DefiniteACS
Possible ACS
Chronic Stable Angina
Non Cardiac Diagnosis
Assess 12 lead ECG Goal = 10 minInitial assesment
– Hx
– PE
– EKG and EKG monitoring
– CXR

0 h/3 h rule-out algorithm of non-ST-elevation acute coronary syndromes using high-
sensitivity cardiac troponin assays.
Authors/Task Force Members et al. Eur Heart J
2015;eurheartj.ehv320
© The European Society of Cardiology 2015. All rights reserved. For permissions please email:

Acute Coronary Syndromes
Non-ST elevation ACS
ST-elevation MI
Cardiac marker +ve
Cardiac marker +ve
Unstable angina
Cardiac marker - ve

Initial assessment of patients with suspected acute coronary syndromes.
Authors/Task Force Members et al. Eur Heart J
2015;eurheartj.ehv320
© The European Society of Cardiology 2015. All rights reserved. For permissions please email:
ECG Ischaemia
12-Lead ECG *During* acute event
Inducible Ischaemia
1) Exercise ECG
2) Stress ECG/Echo
3) Myocardial Perfusion Scanning
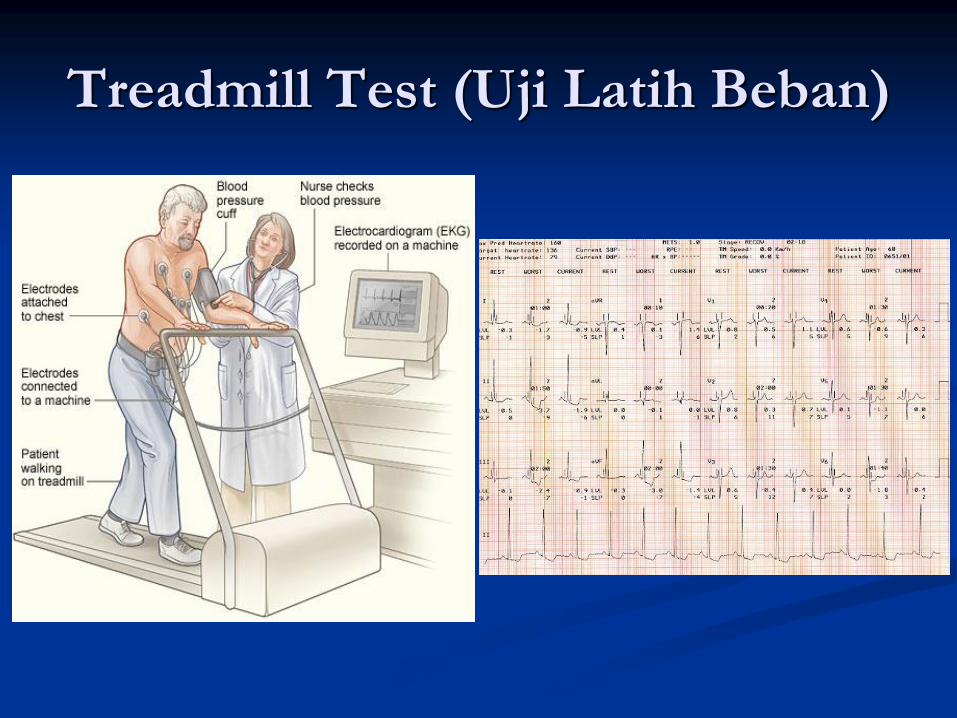
Treadmill Test (Uji Latih Beban)

Echocardiogram
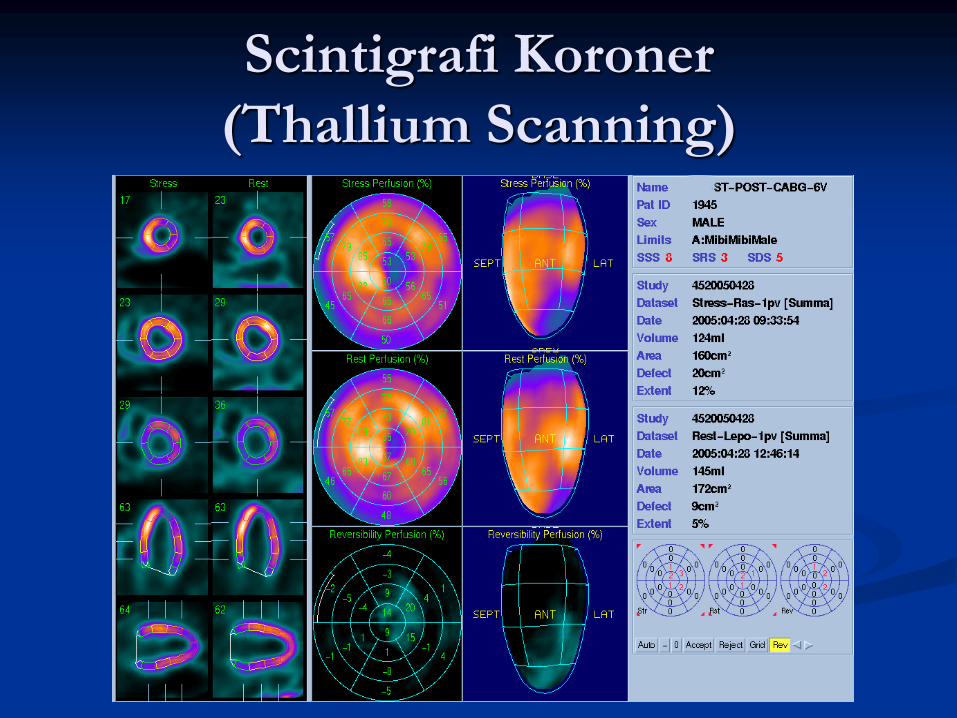
Scintigrafi Koroner
(Thallium Scanning)
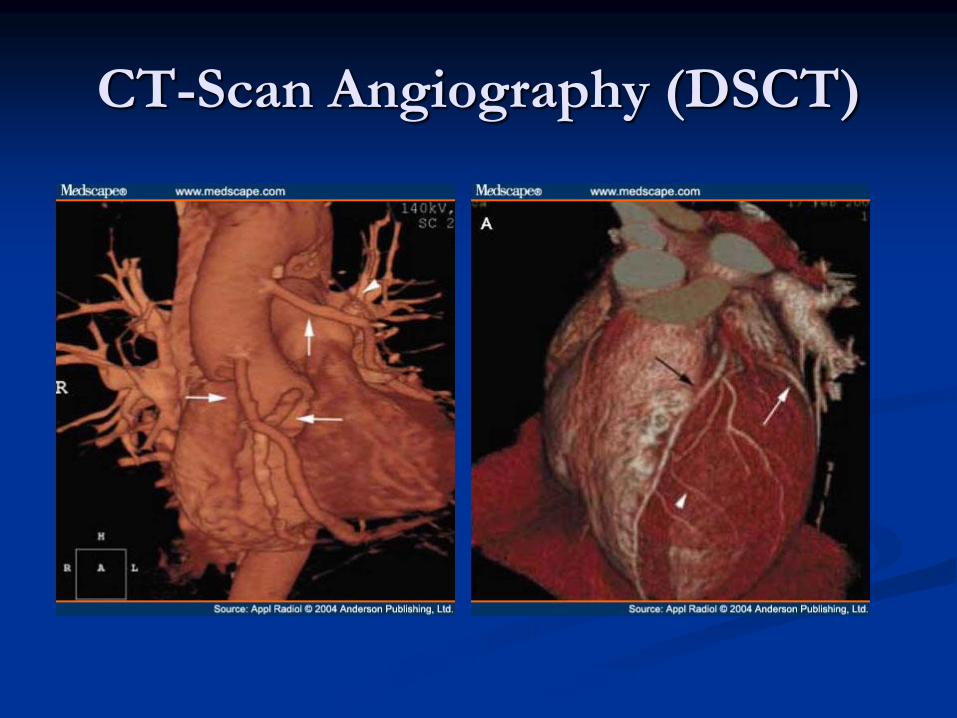
CT-Scan Angiography (DSCT)

Kateterisasi Jantung

Tatalaksana dan Pengobatan

Tata laksana:
Prevensi sekunder dan primer
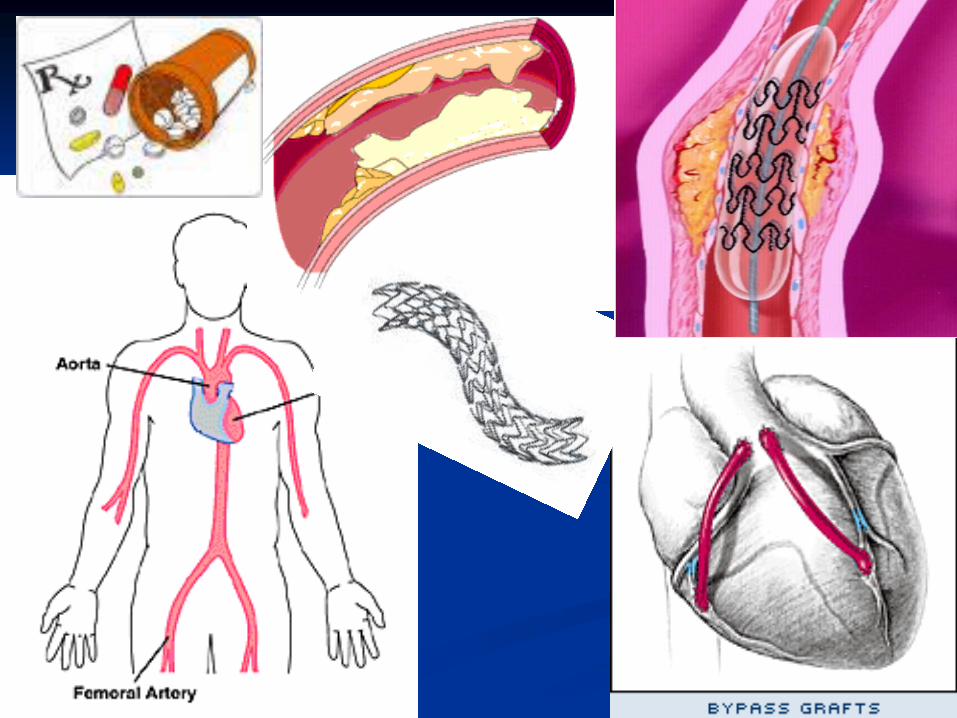
Pengobatan konservatif (obat – obatan)
Pengobatan invasiv (non operatif) denganmetode kateter
Operasi “Bypass” Jantung

Early Hospital Care In ACS


Tatalaksana
PTCA + Stent CABG

Coronary Angiography


Angioplasty dan Stenting
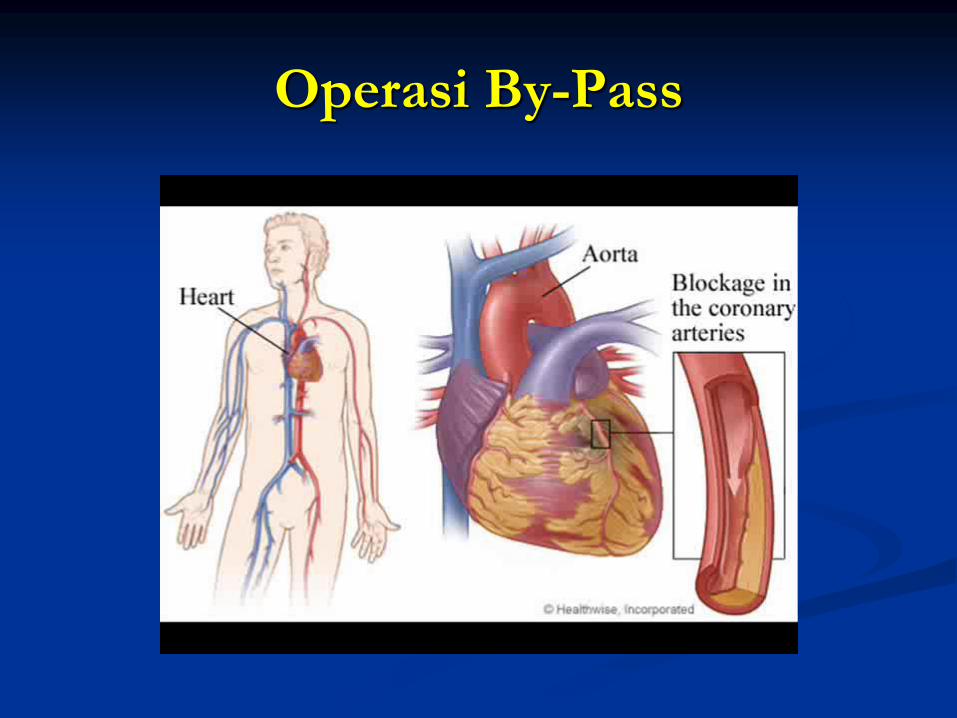
Operasi By-Pass

A- antiplatelets, ACE-I
B- beta-blocker, blood pressure control
C- cholesterol lowering, cigarette
smoking cessation
D- diet, diabetes management
E- exercise
“ A B C D E ”

Terima Kasih







