podd 2015 sonescence
TRANSCRIPT
Ultrasonic Drug Dispersion
A new way to directly deliver drugs to where they are
neededOctober 5, 2015
Ultrasonic drug dispersion
• A New Drug Delivery Method• For serious conditions– examples for serious infections of skin and soft
tissue• Achieves:
a) Local delivery of drug or biologic molecules at therapeutic concentrations to skin, tissue or organs;b) minimal systemic drug exposure
• Product: Durable device + consumables + drug
2
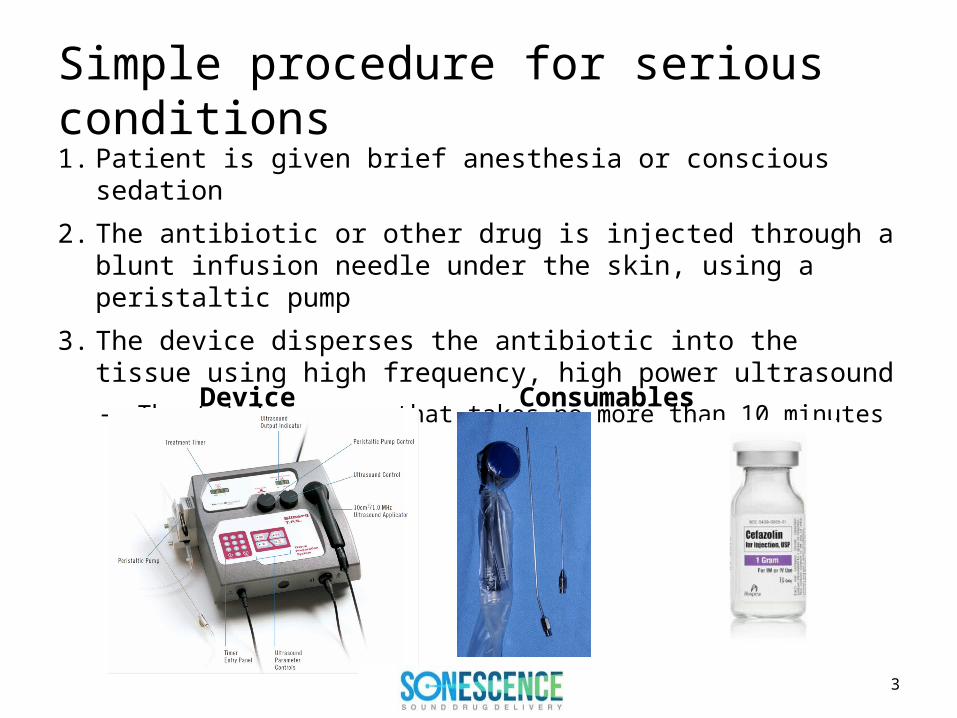
Simple procedure for serious conditions1. Patient is given brief anesthesia or conscious sedation
2. The antibiotic or other drug is injected through a blunt infusion needle under the skin, using a peristaltic pump
3. The device disperses the antibiotic into the tissue using high frequency, high power ultrasound– The total process that takes no more than 10 minutes
Device Consumables Drug
3
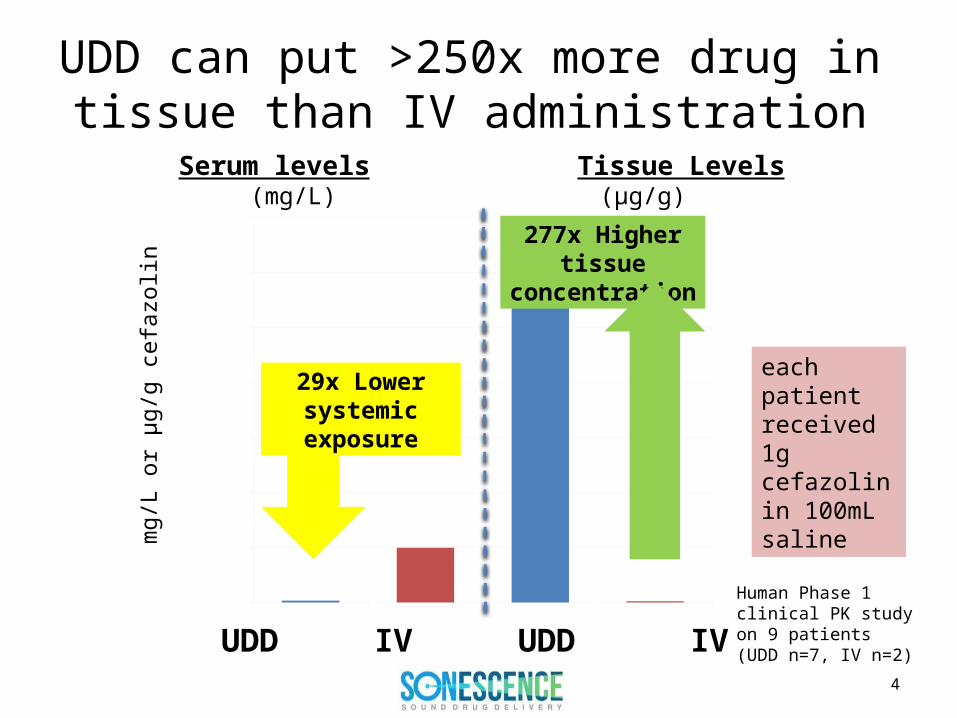
UDD can put >250x more drug in tissue than IV administration
mg/
L or
µg/
g ce
fazo
lin
TPS Serum
IV Serum TPS Tissue
IV Tissue0
200
400
600
800
1,000
1,200
1,400
6.9
199.2
1328
4.8
277x Higher tissue concentration
UDD IV UDD IV
Human Phase 1 clinical PK study on 9 patients (UDD n=7, IV n=2)
29x Lower systemic exposure
Serum levels Tissue Levels (mg/L) (µg/g)
each patient received 1g cefazolin in 100mL saline
4

Example Case Study • Patient: 75-year old female diabetic with open wound of the lower leg• Organisms cultured: Staphylococcus aureus (MRSA) • History: 6 weeks IV antibiotics, 36 days hospitalization, multiple debridements• Treatment: Debridement +UDD 1g cefazolin in 100mL + rotation flap closure and
split thickness skin graph (STSG)• Outcome: Grafts take 100%, infection completely healed; no recurrence at 3
month visit
Clinical evidence of efficacy: treating drug resistant skin and soft tissue infections
*Silberg and Nicolau, 2015 SAWC Poster CR-030
Before UDD cefazolin 3 mo after UDD cefazolin14 days after UDD cefazolin + STSG
5
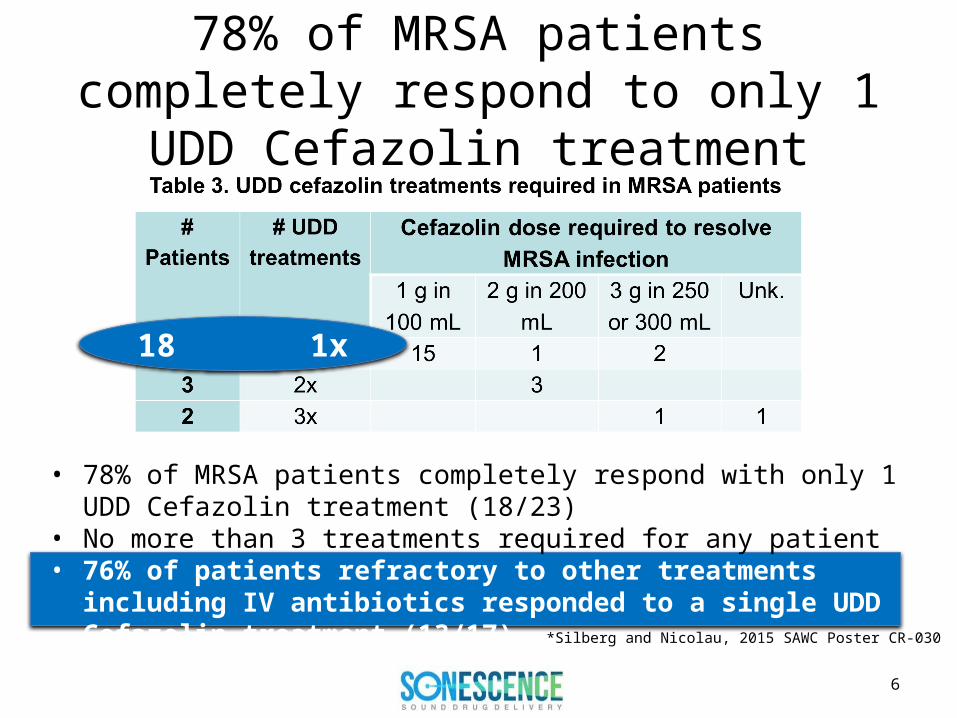
78% of MRSA patients completely respond to only 1 UDD Cefazolin treatment
*Silberg and Nicolau, 2015 SAWC Poster CR-030
• 78% of MRSA patients completely respond with only 1 UDD Cefazolin treatment (18/23)
• No more than 3 treatments required for any patient• 76% of patients refractory to other treatments including IV antibiotics
responded to a single UDD Cefazolin treatment (13/17)
18 1x
6
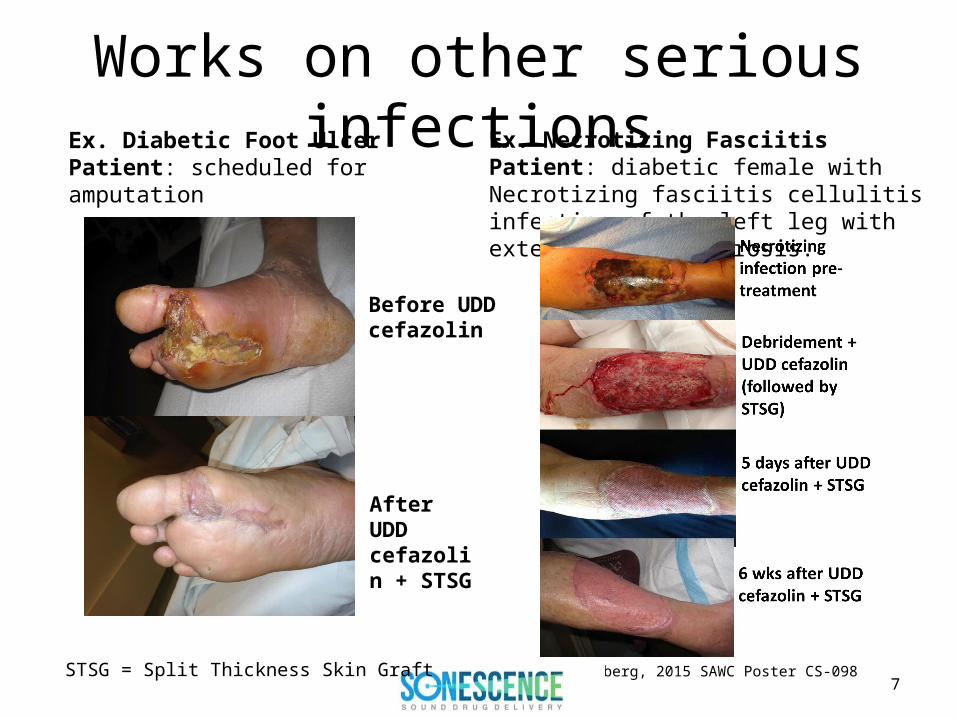
Works on other serious infectionsEx. Necrotizing Fasciitis Patient: diabetic female with Necrotizing fasciitis cellulitis infection of the left leg with extensive skin necrosis.
Ex. Diabetic Foot Ulcer Patient: scheduled for amputation
Before UDD cefazolin
After UDD cefazolin + STSG
*Silberg, 2015 SAWC Poster CS-0987
STSG = Split Thickness Skin Graft

Connecting the dots = a new treatment paradigm
1. NO MRSA isolates resistant to >1,000mg/L Cefazolin
2. Ultrasonic Drug Delivery (UDD) introduced cefazolin to tissue at levels >1,000mg/L
3. UDD Cefazolin eliminated treatment-resistant MRSA infections in ONE treatment in 3/4ths of patients
1. Nicolau, DP and Silberg BN. ICAAC 2015. Poster # C-1071. 2. Silberg BN. Supplement to Plastic and Reconstructive Surgery, 2013 Vol. 132( 4S-1):p51-52.3. Silberg BN and Nicolau, DP. SAWC 2015. Poster # CR-030.
8

Dose sparing: reducing drug exposure
• Vancomycin– Narrow therapeutic window: risk of nephrotoxicity– IV requires carefully timed infusion– Usual Adult Dose for Skin or Soft Tissue Infection (SSTI)
• 15 mg/kg IV every 12 hours (>2g/day for 70kg person)• Duration: 10 to 14 days, depending on the nature and severity of the
infection
• UDD Vancomycin for serious SSTI– 6 patients treated off label
• 50µg to 1mg total dose (in 5-100mL) (>1,000 times LESS than IV)• Only 1 (n=4) or 2 (n=2) treatments required to eradicate infection
(including 1 MRSA case) not 1.5-2 weeks on IV therapy
9
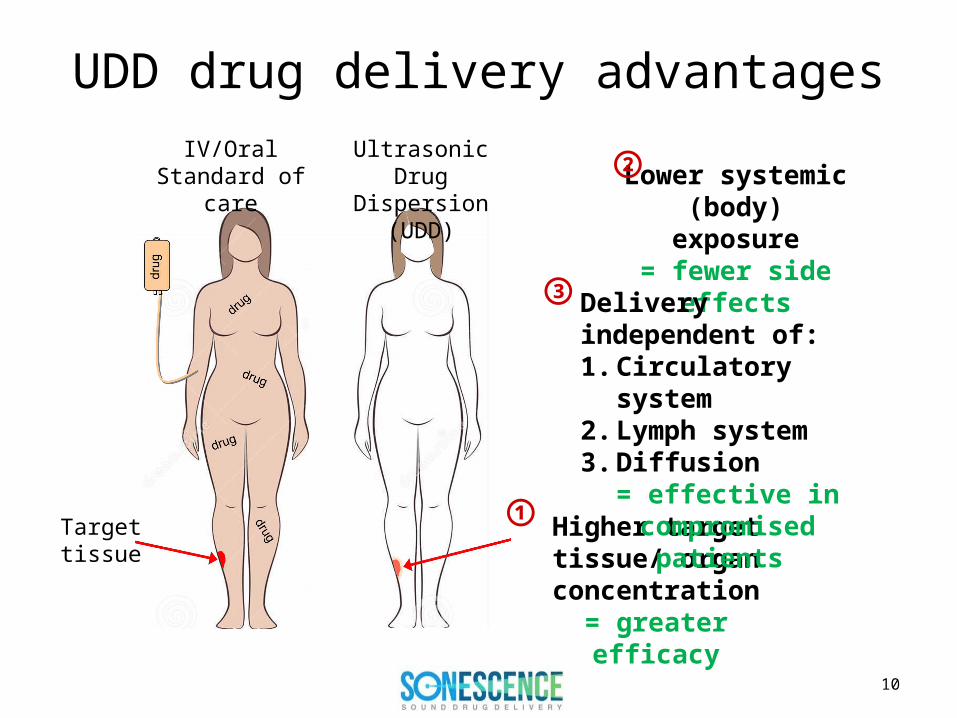
UDD drug delivery advantages
Higher target tissue/ organ concentration
= greater efficacy
IV/OralStandard of care
Ultrasonic Drug Dispersion (UDD)
Target tissue
Lower systemic (body) exposure
= fewer side effects
Delivery independent of:1. Circulatory system2. Lymph system3. Diffusion
= effective in compromised patients
①
②
③
10

Sonescence Team combines surgery, ultrasound, anti-infective and drug delivery expertsMichael J. Weickert, PhD; CEOFormer CEO and co-founder SEA Medical Systems, CBO Corium, CBO Stratagent, Nektar, Inhale, Ligand, Somatogen, Auspex, NIH
Seth J. Putterman, Ph.D.; CTO Professor of Physics Department of Physics & Astronomy, UCLA, President &CEO of Julian Schwinger Foundation for Physics Research, Chair Science Advisory Board Tribogenics Inc. former Board Member Parametric Sound (NASDAQ:PAMT).
Michele Brulé, MBA; COO and Co-Founder, Director Operations, Santa Rosa Antibiotic Effectiveness Project
Barry N. Silberg, M.D., F.A.C.S; CMO and FounderPlastic and Reconstructive Surgeon, inventor TPS system and Ultrasonic Drug Dispersion
David P. Nicolau, PharmD, FCCP, FIDSA, Advisor Director of the Center for Anti-Infective Research and Development and Coordinator for Research in the Department of Medicine, Division of Infectious Disease and Pharmacy at Hartford Hospital, CT
11

Sonescence is seeking UDD partners
• Antibiotic suppliers/partners for serious skin and soft tissue infections
• Development partners for proprietary products in other serious conditions where – targeted therapy has inherent advantages or– dose sparing therapy is beneficial
• Investors
12

In the 1980s Barry Marshall and J. Robin Warren demonstrated that Heliobacter pylori caused gastric ulcers. That led to a simple and effective therapy.
Dr. Barry Silberg discovered how to put enough drug directly into infected tissue to kill resistant organisms. This innovation is simple and its impact on wound healing
and drug delivery could be just as profound as Marshall and Warren’s was for ulcers.
Contact:Michael J. Weickert, Ph.D.