slides process modelling bergen 2012
DESCRIPTION
Slides of our paper "Process modelling and Public Values" presented in Bergen 2012TRANSCRIPT

Claude ROCHET, Bruno TIBERGHIEN, Anaïs SAINT, Aix-Marseille Université, CERGAM, IMPGT
Philippe AGOPIAN, Catherine PARIS-LAPORTE, Valery SOULLEIHET, SDIS 13
! The framework: Streamlining and monitoring the processes using BPMN approach, applied to an emergency service
! The case: : optimizing the cerebrovascular accident (CVA) channel services’ coordination in the Bouches du Rhône
! The actors: the Fire department (SDIS) and the medical emergency service (SAMU) coordinate their processes with hospitals
2
! Three operational steps : " We first have to produce the global modelling of
the channel (processes, sub processes and procedures) according to the BPMN rules.
" Then we will choose and drag out the relevant indicators
" These indicators will permit us to build up the balanced scorecard
3
! Then three vision levels of the process : " COST:
What is the cost of this rescue channel compared to a classical one?
" MANAGEMENT: What are the impacts of this process on the Fire
department budget? What kind of organizational change is required? How to join up public services that have been split in silos?
" IMPACT & EXTERNALITIES: What are the costs saved for the health care system?
What are the quality of life of the relieved patient? How to evaluate the pertinence of such an approach?
4

! WHY A PROCESS MODELING?
" To save people of paralysis for life (20% of CVA are eligible to a thrombolysis)
" To highlight the benefits of the channel for society (costs/benefits)
" To understand the role of the information system in organizational innovation in this public service
5

" Average age is 73 " Third cause of adult death " Around 150.000 strokes per year in France " We expect this number to raise because of the
ageing of the population
! Also called stroke, a cerebrovascular accident (CVA) is a disturbance in the blood supply to the brain. Without treatment, the patient will suffer non-reversible diseases as severe paralysis.
-> It is a public health issue
6

! The lack of an appropriate treatment has for years made room for a « contemplative and wait-and-see attitude » (Canault et al., 2005)
! Nowadays, we have discovered a treatment: a thrombolysis can dissolve a blood clot (detected by MRI) in the brain if it is applied in the four hours following the first symptoms: " Paralysis on one side of the body, aphasia, legs
which steal/fall, paralysis on one side of the face, headaches.
7

! Because of this particular and frequent pathology, health care system actors need to coordinate in a way that anyone on the territory can reach a thrombolysis within four hours if necessary.
! Each universitary hospital center is supposed to have a stroke center. In the Bouches du Rhône, it is located in Marseille (la Timone)… " In this stroke center, an MRI and a neurologist
will always be available to practice a thrombolysis
8

! … But several actors: SAMU, the firemen and their first responders, the hospital and the stroke center.
! So there is a need to coordinate all the actors and monitor the whole channel in real time: that’s why we need the process modeling and the BSC!
9

! According to the French Neurovascular Society (2001): " the organization of stroke units avoids 1 death or
disability for 20 patients treated (120 deaths or disabilities avoided per year).
" The benefits due to such units is not based on the action of a drug, but on the effectiveness of an interactive multidisciplinary team.
! The economic aspect of stroke management can be measured through the average length of hospital : " The specialized units enable a reduction in length of
stay of almost 8% (0,3 days) (Hommel et al., 1999). " A Cochrane meta-analysis revealed that for every 100
patients treated in a stroke unit, there is a reduction of 26 days (Bowen & Yaste, 1994).
10
! But the expected economic impact of the development of stroke units is insufficiently studied in the literature.
! The public health challenge is to implement a rational therapeutic strategy as early as possible coordinating the different actors of the chain. If there is an added cost, it appears justified by the clinical benefits observed (Launois et al., 2002).
! Despite a s ign i f icant increase in the implementation of stroke units in France, we observe a lag between the recommendations adopted by the government and the reality.
11
! The prime functions of an information system: " To provide a unique standard of data for all the
actors involved in the channel (Rochet et al., 2011): that way every process could be standardized and useable by every actor
" To inform people with reliable data (required for our BSC). (Elidrissi & Elidrissi, 2010)
! The Business Process Modeling (BPM) approach: represents the processes of an organization to be able to analyze the global system, which allows us to work on different levels of granularity (Rochet, 2010).
12
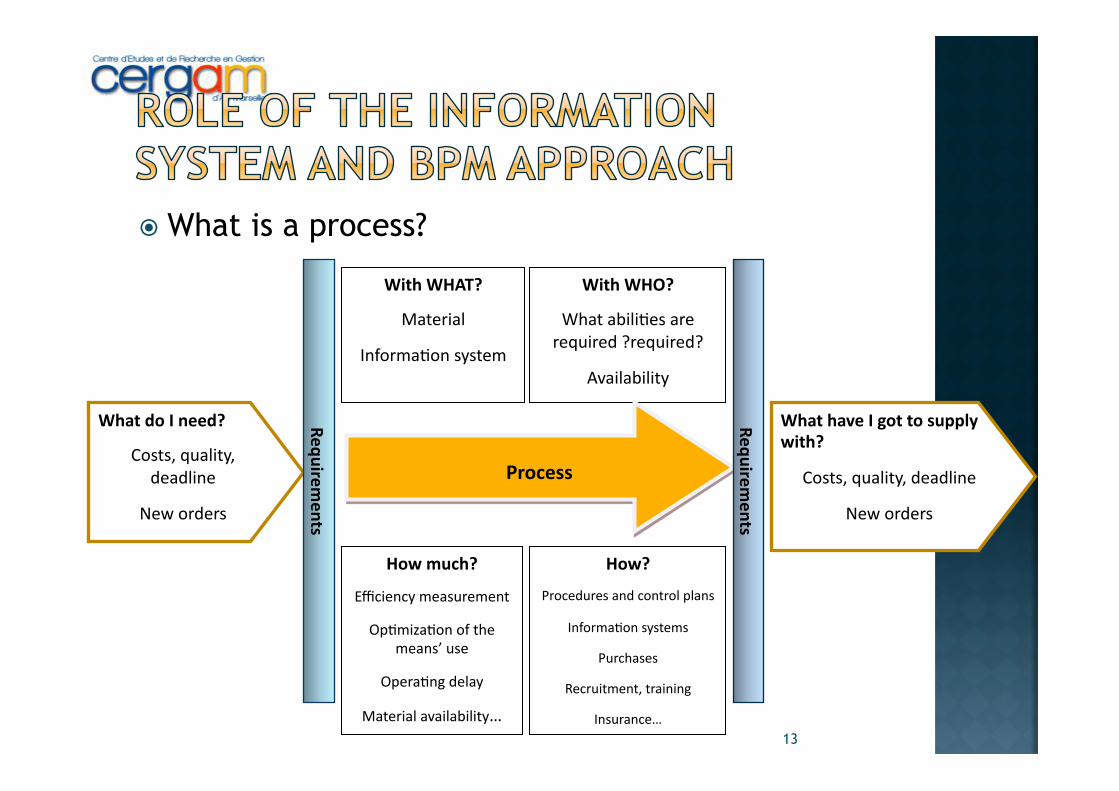
! What is a process?
13
What%do%I%need?%
Costs,&quality,&deadline
New&orders
With%WHAT?
Material&
Informa7on&system&
With%WHO?
What&abili7es&are&required&?required?&
Availability
How%much?
Efficiency&measurement
Op7miza7on&of&the&means’&use&
Opera7ng&delay&
Material&availability…
How?%%
Procedures&and&control&plans
Informa7on&systems
Purchases
Recruitment,&training
Insurance…
Process
What%have%I%got%to%supply%with?
Costs,&quality,&deadline
New&orders
Requirements
Requirements
! So a business process is a set of activities assembled to produce specific outputs for specific customers.
! Humans start to draw the processes without using any hardware…
! … and then we use technology in order to get digitalized processes which will reflect what the humans initially drew.
14

! Drawing a status report: a preliminary search through the literature " Information system in public organization, BPM
approach and performance measurement throughout BSC in the public sector.
! An important phase of observation and an abductive work: " Back and forths between theory and fieldwork…
(Avenier & Gavard-Perret, 2007) " … to produce sense thanks to comparisons
(Charreire Petit & Durieux, 2007)
15
! A research-action approach:
" Immersion of the researcher who will directly work on the problem’s resolution (Allard-Poesi & Maréchal, 2007)…
" … but non-separability of the researcher and the object of study (Giordano & Jolibert, 2008)…
" … and, therefore, an amplification of the bias effect due to behaviour of the actors in relation to the problem (Journé, 2008).
16
17
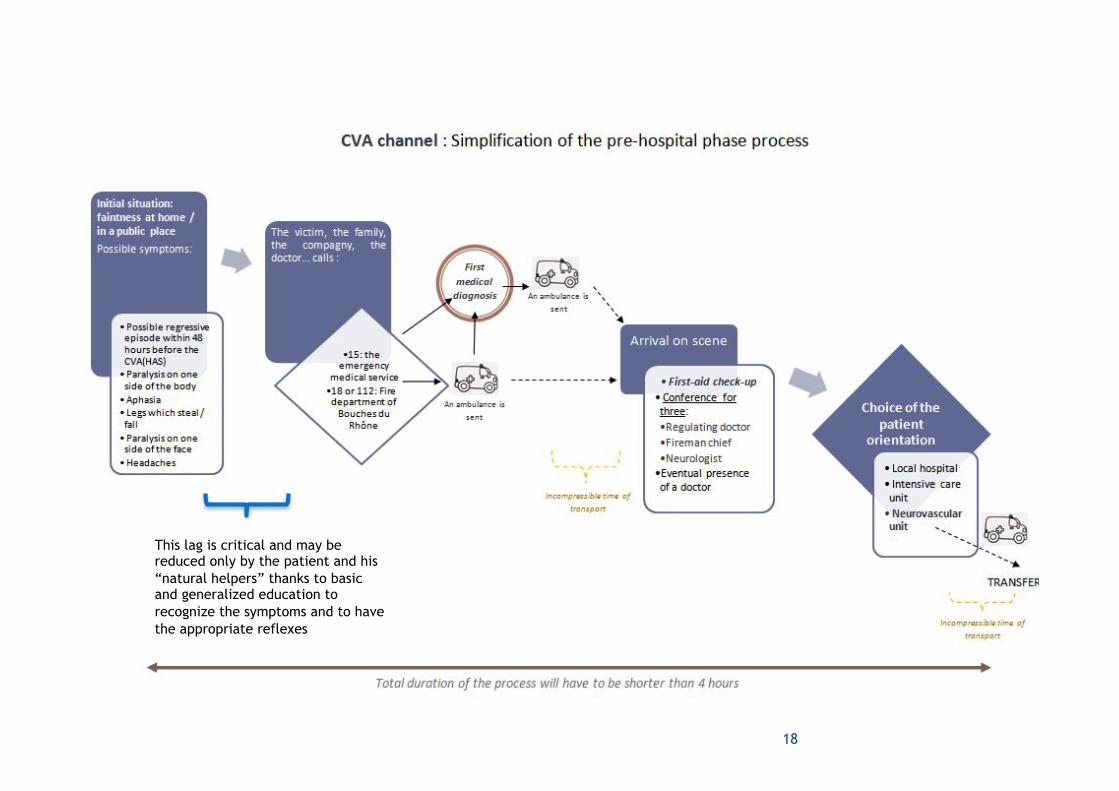
18
This lag is critical and may be reduced only by the patient and his “natural helpers” thanks to basic and generalized education to recognize the symptoms and to have the appropriate reflexes
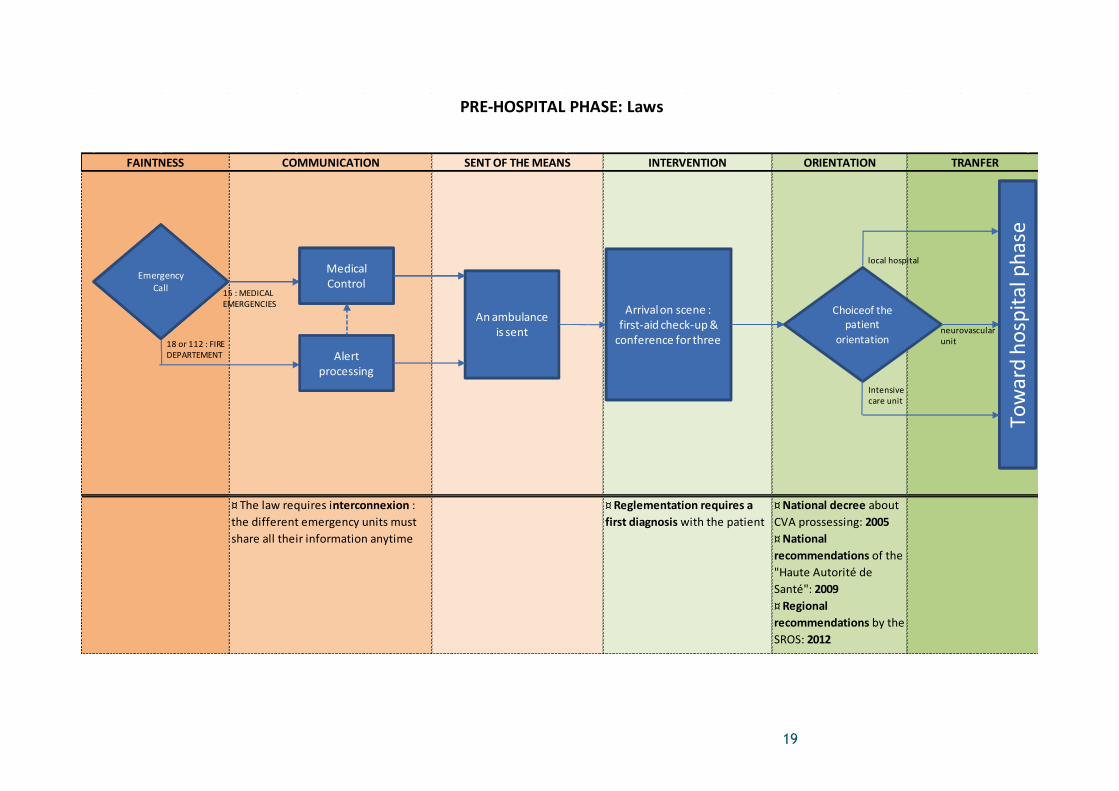
TRANFERINTERVENTION ORIENTATION
PRE+HOSPITAL/PHASE:/Laws
¤"The"law"requires"interconnexion":"the"different"emergency"units"must"share"all"their"information"anytime
¤"Reglementation/requires/a/first/diagnosis/with"the"patient
¤"National/decree"about"CVA"prossessing:"2005/////////////////////////////////////////////////////¤"National/recommendations"of"the""Haute"Autorité"de"Santé":"2009//////////////////////////////////////////////////////////////¤"Regional/recommendations"by"the"SROS:"2012
FAINTNESS COMMUNICATION SENT/OF/THE/MEANS
Appel du"patient"/"de"l'entourage
Bilan"médical
Vers"la"phase"hospitalière
Emergency"Call 15":"MEDICAL
EMERGENCIES
MedicalControl
18"or"112":"FIRE"DEPARTEMENT Alert
processing
Arrival"on"scene":"firstUaid"checkUup"&""conference"for"three
An"ambulance"is"sent
Choiceof"the"patient"
orientation
local"hospital
Intensivecare"unit
neurovascularunit
Toward"ho
spita
l"phase
19
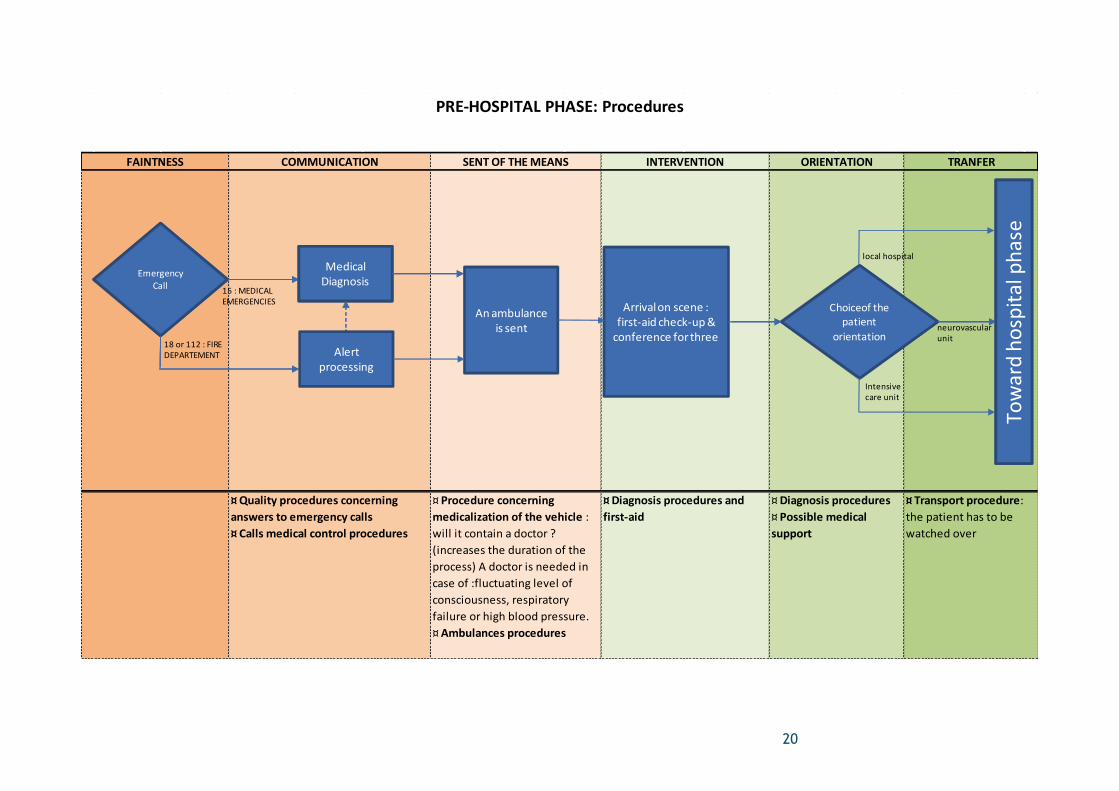
¤"Transport"procedure:"the"patient"has"to"be"watched"over
PRE2HOSPITAL"PHASE:"Procedures
FAINTNESS COMMUNICATION SENT"OF"THE"MEANS INTERVENTION ORIENTATION TRANFER
¤"Quality"procedures"concerning"answers"to"emergency"calls"""""""""""""""""""""""""""""""""""""¤"Calls"medical"control"procedures
¤"Procedure"concerning"medicalization"of"the"vehicle":"will"it"contain"a"doctor"?"(increases"the"duration"of"the"process)"A"doctor"is"needed"in"case"of":fluctuating"level"of"consciousness,"respiratory"failure"or"high"blood"pressure.""""""""""""""""""""""""""""""""""""¤"Ambulances"procedures
¤"Diagnosis"procedures"and"first2aid"
¤"Diagnosis"procedures"""""""""""""""""""""""""""""""""""""""""""""""""¤"Possible"medical"support
Appel du"patient"/"de"l'entourage
Bilan"médical
Choix"de"l'orientation"du"patient
Vers"la"phase"hospitalière
Emergency"Call 15":"MEDICAL
EMERGENCIES
MedicalDiagnosis
18"or"112":"FIRE"DEPARTEMENT
Arrival"on"scene":"firstWaid"checkWup"&""conference"for"three
Choiceof"the"patient"
orientation
local"hospital
Intensivecare"unit
neurovascularunit
Toward"ho
spita
l"phase
Alertprocessing
An"ambulance"is"sent
20

¤"Training'on'transport'conditions''''''''''''''''''''''''''''''''¤"Training'on'patient'surveyance"during"the"transfer"""""""""""""""""""""""""""""""""""""""¤"Informations"about"stroke'center'localisation
PRE7HOSPITAL'PHASE:'Initiatives/Innovations
FAINTNESS COMMUNICATION SENT'OF'THE'MEANS INTERVENTION ORIENTATION TRANFER
¤"Awareness'campaigns'intended'for'the'general'public:"circulation"of"informations"about"CVA"so"everyone"can"recognize"a"stroke
¤"Answerers'training ¤"Preliminary'training'about'CVA'for'the'Fire'Department'actors
¤'Quality'informations'passed'on'the'neurologist'of'the'neurovascular'unit:'will"he"treat"this"patient?""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""¤"Constant'work'with'hospital"and"SAMU"doctors'for'organisational'change
Emergency"Call 15":"MEDICAL
EMERGENCIES
MedicalDiagnosis
18"or"112":"FIRE"DEPARTEMENT
Arrival"on"scene":"firstPaid"checkPup"&""conference"for"three
Choiceof"the"patient"
orientation
local"hospital
Intensivecare"unit
neurovascularunit
Toward"ho
spita
l"phase
Alertprocessing
An"ambulance"is"sent
21
22
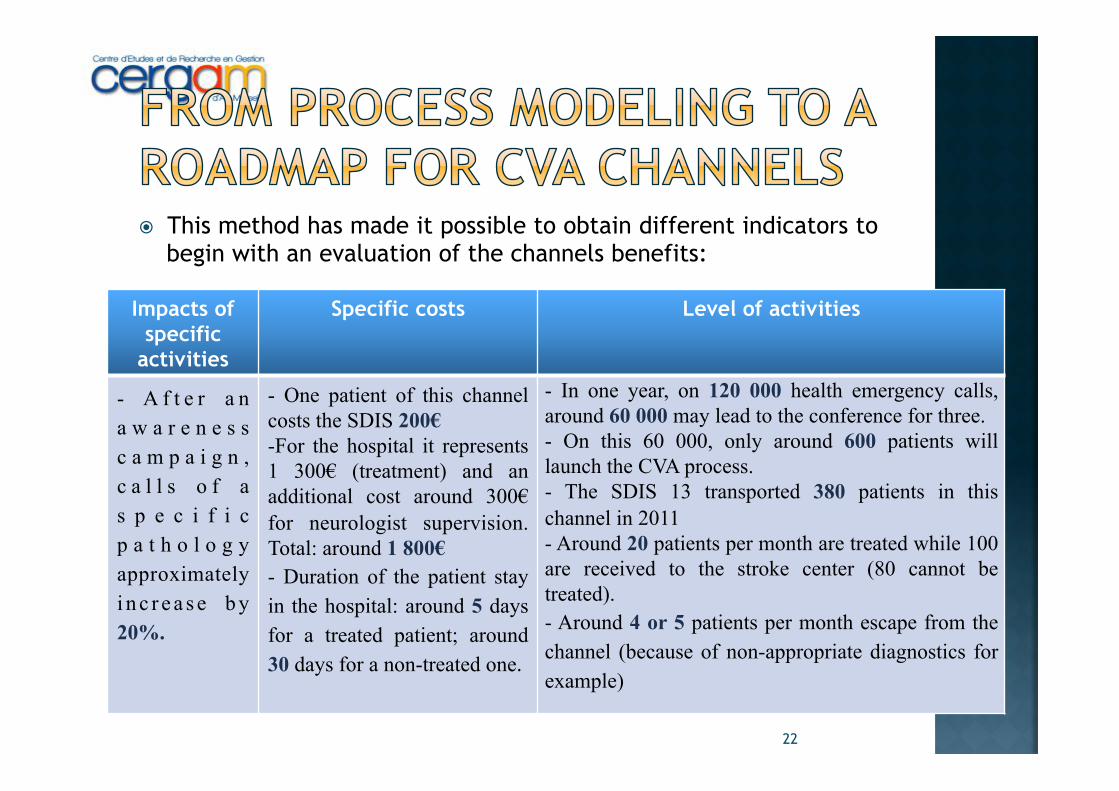
! This method has made it possible to obtain different indicators to begin with an evaluation of the channels benefits:
Impacts of specific
activities
Specific costs Level of activities
- A f t e r a n a w a r e n e s s c a m p a i g n , c a l l s o f a s p e c i f i c p a t h o l o g y approximately i n c r e a s e b y 20%.
- One patient of this channel costs the SDIS 200€ - For the hospital it represents 1 300€ (treatment) and an additional cost around 300€ for neurologist supervision. Total: around 1 800€ - Duration of the patient stay in the hospital: around 5 days for a treated patient; around 30 days for a non-treated one.
- In one year, on 120 000 health emergency calls, around 60 000 may lead to the conference for three. - On this 60 000, only around 600 patients will launch the CVA process. - The SDIS 13 transported 380 patients in this channel in 2011 - Around 20 patients per month are treated while 100 are received to the stroke center (80 cannot be treated). - Around 4 or 5 patients per month escape from the channel (because of non-appropriate diagnostics for example)

! Because of our conviction of the reproducibility of this channel, we can conclude with a roadmap to build up and conduct such an undertaking:
" The crucial point in the functioning of this channel was the coordination needed between the different actors: it led to an organizational change.
" The information quality and the training also played an important role.
" It will be necessary to inform the institutions to obtain the support of higher organizations, and to inform the public by awareness campaigns.
" At the edge, technical aspects may have their importance.
23

24
Calling the
rescue
Prehospital phase
hospital phase
Short term
output
Lon term outcome
The number of stokes is a constant in an homogeneous set of population. If the number fails, it means that patients have escape the process
Socio economic impact Deciding an education campaign
Benefits of extra stroke centers costs
! We proposed an overview of a real stroke channel.
! A BSC is required to pursue this work.
! The channel is reproducible… " Without modifications, in any hospital for strokes " With modifications, to be applied to other
pathologies as heart attack.
25

Thank you for your attention.