selection of anti-egfr antibodies in the treatment of mcrc (abstracts # 3510 and 3511) tanios...
TRANSCRIPT
Selection of Anti-EGFR Antibodies in the Treatment of MCRC (Abstracts # 3510 and 3511)
Tanios Bekaii-Saab, MDThe Ohio State University Comprehensive Cancer Center
Arthur James Cancer Hospital and Solove Research Institute

Potential Conflicts
• Research Grants– NCI/CTEP– Oncolytics Inc– Genentech– Roche– Pfizer– ENZON
• Consultant/Speaker– BMS– Amgen– Genentech– Lilly– Onyx– Array Biopharma
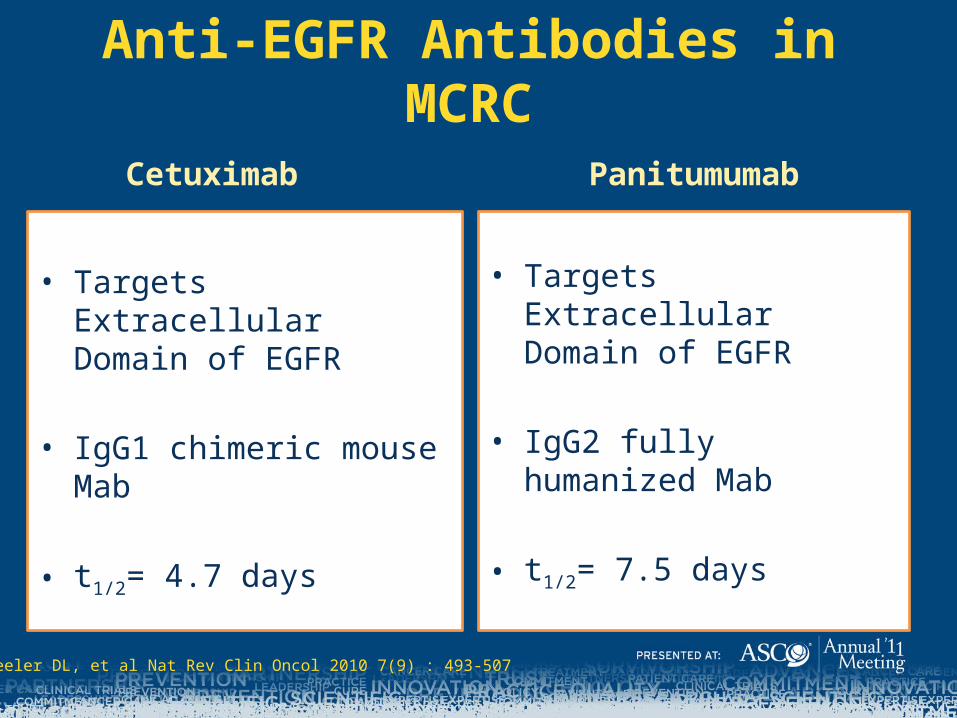
Anti-EGFR Antibodies in MCRC
Cetuximab
• Targets Extracellular Domain of EGFR
• IgG1 chimeric mouse Mab
• t1/2= 4.7 days
Panitumumab
• Targets Extracellular Domain of EGFR
• IgG2 fully humanized Mab
• t1/2= 7.5 days
Wheeler DL, et al Nat Rev Clin Oncol 2010 7(9) : 493-507

WT KRAS MT KRAS
EGFR
ANTI-EGFR ANTIBODY
Bekaii-Saab, T . Adapted from multiple sources: 1- Wheeler DL, et al Nat Rev Clin Oncol 2010 7(9) : 493-507;2- De Roock et al . Lancet Oncology, 2010 11: 753-762; 3- Frattini M , BJC 2007 97; 1139-1145; 4- Di Nicolantonio F et al . Journal of Clin Oncol 2008 26(35); 5705-5712; 5- Loupakis F et al. BJC 2009 101;715-721;
Anti-EGFR Antibodies and KRAS mutations
Codon 12
Codon 13
Codons 61,146 ,others
79%
18%
3%
?MT BRAF 5-10%
Others
~40%

KRAS status as a determinant of response to anti-EGFR antibodies
• Initial retrospective analyses of MCRC trials suggested that patients with KRAS-mutated (MT) tumors will not benefit from EGFR inhibitors
• Health Authorities in the US and EU recently indicated that patients with KRAS codon 12 or 13 MT tumors are not candidates for cetuximab or panitumumab
Allegra et al. J Clin Oncol. 2009;27(12):2091-2096De Rook et al. JAMA. 2010;304(16): 1812-1820
Anti-EGFR antibodies in First Line Treatment of MCRC
• The first introduction of anti-EGFR antibodies to the treatment of MCRC were in the more refractory setting where they became part of the standard of care.
• More recently, a number of prospective phase III randomized studies evaluated the role of adding anti-EGFR antibodies to chemotherapy in the first line treatment of MCRC.
Wheeler DL, et al Nat Rev Clin Oncol 2010 7(9)

Chemotherapy Regimens Containing Anti-EGFR Antibodies in First Line Treatment of mCRC From Phase III Studies
7
Trial
Cetuximab Panitumumab
CRYSTAL1
(KRAS WT)(N=350 vs 316)
COIN2
(KRAS WT)(N=367 vs 362)
NORDIC VII3
(KRAS WT)(N=185 vs 194)
PRIME 2034
(KRAS WT)(N=590 vs 593)
Treatment FOLFIRI FOLFIRI + Cetuximab
FOLF/XEL/OX
FOLF/XEL/OX +
Cetuximab
Cont.5-FU/FA/Ox
Cont.5FU/FA/Ox + Cetuximab
FOLFOX FOLFOX + Panitumumab
OS (mos)P valueHR
20.0 23.50.0093
0.80
17.9 17.00.60
1.038
22.0 20.1 0.661.14
19.7 23.90.170.88
PFS (mos) P valueHR
8.4 9.9 0.0012
0.70
8.6 8.60.60
0.959
8.7 7.9 0.661.07
8.6 10 0.010.80
ORR, %
P value
39.7 57.3
<0.001
57 64
0.049
47 46
0.87
48 57
0.02
1. Van Cutsem, et al. J Clin Oncol 2011 2915) pp 2011-2019. 2. Maughan, et al. J Clin Oncol. 2010;28:15s(suppl; abstr 3502). 3. Tveit, et al. ASCO GI. 2011 (abstr 365). 4. Douillard, et al. ASCO 2011 ( abstr 3510).

Q: How to Shape the Landscape of First Line Treatment of mCRC?
A: Follow the data.
Not That Simple !
• Biologics play a prominent role in the first line treatment of mCRC when added to chemotherapy.
• Which biologic?– Today’s standard is Bevacizumab ( at least in the
US) for most patients – EGFRI vs. VEGFI
• Comparative Data needed for EGFRI vs. VEGFI including in the subgroup of patients with disease confined to the liver
• CALGB/SWOG 80405 • We are lacking predictors for VEGFI while treatment with
EGFRI seems to be getting better refined.
Selection of Biologics in First Line Treatment of Patients with KRAS WT mCRC

Selection of Anti-EGFR Antibodies in First Line Treatment of Patients with KRAS WT mCRC
• In first line treatment, results of PIII studies suggest that panitumumab synergizes with FOLFOX whereby cetuximab may not? – Differences between antibodies? Differential synergism with the 2
antibodies? – Study design/schedule issues?
• Both anti-EGFR antibodies seem to exert a more consistent differential synergism with irinotecan based regimens vs. oxaliplatin ones across lines of therapy ( CRYSTAL , 181, BOND… )– In KRAS MT CRC, both anti-EGFR antibodies exert a negative
interaction with oxaliplatin but not with irinotecan.– Implications on future metastatic studies Chemotherapy backbone
matters!– Implications on adjuvant studies?

• Primary endpoint: DFS• Secondary endpoints: OS, safety
NO147: Adjuvant mFOLFOX6/FOLFIRI ± Cetuximab (KRAS WT and Mutant, Resected
Stage III Colon Cancer)
mFOLFOX6(n=902)
REGISTER
mFOLFOX6 + cetuximab(n=945)
• Adjuvant therapy per primary oncologist
• Report therapy given• Annual status through
year 8
Stage III colon cancer
(N=3768: FOLFOX/Cet)
(N=146: FOLFIRI/Cet)
PREREGISTER KRAS mutant
KRAS WT
Centralized KRAS analysis
FOLFIRI (12 cycles)(n=106)
FOLFIRI + cetuximab (12 cycles)
(n=40)
RANDOMIZE
Huang, et al. ASCO GI. 2011 (abstr 363).
X

% A
live
100
90
80
70
60
50
40
30
20
10
0
Time, Months
0 12 24 36 48 60 72
% A
live
and
Dis
ease
Fre
e
100
90
80
70
60
50
40
30
20
10
0
Time, Months
0 12 24 36 48 60
Arm3-Year Rates, %
(95% CI)HR
(95% CI)P Value
FOLFIRI (N=69)
69.8 (60-82)
0.31 (0.09-1.03)
0.04FOLFIRI + cetuximab (N=26)
92.3 (83-100)
Arm3-Year Rates, %
(95% CI)HR
(95% CI)P Value
FOLFIRI (N=69)
85.2 (77-94)
0.34 (0.08-1.48)
0.13FOLFIRI + cetuximab (N=26)
92.0 (82-100)
NO147 FOLFIRI ± Cetuximab in KRAS WT Patients with Stage III Colon Cancer :
Disease-Free Survival(n=95)
FOLFIRI
FOLFIRI + cetuximab
FOLFIRI
FOLFIRI + cetuximab
Overall Survival(n=95)
Huang, et al. ASCO GI. 2011 (abstr 363).
A Missed Opportunity?
Selection of Anti-EGFR Antibodies: Are all KRAS Mutations in Colorectal Cancer Created Equal ?

Association of Various KRAS Mutations with Outcome in Patients with Colorectal Cancer
Andreyev HJN. BJC: 2001 ; 85(5), 692-696

Association of Various KRAS Mutations with Outcome in Patients with Chemorefractory Colorectal Cancer treated with Cetuximab
Copyright restrictions may apply.
De Roock, W. et al. JAMA 2010;304:1812-1820

In Vitro and In Vivo Effects of the p.G13D MutationEffect of Cetuximab on Cellular Proliferation in Isogenic Cell Lines Proliferation Assay on Isogenic Cell lines
Effect of Cetuximab on Growth of Tumor
De Roock, W. et al. JAMA 2010;304: e-suppl.
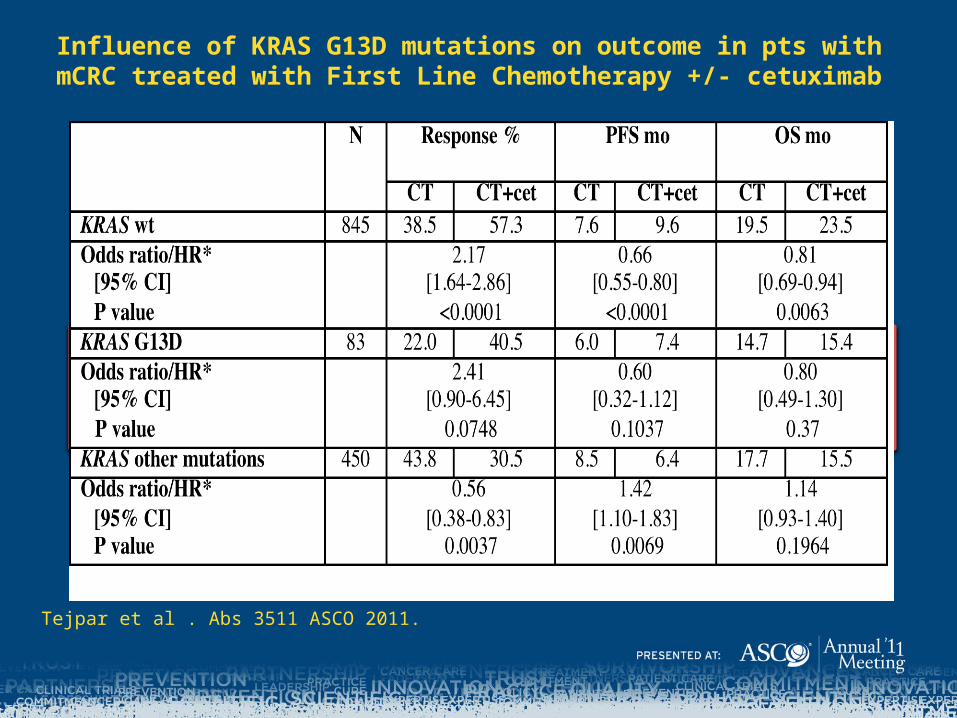
Influence of KRAS G13D mutations on outcome in pts with mCRC treated with First Line Chemotherapy +/- cetuximab
Tejpar et al . Abs 3511 ASCO 2011.

CRYSTAL : OS for patients with KRAS WT disease according to tumor BRAF mutation status.
Van Cutsem E et al. JCO 2011;29:2011-2019
©2011 by American Society of Clinical Oncology
No. of Events
Median OS
[95% CI]
WT
(n=350)
288
20.0
[17.4-21.7]
MT G13D
(n=29)
23
15.8
[12.4-20.0]
MT G12V
(n=40)
37
18.0
[14.0-21.7]
MT Other
(n=114)
96
16.3
[14.7-20.1]
At Risk
WT
MT G13D
MT G12V
MT Other
350 311 246 179 132 92 64 48 18 2 0
29 25 17 10 5 3 2 1 0 0 0
40 39 28 20 12 9 8 5 0 0 0
114 100 82 47 33 26 18 11 2 1 0
CRYSTAL: KRAS evaluable population - ChemoOverall Survival Time
P:\Drugs\Erbitux\EMR_062202\Project_tasks\ASCO_2011\Output\crystal_OS_kras3_4_thicker_chemo.emf, 17MAY11
KRAS WildtypeKRAS Mutation G13DKRAS Mutation G12VKRAS Other Mutations
Kapl
an-M
eier
Est
imat
e
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Overall Survival Time (months)
0 6 12 18 24 30 36 42 48 54 60
Tejpar et al . Abs 3511 ASCO 2011.
KRAS G13D and BRAF mutations are prognostic in MCRC
CRYSTAL (FOLFIRI Only): OS for patients according to tumor KRAS mutation status.
WT KRAS MT KRAS
EGFR
ANTI-EGFR ANTIBODY
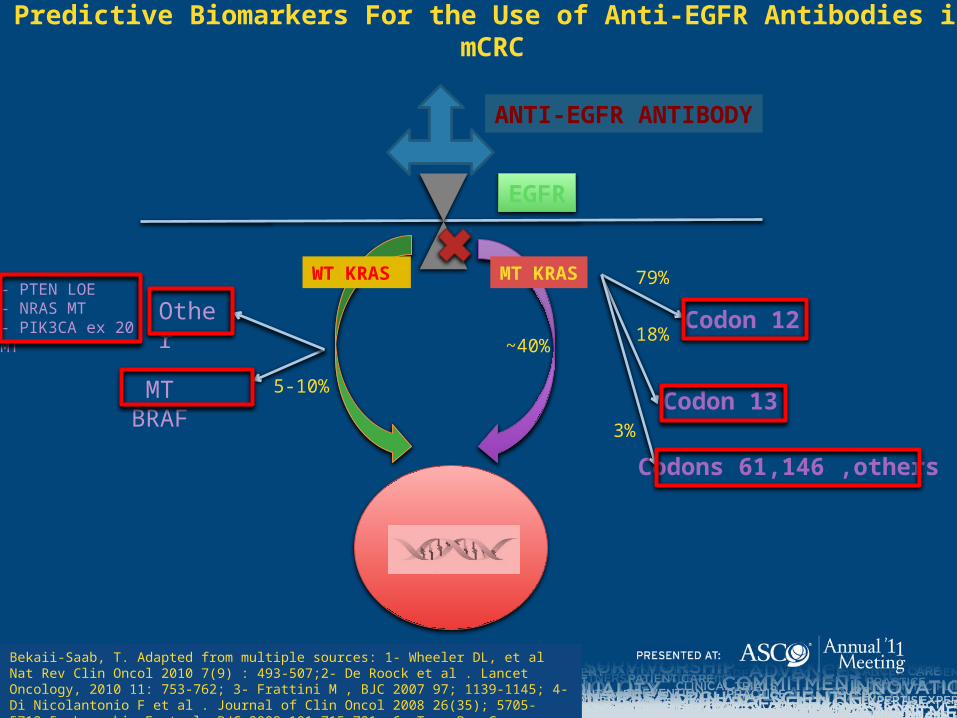
Predictive Biomarkers For the Use of Anti-EGFR Antibodies in mCRC
Codon 12
Codon 13
Codons 61,146 ,others
79%
18%
3%
MT BRAF 5-10%
Other- PTEN LOE- NRAS MT- PIK3CA ex 20 MT
~40%
Bekaii-Saab, T. Adapted from multiple sources: 1- Wheeler DL, et al Nat Rev Clin Oncol 2010 7(9) : 493-507;2- De Roock et al . Lancet Oncology, 2010 11: 753-762; 3- Frattini M , BJC 2007 97; 1139-1145; 4- Di Nicolantonio F et al . Journal of Clin Oncol 2008 26(35); 5705-5712;5- Loupakis F et al. BJC 2009 101;715-721; 6- Tran B . Cancer 2011 ; 1-10.

The EGFR Signaling Network is Large and Complex

Complex Genetic structures in subsets of CRC
• Kras variant sub-populations in WT groups
• KRAS MT are not associated with a single homogenous gene expression patterns
• BRAF MT have a characteristic gene expression pattern defined by MS status.
Tejpar , S et al . ASCO 2010 Abs 3505
Gene Gene name PathwayFold
change P.AdjAQP5 Aquaporin 5 target of ESR1; promotes proliferation
and inhibits apoptosis in chronic myelogenous leukemia; interacts with the MAPK and Rb pathway
5,5 9,7E-21
CTSE cathepsin E is found in highest concentration in the surface of epithelial mucus-producing cells of the stomach. Found in more than half of gastric cancers.
4,8 5,43E-11
SOX8
SRY (sex determining region Y)-box 8
Wnt/beta-catenin signaling 2,6 0,000217
REG4
regenerating islet-derived family, member 4 activator of the EGFR in CRC, involved in gastric and
pancreatic cancers 3,7 1,68E-07
PIWIL1
piwi-like 1intrinsic regulator of the self-renewal capacity of germline and hematopoietic stem cells. 2,5 9,43E-05
AXIN2 Axin 2 Wnt/beta-catenin signaling -2,1 5,65E-06CDX2 caudal type homeobox 2 -2,3 1,16E-10
HSF5 heat shock transcription factor family member 5
-3,1 5,79E-10
TFCP2L1 transcription factor CP2-like 1
-2,3 4,5E-08
GGH gamma-glutamyl hydrolase associated with CIMP+ in colon cancer -3,0 8,54E-08
RNF43 ring finger protein 43 ubiquitin ligase that promotes cell growth and is upregulated in colon cancer
-2,2 1,35E-07
PTPRO
protein tyrosine phosphatase, receptor type,
O
Growth-suppressor; epithelial adherens junctions -3,2 5,65E-06
SPINK1
serine peptidase inhibitor, Kazal type 1
interacting with CTSB -2,9 9,73E-06
SATB2 SATB homeobox 2 promotes growth and metastasis in breast cancer -2,5 1,17E-05
DPEP1 -2,4 2,76E-05
TNNC2 -2,2 9,21E-05
PCLO -2,5 0,00017

Conclusions and Future Directions
• KRAS G13D and BRAF mutations likely have an adverse prognostic effect in mCRC– Modest benefit with the addition of anti-EGFR antibodies– Cost/Benefit question may be difficult to address in a randomized trial– Prospective validation of results is needed– Future studies with anti-EGFR antibodies should include and stratify for
KRAS G13D and BRAF mutations
• KRAS G12 mutation is predictive of lack of response to anti-EGFR antibodies– KRAS G12V likely has no prognostic value in mCRC
• It is likely that complex genetic structures exist in subsets of CRC.– Therapeutic Implications

Take Home Messages For Everyday Clinical Practice
• Anti-EGFR antibodies improve the efficacy of chemotherapy in the first line treatment of patients with KRAS WT mCRC.– There still is a need identify possible superiority of one biologic
vs. the other (EGFRI vs. VEFGI) including in mCRC confined to the liver.
• Outside the confines of a clinical study, testing for KRAS G13D, BRAF and other mutations other than KRAS 12 is not recommended given the questionable lack of their predictive value for the use of Anti-EGFR antibodies in mCRC– Prospective validation including cost-benefit analysis needs
evaluated.