ppt jurnal
DESCRIPTION
pptTRANSCRIPT

JURNAL READING Chest X-ray – Lung Disease
Nathania Christika
406147045


CONSOLIDATION
1. Lobar consolidation
2. Diffuse consolidation
3. Multifocal ill-defined consolidations

Characteristics of Consolidation
• Produces opacities in the lung that can be described as fluffy, cloudlike, and hazy.
• The opacities tend to be confluent, merging into one another.
• The margins of airspace disease are fuzzy and indistinct.
• Air bronchograms or the silhouette sign may be present.



Shillouete Sign
Solid black arrow : hilangnya bayangan batas kanan jantung Dotted black arrow : bayangan hemidiafragma kanan tidak hilang

Key sign to recognizing Pneumonia
• More opaque than surrounding normal lung. • In airspace disease, the margins may be fluffy and indistinct
except where they abut a pleural surface like the interlobar fissures where the margin will be sharp.
• Interstitial pneumonias will cause a prominence of the interstitial tissues of the lung in the affected area; in some cases, the disease can spread to the alveoli and resemble airspace disease.
• Pneumonia tends to be homogeneous in density. • Lobar pneumonias may contain air bronchograms. • Segmental pneumonias may be associated with atelectasis in
the affected portion of the lung.

Right upper lobe pneumococcal pneumonia
Dotted white arrow : air bronchograms Solid white arrow : The inferior margin of the pneumonia is more sharply demarcated because it is in contact with the minor fissure

Lobar Pneumonia
• Diagnosis
Pneumonia - consolidation with pus
• Differential diagnosis of consolidation Pneumonia - airways full of pus Cancer - airways full of cells Pulmonary haemorrhage - airways full of blood Pulmonary oedema - airways full of fluid

Bronchopneumonia
Multiple irregularly marginated patches of airspace disease are present in both lungs (solid white arrows). The disease is spread centrifugally via the tracheobronchial tree to many foci in the lung at the same time so it frequently involves several segments. Because lung segments are not bound by fissures, the margins of segmental pneumonias tend to be fluffy and indistinct. No air bronchograms are present because inflammatory exudate fills the bronchi as well as the airspaces around them.

Acute pulmonary alveolar edema
• Solid white arrows : Fluffy, bilateral, perihilar airspace disease with indistinct margins, sometimes described as having a bat-wing or angel-wing.
• No air bronchograms are seen.
• The heart is enlarged.
• This represents pulmonary alveolar edema secondary to congestive heart failure.

BATWING :
• Konsolidasi bilateral pada perihilar
• Khas pada Edem Pulmo
REVERSED BATWING :
• Konsolidasi perifer/subpleura
• Ditemukan pada penyakit paru kronis

Batwing & Reverse Batwing

INTERSTITIAL DISEASE
1. Reticular
2. Nodular
2. Reticonodular

The patterns of interstitial lung disease
Reticular Nodular Reticulonodular, have a mixture of
both a reticular (lines) and nodular (dots)
pattern

Characteristics of Interstitial Lung Disease
• Interstitial disease has discrete reticular, nodular, or reticulonodular patterns.
• “Packets” of disease are separated by normal-appearing, aerated lung.
• Margins of “packets” of interstitial disease are usually sharp and discrete.
• Disease may be focal or diffusely distributed in the lungs.
• Usually no air bronchograms are present.

1. RETICULAR :

Pulmonary interstitial edema secondary to congestive heart failure
Black circle : A close-up view of the right lung shows an accentuation of the pulmonary interstitial markings.
White circle : Multiple Kerley B lines represent fluid in thickened interlobular septa.
Solid black arrow : Fluid is seen in the inferior accessory fissure.
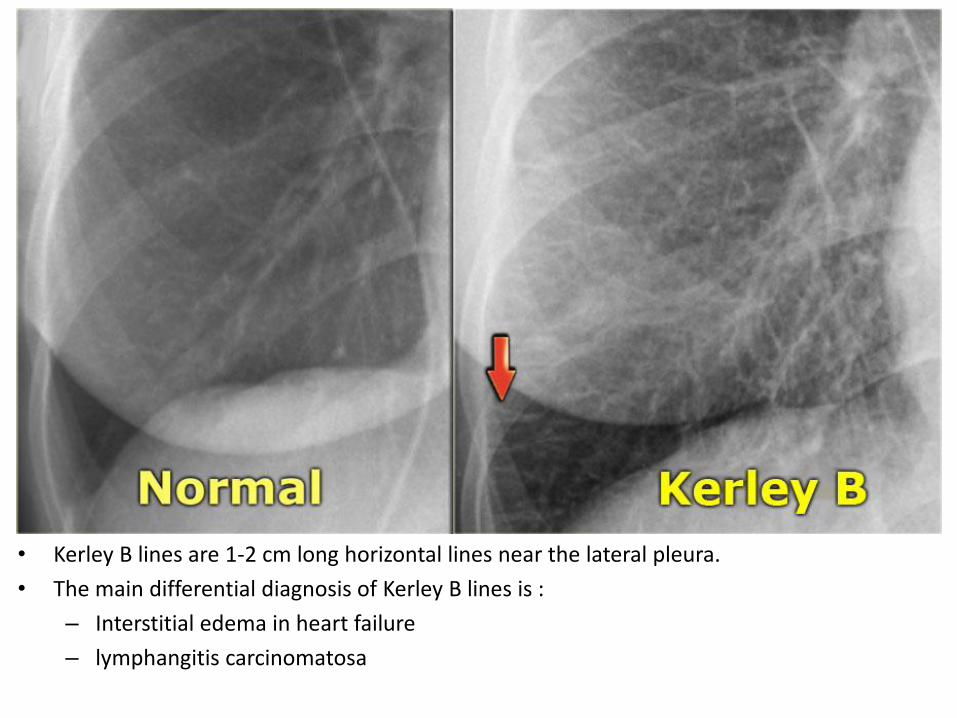
• Kerley B lines are 1-2 cm long horizontal lines near the lateral pleura.
• The main differential diagnosis of Kerley B lines is :
– Interstitial edema in heart failure
– lymphangitis carcinomatosa

2. NODULAR :

Adenocarcinoma
Solid white arrow : A mass is seen in the right upper lobe.
Solid black arrow : Its margin is slightly indistinct along the superolateral border.


Metastases to the lung
• A : Multiple discrete nodules of varying size are present throughout both lungs (solid white arrows).
• B : The interstitial markings in the right lung are prominent (solid white arrow), there are septal lines (dotted black arrow) and lymphadenopathy (solid black arrows) from lymphangitic spread of a bronchogenic carcinoma.
• C : In this case, the lung cancer has grown through the chest wall (solid white arrow) and invaded it by direct extension.


3. RETICULONODULAR :
Sarcoidosis

Sarcoidosis
Solid black arrow : Bilateral hilar.
Dotted black arrow : Right paratracheal adenopathy.
Blcak circle : In addition, the patient has diffuse, bilateral interstitial lung disease.

Membedakan konsolidasi dengan insterstitial
Always look at the peripheral margins of parenchymal lung disease to best determine the nature of the “packets” of abnormality and to help in differentiating airspace disease from interstitial disease. Solid black arrow : Notice how a portion of this disease appears confluent, like airspace disease. Black circle : At the periphery of this disease, this is more clearly seen to be reticular interstitial disease.

ATELECTASIS 1. Lobar atelectasis
2. Total atelectasis

• Atelectasis or lung-collapse is the result of loss of air in a lung or part of the lung with subsequent volume loss due to airway obstruction or compression of the lung by pleural fluid or a pneumothorax.

1. Lobar Atelectasis

• The most common causes of atelectasis are:
– Bronchial carcinoma in smokers
– Mucus plug in patients on mechanical ventilation or astmathics (ABPA)
– Malpositioned endotracheal tube
– Foreign body in children

a) Right upper lobe atelectasis


b) Right middle lobe atelectasis
• The findings are :
– Blurring of the right heart border (silhouette sign)
– Triangular density on the lateral view as a result of collapse of the middle lobe

c) Right lower lobe atelectasis
• Notice the abnormal right border of the heart. • The right interlobar artery is not visible, because it is not surrounded by aerated lung but by the collapsed
lower lobe. • Notice the reappearance of the right interlobar artery (red arrow) and the normal right heart border
(blue arrow).
Lower lobe atelectasis. Follow up

d) Left upper lobe atelectasis
• Minimal volume loss with elevation of the left diaphragm
• Abnormal left hilus, i.e. possible obstructing mass

e) Left lower lobe atelectasis
• There is a triangular density seen through the cardiac shadow.
• This is confirmed on the lateral view.
• We cannot see the lower lobe vessels, because they are surrounded by the atelectatic lobe.
• Normally when you follow the thoracic spine form top to bottom, the lower region becomes less opaque. (blue arrow).

2. Total atelectasis
The entire right hemithorax is opacified. The trachea has shifted toward the right (solid black arrow), and the heart is displaced toward the right as well (solid white arrow). Both of these mobile structures have moved toward the side of opacification.


1. Seorang anak perempuan datang dengan keluhan batuk berdahak sudah 1 minggu, disertai dengan sesak nafas. Pemeriksaan radiologi apa yang anda usulkan?
2. Dari hasil pemeriksaan tersebut, didapatkan hasil :
Apakah kelainan yang ditemukan pada foto tersebut?

3. Seorang laki-laki datang dengan sesak nafas sejak 2 jam yang lalu. Dada terasa tertekan, ekstermitas bengkak. Pada pemeriksaan TD 150/100mmHg. Dari hasil pemeriksaan tersebut, didapatkan hasil :
Apakah kelainan yang tampak pada foto tersebut?

4. Seorang laki-laki datang dengan sesak nafas. Pada pemeriksaan fisik, stem fremitus kanan dan kiri tidak sama kuat. Dilakukan pemeriksaan radiologi dan didapatkan hasil :
Apakah kelainan yang tampak pada foto tersebut?

5. Bagaimana terbentuknya konsolidasi?
6. Apakah yang dimaksud Silhouette sign?
7. Pasien laki-laki datang dengan keluhan batuk berdarah sudah 3 minggu. Pasien juga mengeluh dadanya sesak dan badannya lemas. Setelah dilakukan pemeriksaan radiologi, didapatkan hasil :
Apakah kelainan yang tampak pada foto tersebut?

8. Bagaimana cara menegakkan diagnosis pada foto tersebut?
9. Seorang laki-laki usia 60 tahun datang dengan keluhan batuk sejak 2 minggu yang lalu. Pasien memiliki riwayat merokok sejak usia 20 tahun. Hasil pemeriksaan radiologi didapatkan :
Apakah kelainan yang tampak pada foto tersebut?

10. Karena tidak mendapatkan pengobatan yang tepat, akhirnya pasien datang kembali dengan kondisi sakit berat, sesak nafas, dan badan lemas. Pemeriksaan radiologi didapatkan hasil :
Apakah kelainan yang tampak pada foto tersebut?


1. Foto x-ray thorax
2. Konsolidasi pada lobus media paru kanan.
3. Konsolidasi bilateral (diffuse).
4. Efusi pleura kanan. Sudut costophrenicus tumpul, diafragma datar.
5. Konsolidasi terbentuk akibat tergantinya isi alveolus dengan pus/air/darah/sel.
6. Silhouette sign adalah hilangnya bayangan organ yang normal.
7. Reticulonodular.
8. Melihat bagian perifer.
9. SPN
10. Atelektasis paru kanan dengan efusi pleura kanan