papel de la anatomÍa patolÓgica en el … · papel de la anatomÍa patolÓgica en el diagnÓstico...
TRANSCRIPT
PAPEL DE LA ANATOMÍA PATOLÓGICA EN EL DIAGNÓSTICO
DE LA PANCREATITIS AUTOINMUNEDra. Mª Teresa Salcedo
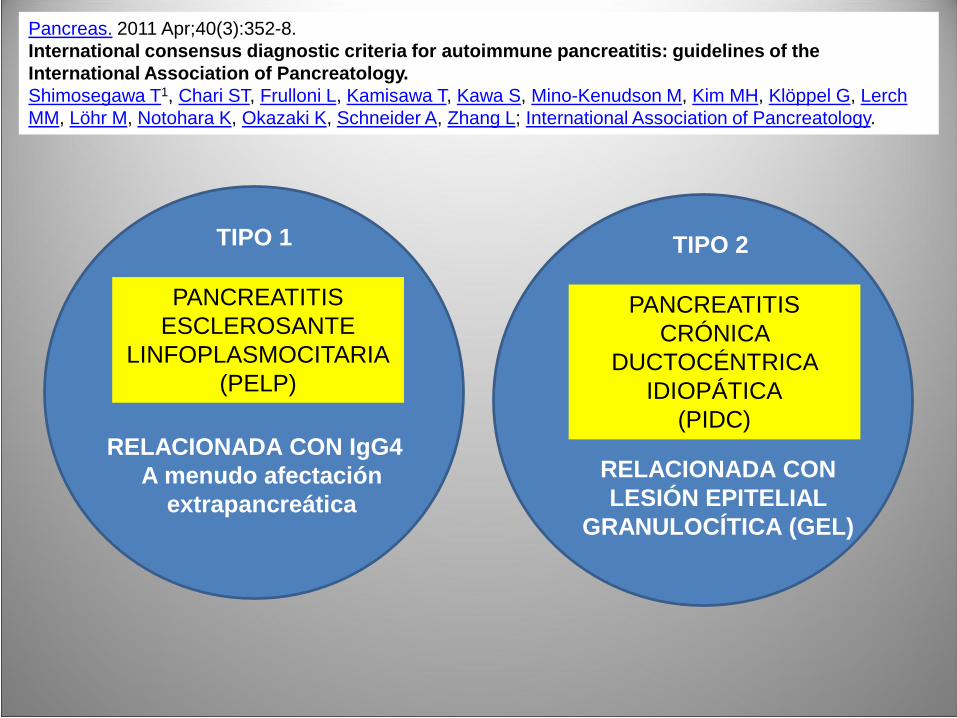
TIPO 1
PANCREATITIS ESCLEROSANTE
LINFOPLASMOCITARIA(PELP)
RELACIONADA CON IgG4A menudo afectación
extrapancreática
TIPO 2
PANCREATITIS CRÓNICA
DUCTOCÉNTRICA IDIOPÁTICA
(PIDC)
RELACIONADA CON LESIÓN EPITELIAL
GRANULOCÍTICA (GEL)
Pancreas. 2011 Apr;40(3):352-8.International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the International Association of Pancreatology.Shimosegawa T1, Chari ST, Frulloni L, Kamisawa T, Kawa S, Mino-Kenudson M, Kim MH, Klöppel G, Lerch MM, Löhr M, Notohara K, Okazaki K, Schneider A, Zhang L; International Association of Pancreatology.

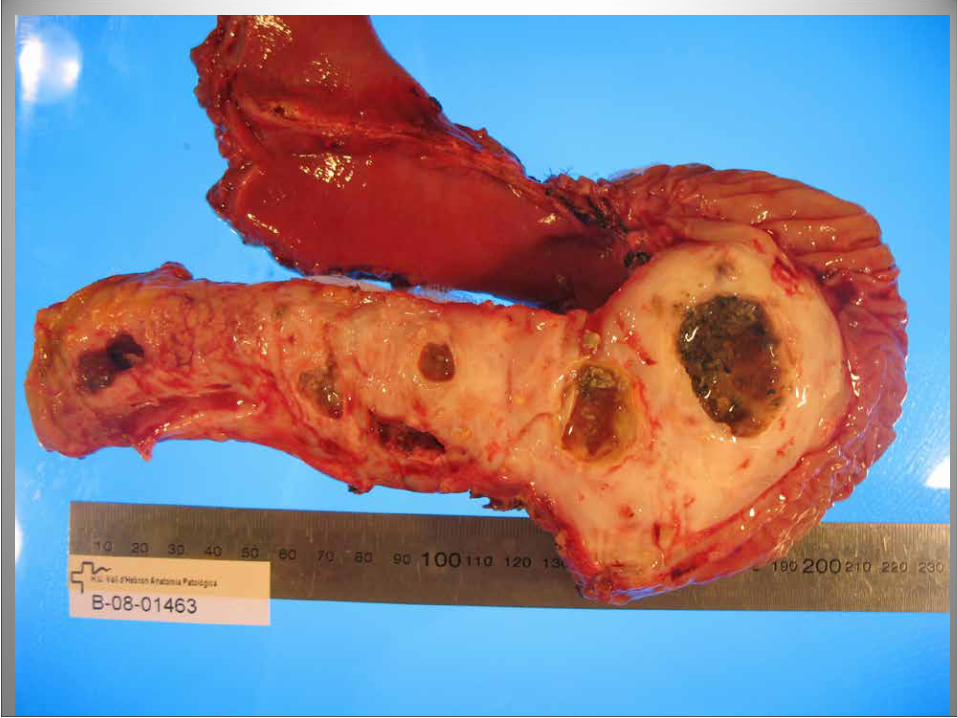
RESECCIÓN POR MASA PANCREÁTICA
PANCREATITIS Vs CARCINOMA
PANCREATITIS AUTOINMUNE (PAI)ADK DUCTAL
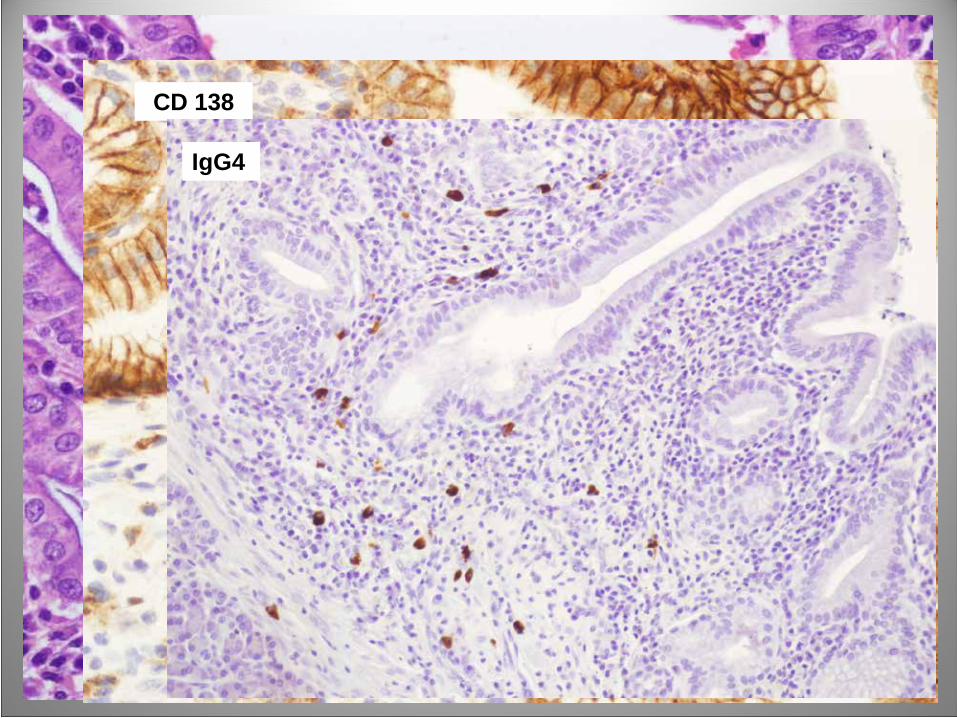
CD 138
IgG4
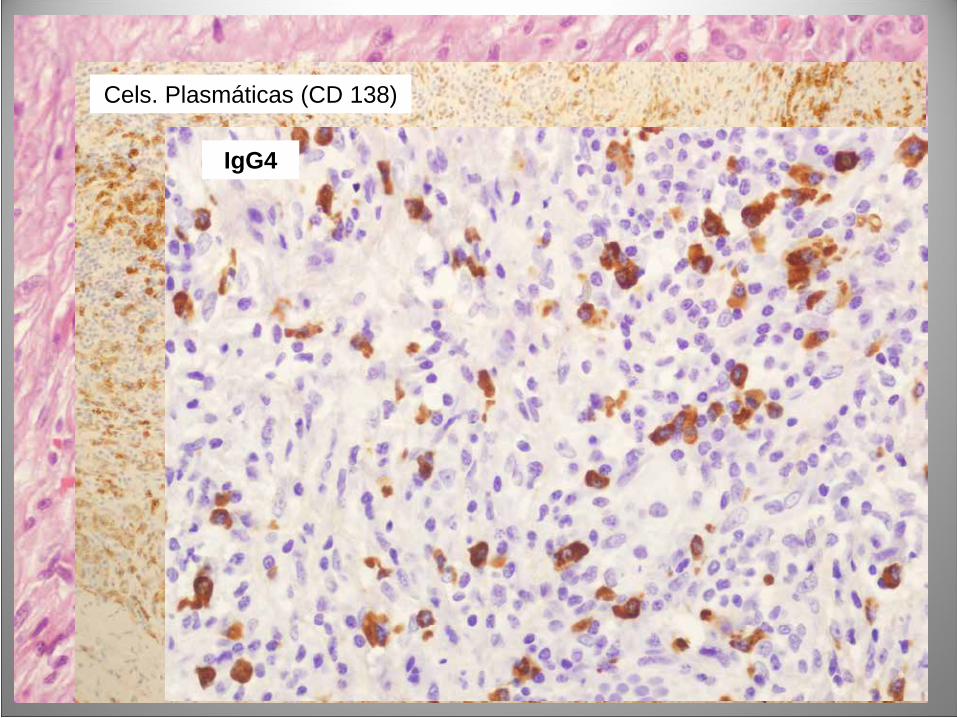
Cels. Plasmáticas (CD 138)
IgG4
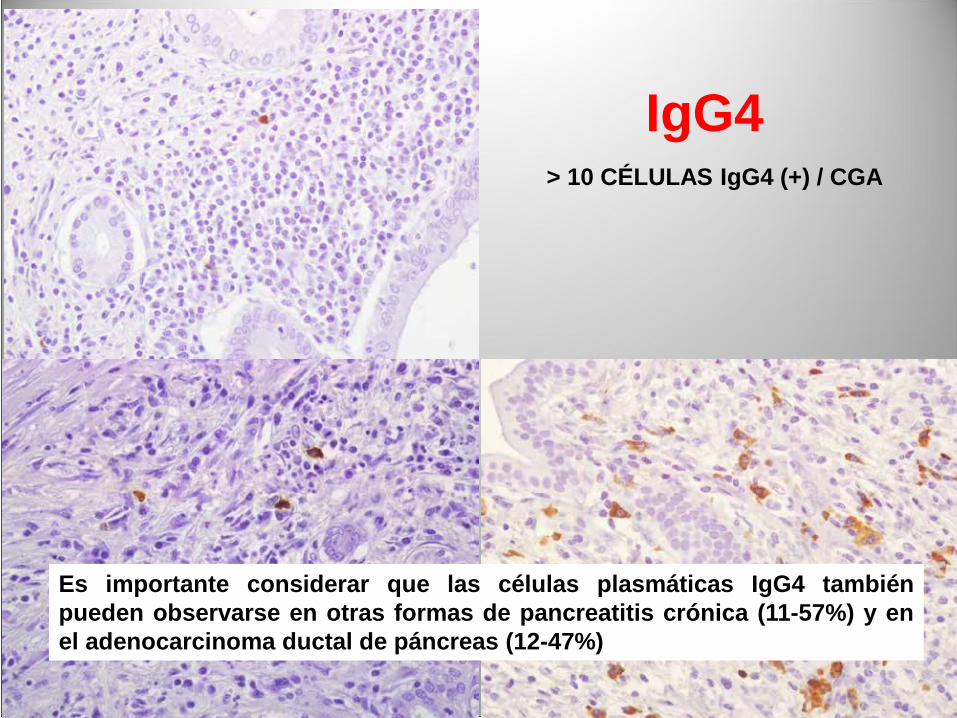
> 10 CÉLULAS IgG4 (+) / CGA
IgG4
Es importante considerar que las células plasmáticas IgG4 tambiénpueden observarse en otras formas de pancreatitis crónica (11-57%) y enel adenocarcinoma ductal de páncreas (12-47%)
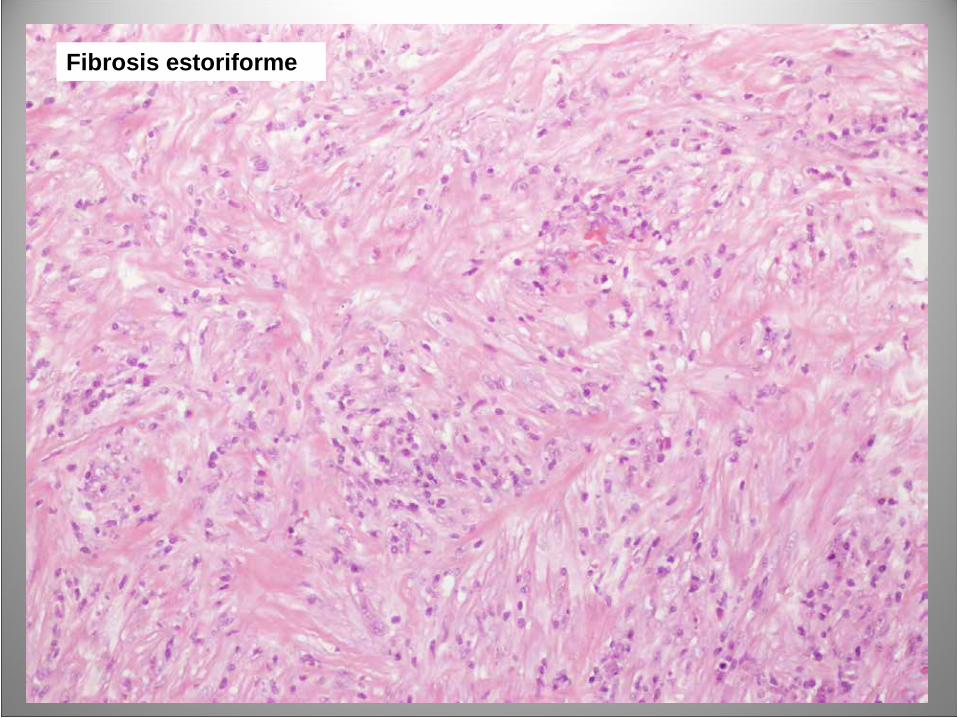
Fibrosis estoriforme
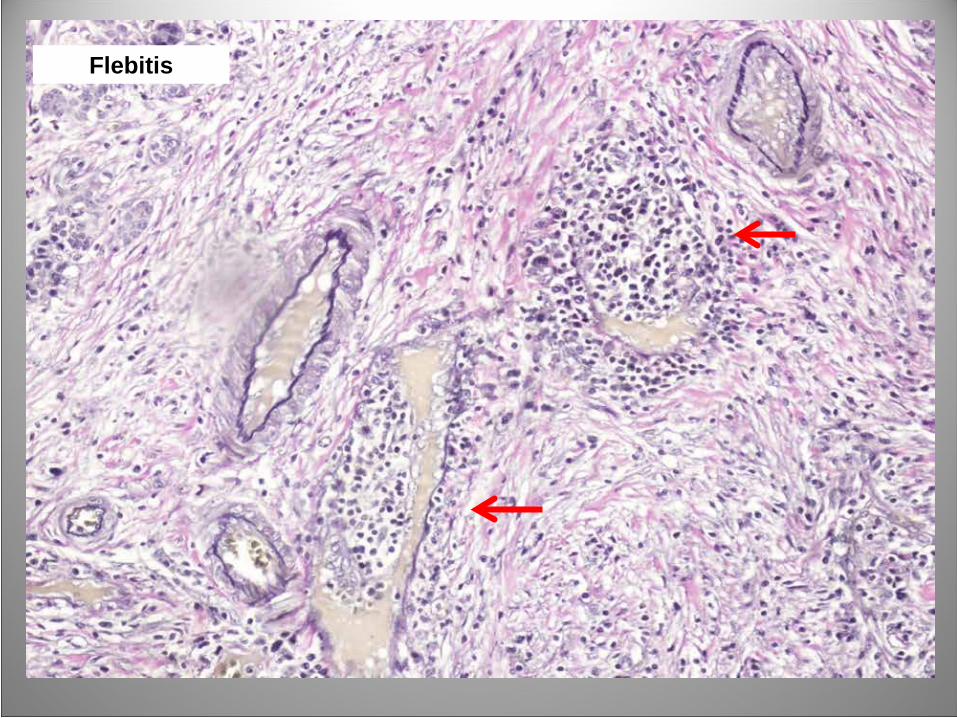
Flebitis
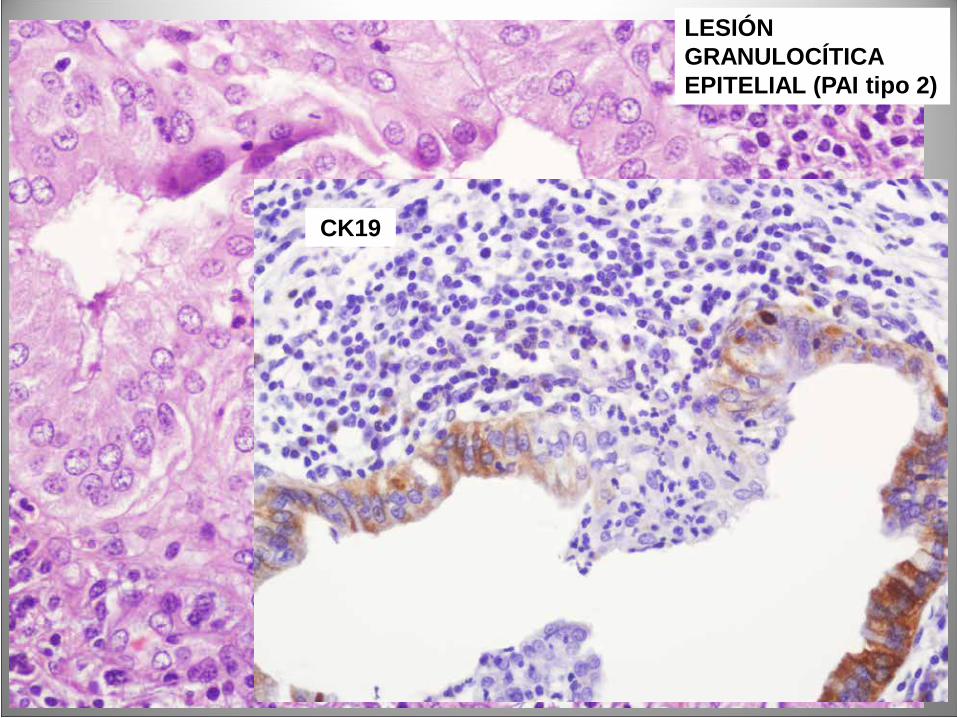
LESIÓN GRANULOCÍTICA EPITELIAL (PAI tipo 2)
CK19
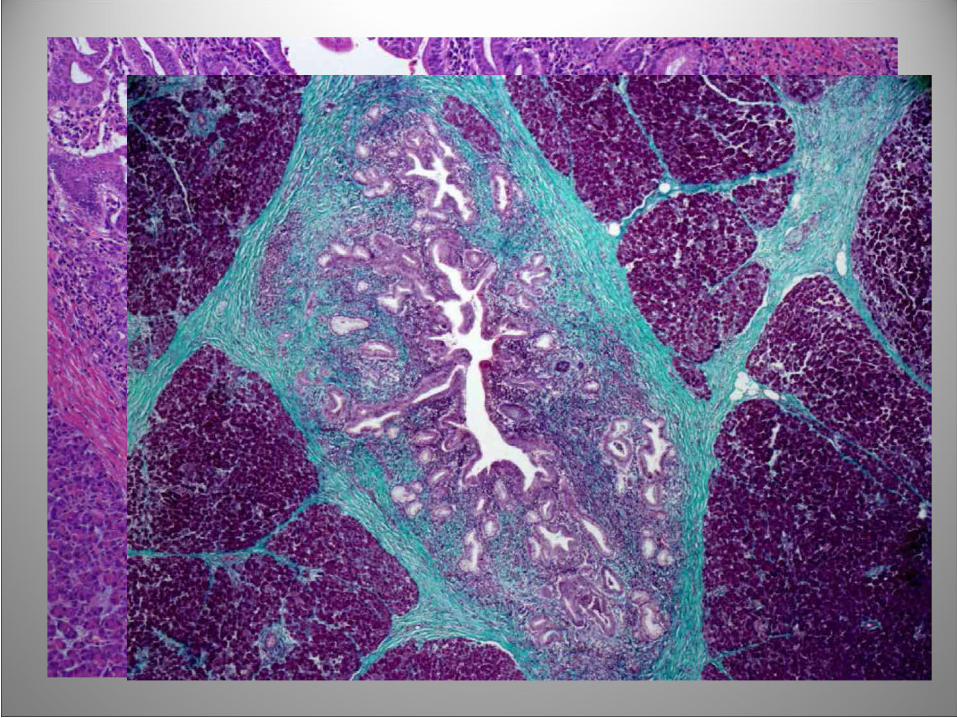
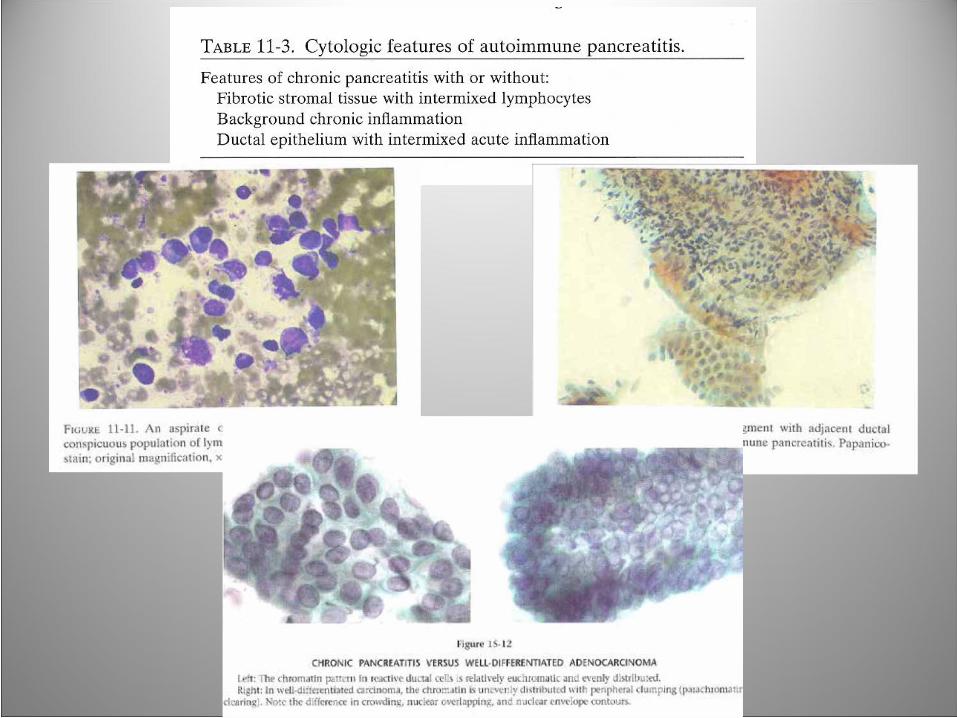
HALLAZGOS HISTOLÓGICOS EN LA PAI
•Infiltración linfoplasmocitaria alrededor de
ductos interlobulares.
• Infiltrado inflamatorio celular en el estroma
• Fibrosis densa (estoriforme)
• Flebitis obliterativa linfocítica
• Lesión epitelial granulocítica (GEL)
• Infiltración por células plasmáticas IgG4 +Shimosegawa T, Chari ST, et al. International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the International Association of Pancreatology.Pancreas 2011 Apr;40(3):352-8
TIPO DE MUESTRAS PARA EL ESTUDIO
ANATOMOPATOLÓGICO DE LA PAI:
• PAAF
• BIOPSIA
• PIEZA QUIRÚRGICA
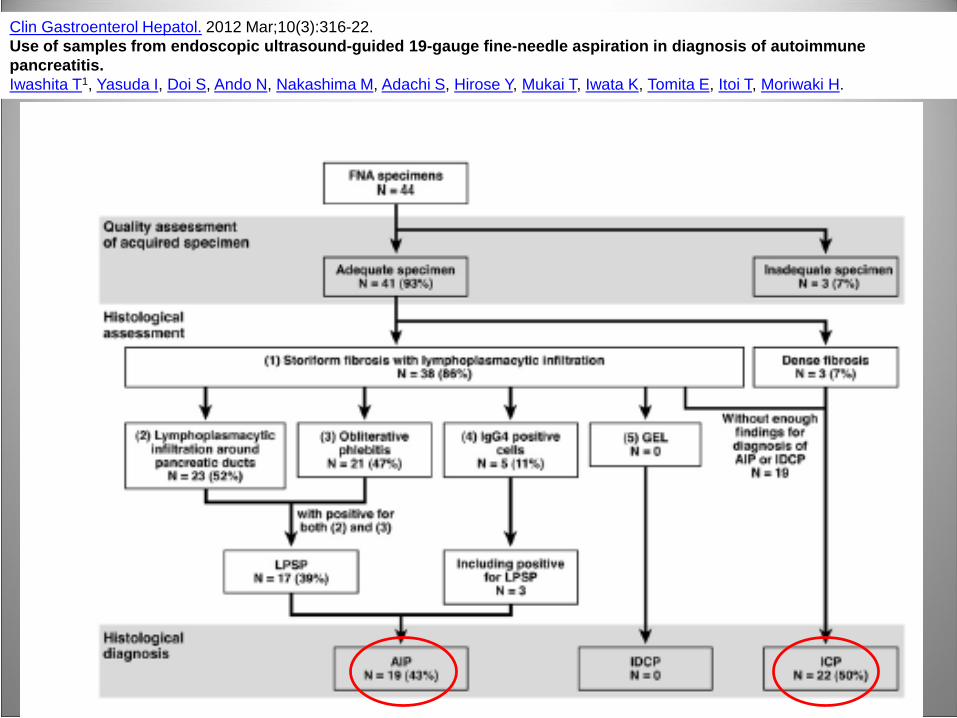
Clin Gastroenterol Hepatol. 2012 Mar;10(3):316-22. Use of samples from endoscopic ultrasound-guided 19-gauge fine-needle aspiration in diagnosis of autoimmune pancreatitis.Iwashita T1, Yasuda I, Doi S, Ando N, Nakashima M, Adachi S, Hirose Y, Mukai T, Iwata K, Tomita E, Itoi T, Moriwaki H.

Levy MJ, Wiersema RJ et al. Chronic pancreatitis: focal pancreatitis or cancer? Is there a role for
FNA/biopsy?. Autoimmune pancreatitis. Endoscopy 2006;38:S30-S35. (N:14; D(X) en el 57%)
Mizuno N, Bathia V et al. Histological diagnosis of autoimmune pancreatitis using EUS-guided
trucut biopsy: a comparision study with EUS-FNA. J Gastroenterol 2009;44:742-750 (N: 11; D(x)
en el 45%)

NILP
PARENQUIMAILP
PERIDUCTAL PLASMÁTICASIgG4 SUERO
(mg/dL) FLEBITISFIBROSIS
ESTORIFORME DIAGNÓSTICO
1 leve fibrosante leve No 230 (↑) No No PCO
2 moderado marcado ++, IgG4 (-) 53 (N) Sí Sí PAI "sugestiva"
3 leve fibrosante leve +, IgG4 (-) 55 (N) Sí No PCO
4 moderado moderado ++, IgG4 (++) NR Sí Sí PAI “concluyente"
5 moderado leve +, IgG4 (-) 68 (N) No No PAI "dudosa"
6 leve leve +, no IgG4 20 (N) No Sí PCO
7 leve leve +, IgG4 (-) NR No No PCO
8 leve leve +, IgG4 (-) 60 (N) No Sí PCO
9 ausente ausente No 139 (N) No No Esclerosis
10 marcada marcada +++, IgG4 (+++) 350 (↑) Sí Sí PAI "concluyente"
11 leve leve +, IgG4 (+) 281 (↑) Sí No PAI "dudosa"
12 marcada marcada +++, IgG4 (+++) 15 (N) Sí Sí PAI "concluyente"
13 marcada moderada +++, IgG4 (++) NR Sí Sí PAI “concluyente"
VALORACIÓN DE LA IgG4 EN EL DIAGNÓSTICO DE LA PANCREATITIS AUTOIMMUNE, UNA ENTIDAD INFRADIAGNOSTICADA.
Salcedo MT*, Montero MA*, Jimenez P*, Córdova H**, Molero X**, Balsells J ***, * Ramon y Cajal S*, Allende H*. *Departamento deAnatomía Patológica. **Departamento de Medicina Interna. ***Departamento de Cirugía. Hospital Universitario Vall d´Hebron.Barcelona
13 pacientes (2000-2010):10 piezas de pancreatoduodenectomía,1 pieza de resección pancreática córporo-caudal y 2 biopsias tru-cut (casos 2 y 11)
ILP: infiltrado linfoplasmocitario periductal; PCO: pancreatitis crónica ordinaria: PAI "concluyente:> 10 cél. IgG4 / CGA positivas; PAI "sugestiva“: 5-10 cél. IgG4 positivas / CGA) y PAI "dudosa”: <5 cél. IgG4 positivas / CGA.
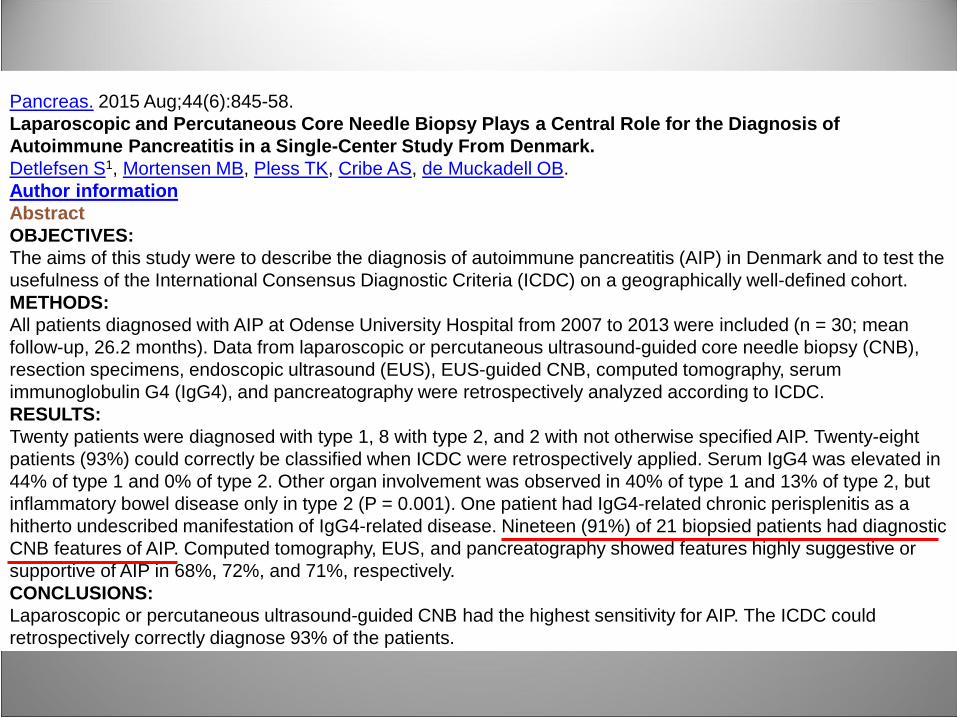
Pancreas. 2015 Aug;44(6):845-58.Laparoscopic and Percutaneous Core Needle Biopsy Plays a Central Role for the Diagnosis of Autoimmune Pancreatitis in a Single-Center Study From Denmark.Detlefsen S1, Mortensen MB, Pless TK, Cribe AS, de Muckadell OB.Author informationAbstractOBJECTIVES:The aims of this study were to describe the diagnosis of autoimmune pancreatitis (AIP) in Denmark and to test the usefulness of the International Consensus Diagnostic Criteria (ICDC) on a geographically well-defined cohort.METHODS:All patients diagnosed with AIP at Odense University Hospital from 2007 to 2013 were included (n = 30; mean follow-up, 26.2 months). Data from laparoscopic or percutaneous ultrasound-guided core needle biopsy (CNB), resection specimens, endoscopic ultrasound (EUS), EUS-guided CNB, computed tomography, serum immunoglobulin G4 (IgG4), and pancreatography were retrospectively analyzed according to ICDC.RESULTS:Twenty patients were diagnosed with type 1, 8 with type 2, and 2 with not otherwise specified AIP. Twenty-eight patients (93%) could correctly be classified when ICDC were retrospectively applied. Serum IgG4 was elevated in 44% of type 1 and 0% of type 2. Other organ involvement was observed in 40% of type 1 and 13% of type 2, but inflammatory bowel disease only in type 2 (P = 0.001). One patient had IgG4-related chronic perisplenitis as a hitherto undescribed manifestation of IgG4-related disease. Nineteen (91%) of 21 biopsied patients had diagnostic CNB features of AIP. Computed tomography, EUS, and pancreatography showed features highly suggestive or supportive of AIP in 68%, 72%, and 71%, respectively.CONCLUSIONS:Laparoscopic or percutaneous ultrasound-guided CNB had the highest sensitivity for AIP. The ICDC could retrospectively correctly diagnose 93% of the patients.
CONCLUSIONES•LA PANCREATITIS AUTOINMUNE PROBABLEMENTE SIGA SIENDO UNA
ENTIDAD INFRADIAGNOSTICADA
•LOS CRITERIOS HISTOLÓGICOS ESTÁN BIEN DEFINIDOS, AUNQUE
AMBOS TIPOS DE PAI PUEDEN COMPARTIR MÁS DE UNO.
• LA BIOPSIA PANCREÁTICA Y LA PAAF POR ECO ENDOSCOPIA SON
ESTUDIOS ADECUADOS PARA EL DIAGNÓSTICO DE PAI CUANDO
EXISTE UNA SOSPECHA CLÍNICA. AUNQUE PUEDEN MOSTRAR
LIMITACIONES DEBIDO A LA NATURALEZA PARCHEADA DE LA
ENFERMEDAD Y AL TAMAÑO DE LA MUESTRA
Bibliografía:1. Shimosegawa T, Chari ST, et al. International consensus diagnostic criteria for autoimmune
pancreatitis: guidelines of the International Association of Pancreatology. Pancreas 2011Apr;40(3):352-8.
2. Chari ST, Kloeppel G et al. Histopathologic and Clinical Subtypes of Autoimmune Pancreatitis: TheHonolulu Consensus Document. Pancreatology. 2011 Jan 18;10(6):664-672.
3. Iwashita T, Yasuda I et al.Use of samples from endoscopic ultrasound-guided 19-gauge fine-needleaspiration in diagnosis of autoimmune pancreatitis. Clin Gastroenterol Hepatol. 2012 Mar;10(3):316-22.
4. Levy MJ, Wiersema RJ et al. Chronic pancreatitis: focal pancreatitis or cancer? Is there a role forFNA/biopsy?. Autoimmune pancreatitis. Endoscopy 2006;38:S30-S35.
5. Mizuno N, Bathia V et al. Histological diagnosis of autoimmune pancreatitis using EUS-guided trucutbiopsy: a comparision study with EUS-FNA. J Gastroenterol 2009;44:742-750
6. Friedlander J, Quiros JA, et al. Diagnosis of autoimmune pancreatitis vs neoplasms in children withpancreatic mass and biliary obstruction. Clin Gastroenterol Hepatol. 2012 Sep;10(9):1051-5.e1.
7. Zamboni G, Lütges J, et al. Histopatological features of diagnostic and clinical relevance inautoimmune pancreatitis: a study of 53 resection specimens and 9 biopsy specimens. Virchows Arch220;445:552-563
8. Deftlesen S, Mortensen MB et al.Laparoscopic and Percutaneous Core Needle Biopsy Plays aCentral Role for the Diagnosis of Autoimmune Pancreatitis in a Single-Center Study From Denmark.Pancreas 2015 Aug;44(6):845-58
9. Deftesen S, Bräsen JH, et al. Deposition of complement C3c, Immunoglobulin (Ig)G4 and IgG at thebasement membrane of pancreatic ducts and acini in autoimmune pancreatitis. Histopathology 2010;57:825835.
10. Kubota K, Kato S et al. Usefulness of endoscopic biopsy using FOXP3(+) Treg up-regulation in theduodenal papilla in the differential diagnosis between autoimmune pancreatitis and pancreatic cancer.J Hepatobiliary Pancreat Sci. 2010 Nov 27.
11. Jung JG, Lee JK, et al. Comparison of endoscopic retrograde cholangiopancreatography withpapillary biopsy and endoscopic ultrasound-guided pancreatic biopsy in the diagnosis of autoimmunepancreatitis.Pancreatology 2015;15(3):259-264.