prairie view a&m university college of …€¦ · prairie view a&m university college of...
TRANSCRIPT
PRAIRIE VIEW A&M UNIVERSITY
COLLEGE OF NURSING
N4282 – ADULT HEALTH NURSING II PRACTICUM
CARE PLAN EVALUATION
NAME: DATE:
1. Demographic Data……………………………………………………………………………… (3)
A. History of present Illness
B. Chief Complaint
2. PATHOPHYSIOLGY TREE ………………………………………..………………………… (5)
Logical Flow
3. SYSTEMIC ASSESSMENT …………………………………………………………………..……(52)
A. Respiratory System(4)
B. Cardiovascular System (4)
C. Renal System (4)
D. Gastrointestinal System (4)
E. Neurologic System (4)
F. Integument & Immune system (4)
G. Nutrition & Metabolic System (4)
H. Pain & Comfort System (4)
I. Activity Mobility System (4)
J. Psychosocial/ Self Concept (4)
K. Teaching Learning Needs (3)
L. Discharge Planning (3)
M. Medication sheet (3)
N. Lab Data (3)
4. GOAL STATEMENTS ………………………………………………………………………...…… (9)
A. Derived from nursing diagnoses (3)
B. Goal/Outcome criteria measurable (3)
C. Time frame (3)
5. INTERVENTIONS …………………………………………………………………………………..(23)
A. Individualized/appropriate interventions (8)
B. Rationale for interventions (8)
C. Teaching Plan (5)
D. Reference for interventions/rationales (2)
6. EVALUATION ………………………………………………………………………………………(8)
A. Evaluates client’s response in relation to outcome criteria (4)
B. Overall statement in relation to goal (4)
GRADE NOTE: A grade of 75% or above is satisfactory.
FACULTY
Student’s Name: Date:
Patient Demographic Data
Age: Gender: Unit: Room/Bed:
Religious Preference: Marital Status: Ethnic Origin:
Date of Admission:
Admitting Diagnosis:
Secondary Diagnoses:
Chronic/Pre-existing Disorders:
Chief Complaint: Have the patient state in his/her own words why he/she came to the hospital.
History of present illness – from onset to present:
Referential sources must be cited – this includes but is not limited to drug books, care plan
books, lab books, other textbooks and any source you use to prepare this document.
Revised Fall 2010
Patient Health History
Asthma [ ] Angina [ ] Anemia [ ]
Emphysema [ ] MI [ ] Phlebitis [ ]
Bronchitis [ ] Hypertension [ ] Peripheral Vascular disease [ ]
Pneumonia [ ] Rheumatic Fever [ ] Blood dyscrasias [ ]
TB [ ] Congenital Heart Defects [ ] Blood loss [ ]
Pacemaker [ ] Stroke [ ]
Skin disease [ ] Bladder infections [ ] STD’s [ ]
Burns [ ] Kidney disease [ ] Alcoholism [ ]
Ulcer [ ] Diabetes [ ] Mental illness [ ]
Fractures [ ] Arthritis [ ] Depression [ ]
Dental problems [ ] Cancer [ ] Mental retardation [ ]
Others:
Surgeries (with dates and reason for surgery):
Home Medications
Prescription:
Over-the-counter:
Herbal:
Vital Signs: BP L - R - lying - sitting* - standing* -
*if appropriate
Heart Rate: Respiratory Rate: Temperature: route:
Allergy:
Laboratory and Other Diagnostic Tests
Please complete using the most recent results available. Indicate abnormal results with a red arrow up (high) or
down (low) next to the value. Please include results from other tests (x-rays, EKG, CT, MRI, EGD, scopes, etc.) on
an additional piece of paper. Interpret abnormal values on this blank page – individualize to YOUR patient.
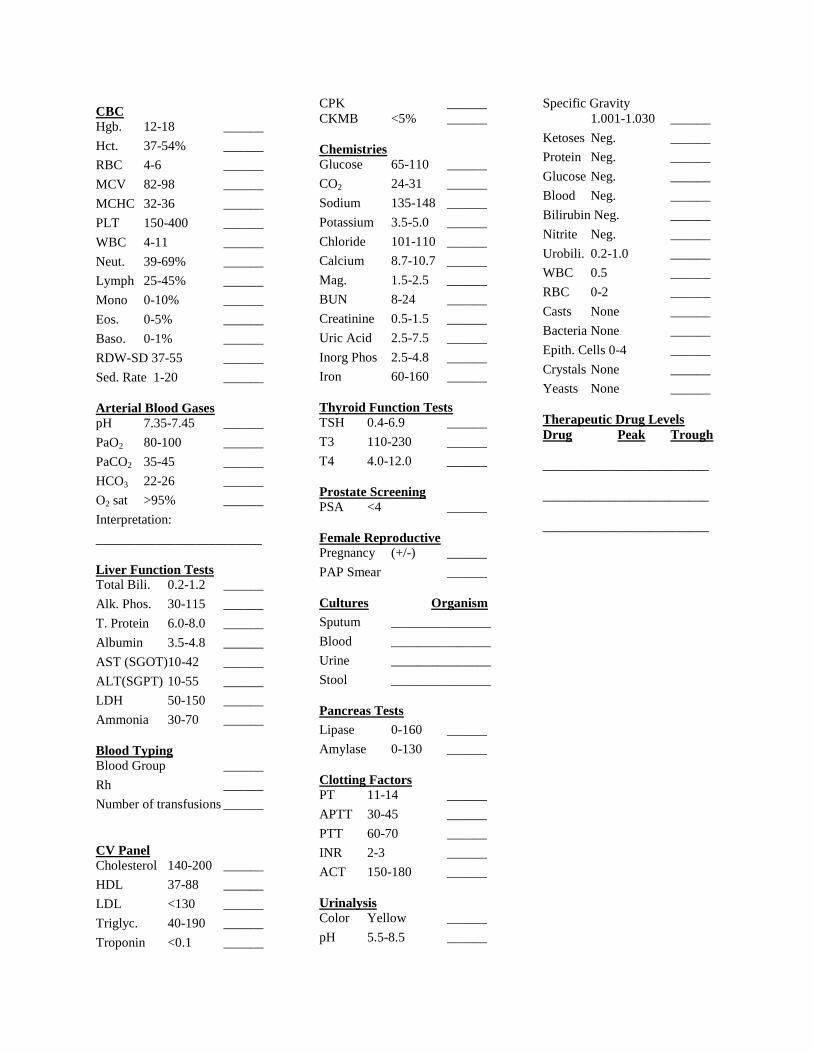
CBC
Hgb. 12-18 ______
Hct. 37-54% ______
RBC 4-6 ______
MCV 82-98 ______
MCHC 32-36 ______
PLT 150-400 ______
WBC 4-11 ______
Neut. 39-69% ______
Lymph 25-45% ______
Mono 0-10% ______
Eos. 0-5% ______
Baso. 0-1% ______
RDW-SD 37-55 ______
Sed. Rate 1-20 ______
Arterial Blood Gases
pH 7.35-7.45 ______
PaO2 80-100 ______
PaCO2 35-45 ______
HCO3 22-26 ______
O2 sat >95% ______
Interpretation:
_________________________
Liver Function Tests
Total Bili. 0.2-1.2 ______
Alk. Phos. 30-115 ______
T. Protein 6.0-8.0 ______
Albumin 3.5-4.8 ______
AST (SGOT)10-42 ______
ALT(SGPT) 10-55 ______
LDH 50-150 ______
Ammonia 30-70 ______
Blood Typing
Blood Group ______
Rh ______
Number of transfusions ______
CV Panel
Cholesterol 140-200 ______
HDL 37-88 ______
LDL <130 ______
Triglyc. 40-190 ______
Troponin <0.1 ______
CPK ______
CKMB <5% ______
Chemistries
Glucose 65-110 ______
CO2 24-31 ______
Sodium 135-148 ______
Potassium 3.5-5.0 ______
Chloride 101-110 ______
Calcium 8.7-10.7 ______
Mag. 1.5-2.5 ______
BUN 8-24 ______
Creatinine 0.5-1.5 ______
Uric Acid 2.5-7.5 ______
Inorg Phos 2.5-4.8 ______
Iron 60-160 ______
Thyroid Function Tests
TSH 0.4-6.9 ______
T3 110-230 ______
T4 4.0-12.0 ______
Prostate Screening PSA <4 ______
Female Reproductive Pregnancy (+/-) ______
PAP Smear ______
Cultures Organism
Sputum _______________
Blood _______________
Urine _______________
Stool _______________
Pancreas Tests
Lipase 0-160 ______
Amylase 0-130 ______
Clotting Factors
PT 11-14 ______
APTT 30-45 ______
PTT 60-70 ______
INR 2-3 ______
ACT 150-180 ______
Urinalysis
Color Yellow ______
pH 5.5-8.5 ______
Specific Gravity
1.001-1.030 ______
Ketoses Neg. ______
Protein Neg. ______
Glucose Neg. ______
Blood Neg. ______
Bilirubin Neg. ______
Nitrite Neg. ______
Urobili. 0.2-1.0 ______
WBC 0.5 ______
RBC 0-2 ______
Casts None ______
Bacteria None ______
Epith. Cells 0-4 ______
Crystals None ______
Yeasts None ______
Therapeutic Drug Levels
Drug Peak Trough
_________________________
_________________________
_________________________

Family Health History Key: M = mother; F = father; S = sibling; GP = grandparent; C = child
Asthma Angina Anemia
Emphysema MI Phlebitis
Bronchitis Peripheral vascular disease Hypertension
Pneumonia Rheumatic Fever Blood dyscrasias
TB Congenital Heart Defects Blood loss
Pacemaker Stroke
Skin disease Bladder infection STD’s
Burns Kidney disease Alcoholism
Ulcer Diabetes Mental illness
Fractures Arthritis Depression
Dental problems Cancer Mental retardation
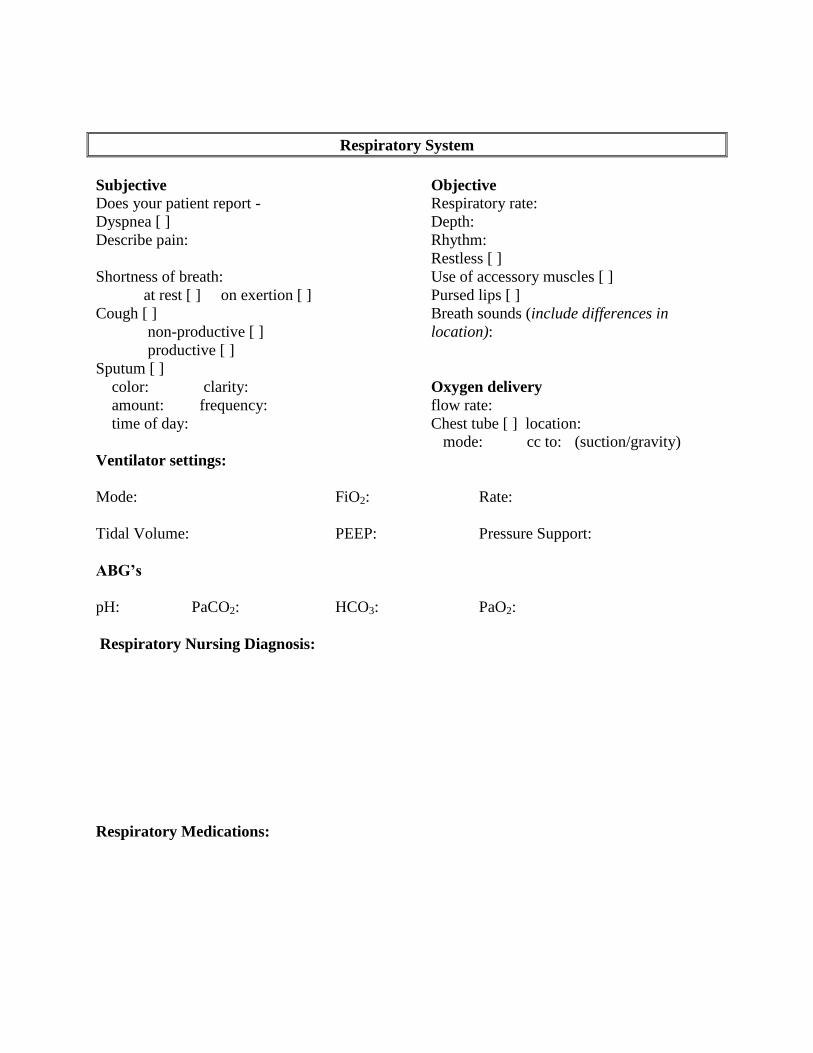
Respiratory System
Subjective Objective
Does your patient report - Respiratory rate:
Dyspnea [ ] Depth:
Describe pain: Rhythm:
Restless [ ]
Shortness of breath: Use of accessory muscles [ ]
at rest [ ] on exertion [ ] Pursed lips [ ]
Cough [ ] Breath sounds (include differences in
non-productive [ ] location):
productive [ ]
Sputum [ ]
color: clarity: Oxygen delivery
amount: frequency: flow rate:
time of day: Chest tube [ ] location:
mode: cc to: (suction/gravity)
Ventilator settings:
Mode: FiO2: Rate:
Tidal Volume: PEEP: Pressure Support:
ABG’s
pH: PaCO2: HCO3: PaO2:
Respiratory Nursing Diagnosis:
Respiratory Medications:

Cardiovascular/Peripheral Vascular System
Subjective Objective
Blood Pressure R - L -
Does your patient report - Apical heart rate: Rhythm:
Cardiac pattern:
Claudication [ ] Murmur:
Edema [ ] S3 [ ] S4 [ ]
location: Extremities:
time of day: Pulses (include grade)
Numbness - radial: pedal:
location: posterior tibial:
precipitating event Capillary refill:
Edema(include grade)
location/grade/ description
Color:
Pale [ ] Jaundice [ ]
Central cyanosis [ ] Peripheral cyanosis [ ]
Hemodynamic Monitoring Clubbing [ ]
Location of PMI:
PA catheter [ ]
PAP: PWP:
CO:
Arterial line [ ]
Location:
Cardiac Nursing Diagnosis:
Cardiac Medications:
Renal System

Subjective Objective
Does your patient report - Bladder
Distended [ ] Non-distended [ ]
Incontinence [ ] Intake for last 24 hours:
Stress Incontinence [ ] Output for last 24 hours:
When does it occur? Positive/negative balance:
Urgency [ ] Frequency [ ] Catheter [ ]
Retention [ ] Enuresis [ ] Type:
Pain / burning [ ] Urine color: clarity:
Urine color: Clarity: Continent [ ] Incontinent [ ]
Renal Nursing Diagnosis:
Renal Medication:
Gastrointestinal System
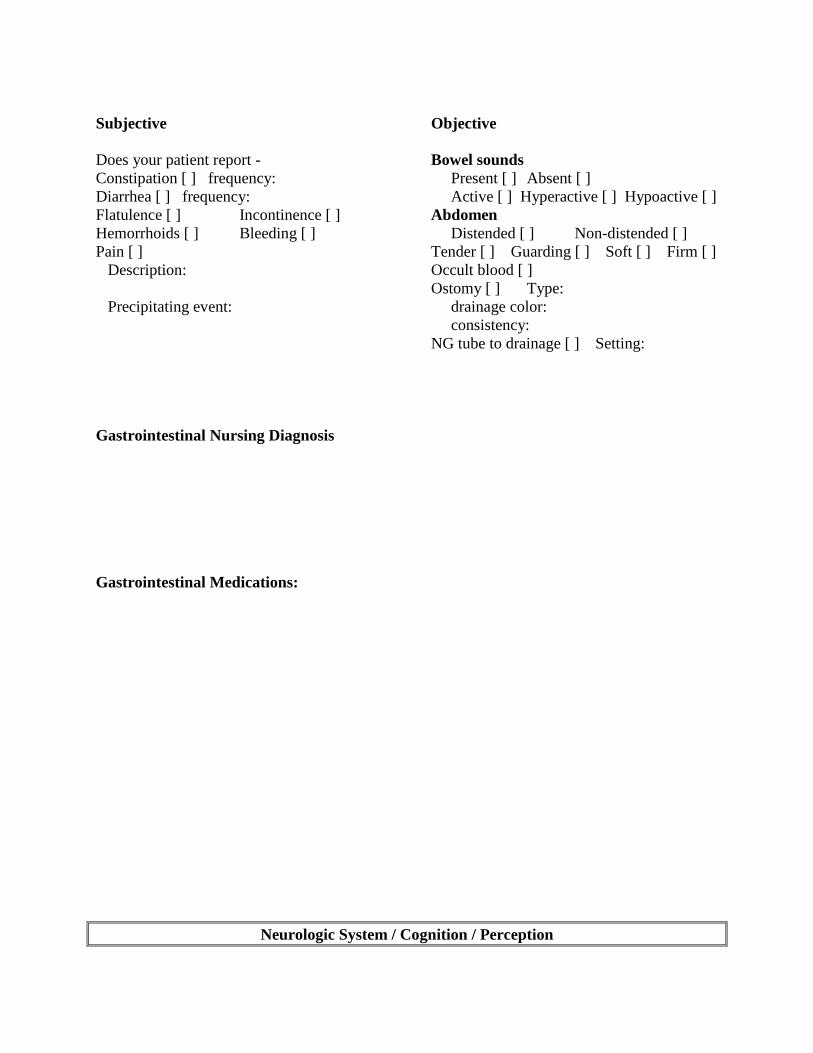
Subjective Objective
Does your patient report - Bowel sounds
Constipation [ ] frequency: Present [ ] Absent [ ]
Diarrhea [ ] frequency: Active [ ] Hyperactive [ ] Hypoactive [ ]
Flatulence [ ] Incontinence [ ] Abdomen
Hemorrhoids [ ] Bleeding [ ] Distended [ ] Non-distended [ ]
Pain [ ] Tender [ ] Guarding [ ] Soft [ ] Firm [ ]
Description: Occult blood [ ]
Ostomy [ ] Type:
Precipitating event: drainage color:
consistency:
NG tube to drainage [ ] Setting:
Gastrointestinal Nursing Diagnosis
Gastrointestinal Medications:
Neurologic System / Cognition / Perception

Subjective Objective
Does your patient report - Orientation
Headaches [ ] Type: Time [ ] Place [ ] Person [ ]
Frequency: Level of consciousness
Precipitating event: Alert [] Drowsy [ ] Confused [ ]
Impaired vision [ ] Glasses [ ] Lethargic [ ] Glasgow coma scale:
Vertigo [ ] Syncope [ ] Memory: Recent [ ] Remote [ ]
Numbness [ ] Location: Pupils (size, symmetry) OD: OS:
Precipitating event: Communication
Tingling [ ] Location: Primary language:
Weakness [ ] Location: speaks [ ] reads [ ] writes [ ]
Paraplegia [ ] Cause: English:
Tetraplegia [ ] Cause: speaks [ ] reads [ ] writes [ ]
Speech impairment [ ]
describe:
Neurologic Nursing Diagnosis
Neurologic Medications:

Protective Function – Integument & Immune System
Subjective Objective
Bruises:
Does your patient report - Describe(location, color, size)___________
Pruritus [ ] ___________________________________
Location:
Lesions [ ] Wounds:
Describe(location, color, size): Describe(location, color, size):
Rash [ ] Pressure sores:
Describe(location, color, size): Describe(location, color, size):
Allergies [ ] Other lesions:
Describe (including reaction): Describe(location, color, size):
Mucous membranes:
Moist [ ] Dry [ ]
Pale [ ] Normal for patient [ ]
Body temperature:
Route:
Protective Function Nursing Diagnosis
Protective Function Medications:
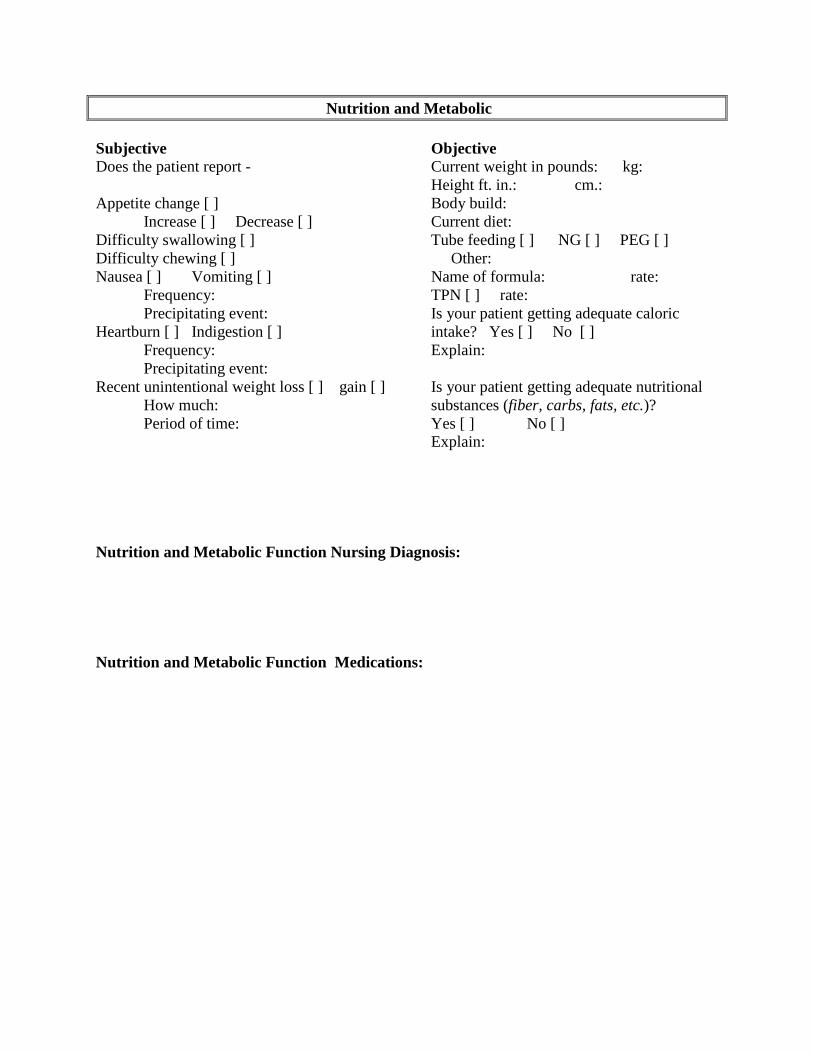
Nutrition and Metabolic
Subjective Objective
Does the patient report - Current weight in pounds: kg:
Height ft. in.: cm.:
Appetite change [ ] Body build:
Increase [ ] Decrease [ ] Current diet:
Difficulty swallowing [ ] Tube feeding [ ] NG [ ] PEG [ ]
Difficulty chewing [ ] Other:
Nausea [ ] Vomiting [ ] Name of formula: rate:
Frequency: TPN [ ] rate:
Precipitating event: Is your patient getting adequate caloric
Heartburn [ ] Indigestion [ ] intake? Yes [ ] No [ ]
Frequency: Explain:
Precipitating event:
Recent unintentional weight loss [ ] gain [ ] Is your patient getting adequate nutritional
How much: substances (fiber, carbs, fats, etc.)?
Period of time: Yes [ ] No [ ]
Explain:
Nutrition and Metabolic Function Nursing Diagnosis:
Nutrition and Metabolic Function Medications:

Pain and Comfort
Subjective Objective
Does your patient report - Facial grimacing Yes [ ] No [ ]
Pain Yes [ ] No [ ] Emotional response Yes [ ] No [ ]
Location: Does pain limit activities? Yes [ ] No [ ]
Describe:
Intensity (0 – 10): Guarding Yes [ ] No [ ]
Descriptors: How often does the patient request or
receive pain medication?
Precipitating event:
Does the pain medication “hold”
Relieved by: patient’s pain until the next dose is due?
Yes [ ] No [ ]
Pain and Comfort Nursing Diagnosis:
Pain and Comfort Medications:

Activity / Mobility
Subjective Objective
Does your patient report - Amputation Yes [ ] No [ ]
Fatigue [ ] Boredom [ ] Limb:
Irritability [ ] Insomnia [ ] Fractures Yes [ ] No [ ]
Needs assistance with: Location:
Bathing [ ] Dressing [ ]
Feeding [ ] Toileting [ ] Gait: good balance [ ] poor balance [ ]
Oral hygiene [ ] Turning [ ] bed rest [ ] limp [ ]
Ambulation [ ] Muscle strength (grade)
Sleep pattern: Legs R: L:
hours/night: Arms R: L:
# of times up to bathroom: Shoulders R: L:
daytime naps: Neck:
Other: Head:
ROM full [ ] limited [ ] weakness [ ]
describe:
Does your patient feel rested after a night’s
sleep? Yes [ ] No [ ] Current aids: Cane [ ] Crutches [ ] Brace [ ]
Sleep apnea? Yes [ ] No [ ] Walker [ ] Wheelchair [ ] Trapeze [ ]
Splint [ ] Prosthesis [ ]
Activity/ Mobility Nursing Diagnosis:
Activity/ Mobility Medications:
Psychosocial / Self-Concept
Subjective Objective
Does your patient report - Presenting appearance:
Smoker Yes [ ] No [ ]
How much (ppd):
How long (age began):
Want to stop Yes [ ] No [ ] Cues to self-concept:
Alcohol consumption Yes [ ] No [ ] Makes eye contact Yes [ ] No [ ]
How much: If no, does client belong to an ethnic group
How often: that considers eye contact inappropriate?
Recreational drugs Yes [ ] No [ ] Yes [ ] No [ ]
Drug(s) of choice: Repetitive actions (i.e. twisting hands)
How often: Other cues to self-concept:
Date of last use:
Cage-Aid Emotional status:
•Have you felt you ought to cut down on Calm [ ] Anxious [ ] Angry [ ]
your drinking or drug use? Fearful [ ] Withdrawn [ ] Irritable [ ]
•Have people annoyed you by criticizing Euphoric [ ] Depressed [ ]
your drinking or drug use? Give objective data to support this your
•Have you felt bad or guilty about your assessment of the patient’s emotional status:
drinking or drug use?
•Have you ever had a drink or used drugs
in the morning (eye-opener) to steady
your nerves, or get rid of a hangover,
or get the day started?
Recent stressors (subjective):
Job loss [ ] Job change [ ] Retirement [ ] Marriage [ ] Divorce/separation [ ]
Death of significant other [ ] Who?
Circumstances:
How do you handle stress?
Who do you share your problems with?
Religious beliefs and practices that may effect health care:
Ethnic beliefs and practices that may effect health care:
Psychosocial Nursing Diagnosis:
Psychosocial Medications:
Teaching / Learning Needs
Knowledge / perception of current situation:
Expectations of treatment:
Factors affecting ability to learn - Age: Gender:
Highest level of education completed:
Developmental stage (i.e. Erickson):
How does your patient learn best? Audio [ ] Visual [ ] Kinesthetic [ ]
What type of experience has your patient had with learning/education (i.e. successful, frustrating,
etc.)?
Knowledge Deficit Diagnosi:

Discharge Planning
Anticipated date of discharge:
Type of work/employment prior to hospitalization:
Anticipated changes in ability to continue current type of work:
Financial considerations
Private insurance [ ] Public assistance [ ] Third party responsibility [ ]
Disability insurance [ ] Available sick leave [ ]
Financial resources available to client through referral:
Living/home considerations
Who does the patient currently live with?
Does the client have a multi-level home or apartment? Yes [ ] No [ ]
Will the client need assistance with any of the following upon discharge?
Food preparation [ ] Shopping [ ]
Ambulation [ ] Transportation [ ]
Medication [ ] Wound care [ ] Other treatments [ ]
Personal hygiene [ ]
Other:
Resources
Family or significant others who can stay with him/her or attend to him/her daily?
Resources for professional home health assistance:
Physical: Will the patient need home alterations (i.e. ramp, tub handle, etc.)?
Are resources available for these items?

Pathophysiology Tree of Major Health Problems
Include admitting medical diagnosis/diagnoses.
Medications
DRUG: Generic Trade
Route Dosage Time
Indications for use
Reason drug was prescribed for this client
Side effects
Nursing implications
Describe action in layman’s terms (client/family teaching)
DRUG: Generic Trade
Route Dosage Time
Indications for use
Reason drug was prescribed for this client
Side effects
Nursing implications
Describe action in layman’s terms (client/family teaching)
NURSING DIAGNOSES*
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
*Be sure to include problem, etiology, and manifestation. This is to be a PRIORITIZED list.

Nursing Diagnoses
Nursing Diagnosis Human Response R/T Etiology
Goals/
Outcome Criteria
Interventions Specific & Individualized
Rationales
with references
Evaluation Did the patient achieve the
goal?
Teaching Plan
Knowledge Based
Nursing Diagnosis
Teaching / Learning
Goals & Objectives
Content Method Evaluation Did the patient / s.o. achieve
the goals/objectives? How?
