post operative complications
DESCRIPTION
Post operative complications. อาจารย์ที่ปรึกษา อ.พญ.พิมประภา กัณฑะษา จัดทำโดย นสพ . กมลศักดิ์ อุ่นตา นสพ.รัฐศาสตร์ พุ่มรส นสพ.พิมลศักดิ์ ศรีธรรมา นสพ.ใหม่ จำปาศักดิ์ โรงพยาบาลพิจิตร. Content. Wound complication Thermal regulation complication Pulmonary complication - PowerPoint PPT PresentationTRANSCRIPT

Post operative complications
อาจารย์�ที่�ปร�กษาอ.พญ.พ�มประภา กั ณฑะษา
จ�ดที่�าโดย์นสพ. กัมลศั กัดิ์�� อ� �นตา
นสพ.ร ฐศัาสตร� พ� �มรส
นสพ.พ�มลศั กัดิ์�� ศัร�ธรรมา
นสพ.ใหม� จำ!าปาศั กัดิ์��
โรงพย์าบาลพ�จ�ตร1

Content• Wound complication• Thermal regulation complication• Pulmonary complication• Endocrine complication• Cardiovascular complication• Neurological complication• Renal complication• GI complication• HEENT complication
2

WOUND COMPLICATIONS
3

Wound Complications
1. Wound infection2. Wound hematoma3. Wound seroma4. Wound dehiscence
4
Surgical and environment factorPre-op, Intra-op, Post-op
Microbial factorStaphylococcus aureusEnteric organism in the boweloperations
Host factor U/D
Wound infection
5

Classification of operative wounds and risk of infection
Classification Criteria Risk (%)Clean Elective, not emergency, nontraumatic,
primarily closed; no acute inflammation; no breka in technique; respiratory, gastrointestinal, biliary and genitourinary tracts not entered
2<
Clean-contaminated
Urgent or emergency case that is otherwise clean; elective opening of respiratory, gastrointestinal, biliary or genitourinary tract with minimal spillage (e.g., appendectomy) not encountering infected urine or bile; minor technique break
10<
Contaminated Nonpurulent inflammation; gross spillage from gastrointestinal tract; entry into biliary or genitourinary tract in the presence of infected bile or urine; major break in technique; penetrating trauma < 4 hours old; chronic open wounds to be grafted or covered
Approx. 20
Dirty Purulent inflammation(e.g., abscess); preoperative perforation of respiratory, gastrointestinal, biliary or genitourinary tract; penetratinbg trauma > 4 hours old
Approx. 40
6

Clinical presentation
• Inflammatory sign– Pain – Swollen and edematous– redness and cellulitis– warmth
• Fever , Heart rate increase
• Day 5th – 8th postoperative days
7

Mangement
• Depends on the extent of destruction and the type of the wound infection
• Simple collection of purulent material in skin and subcutaneous.
• Opening the incision and drainage
• Debridement
8

Wound hematoma
• Caused by inadequate hemostasis• Pain and swelling• Serosanguinous in drainage
• Wound opened and evacuated • Closed suction (predisposing factor/ hemostasis)• Correct hemostasis problem
9

Wound seroma• Lymph collection• Large area of lymph-bearing tissues are transected• Fertile ground for bact wound infect
• Management repeat aspiration/ closed suction drainage
10
Wound dehiscence
• The seperation within the fascial layer
• Usually of the abdomen
• Generally caused by technical factor
• Incision in vertical horizontal incision
11

Wound dehiscence (Cont.)
• Factors– Malnutrition– Hypoproteinemia – morbid obesity– Malignancy w/ immunologic deficiency– Uremia– DM – Coughing increase abd. Pressure– Remote infection
12

Wound dehiscence (Cont.)
• Local factors
– Midline vertical incision
– Hemorrhage
– Wound infection
– Poor technique
13

Prevention
• Correct factor : infection, nutrition, blood sugar
• Midline incision oblique, transverse incision
• Mass closure suture
• Suture material
• Chromic catgut dehiscence
• Nylon, prolene, steel wire
• Dexon, vicryl
14
Thermal regulation complications
15

Thermal regulation
1. Fever2. Malignant Hyperthermia3 . Hypothermia
16

Post-operative fever
17

Pathophysiology• Fever >38ºC is common after surgery• Usually inflammatory stimulus of surgery and resolves
spontaneously• Fever = response to cytokine release
– Fever-associated cytokines are released by tissue trauma and do not necessarily signal infection
– Cytokines produced by monocyte, macrophages, endothelial cells
– Fever-associated cytokines = IL-1, IL-6, TNF-alpha, IFN-gamma
18

สาเหต�ที่�พบบ�อย์ ใช้ ต�วย์�อคื#อ “ 5W” โดย์เก�ดเร�ย์งล�าด�บหล�งการผ่�าต�ดด�งนี้�&
•Wind, POD1-2: the lungs, i.e. pneumonia, aspiration, and pulmonary embolism, but not atelectasis•Water, POD3-5: urinary tract infection•Walking (or VEINS, which then sounds like "Weins"), POD4-6: deep vein thrombosis or pulmonary embolism•Wound, POD5-7: surgical site infection, which in obstetrics or gynaecology, may refer to the Womb.•Wonder drugs or “What did we do?”, POD7+: drug fever, infections related to intravenous lines
19

Causes of Postoperative Fever
20

21
Malignant Hyperthermia
• After exposure to a triggering GA (anesthetic complications)
• Occurs rare in 1 in 30,000 to 50,000 adults .
22
INCIDENCE
• 1:12 000 - 1:40 000
• Male = Female
• No racial difference
23

• Susceptibility to MH is inherited as an
AD disease (mutation)
Altered Ca2+ regulation in skeletal muscle
Abnormal release of Ca2+
Prolonged activation of muscle filaments
Excessive generation of heat .
• If untreated : myocyte death rhabdomyolysis hyperK & myoglobulinuria .
24

Clinical presentation
• Rapid rise in body temp ,usually during the initiaton of a GA after admin. of succinylcl.or potent inhalation agent ,particularly halothane
• Metabolic acidosis & e’lyte imbalance (hyperCa2+)
• Hypotonicity of skeletal muscle (acidosis)
• >42 C hypercapnia, cardiac arrhythmia
25
FULMINANT CRISIS
• Tachycardia
• Metabolic acidosis, O2 sat, pCO2
• Muscle rigidity• Electrolyte disturbance• Arrhythmias• Myoglobinuria• Hyperthermia
26

DIAGNOSIS, consider MH if
• Masseter muscle spasm after sux• Unexplained, unexpected
tachycardia• Unexplained, unexpected
increase in end - tidal CO2
27

EARLY MANAGEMENT 1
• STOP ALL ANAESTHETIC VAPOURS
• CHANGE TO CLEAN ANAESTHETIC BREATHING SYSTEM
• ABANDON SURGERY IF FEASABLE
28

EARLY MANAGEMENT 2
• DANTROLENE
• MEASURE ABGs, K+ AND CK
• MEASURE CORE TEMP
• COOL PATIENT
29

Hypothermia
• Core temperature below 35° C• 80% of elective operative procedu
res are associated with a drop in body temperature
• 50% of trauma patients are hypot hermic on arrival in the operating
suite.
30

Risk Factors for Decreased Thermostability
31
• C ool ambient room temp.
• R apid administration of IV fluids or blood.
• Prolonged surgical procedure
• Advanced age
• Opioid analgesia
• Propofol causes vasodilation and significant redistribution hypothermia
32
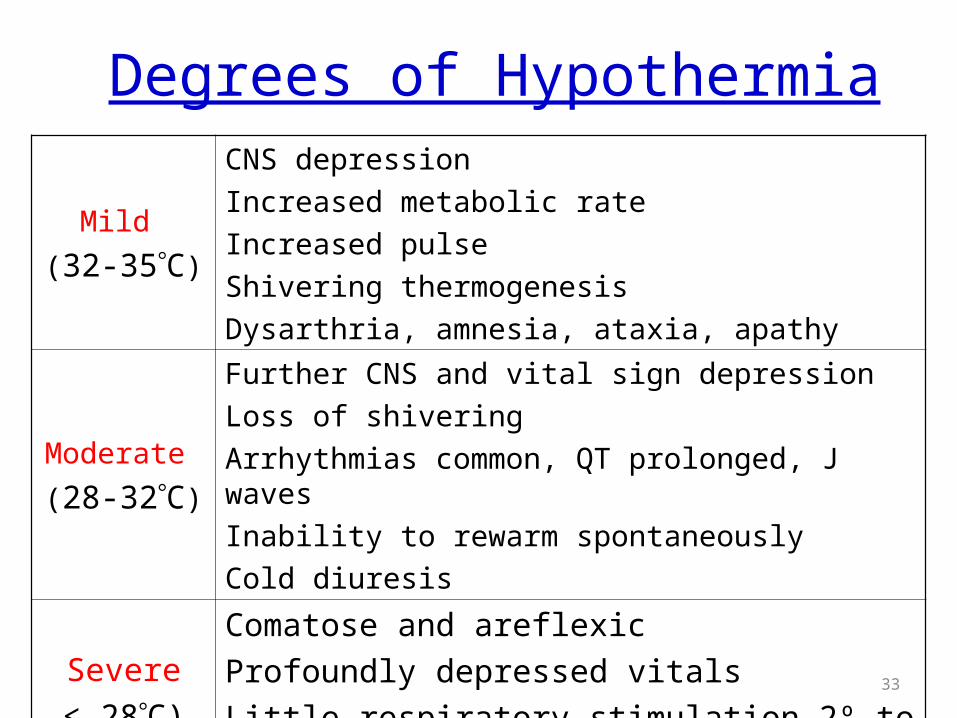
Degrees of Hypothermia
Mild
(32-35C)
CNS depression
Increased metabolic rate
Increased pulse
Shivering thermogenesis
Dysarthria, amnesia, ataxia, apathy
Moderate
(28-32C)
Further CNS and vital sign depression
Loss of shivering
Arrhythmias common, QT prolonged, J waves
Inability to rewarm spontaneously
Cold diuresis
Severe
< 28C)
Comatose and areflexic
Profoundly depressed vitals
Little respiratory stimulation 2º to low CO233

• A core temperature < 35°C after surgery
• Hypertension (S ympathetic NE vasoconstricti on elevated arterial blood pressure)
• Shivering, uncomfortable cold sensation
Clinical presentation
34

• Core To < 35°C
• Early postoperative ischemia
• Ventricular tachyarrhythmia.
• Coagulation defect bleeding– Impairs platelet function – Reduces the activity of coagulation factors
35

• Poor healing and infection.
– Impaired macrophage function
– Reduced tissue oxygen tension
– Impaired collagen deposition
– Relative diuresis
– Compromised hepatic function
– Neurologic manifestations .
• Impaired - acid base balance
• In severe cases the patient
– Bradycardia low BP
– Decrease RR
– Comatose
36

• Monitoring core temperature, – Undergoing body cavity surgery– Surgery lasting longer than 1 hour– Children and the elderly– General-epidural anesthesia
• Anesthetized and during skin preparation significant evaporative cooling can take place the patient is kept warm by increasing the ambient temperature and using heated humidifiers and warmed IV fluid .
Prevention
37

Treatment
• Warm blankets• Forced-air warming devices• Infusion of blood and IV fluids through a warming
device• Heating and humidifying inhalational gases • Peritoneal lavage with warmed fluids• In rare cases, cardiopulmonary bypass
38