miss.kamlah - جامعة آل...
TRANSCRIPT

Miss.kamlah 1

Miss.kamlah 2
Anatomy The brain, spinal cord are the major structures of
the nervous system.
The brain is protected by the skull & covered by three lyres of tissue called the meninges- the dura mater, archniod, & pia mater.
Cerebrospinal fluid circulate within the ventricles of the brain & around the brain & spinal cord.
CSF is produced in pia mater, then pass through canals to the lateral ventricle then to the third ventricle then to the forth ventricle then reabsorbed by the archniod layer ( this process takes about 6 hours)

Miss.kamlah 3

Miss.kamlah 4
Pediatric differences
The brain & spinal cord are formed from the neural plate, which evolve into the neural groove & neural folds by the third week of gestation.
The groove closes to form the neural tubes which become the central nervous system.
In infants, the cranial bones & vertebrae are not completely ossified putting the child at risk for injury.
Fontanels are spaces in connective tissue that allow for normal brain growth. (anterior, posterior).

Miss.kamlah 5
By 12 years of age the sutures are completely ossified & can not be separated.
At birth, the nervous system is complete but immature. So growth of brain continues until the child is 12-15 years of age.
Myelination, the progressive covering of myelin of lipid protein sheath, is also incomplete at birth.
As myelination progress, the primitive reflexes disappears. And this process continues throughout childhood.

Miss.kamlah 6
Diagnostic tests used to evaluate Neurological condition
CT scan.
EEG: electroencephalogram.
ICP: intracranial pressure monitoring.
Lumber puncture.
MRI.
X-ray.
Ultrasound.
CSF culture, analysis.
Glascocoma scale.

Miss.kamlah 7
Older child & adult Infant & young children Score Category
SpontaneousSpontaneous opining 4Eye opining
To verbal stimuliTo loud noise 3
To painTo pain2
No response No response 1
Oriented * 3Smiles. Coos, cries 5Verbal response
ConfusedIrritable; cries 4
Inappropriate word Inappropriate crying 3
Incomprehensible word
Grunt; moans2
No response No response 1
Obeys commands Spontaneous movement 6Motor response
Localize painWithdraws to touch 5
Withdraw to painWithdraw to pain4
Flexion to painAbnormal flexion 3
Extension to pain Abnormal extension 2
No response No response 1

Miss.kamlah 8
Assessment Guide lines Clascocoma scale Level of copiousness
Assess function of cranial nerves. Cranial nerves
Assess by palpation Fontanels & statures
Assess use of verbal skills Cognitive function
Equal, round, react to light, accommodation
Pupils
Meanly heart rate, respiratory rate Vital signs
Assess reflexes, fine & motor functionPosture & movements
Assess neck rigidity Neck stiffness
Assess level of pain Pain

Miss.kamlah 9
Miss.kamlah 10
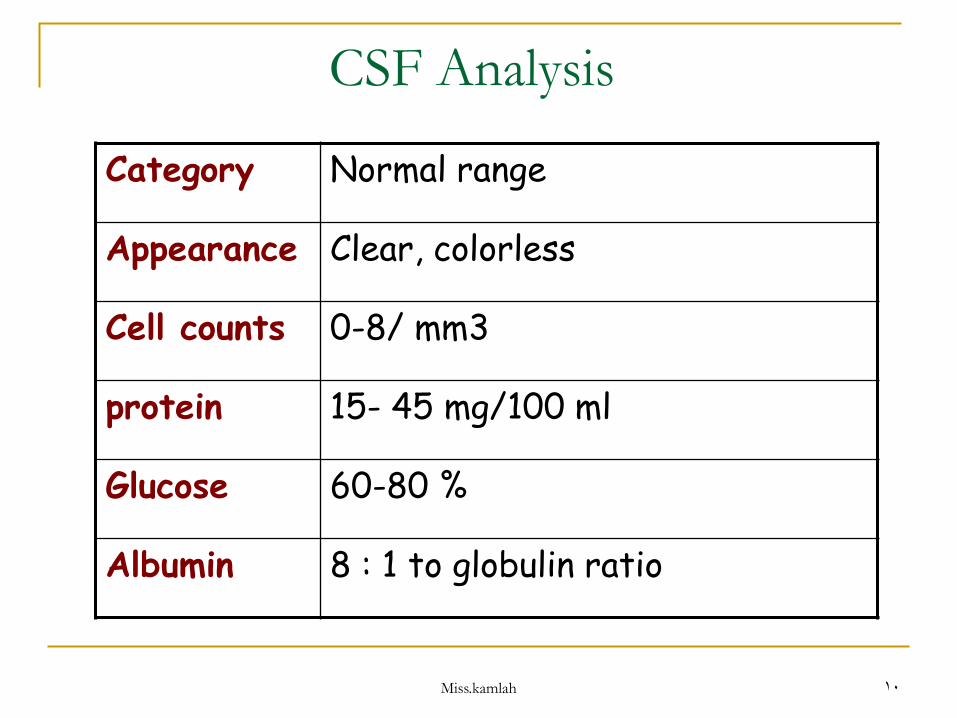
CSF Analysis
Normal range Category
Clear, colorless Appearance
0-8/ mm3 Cell counts
15- 45 mg/100 mlprotein
60-80 % Glucose
8 : 1 to globulin ratio Albumin

Miss.kamlah 11
Signs of increased intracranial pressure
Signs Timing of signs
headache, visual disturbances, nausea & vomiting, dizziness or vertigo
Early signs
Irritability, bulging fontanel, wide stature, increased head circumference
Infant has above signs plus:
Decrease in level of consciousness, bradycardia, irregular respiration, fixed dilated pupils.
Late signs

Miss.kamlah 12
Seizure Disorders Seizures are periods of abnormal electrical
discharges in the brain that causes involuntary movements as well as, behavioral & sensory alteration.
Epilepsy is a chronic disorder characterized by recurrent, unprovoked seizures secondary to CNS disorder.
It has two main types:
1- partial or focal seizure.
2- generalized seizure

Miss.kamlah 13
Etiology & Pathophsiology Chemical changes occur in the neurons will create an
electrical negativity that enable the transfer of information between neurons.
When an excessive number of these cells become excited, they discharge abnormally.
Some seizure are idiopathic & not provoked, while others can be provoked by stimuli such as: emotional stress, anxiety, fatigue, infections, trauma, hypoglycemia, hypotonic dehydration, endocrine dysfunction, electrolyte imbalance, toxins, tumors.
The focal seizures are caused by abnormal electrical activity in one hemisphere, or specific area of the cerebral cortex. That results in localized symptoms related to the region of the cortex affected.
Miss.kamlah 14
In the generalized seizures; they results from a diffuse electrical activity that begin in both hemispheres & spread throughout the cortex into the brainstem. As a result, the movements & spasm displayed by the child are bilateral & symmetric.
The length of the seizure is important, the child may become cyanotic or pale & hypoglycemic due to increase in the metabolic rate.
Febrile seizures are generalized seizures occur in children who have high grade fever (>39c) in association with acute illness. It involves generalized tonic-clonic movements that lasts less than 15 minutes.
Miss.kamlah 15
Clinical manifestations
It depend on the type & duration of seizures.
Seizures has four stages:
1- the Aura: the first stage, in which the child experience an olfactory or visual sensory sensation that may provide an early warning sign of seizure.
2- tonic phase: the contraction phase, where muscle is contracted, the patient is unconscious.
3- clonic phase: the phase that involves periods of contractions & relaxations.
4- the postictal period: it follows the seizure activity, the patient's level of consciousness is decreased. It ranged from 30 min to 2 hours.

Miss.kamlah 16

Miss.kamlah 17
Diagnostic tests:
MRI.
CT scan.
EEG
CBC
Lumbar puncture.
Lead level.
Urine culture.
Past History

Miss.kamlah 18
Clinical therapy
In febrile seizures, no anticonvulsant therapy is administered in both short & long term treatment due to their side effects.
So parent are taught to lower fever by using antipyretic & keeping the child cool with light clothing. As well as protect the child from injury in future seizure.
If the seizure is sever or the child experience a second episode, the parent may be given rectal diazepam or diazepam gel.

Miss.kamlah 19
Continue… Any child with a generalized seizure lasting longer
than 10 minutes needs to be monitored for electrolytes, glucose, blood gases, increasing fever, & abnormal blood pressure.
Anticonvulsant are given rectaly or intravenously to control seizure. Most children respond to monotherapy (use of single drug a time) to minimize the side effects of sleepiness, decreased attention & memory, difficulty of speech, ataxia, & diplopia.
Observe the child for status epilepticus ( which is a contentious seizure that lasts for longer than 30 minutes or s series of seizure during which the consciousness is not regained).
Miss.kamlah 20
Nursing managements
Possible nursing diagnosis:
Ineffective breathing patterns.
Ineffective airway clearness.
Altered tissue perfusion.
Impaired gas exchange.
Risk for trauma.
Anxiety

Miss.kamlah 21
Continue… Maintain airway patency by:
1. Place nothing in the child’s mouth, to not broke teeth that could leads to aspiration.
2. Position the child on the side so secretion will be drain out.
3. Ensure adequate oxygenation.
4. If the child in hospital put on O2 supplement.
Ensure safety by:
1. Protect the child from violent seizures.
2. Elevate side rail if the child on the bed and pad them.
3. The child should not be left alone. E.g. in bathtub.
Miss.kamlah 22
Administer medication:
1. Take especial precautions when administering intravenous medication during emergency management.
2. If medication are given intravenously, it must be given slowly to minimize the risk of respiratory or circulatory collapse.
3. Rectal medication is the safest method to give medication at home, but oral medication can be prescribed for children with mild infrequent seizures.
Provide emotional support.

Miss.kamlah 23
Reye’s Syndrome
Is a disorder that includes hepatic dysfunction & an acute encephalopathy (a cerebral dysfunction caused by a toxic, injury, inflammatory, or anoxic insult that may result in permanent tissue damage).
The condition is associated with the use of aspirin especially in children under the age of five.
The etiology is unknown, an encephalopathy occur after the child had a mild viral infection or when the child has been given aspirin or aspirin containing products.
The syndrome is characterized by cerebral edema, hypoglycemia, & enlarged liver.
Miss.kamlah 24
Symptoms started with nausea & vomiting, mental status changes, seizure , progressive unresponsiveness.
It has five stages in which each stage is characterized by progressive symptoms.
Treatment includes: hospitalization in the ICU, put the child on MV if child in coma, monitor blood gases.
monitoring the child physical status, provide emotional support, teaching the parents about the disease process.

Miss.kamlah 25
Structural defects
Microcephaly: indicates a small brain with a head circumference that is more than 3 standard deviation below the mean for age & sex.
It may be caused by chromosomal abnormality, maternal infections.
Those children have mental retardation.
There is no treatment for microcephaly.

Miss.kamlah 26

Miss.kamlah 27
Hydrocephalus Is the body’s response to imbalance between the
production & absorption of the CSF. It is often congenital but can be acquired.
CSF is produced at constant rate of 0.3 ml per minute. When the balance disturbed, the ventricles become enlarged.
In children with post infection meningitis, intra ventricular hemorrhage, or a congenital malformation in subarachniod space;
the absorption process in the archniod layer become impaired, leading to hydrocephalus.

Miss.kamlah 28

Miss.kamlah 29
Clinical manifestations Diagnostic tests
It vary with the age of the child.
Rapidly increasing head circumference, tense bulging fontanels, hyperreflexia, poor feeding.
Difficulty holding head up, vomiting, apnea, cardiopulmonary depression.
MRI
CT scan
Head circumference

Miss.kamlah 30
Clinical therapy It involves removing the obstruction or creating a new
CSF pathway to divert excess CSF. A catheter or shunt is placed in the ventricle and
passes the CSF to the peritoneal cavity, atrium of the heart, or the pleural spaces.
Shunt system is consist of 4 parts: a ventricular catheter, a pumping chamber or reservoir, a one-way pressure valve & a distal catheter.
Mechanical complication may include blockage of the catheter, kinking of the tubing or valve breakdown.
As well as infections of the shunt, so CSF culture is needed. The shunt must be removed & replaced by another when the CSF culture is sterile.

Miss.kamlah 31

Miss.kamlah 32
Nursing management Provide emotional support. Position the child carefully; don’t strain the neck
muscle since they must support the large head. Provide good skin care. Reduce the chances for skin breakdown by placing
sheepskin under the head. Provide small feeding with frequent barbing because
the infant is prone to vomiting. Elevate the head of the bed to facilitate rapid CSF
drainage. Take V/S every 2-4 hours. Use aseptic technique when performing incision care Monitor the child for malfunction of the catheter,
increased intracranial pressure or infection.

Miss.kamlah 33
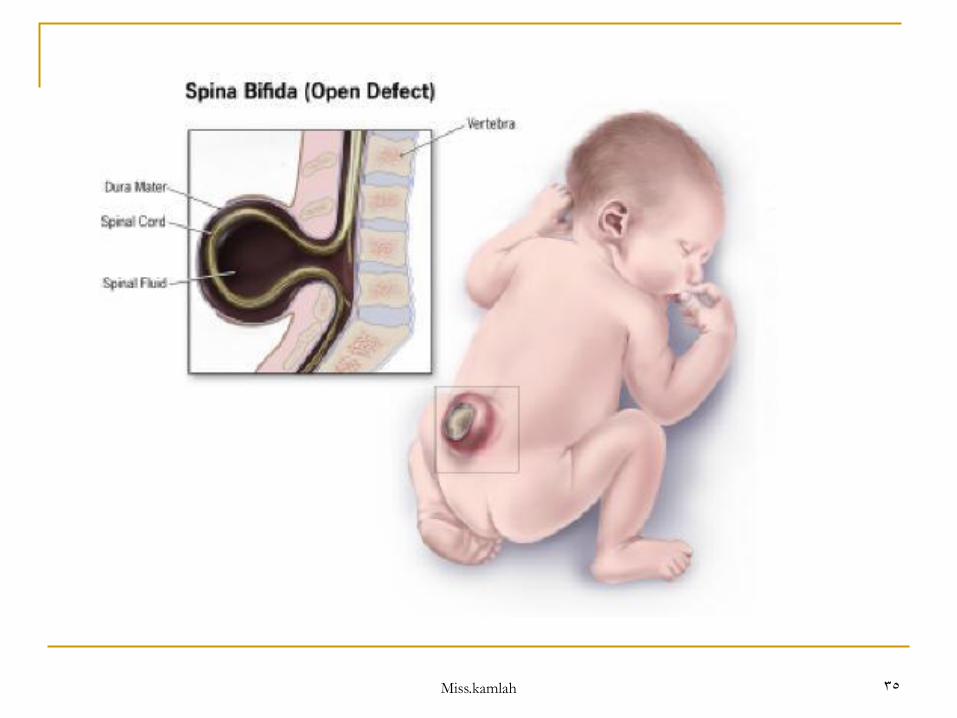
Myelomeningocele & Spina Bifida
Myelomeningocele is referred to a malformation of the spinal cord & spinal canal.
Spina bifida is referred to a defect in one or more vertebrae through which spinal cord contents can protrude.
It can occur along the vertebral column, but it occur most commonly on the lumber & sacral region.
It has unknown cause, it is associated with the use of medication, chemicals, genetic factors, maternal health conditions, as gestational diabetes, folic acid deficiency.

Miss.kamlah 34
Miss.kamlah 35

Miss.kamlah 36
Clinical Manifestations
A sac- like protrusion on the infant’s back indicates meningocele or myelomeningocele.
Sensory loss in the legs, around the anus, genetalia, & feet.
If the sac on the thoracic or lumbar 1-2 level: paralysis in the legs, weakness, & sensory loss of the trunk.
At lumbar 3 level: can flex the hip & extended the knee but ankles & toes are paralyzed.
At lumbar 4-5 level: can flex the hip & extend the knees; weak or absent ankle extension, toe flexion.
Sacral level: mild weakness in the ankles & toes; bladder & bowel function may be affected.
Miss.kamlah 37
Therapy Surgery to close & repair the lesion usually within 24-
48 hours of the infant's birth to reduce infection.
Nurses must provide preoperative & postoperative care.
Place the child in prone position with gentile handling of the child to prevent rupture of the sac & reduce the chance of infection.
Monitor CSF leakage. Monitor for signs of symptoms of infection such as
meningitis. Gentile range of motion exercise must be started to
prevent muscles atrophy.

Miss.kamlah 38
Infectious Diseases
It includes:
1. Bacterial meningitis.
2. Viral meningitis.
3. Encephalitis.

Miss.kamlah 39
Bacterial meningitis (septic)
Meningitis is an inflammation of the meninges, that can be bacterial or viral.
Bacterial meningitis is more virulent than viral meningitis & some times fatal.
Bacterial meningitis occur secondary to other infections such as otitis media, sinusitis, pharyngitis, cellulites, pneumonia, TB or due to brain trauma or neurosurgical procedure.

Miss.kamlah 40

Miss.kamlah 41
The majority of organisms that cause bacterial meningitis are Haemophilus influenza type b, Nesseria meningitis & streptococcus pneumonia.
in many cases, bacteremia spread the infection to the CNS where it inters the subarachnoid space.
An inflammatory response then follows, leading WBCs to accumulate & covering the surface of the brain with a thick, white, purulent exudates.
If infection reaches the ventricles, it will obstruct the flow of CSF causing increased intracranial pressure & hydrocephalus.

Miss.kamlah 42
Viral meningitis ( Aseptic)
Is an inflammatory process characterized by an increased number of blood cells & protein in the CSF.
The enteroviruses if often the cause of more than 80% of viral meningitis cases.
The child usually does not appear ill as in the bacterial meningitis.

Miss.kamlah 43
Clinical manifestations In bacterial meningitis:
The onset is sudden or develops over 1-2 days.
Symptoms includes high grade fever, poor feeding, vomiting, diarrhea, restless, lethargic or irritable.
In older children, they may show delirium, impaired consciousness & joint pain.
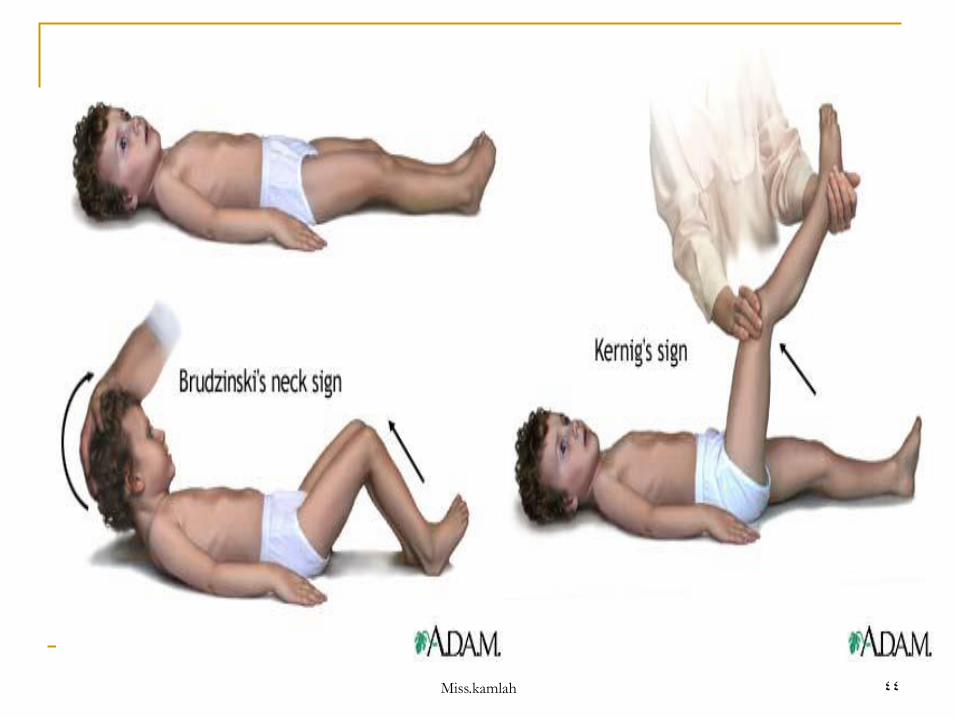
As well as to headache, photophobia, nuchal rigidity (resistance to neck flexion), positive Kernig’s or Brudzinski sign or both.
Symptoms can develop to include seizures, apnea, cerebral edema, DIC, shock, & increased intracranial pressure.
Miss.kamlah 44
Miss.kamlah 45
In viral meningitis:
The child develops general malaise, may be irritable, has low grade fever, headache, photophobia, gastrointestinal distress, upper respiratory symptoms.
Stiff neck, back pain, positive Kernig’s or Brudzinski sign or both, the child have tense anterior fontanel.
The symptoms usually resolved within 3-10 days spontaneously. Seizures are rare.
The child assume opisthotonic position, with the neck & head are hyperextend to relief discomfort.

Miss.kamlah 46
Diagnostic tests:
Diagnosis is based on:
History & physical examination.
CBC.
Blood culture.
Lumber puncture.
Ct scan.
CSF analysis & culture. That shows decreased glucose levels in the CSF in bacterial meningitis and elevated WBCs & protein in viral meningitis.
Miss.kamlah 47
Clinical therapy
In the majority of cases, antibiotic are administered as soon as tests obtained.
Antibiotic commonly used to treat bacterial meningitis includes ampicillin, aminoglycoside, cefotaxime & vancomycin.
Cortecocosteriod are given to the child who is over than 6 weeks to age to reduce the risk of sever neurological sequelae such as sensorineural hearing loss, especially in cases of Haemophilus influenza type b.

Miss.kamlah 48
Continue…
Medication to decreased the high intracranial pressure such as manitol, antipyretic, high-dose of barbiturate.
The child must kept NPO, and IVF is started.
In viral meningitis:
until the diagnosis is confirmed, the child is treated aggressively, as he or she has bacterial meningitis. Treatment is supportive of symptoms.

Miss.kamlah 49
Nursing interventions:
Monitor respiratory & neurological status.
Maintain hydration.
Administer medication.
Prevent complications.
Promote the child’s comfort with reduced stimulation (dim light, quiet room) & by placing him in a side-lying position.
Isolate the child until the organism is detected and effective treatment is underway.
Relive isolation after 48 hours from antibiotic treatment started.

Miss.kamlah 50
Encephalitis
An acute condition of an inflammation of the brain tissue. It could occur as a direct of primary infection by an organism that past the blood brain barrier.
Sign & symptoms vary according to the causative organism & the location of the infection.
Initially the child shows sever headache & fever, followed by altered mental status or focal neurological signs.
Meningial irritation signs are common such as , photophobia, nuchal rigidity, positive Kernig’s or Brudzinski sign or both.
Focal or generalized seizures may be present.

Miss.kamlah 51
Diagnosis is based on history & laboratory findings, CSF analysis, MRI, EEG, CT scan.
Treatment must include both pharmacological & supportive treatment.
As in bacterial meningitis, antibiotic treatment is started until CSF culture is done and causative organism is identified.
Nursing intervention is same as in meningitis.