stem cell harvesting device with passive flexible drilling
TRANSCRIPT

Ohashi, K.; Hata, N.; Matsumura, T.; Ogata, T.; Yahagi, N.; Sakuma, I.; Dohi, T., Stem cell harvesting device with passive flexible dr illing unit for bone marrow transplantation. IEEE Transactions on Robotics and Automation, 19(5), 810- 817, 2003 ATRE Lab, Univ. of Tokyo
1
Abstract— A novel device is described for efficiently harvesting bone marrow in bone marrow transplantation that uses a newly developed passive flexible drilling unit and suction mechanism. The device reduces the invasiveness of bone marrow harvesting by collecting stem cells from the iliac bone with minimal punctures and by reducing the operation time and the contamination by T cells. The device is inserted into the medullary space from the iliac crest and aspirates the bone marrow while an end-mill on the tip of the drilling unit drills through the cancellous bone to create a curved path. In-vitro and in-vivo pig studies showed that the de-vice can be inserted into the medullary space of the pig iliac bone, 131 mm by 32.1 mm/min, and used to harvest about six times as much bone marrow per puncture as the conventional aspiration method. They also showed that the device can generate higher and longer negative pressure (–76.9 kPa for 5.96 sec) than the aspira-tion method (–41.8 kPa for 4.97 sec). The device, when applied in clinical study, will reduce invasiveness by harvesting denser graft from a wider area of the iliac bone compared to the conventional aspiration method, although minimal puncturing is required.
Index Terms — biomedical equipment, bone marrow trans-plantation, drilling, flexible device, hematopoietic stem cells
I. INTRODUCTION ver the past three decades, bone marrow transplantation
(BMT) has been established as a standard curative form of therapy for various acquired hematological malignancies
and congenital immune deficiencies such as leukemia and lym-phoma [1]. One of the most common procedure for BMT is aspiration method where hematopoietic stem cells are collected from donors’ bone marrow in the iliac bone using bone marrow needles [2]. The Aspiration Method has been widely used clinically for its simplicity. The method is an easy procedure for internists to perform, and requires only bone marrow needles.
Manuscript received June 29, 2002. This work was supported in part by Grant-in-Aid for Scientific Research (A-14702070 and B-13558103). NH was supported by Toyota Physical and Chemical Research Institute, Kurata grants, and the Suzuken Memorial Foundation
Kota Ohashi, Nobuhiko Hata and Takeyoshi Dohi are with the Advanced Therapeutic and Rehabilitation Engineering Laboratory (ATRE Lab.), Gradu-ate School of Information Science and Technology, the University of Tokyo, 7-3-1 Hongo, Tokyo, Japan (e-mail: kotaoha,noby,[email protected])
Ichiro Sakuma is with the Biomedical Precision Engineering Laboratory (BMPE Lab.), Graduate School of Frontier Sciences, the University of Tokyo, 7-3-1 Hongo, Tokyo, Japan (e-mail: [email protected])
Naoki Yahagi, Tomoko Matsumura and Toru Ogata are with Graduate School of Medicine, the University of Tokyo, 7-3-1 Hongo, Tokyo, Japan (e-mail: [email protected], tmatsumu-tky, [email protected])
On the other hand, several reports have been published ar-guing the invasiveness of the Aspiration Method [3]. The method occasionally causes complications and exceptionally life-threatening ones. Buckner reported that six donors out of 1160 had life-threatening complications: cardiopulmonary ar-rest, infectious nature, and cerebrovascular embolic episode [4]. The Japan Marrow Donor Foundation reported that the 14% of donors had transient fever and the 82% felt pain to some extent after the procedure of the Aspiration Method.
In general, complications following bone marrow collection using the Aspiration Method are caused by three complex but related factors: extensive puncturing by the aspiration needles, low density of harvested graft, and long procedure time under general anesthesia. First, one puncture of aspiration needle can collect 10cc of bone marrow, totaling 50 to 300 puncturing in a procedure to collect 500 to 1200 cc [5]. Furthermore, the den-sity of harvested graft tends to become smaller over procedure, which also leads to excessive puncture, hence longer procedure time under general anesthesia. Moreover, if the density of harvested graft is low, harvested graft includes much contami-nation from peripheral blood, which contains greater than 20% of T cells that can cause the patient acute graft vs. host disease (GVHD, a form of rejection) [6].
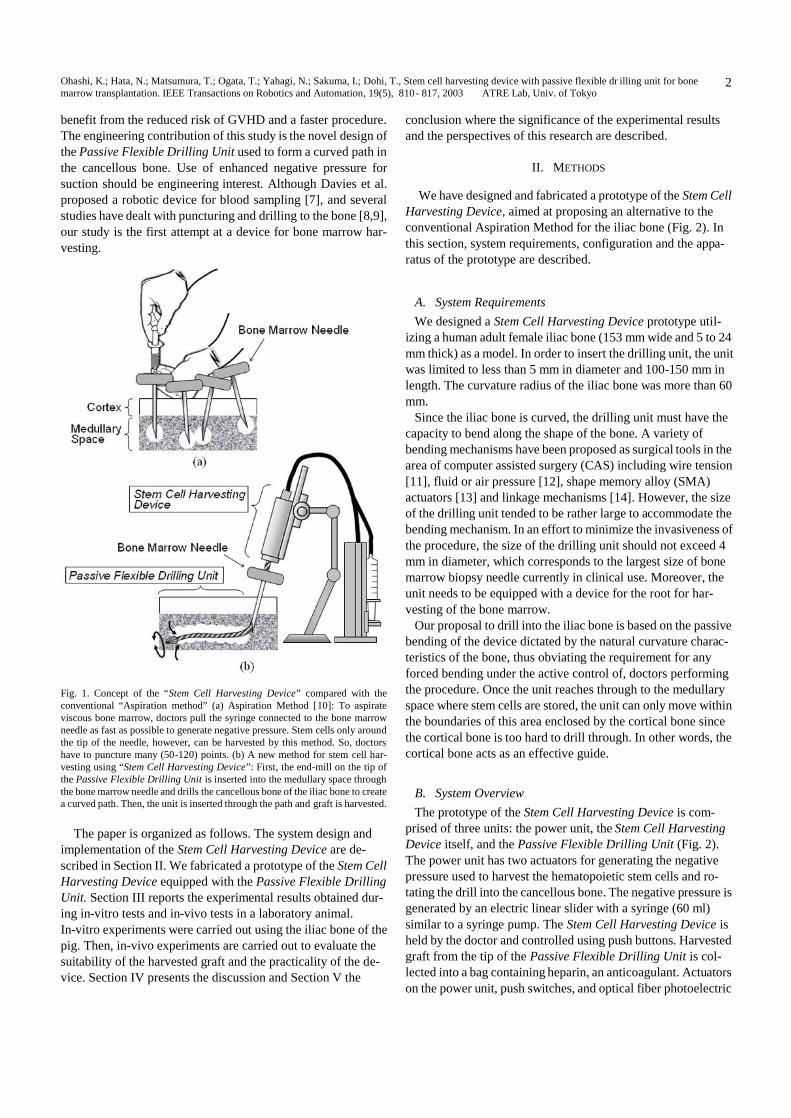
Our proposal to overcome these issues is to use of a newly developed robotic device supported by two significant and novel mechanisms (Fig.1): a long flexible drill to approach the medullary space by passively bending the drill and producing a curved approach channel, and a suction harvest graft using negative pressure generated by an actuator. The drilling unit, or Passive Flexible Drilling Unit, is a catheter inserted into the medullary space of the iliac bone through a bone marrow needle. The unit also functions as a trochanter with an end-mill on the tip of the unit drilling the cancellous bone to create a curved path. The harvesting device is called Stem Cell Harvesting Device that generates negative pressure to harvest viscous bone marrow efficiently.
In this paper, we summarized the mechanism and design criteria of the Stem Cell Harvesting Device with Passive Flexi-ble Drilling Unit, followed by evaluation study from in-vitro animal experiments and in-vivo laboratory tests. The clinical contribution of this study is to lessen the invasiveness to donors by harvesting denser graft from wider area of the iliac bone than conventional aspiration method, though minimal puncturing is required. Additionally, patients and doctors both benefit from
Stem Cell Harvesting Device with Passive Flexible Drilling Unit for Bone Marrow Transplantation
Kota Ohashi, Student Member, IEEE, Nobuhiko Hata, Member, IEEE, Tomoko Matsumura, Toru Ogata, Naoki Yahagi, Ichiro Sakuma and Takeyoshi Dohi
O
Ohashi, K.; Hata, N.; Matsumura, T.; Ogata, T.; Yahagi, N.; Sakuma, I.; Dohi, T., Stem cell harvesting device with passive flexible dr illing unit for bone marrow transplantation. IEEE Transactions on Robotics and Automation, 19(5), 810- 817, 2003 ATRE Lab, Univ. of Tokyo
2
benefit from the reduced risk of GVHD and a faster procedure. The engineering contribution of this study is the novel design of the Passive Flexible Drilling Unit used to form a curved path in the cancellous bone. Use of enhanced negative pressure for suction should be engineering interest. Although Davies et al. proposed a robotic device for blood sampling [7], and several studies have dealt with puncturing and drilling to the bone [8,9], our study is the first attempt at a device for bone marrow har-vesting.
Fig. 1. Concept of the “Stem Cell Harvesting Device” compared with the conventional “Aspiration method” (a) Aspiration Method [10]: To aspirate viscous bone marrow, doctors pull the syringe connected to the bone marrow needle as fast as possible to generate negative pressure. Stem cells only around the tip of the needle, however, can be harvested by this method. So, doctors have to puncture many (50-120) points. (b) A new method for stem cell har-vesting using “Stem Cell Harvesting Device”: First, the end-mill on the tip of the Passive Flexible Drilling Unit is inserted into the medullary space through the bone marrow needle and drills the cancellous bone of the iliac bone to create a curved path. Then, the unit is inserted through the path and graft is harvested.
The paper is organized as follows. The system design and
implementation of the Stem Cell Harvesting Device are de-scribed in Section II. We fabricated a prototype of the Stem Cell Harvesting Device equipped with the Passive Flexible Drilling Unit. Section III reports the experimental results obtained dur-ing in-vitro tests and in-vivo tests in a laboratory animal. In-vitro experiments were carried out using the iliac bone of the pig. Then, in-vivo experiments are carried out to evaluate the suitability of the harvested graft and the practicality of the de-vice. Section IV presents the discussion and Section V the
conclusion where the significance of the experimental results and the perspectives of this research are described.
II. METHODS
We have designed and fabricated a prototype of the Stem Cell Harvesting Device, aimed at proposing an alternative to the conventional Aspiration Method for the iliac bone (Fig. 2). In this section, system requirements, configuration and the appa-ratus of the prototype are described.
A. System Requirements We designed a Stem Cell Harvesting Device prototype util-
izing a human adult female iliac bone (153 mm wide and 5 to 24 mm thick) as a model. In order to insert the drilling unit, the unit was limited to less than 5 mm in diameter and 100-150 mm in length. The curvature radius of the iliac bone was more than 60 mm.
Since the iliac bone is curved, the drilling unit must have the capacity to bend along the shape of the bone. A variety of bending mechanisms have been proposed as surgical tools in the area of computer assisted surgery (CAS) including wire tension [11], fluid or air pressure [12], shape memory alloy (SMA) actuators [13] and linkage mechanisms [14]. However, the size of the drilling unit tended to be rather large to accommodate the bending mechanism. In an effort to minimize the invasiveness of the procedure, the size of the drilling unit should not exceed 4 mm in diameter, which corresponds to the largest size of bone marrow biopsy needle currently in clinical use. Moreover, the unit needs to be equipped with a device for the root for har-vesting of the bone marrow.
Our proposal to drill into the iliac bone is based on the passive bending of the device dictated by the natural curvature charac-teristics of the bone, thus obviating the requirement for any forced bending under the active control of, doctors performing the procedure. Once the unit reaches through to the medullary space where stem cells are stored, the unit can only move within the boundaries of this area enclosed by the cortical bone since the cortical bone is too hard to drill through. In other words, the cortical bone acts as an effective guide.
B. System Overview The prototype of the Stem Cell Harvesting Device is com-
prised of three units: the power unit, the Stem Cell Harvesting Device itself, and the Passive Flexible Drilling Unit (Fig. 2). The power unit has two actuators for generating the negative pressure used to harvest the hematopoietic stem cells and ro-tating the drill into the cancellous bone. The negative pressure is generated by an electric linear slider with a syringe (60 ml) similar to a syringe pump. The Stem Cell Harvesting Device is held by the doctor and controlled using push buttons. Harvested graft from the tip of the Passive Flexible Drilling Unit is col-lected into a bag containing heparin, an anticoagulant. Actuators on the power unit, push switches, and optical fiber photoelectric
Ohashi, K.; Hata, N.; Matsumura, T.; Ogata, T.; Yahagi, N.; Sakuma, I.; Dohi, T., Stem cell harvesting device with passive flexible dr illing unit for bone marrow transplantation. IEEE Transactions on Robotics and Automation, 19(5), 810- 817, 2003 ATRE Lab, Univ. of Tokyo
3
switches on the device are controlled by a stored programmable motion controller1.
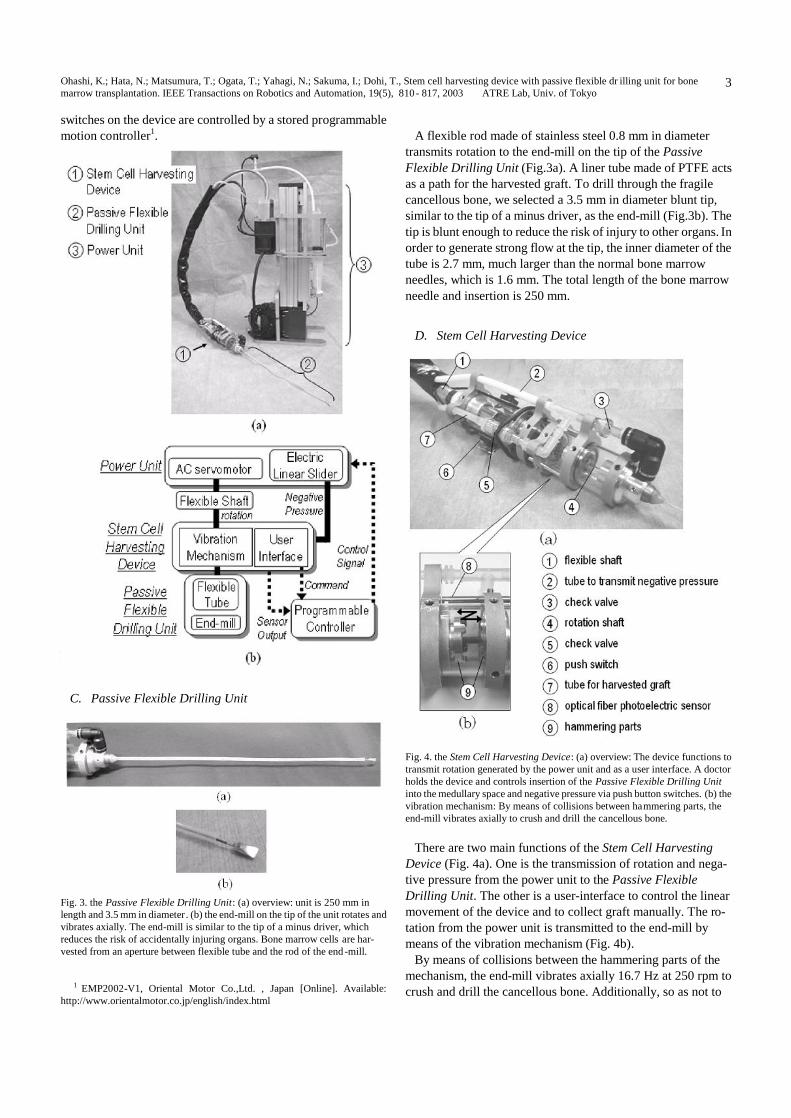
Fig. 2. Prototype of the Stem Cell Harvesting Device: (a) Overview of the system: (b) System configuration: comprised of three units, the Stem Cell Harvesting Device, the Passive Flexible Drilling Unit, and a power unit con-trolled by a stored programmable controller.
C. Passive Flexible Drilling Unit
Fig. 3. the Passive Flexible Drilling Unit: (a) overview: unit is 250 mm in length and 3.5 mm in diameter . (b) the end-mill on the tip of the unit rotates and vibrates axially. The end-mill is similar to the tip of a minus driver, which reduces the risk of accidentally injuring organs. Bone marrow cells are har-vested from an aperture between flexible tube and the rod of the end -mill.
1 EMP2002-V1, Oriental Motor Co.,Ltd. , Japan [Online]. Available:
http://www.orientalmotor.co.jp/english/index.html
A flexible rod made of stainless steel 0.8 mm in diameter
transmits rotation to the end-mill on the tip of the Passive Flexible Drilling Unit (Fig.3a). A liner tube made of PTFE acts as a path for the harvested graft. To drill through the fragile cancellous bone, we selected a 3.5 mm in diameter blunt tip, similar to the tip of a minus driver, as the end-mill (Fig.3b). The tip is blunt enough to reduce the risk of injury to other organs. In order to generate strong flow at the tip, the inner diameter of the tube is 2.7 mm, much larger than the normal bone marrow needles, which is 1.6 mm. The total length of the bone marrow needle and insertion is 250 mm.
D. Stem Cell Harvesting Device
Fig. 4. the Stem Cell Harvesting Device: (a) overview: The device functions to transmit rotation generated by the power unit and as a user interface. A doctor holds the device and controls insertion of the Passive Flexible Drilling Unit into the medullary space and negative pressure via push button switches. (b) the vibration mechanism: By means of collisions between hammering parts, the end-mill vibrates axially to crush and drill the cancellous bone.
There are two main functions of the Stem Cell Harvesting
Device (Fig. 4a). One is the transmission of rotation and nega-tive pressure from the power unit to the Passive Flexible Drilling Unit. The other is a user-interface to control the linear movement of the device and to collect graft manually. The ro-tation from the power unit is transmitted to the end-mill by means of the vibration mechanism (Fig. 4b).
By means of collisions between the hammering parts of the mechanism, the end-mill vibrates axially 16.7 Hz at 250 rpm to crush and drill the cancellous bone. Additionally, so as not to
Ohashi, K.; Hata, N.; Matsumura, T.; Ogata, T.; Yahagi, N.; Sakuma, I.; Dohi, T., Stem cell harvesting device with passive flexible dr illing unit for bone marrow transplantation. IEEE Transactions on Robotics and Automation, 19(5), 810- 817, 2003 ATRE Lab, Univ. of Tokyo
4
drill through the cortical bone accidentally and injure internal organs, the mechanism does not transmit power until the end-mill yields valid axial motion due to counterforce from the cancellous bone detected by an optical fiber photoelectric sen-sor.
E. Power Unit For Negative Pressure And Drilling To generate negative pressure, the power unit contains an
electric linear slider. The slider is equipped with a 60 cc syringe normally used in the clinical field and pulls it like a syringe pump. The stroke of the slider is 100 mm. A tube to transmit negative pressure is connected from the syringe to the Stem Cell Harvesting Device through check valves so that backward flow is not generated accidentally.
The power unit also generates rotation for the end-mill via an AC servomotor. The shaft of the motor is connected to the vi-bration mechanism of the device by means of a flexible shaft that is 800 mm in length and 8.0 mm in diameter.
III. EXPERIMENTAL RESULTS The device has two main functions: drilling the cancellous
bone and harvesting bone marrow cells. First, as an investiga-tion of the mechanical performance to drill the cancellous bone, in-vitro experiments on a pig iliac bone were carried out. Sec-ondly, as an investigation of the mechanical performance to harvest bone marrow cells, an experiment was carried out on a phantom.
Then, in-vivo experiments were carried out on the iliac bone of laboratory animals to evaluate the availability of the har-vested graft and the usability of the device.
A. in-vitro Experiments Of Drilling Then, we carried out in-vitro experiments to evaluate the
mechanical performance of drilling using the iliac bone of the pig, which is similar to that of humans with respect to cutting [15]. The prototype was inserted into the medullary space from a spot in the iliac crest.
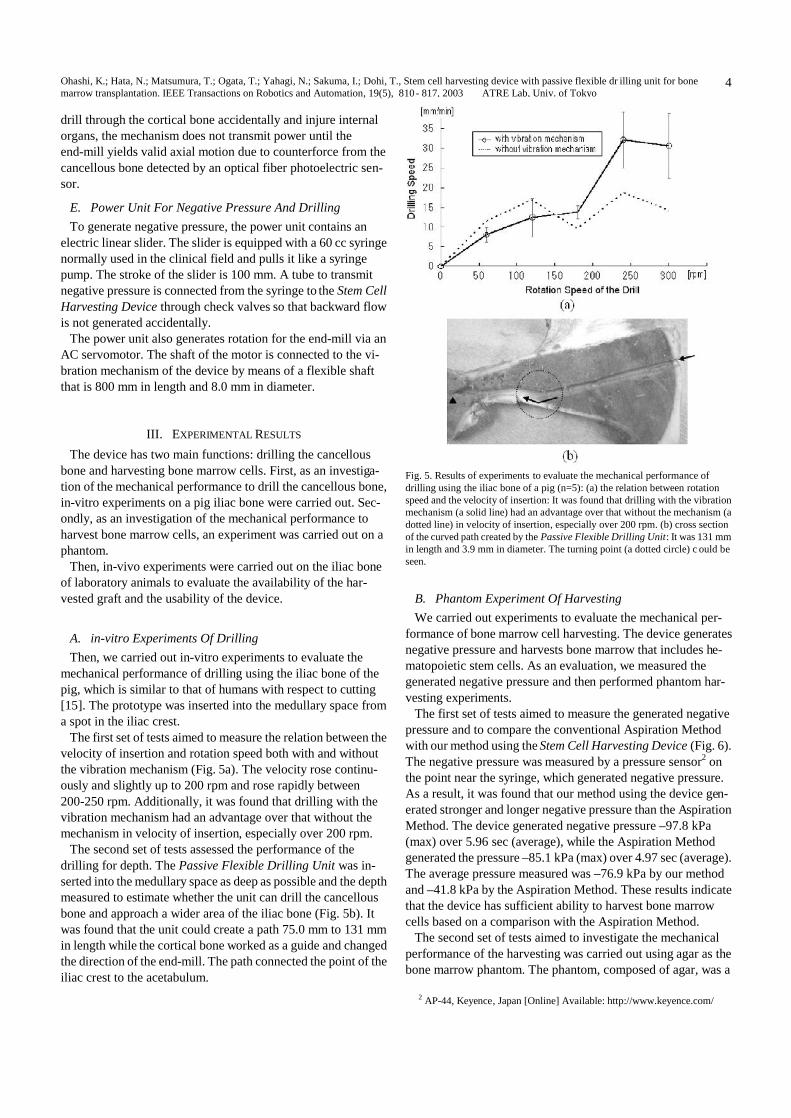
The first set of tests aimed to measure the relation between the velocity of insertion and rotation speed both with and without the vibration mechanism (Fig. 5a). The velocity rose continu-ously and slightly up to 200 rpm and rose rapidly between 200-250 rpm. Additionally, it was found that drilling with the vibration mechanism had an advantage over that without the mechanism in velocity of insertion, especially over 200 rpm.
The second set of tests assessed the performance of the drilling for depth. The Passive Flexible Drilling Unit was in-serted into the medullary space as deep as possible and the depth measured to estimate whether the unit can drill the cancellous bone and approach a wider area of the iliac bone (Fig. 5b). It was found that the unit could create a path 75.0 mm to 131 mm in length while the cortical bone worked as a guide and changed the direction of the end-mill. The path connected the point of the iliac crest to the acetabulum.
Fig. 5. Results of experiments to evaluate the mechanical performance of drilling using the iliac bone of a pig (n=5): (a) the relation between rotation speed and the velocity of insertion: It was found that drilling with the vibration mechanism (a solid line) had an advantage over that without the mechanism (a dotted line) in velocity of insertion, especially over 200 rpm. (b) cross section of the curved path created by the Passive Flexible Drilling Unit: It was 131 mm in length and 3.9 mm in diameter. The turning point (a dotted circle) c ould be seen.
B. Phantom Experiment Of Harvesting We carried out experiments to evaluate the mechanical per-
formance of bone marrow cell harvesting. The device generates negative pressure and harvests bone marrow that includes he-matopoietic stem cells. As an evaluation, we measured the generated negative pressure and then performed phantom har-vesting experiments.
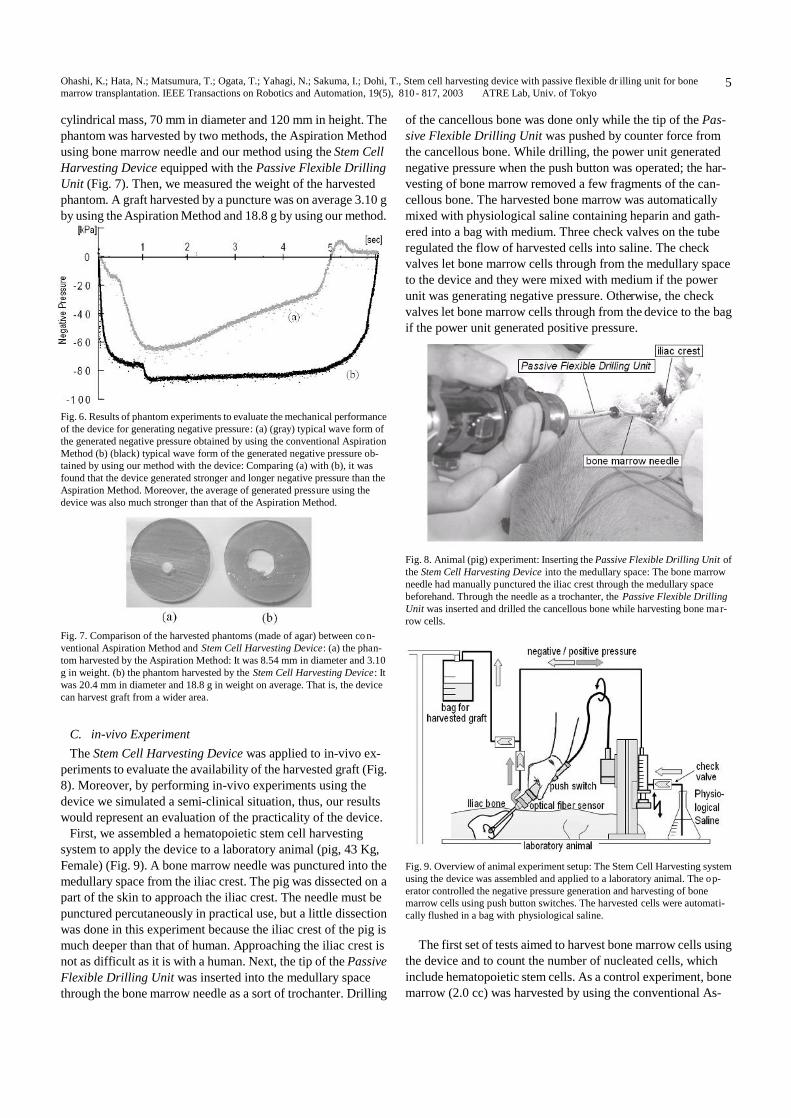
The first set of tests aimed to measure the generated negative pressure and to compare the conventional Aspiration Method with our method using the Stem Cell Harvesting Device (Fig. 6). The negative pressure was measured by a pressure sensor2 on the point near the syringe, which generated negative pressure. As a result, it was found that our method using the device gen-erated stronger and longer negative pressure than the Aspiration Method. The device generated negative pressure –97.8 kPa (max) over 5.96 sec (average), while the Aspiration Method generated the pressure –85.1 kPa (max) over 4.97 sec (average). The average pressure measured was –76.9 kPa by our method and –41.8 kPa by the Aspiration Method. These results indicate that the device has sufficient ability to harvest bone marrow cells based on a comparison with the Aspiration Method.
The second set of tests aimed to investigate the mechanical performance of the harvesting was carried out using agar as the bone marrow phantom. The phantom, composed of agar, was a
2 AP-44, Keyence, Japan [Online] Available: http://www.keyence.com/
Ohashi, K.; Hata, N.; Matsumura, T.; Ogata, T.; Yahagi, N.; Sakuma, I.; Dohi, T., Stem cell harvesting device with passive flexible dr illing unit for bone marrow transplantation. IEEE Transactions on Robotics and Automation, 19(5), 810- 817, 2003 ATRE Lab, Univ. of Tokyo
5
cylindrical mass, 70 mm in diameter and 120 mm in height. The phantom was harvested by two methods, the Aspiration Method using bone marrow needle and our method using the Stem Cell Harvesting Device equipped with the Passive Flexible Drilling Unit (Fig. 7). Then, we measured the weight of the harvested phantom. A graft harvested by a puncture was on average 3.10 g by using the Aspiration Method and 18.8 g by using our method.
Fig. 6. Results of phantom experiments to evaluate the mechanical performance of the device for generating negative pressure: (a) (gray) typical wave form of the generated negative pressure obtained by using the conventional Aspiration Method (b) (black) typical wave form of the generated negative pressure ob-tained by using our method with the device: Comparing (a) with (b), it was found that the device generated stronger and longer negative pressure than the Aspiration Method. Moreover, the average of generated pressure using the device was also much stronger than that of the Aspiration Method.
Fig. 7. Comparison of the harvested phantoms (made of agar) between co n-ventional Aspiration Method and Stem Cell Harvesting Device: (a) the phan-tom harvested by the Aspiration Method: It was 8.54 mm in diameter and 3.10 g in weight. (b) the phantom harvested by the Stem Cell Harvesting Device: It was 20.4 mm in diameter and 18.8 g in weight on average. That is, the device can harvest graft from a wider area.
C. in-vivo Experiment The Stem Cell Harvesting Device was applied to in-vivo ex-
periments to evaluate the availability of the harvested graft (Fig. 8). Moreover, by performing in-vivo experiments using the device we simulated a semi-clinical situation, thus, our results would represent an evaluation of the practicality of the device.
First, we assembled a hematopoietic stem cell harvesting system to apply the device to a laboratory animal (pig, 43 Kg, Female) (Fig. 9). A bone marrow needle was punctured into the medullary space from the iliac crest. The pig was dissected on a part of the skin to approach the iliac crest. The needle must be punctured percutaneously in practical use, but a little dissection was done in this experiment because the iliac crest of the pig is much deeper than that of human. Approaching the iliac crest is not as difficult as it is with a human. Next, the tip of the Passive Flexible Drilling Unit was inserted into the medullary space through the bone marrow needle as a sort of trochanter. Drilling
of the cancellous bone was done only while the tip of the Pas-sive Flexible Drilling Unit was pushed by counter force from the cancellous bone. While drilling, the power unit generated negative pressure when the push button was operated; the har-vesting of bone marrow removed a few fragments of the can-cellous bone. The harvested bone marrow was automatically mixed with physiological saline containing heparin and gath-ered into a bag with medium. Three check valves on the tube regulated the flow of harvested cells into saline. The check valves let bone marrow cells through from the medullary space to the device and they were mixed with medium if the power unit was generating negative pressure. Otherwise, the check valves let bone marrow cells through from the device to the bag if the power unit generated positive pressure.
Fig. 8. Animal (pig) experiment: Inserting the Passive Flexible Drilling Unit of the Stem Cell Harvesting Device into the medullary space: The bone marrow needle had manually punctured the iliac crest through the medullary space beforehand. Through the needle as a trochanter, the Passive Flexible Drilling Unit was inserted and drilled the cancellous bone while harvesting bone mar-row cells.
Fig. 9. Overview of animal experiment setup: The Stem Cell Harvesting system using the device was assembled and applied to a laboratory animal. The op-erator controlled the negative pressure generation and harvesting of bone marrow cells using push button switches. The harvested cells were automati-cally flushed in a bag with physiological saline.
The first set of tests aimed to harvest bone marrow cells using
the device and to count the number of nucleated cells, which include hematopoietic stem cells. As a control experiment, bone marrow (2.0 cc) was harvested by using the conventional As-
Ohashi, K.; Hata, N.; Matsumura, T.; Ogata, T.; Yahagi, N.; Sakuma, I.; Dohi, T., Stem cell harvesting device with passive flexible dr illing unit for bone marrow transplantation. IEEE Transactions on Robotics and Automation, 19(5), 810- 817, 2003 ATRE Lab, Univ. of Tokyo
6
piration Method. Then, we compared two methods: using the Stem Cell Harvesting Device vs. using the conventional Aspi-ration Method (Table I).
TABLE I
COMPARISON OF HARVESTED GRAFT BY CONVENTIONAL ASPIRATION METHOD AND THE STEM CELL HARVESTING DEVICE:
By using the device, the number of harvested nucleated cells
per minute was 2.05 times more than the Aspiration Method. Moreover, the number of nucleated cells per puncture was 6.04 times more than the Aspiration Method. From the viewpoint of density, however, the Aspiration Method could harvest much (3.73 times) denser graft than our method using the device. These results mean that the device harvested stem cells effi-ciently with minimal punctures.
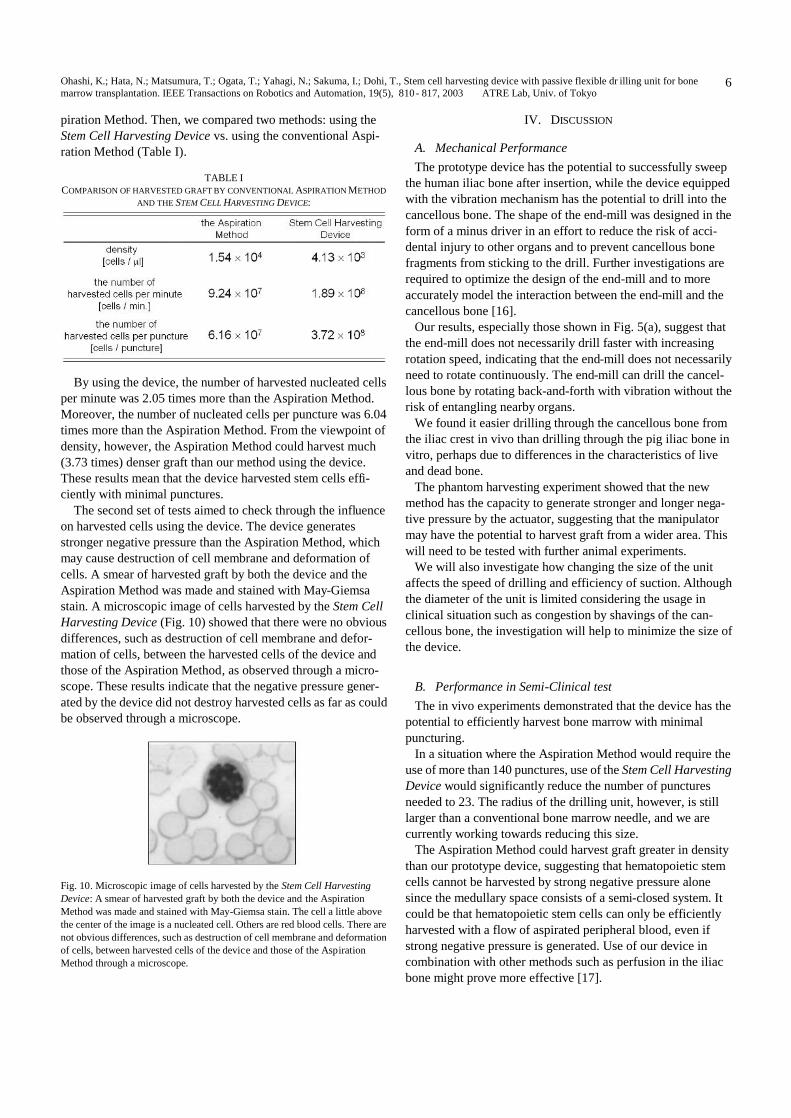
The second set of tests aimed to check through the influence on harvested cells using the device. The device generates stronger negative pressure than the Aspiration Method, which may cause destruction of cell membrane and deformation of cells. A smear of harvested graft by both the device and the Aspiration Method was made and stained with May-Giemsa stain. A microscopic image of cells harvested by the Stem Cell Harvesting Device (Fig. 10) showed that there were no obvious differences, such as destruction of cell membrane and defor-mation of cells, between the harvested cells of the device and those of the Aspiration Method, as observed through a micro-scope. These results indicate that the negative pressure gener-ated by the device did not destroy harvested cells as far as could be observed through a microscope.
Fig. 10. Microscopic image of cells harvested by the Stem Cell Harvesting Device: A smear of harvested graft by both the device and the Aspiration Method was made and stained with May-Giemsa stain. The cell a little above the center of the image is a nucleated cell. Others are red blood cells. There are not obvious differences, such as destruction of cell membrane and deformation of cells, between harvested cells of the device and those of the Aspiration Method through a microscope.
IV. DISCUSSION
A. Mechanical Performance The prototype device has the potential to successfully sweep
the human iliac bone after insertion, while the device equipped with the vibration mechanism has the potential to drill into the cancellous bone. The shape of the end-mill was designed in the form of a minus driver in an effort to reduce the risk of acci-dental injury to other organs and to prevent cancellous bone fragments from sticking to the drill. Further investigations are required to optimize the design of the end-mill and to more accurately model the interaction between the end-mill and the cancellous bone [16].
Our results, especially those shown in Fig. 5(a), suggest that the end-mill does not necessarily drill faster with increasing rotation speed, indicating that the end-mill does not necessarily need to rotate continuously. The end-mill can drill the cancel-lous bone by rotating back-and-forth with vibration without the risk of entangling nearby organs.
We found it easier drilling through the cancellous bone from the iliac crest in vivo than drilling through the pig iliac bone in vitro, perhaps due to differences in the characteristics of live and dead bone.
The phantom harvesting experiment showed that the new method has the capacity to generate stronger and longer nega-tive pressure by the actuator, suggesting that the manipulator may have the potential to harvest graft from a wider area. This will need to be tested with further animal experiments.
We will also investigate how changing the size of the unit affects the speed of drilling and efficiency of suction. Although the diameter of the unit is limited considering the usage in clinical situation such as congestion by shavings of the can-cellous bone, the investigation will help to minimize the size of the device.
B. Performance in Semi-Clinical test The in vivo experiments demonstrated that the device has the
potential to efficiently harvest bone marrow with minimal puncturing.
In a situation where the Aspiration Method would require the use of more than 140 punctures, use of the Stem Cell Harvesting Device would significantly reduce the number of punctures needed to 23. The radius of the drilling unit, however, is still larger than a conventional bone marrow needle, and we are currently working towards reducing this size.
The Aspiration Method could harvest graft greater in density than our prototype device, suggesting that hematopoietic stem cells cannot be harvested by strong negative pressure alone since the medullary space consists of a semi-closed system. It could be that hematopoietic stem cells can only be efficiently harvested with a flow of aspirated peripheral blood, even if strong negative pressure is generated. Use of our device in combination with other methods such as perfusion in the iliac bone might prove more effective [17].

Ohashi, K.; Hata, N.; Matsumura, T.; Ogata, T.; Yahagi, N.; Sakuma, I.; Dohi, T., Stem cell harvesting device with passive flexible dr illing unit for bone marrow transplantation. IEEE Transactions on Robotics and Automation, 19(5), 810- 817, 2003 ATRE Lab, Univ. of Tokyo
7
It should be pointed out that during the in vivo experiments, the device malfunctioned at times due to the deposition of cancellous bone shavings, fat tissue and other material despite flushing with physiological saline. The design mechanism of the device will require further investigations.
C. Perspective Further investigations are needed to ascertain whether the
Stem Cell Harvesting Device can collect enough viable hema-topoietic stem cells for use as graft in bone marrow transplan-tations. Biological tests such as colony assays and flow cy-tometry would be useful in this respect.
The interest in bone marrow cells has increased rapidly be-cause of their potential therapeutic use in immune deficiencies and hematological malignancies [18], tissue engineering and other cell therapies [19,20]. While the use of peripheral blood stem cell transplantation (PBSCT, harvesting stem cells from peripheral blood) has increased, some problems concerning donors have recently been reported [21]. The development of methods for the ex-vivo expansion of stem cells has been in-vestigated [22,23], and could be successfully utilized in con-junction with the Stem Cell Harvesting Device.
Although we opted for a passive bending mechanism for use with our device, an active bending mechanism within the can-cellous bone might prove effective in other applications such as orthopedic surgery. We intend to investigate an active bending mechanism as a tool for use in the CAS system where the bending kinematics of flexible snake-like robots can be docu-mented in detail. Chirikjian proposed a method for optimizing robot configurations that have a large degree of kinematic re-dundancy based on a continuum formulation of kinematics [24]. Suzumori reported on the characteristics of a flexible micro-actuator driven by an electro-pneumatic system [25], while Wilson reported on the mechanical behavior of a bellows-type flexible manipulator [26]. We intend to apply and refine these principles in relation to our future investigations.
V. CONCLUSION We reported the development of a new method of harvesting
stem cells for bone marrow transplantation that uses an inno-vative device, the Stem Cell Harvesting Device equipped with the Passive Flexible Drilling Unit. By using this device, more stem cells can be harvested from the iliac bone of donors with minimal punctures.
Secondly, we fabricated a prototype of the device and carried out experiments to evaluate whether it can create a curved path and harvest bone marrow. In the drilling experiments using a pig iliac bone, the device was inserted into the medullary space from the iliac crest 75.0-131 mm by 32.1 mm/min, enough to sweep the human iliac bone. Additionally, the prototype har-vested a 18.8 g bone marrow phantom in one puncture, about six times as much as the conventional Aspiration Method. These results indicate that the device has sufficient ability to harvest stem cells based on a comparison with the Aspiration Method.
In-vivo experiments to simulate a semi-clinical situation showed that the device has the potential to harvest bone marrow efficiently with minimal punctures though some problems emerged that would interfere with clinical use. By using the device, the number of harvested nucleated cells per second is 2.05 times more than the Aspiration Method. Moreover, the number of nucleated cells per puncture is 6.04 times more than the Aspiration Method. From the viewpoint of density, however, the Aspiration Method could harvest much denser graft than our method using the device. The microscopic observation of the harvested cells indicated that negative pressure generated by the device did not destroy harvested cells.
It is clear that the Stem Cell Harvesting Device, inserted into the medullary space curvedly using the Passive Flexible Drill-ing Unit and harvesting stem cells mechanically, has the po-tential to become an alternative to the Aspiration Method and minimize the invasion of donors and patients, though further improvements and experiments remain to be carried out.
ACKNOWLEDGEMENTS This study was partially supported by Grants-in-Aid for
Scientific Research (A-14702070 and B-13558103). NH was supported by the Toyota Physical and Chemical Research In-stitute, Kurata grants, and the Suzuken Memorial Foundation. The authors are grateful for the support of Dr. Utako Machida, Dr. Yuji Tanaka, Dr. Sachiko Seo, Dr. Shigeru Chiba, and Dr. Hisamaru Hirai.
REFERENCES [1] E.D. Thomas: “Does bone marrow transplantation confer a normal life
span?,” N. Engl. J. of Med. (1999) 341, pp. 50-51 [2] E. D. Thomas, and R. Storb: “Technique for human marrow grafting,”
Blood, Oct., 36(4) (1970) pp. 507-15 [3] D.F. Stroncek, PV. Holland, G. Bartch, T. Bixby, RG. Simmons, J.H.
Antin, K.C. Anderson, R.C. Ash, B.J. Bolwell, J.A. Hansen, et al., ”Ex-periences of the first 493 unrelated marrow donors in the National Marrow Donor Program,” Blood, Apr 1; 81(7) (1993) pp. 1940-6
[4] C.D. Buckner, R.A. Clift, J.E. Sanders, P. Stewart, W.I. Bensinger, K.C. Doney, K.M. Sullivan, R.P. Witherspoon, H.J. Deeg, F.R. Appelbaum, et al.: “Marrow harvesting from normal donors,” Blood, Sep; 64(3) (1984) pp.630-4
[5] H. J. Deeg, H.G. Klingemann, G.L. Phillips, and G. Van Zant, A Guide to Blood and Marrow Transplantation 3rd edn . Berlin Heidelberg: Springer-Verlag (1999) ch. 2, pp. 75-80
[6] T. Kushida, M. Inaba, K. Ikebukuro, T. Nagahama, H. Oyaizu, H. Lee, T. Ito, N. Ichioka, H. Hisha, K. Sugiura, S. Miyashima, N. Ageyama, F. Ono, H. Iida, R. Ogawa, and S. Ikehara: “A New Method for Bone Marrow Cell Harvesting,” Stem Cells, Vol. 18, No.6 (2000) pp. 453 -456
[7] A. Zivanovic and L. Davies: “A Robotic System for Blood Sampling”, IEEE Trans. On Information Technology and Biomedicine, Vol.4, No.1 (2000) pp. 8-14
[8] P.N. Brett, T.J. Parker, A.J. Harrison, T.A. Thomas and A. Carr: “Simulation of resistance forces acting on surgical needles”, Proc. of Inst. Mechanical Engineers, pt. H, Vol.211 (1997) pp.335 -347
[9] A. Petersik, B. Pflesser, U. Tiede, K.H. Hohne and R. Leuwer: “Realistic haptic volume interaction for petrous bone surgery simulation”, Proc. of CARS, Paris, June. 2002, pp.252-257
[10] A. Islam, Manual of Bone Marrow Examination. Amsterdam: Harwood Academic Publishers (1990) ch. 2, pp. 5 -29
[11] P. Dario: “A Novel Mechatronic Tool for Computer-Assisted Arthro-scopy”, IEEE Trans. on Information Technology in Biomedicine Vol.4, No.1 (2000) pp. 15-28
Ohashi, K.; Hata, N.; Matsumura, T.; Ogata, T.; Yahagi, N.; Sakuma, I.; Dohi, T., Stem cell harvesting device with passive flexible dr illing unit for bone marrow transplantation. IEEE Transactions on Robotics and Automation, 19(5), 810- 817, 2003 ATRE Lab, Univ. of Tokyo
8
[12] K. Ikuta, H. Ichikawa, and K. Suzuki: “Safety-Active Catheter with Multiple-Segments Driven by Micro Hydraulic Actuators”, Proc. of MICCAI, Tokyo, September. 2002, pp. 182-191
[13] T. Fukuda, S. Guo, K. Kosuge, F. Arai, M. Negoro, and K. Nakabayashi: “Micro active catheter system with multi degrees of freedom,” Proc. of ICRA, San Diego, May. 1994, pp. 2290-2295
[14] H. Yamashita, K. Daeyoung, N. Hata, T. Dohi: "Multi-slider Linkage Mechanism for Endoscopic Manipulator", Proc. of CARS, Paris, June. 2002, pp.1086
[15] S. Itoh, “Development of the material for simulating the friction of hu-man bone cutting,” Bull. of Japan Society of Mechanical Engineers 26-222 (1983) pp. 2295
[16] V. Colla, B. Allotta: “Wavelet-Based Control of Penetration in a Mechatronic Drill for Orthopaedic Surgery”, Proc. of ICRA, Lueben, May. 1998, pp. 711-716
[17] T. Kushida, M. Inaba, K. Ikebukuro, N. Ichioka, T.Esumi, H. Oyaizu, T.Yoshimura, T. Nagahama, K.Nakamura, T. Ito, H. Hisha, K. Sugiura, R.Yasumizu, H. Iida, and S. Ikehara: “Comparison of Bone Marrow Cells Harvested from Various Bones of Cynomolgus Monkeys at Various Ages by Perfusion or Aspiration Methods: A Preclinical Study for Hu-man BMT,” Stem Cells, Vol. 20, No.2 (2002) pp. 155-162
[18] A.M. Marmont: “Immune ablation followed by allogeneic or autologous bone marrow transplantation: a new treatment for severe autoimmune diseases? ,” Stem Cells Vol.12, No.1 (1994) pp. 125-135
[19] J. Kohyama, H. Abe, T. Shimazaki, A. Koizumi, K. Nakashima, S. Gojo, T. Taga, H. Okano, J. Hata, and A. Umezawa: “Brain from bone: efficient "meta-differentiation" of marrow stroma-derived mature osteoblasts to neurons with Noggin or a demethylating agent.,” Differentiation Oct; 68 (4-5) (1996) pp. 235-44
[20] P. Bianco, M. Riminucci, S. Gronthos, and P.G. Robey: “Bone marrow stromal stem cells: nature, biology, and potential applications ,” Stem Cells, 19(3) (2001) pp. 180-92
[21] S.J. Forman, K.G. Blume, and E.D. Thomas, Bone Marrow Transplan-tation. Boston: Blackwell Scientific Publications (1999) ch. 21, pp. 259-269
[22] J. Jaroscak: “A phase 1 trial of augment of unrelated umbilical cord blood transplantation with ex-vivo expanded cells,” Blood Suppl.1, (1998) pp. 646a
[23] X. Sui: “gp130 and c-Kit signalings synergize for ex vivo expansion of human primary hematopoietic progenitor cells”, Proc. of Natl. Acad. Sci. USA 92 (1995) pp. 2859-2863
[24] G.S. Chirikjian and J.W. Burdick: “Kinematically Optimal Hy-per-Redundant Manipulator Configurations”, IEEE Trans. on Robotics and Automation, Vol.11, No.6 (1995) pp.794-806
[25] K. Suzumori, S. Iikura and H. Tanaka: “Development of Flexible Mi-croactuator and Its Applications to Robotic Mechanisms”, Proc. of ICRA, Sacramento, April. 1991, pp.1622-1627
[26] J.F. Wilson and U. Mahajan: “The Mechanics and Positioning of Highly Flexible Manipulator Limbs”, ASME J. of Mechanisms, Transmissions, and Automation in Design, Vol.111 (1989) pp.232-237
Kota Ohashi (S’98) was born in Tokyo, Japan, on December 7, 1972. He received the B.E., M.E. and Ph.D. degrees in precision machinery engineering from the University of Tokyo, Tokyo, Japan in 1997, 2000 and 2003, respectively.
He is currently a postdoctoral student of Advanced Therapeutic and Rehabilitation Engineering labora-tory (ATRE Lab.), Graduate School of Information Science and Technology, the University of Tokyo. His main research interests lie in devices for minima-
lly invasive surgery and mechatronics for assistive technology. Dr. Ohashi is a member of Japan Society of Computer Aided Surgery, Me-
chanical Engineers and the Robotics Society of Japan. He was awarded first prize of the paper competition 2002 from the Japan Chapter of IEEE EMBS.
Nobuhiko Hata (M’01) was born in Hyogo, Japan, on June 25, 1970. He received the B.E. degree in precision machinery engineering in 1993 from School of Engineering, The University of Tokyo, Tokyo, Japan, and the M.E. and the Doctor of En-gineering degrees in precision machinery engineering in 1995 and 1998 respectively, both from Graduate School of Engineering, The University of Tokyo, Tokyo, Japan. He was a research fellow from 1995 to 2000 and
then became Instructor in Radiology in 2000, both at Department of Radiology, Brigham and Women’s Hospital, Boston, MA. Since April of 2001, he has been Assistant Professor at Department of Mech-ano-Informatics, Graduate School of Information Science and Technology, The University of Tokyo, Tokyo, Japan. His research focus has been on medical image processing and robotics in image-guided surgery. His achievements include neurosurgical navigation combined with ultrasound imaging, surgical robot for use in magnetic resonance imager, and motion-adaptable surgical robot for any intra-operative imager. Since he joined Department of Mech-ano-Informatics, The University of Tokyo, his research area expanded to ge-neric surgical robots not necessary for use with imaging system.
Dr. Hata is a member of various processional societies including International Society of Computer Aided Surgery, IEEE Engineering in Medicine and Bi-ology Society, Japan Society of Computer Aided Surgery, American Associa-tion of Promotion of Science.
Tomoko Matsumura was born in Osaka, Japan, on August 31, 1970. She received the M.D. and Ph.D. degrees in medicine from the University of Tokyo, Japan, in 1996 and 2003, respectively. She has worked as a physician in Japan since 1996,
mainly in the hematological stem cell transplantation unit. She is currently a post-doctoral student of Department of Hematology and Oncology, Graduate School of Medicine, the University of Tokyo.
Dr.Matsumura is a member of Japanese Society of Internal Medicine, Japanese Society of Hematology, and Japanese Society of Clinical Hematology.
Toru Ogata was born in Tokyo, Japan, on February 17, 1970. He graduated and received the M.D. degree in 1995 from the School of Medicine, The University of Tokyo, Tokyo, Japan, where he is currently working toward the Ph.D. degree in the Graduate School of Medicine.
He had a clinical career in Tokyo, Japan, for several years. His main research is related to regeneration of central and peripheral nervous systems. Dr. Ogata is a member of the Japanese Orthopaedic
Association and Society for Neuroscience of U.S.A.
Naoki Yahagi was born in Yokohama, Japan, on January 27, 1956. He received the M.D. from School of Medicine, Kanazawa University, Japan, in 1981, and the Degree of Medical Science from School of Medicine, Shiga University of Medical Science, Japan, in 1991. He was a Professor in the Graduate School of Frontier
Science and Faculty of Engineering, The University of Tokyo from 1999 - 2001. He is currently a Professor in the Department of Emergency and Critical Care Medi-
cine, Graduate School of Medicine, The University of Tokyo. His current research interests have focused on the establishment of “Vital Care
Network System” which is the system for monitoring a large mass of citizens’ vital signs continuously using non-invasive wearable monitors for early alert of physical disorders and covered by emergency medical system.

Ohashi, K.; Hata, N.; Matsumura, T.; Ogata, T.; Yahagi, N.; Sakuma, I.; Dohi, T., Stem cell harvesting device with passive flexible dr illing unit for bone marrow transplantation. IEEE Transactions on Robotics and Automation, 19(5), 810- 817, 2003 ATRE Lab, Univ. of Tokyo
9
Ichiro Sakuma received the B.S., the M.S., and the Ph.D. degrees in precision machinery engineering from the University of Tokyo, Tokyo, Japan, in 1982. 1984, and 1989, respectively. He was Research Associate at the Department of
Precision Machinery Engineering in Faculty of Engi-neering, the University of Tokyo from 1985 to 1987. He was an Associate Professor at the Department of Applied Electronic Engineering, Tokyo Denki Uni-versity, Saitama, Japan, from 1991 to 1999 and an As-
sociate Professor at the Institute of Environmental Studies Graduate School of Frontier Sciences, the University of Tokyo, from 1999 to 2001. He is currently a Professor at the Institute of Environmental Studies Graduate School of Frontier Sciences, the University of Tokyo. His research interests are in biomedical instrumentation, simulation of bio-
medical phenomena, computer-assisted intervention, and surgical robotics.
Takeyoshi Dohi, Dr. Eng, received the M. Eng. and the Dr. Eng. degrees in precision machinery engi-neering from the University of Tokyo, Tokyo, Japan in 1974 and 1977 respectively. After brief research fellowship in Institute of Medical Science, The Uni-versity of Tokyo, he joined Tokyo Denki University, Tokyo, Japan in 1979 as a Lecturer and then became Associate Professor in 1981.From 1981 to 1988, he was Associate Professor of The University of Tokyo in precision machinery engineering. Since 1988 he holds full Pro-
fessor position in The University of Tokyo, where he presently is Professor in information science and technology. His research interests include com-puter-aided surgery, rehabilitation robotics, artificial organs, and neuro-in-formatics. He is a board member of numerous domestic society and international pro-
fessional societies including International Society for Computer Aided Surgery (ISCAS), International Union for Physical and Engineering Sciences in Medi-cine (IUPESM), and Medical Image Computing and Computer Assisted In-tervention (MICCAI). He was also the General Chair of MICCAI2002 held in Tokyo, Japan in September, 2002.