노인환자에서약물처방의실제 - kaim.or.kr 광일.pdf · pdf file•...
TRANSCRIPT

환 에 약물처방 실
- 심혈 계 약물 -
울 학 과 학 내과학 실당 울 학 병원 내과, 료 터
내과학회 2009-10-24

례 1. 72 여 환
• 72 여 환 가 어지럼 래 내원하 다. 당뇨병 경 혈당강하제 복용 5 전 TIA
원한 병 었다. 혈압 좌 상 에150/88 mmHg, 우 상 에 140/80 mmHg정되었다.
– Q1> 환 혈압 얼마 가?
– Q2> 환 에 우 적 추천되 혈압약제 ?
– Q3> 혈압 조절 목 ?

• Establishing blood pressure levels– Pseudohypertension, “White-coat hypertension”에주의
– Peripheral vascular disease: 양측혈압차이
• Identifying secondary causes of hypertension– 특히, Renovascular HT
• Evaluating the overall cardiovascular risk – Risk factors
– Target organ damage
– Concomitant diseases or accompanying clinical conditions
Diagnostic evaluation

Optimal anti-hypertensive drug in elderly
• Potent BP lowering effect
• Stable 24h BP control
• Once daily regimen
• Few drug-drug and/or drug-disease interaction
• Good compliance
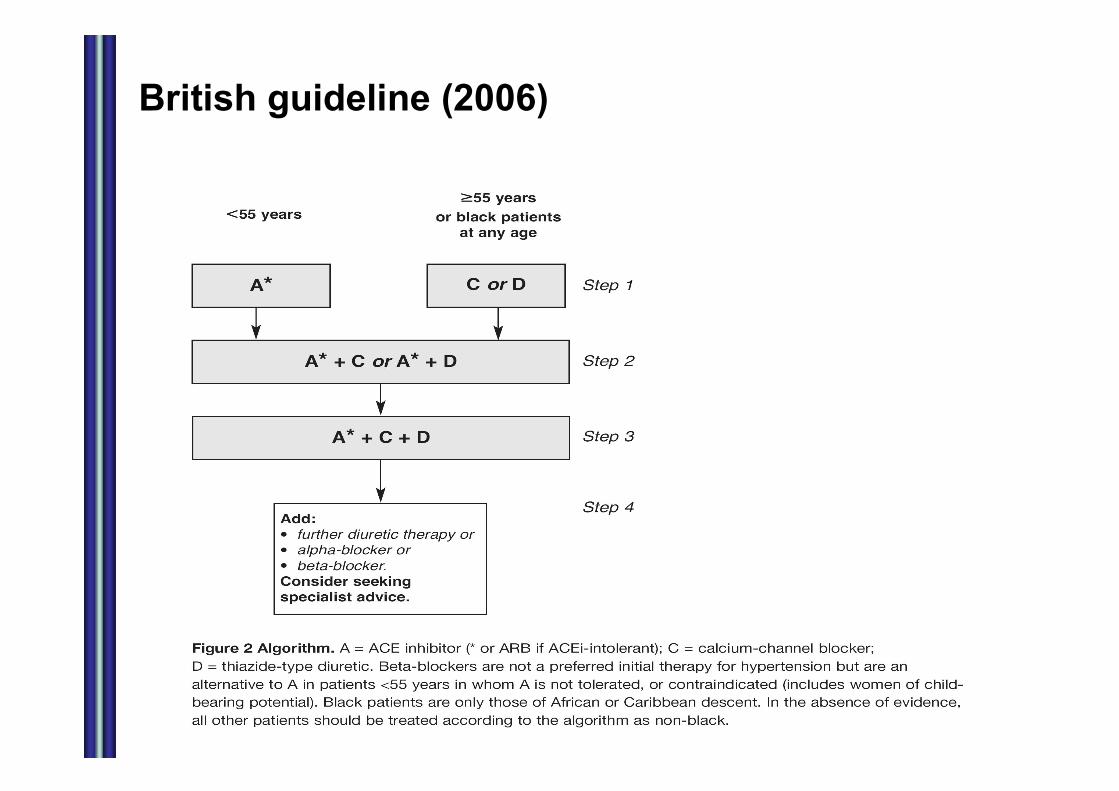
British guideline (2006)
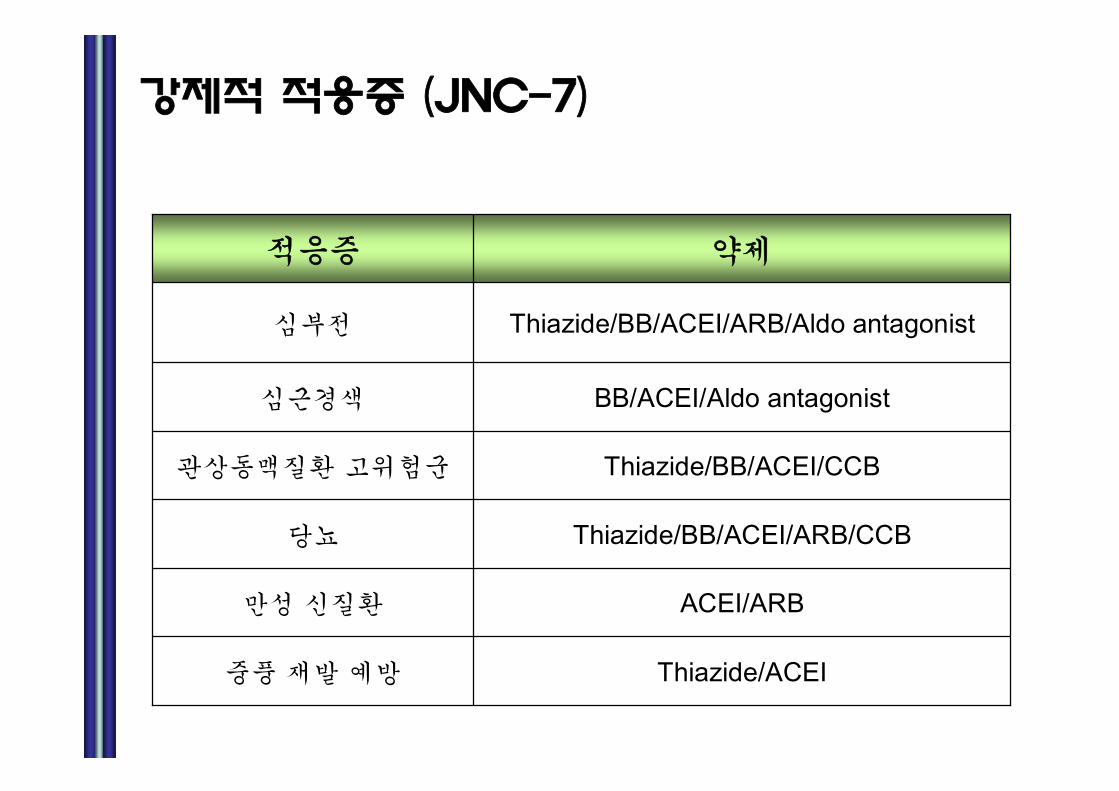
강 (JNC-7)
Thiazide/ACEI풍 재
ACEI/ARB만 신질환
Thiazide/BB/ACEI/ARB/CCB당뇨
Thiazide/BB/ACEI/CCB상동맥질환 고 험군
BB/ACEI/Aldo antagonist심근경색
Thiazide/BB/ACEI/ARB/Aldo antagonist심부
약응증

Initiation of antihypertensive treatment
ESH-ESC Guideline, Journal of Hypertension 2007, 25:1105–1187

ACE inhibitor; Better for CHD
ACE-inhibitors Calcium Channel Blockers
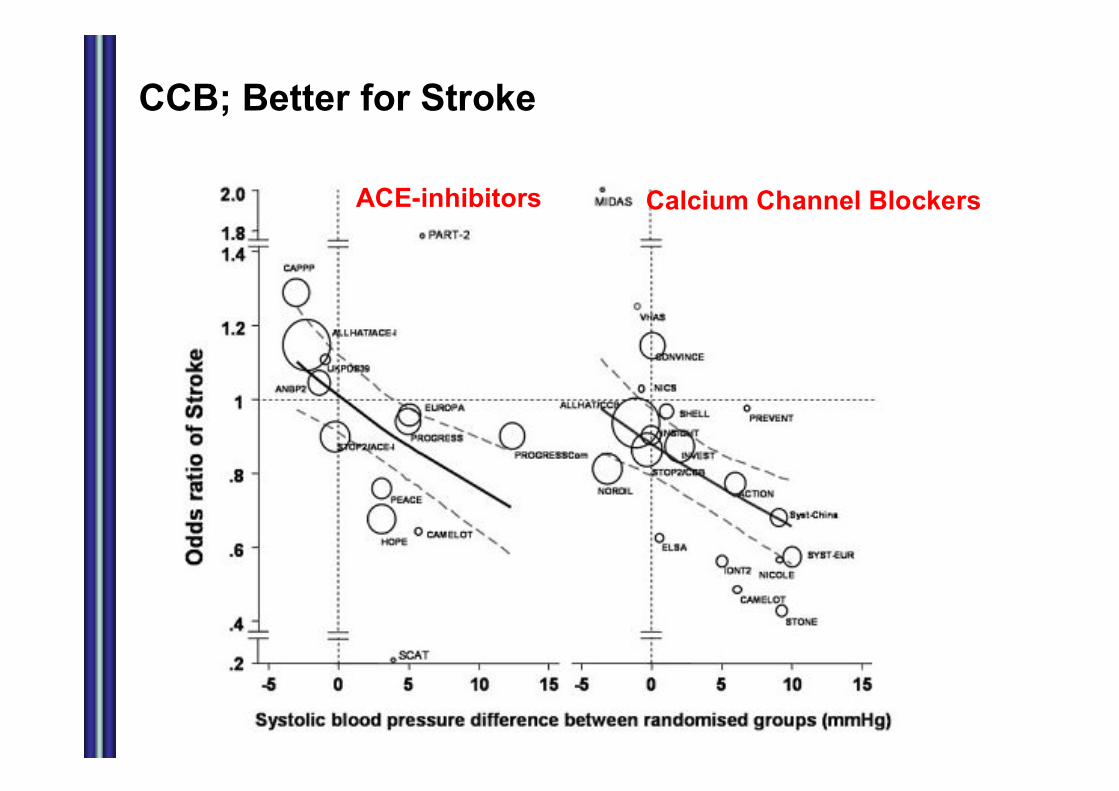
CCB; Better for Stroke
ACE-inhibitors Calcium Channel Blockers

고혈압 약물 병용 법
Diuretics
ARBs
CCBs
ACEI
b- blocker
a-blocker
DiureticsDiuretics
CCBsCCBs
bb-- blockerblocker
ACEI, ACEI, ARBsARBs

Target Blood Pressure in the Elderly
• JSH 2004 < 140 / 90 mmHg
(temporary target: < 150 / 90 mmHg for old elderly)
• ESH/ESC 2007 < 140 / 90 mmHg
• JNC 7 (2003) < 140 / 90 mmHg

Cerebral blood flow; Range of autoregulation
Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2004)

Therapeutic Guideline for Elderly HT
<150 mmHg<150 mmHg<140 mmHgSBP
<90 mmHg<90 mmHg<90 mmHgDBP
80~70~60~AgeTarget BP
Life style modification
Ca Antagonist or ACEI/ ARB
Diureticsor ACEI/ ARB
Ca Antagonistor Diuretics
Ca Antagonist + ACEI/ARB + Diuretics
2~3 Months
2~3 Months
Calcium Antagonist ACEI/ ARBDiuretics

례 2-(1). 75 여 환
• 75 여 환 가 조절되지 않 고혈압 래 방 하다. 20 전 고혈압 진단 받고 슘 항제 조절되었
나 최근 혈압 180/100mmHg 상 정되 호 곤란상 주 나타난다고 한다.
– Q1> 환 에 고 해야 할 상황 ?
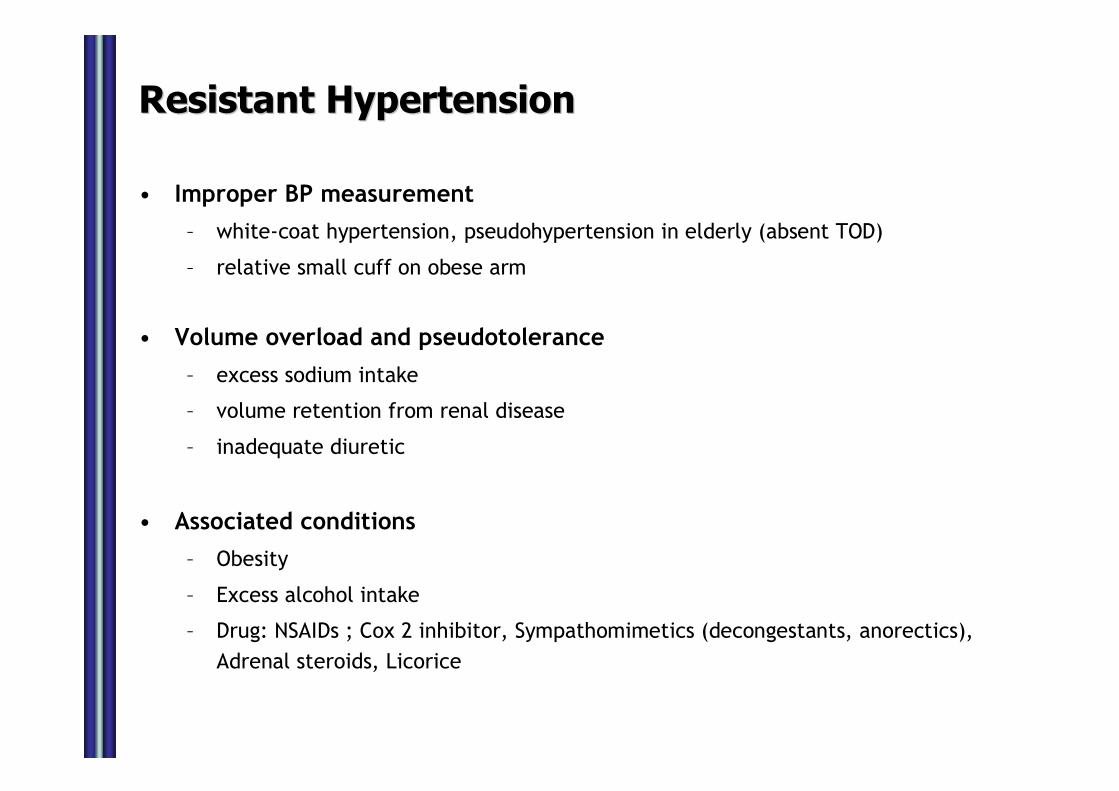
Resistant HypertensionResistant Hypertension
• Improper BP measurement
– white-coat hypertension, pseudohypertension in elderly (absent TOD)
– relative small cuff on obese arm
• Volume overload and pseudotolerance
– excess sodium intake
– volume retention from renal disease
– inadequate diuretic
• Associated conditions
– Obesity
– Excess alcohol intake
– Drug: NSAIDs ; Cox 2 inhibitor, Sympathomimetics (decongestants, anorectics),
Adrenal steroids, Licorice

례 2-(2). 72 여 환
• 혈압조절 해 ACE inhibitor 추가하고 2주 후 래 방시 혈압 120/70 mmHg 조절되었 나 혈액검사에BUN/Cr 40/2.7, potassium 5.8mmol/L 상승되었다.
– Q2> 환 에게 적절한 조 심되 진단 ?

Renovascular hypertension
례 3. 80 남 환
• 80 남 환 가 어지럼 과 반복적 낙상래 방 하 다. 5 전 항고혈압제
복용하고 었 혈압 조절되었다고한다.
– Q1> 환 에 고 해야 할 상적 진단 ?
– Q2> 환 최근 억 저하되고 변 조절하 능 저하되고 우울한 낌 주 낀다고 한다. 환 에 찰되 혈압 변화가 러한상과 가?
Common problem in elderly HT patients
• Orthostatic hypotension
• Postprandial hypotension
• White-coat hypertension
• Masked hypertension
• Fluid, electrolyte imbalance
• Polypharmacy


Postural hypotension
• More frequent in older patients
– with systolic HT, DM
– those taking diuretics, venodilators (nitrates, alpha-blocker,
sildenafil-like drug), and some psychotropic drug
• BP check in upright position
• Avoid volume depletion and rapid dose titration
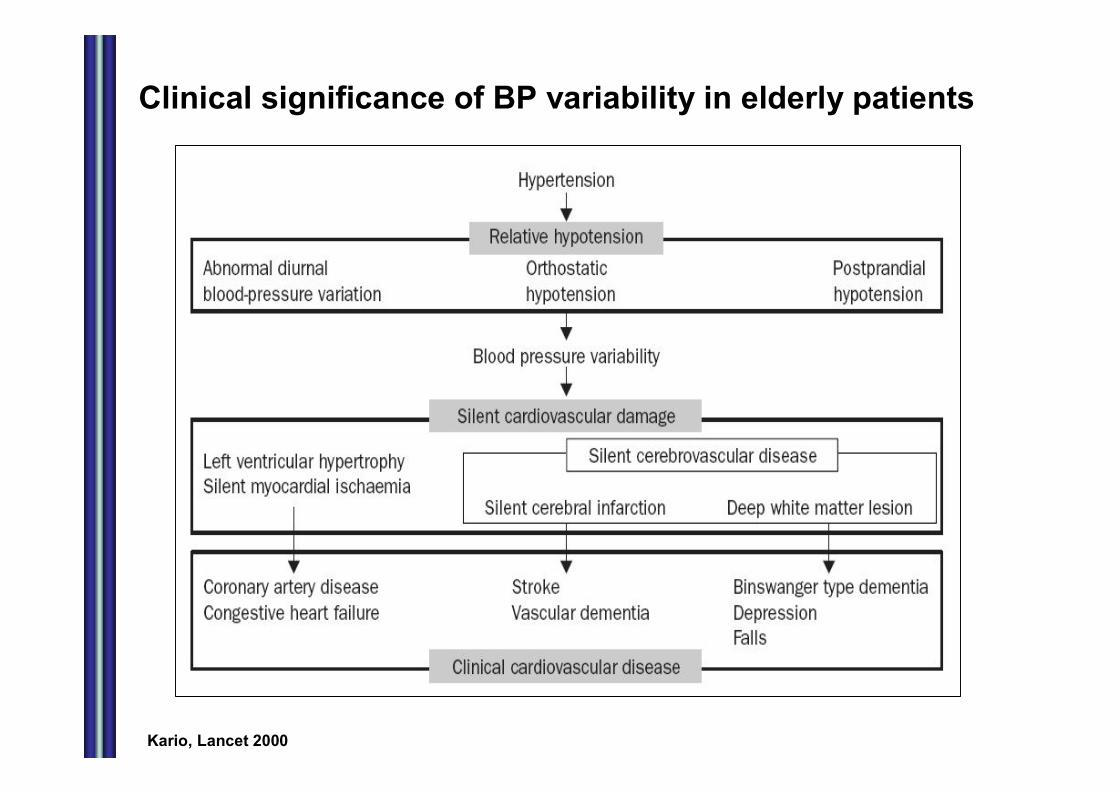
Clinical significance of BP variability in elderly patients
Kario, Lancet 2000

Cerebral white matter change in elderly
• Cerebral ischemic microangiopathy
• Abnormal cerebral blood flow
• Reduced perfusion of watershed area
Periventricular & subcortical white matter lesion
Disruption of frontal-subcortical circuits
Fall Cognitive decline and
dementia
Depression Urge urinary incontinence
Kuo & Lipsitz, Gerontology 2004
Gait disturbance
Executive dysfunction
Loss of motivation
and initiation
Hyper-reflexic
detrusormuscle
Cardiovascular risk factor
Aging

례 4. 86세남자환자
• 고혈압, 지천식 로 래 진료 환 가 최근악화 호흡곤란 로 래 내원하 다. 래에 측 한혈압 138/76 mmHg, 심박수 112 회/ 었심 도 검사에 동 빈맥, 심초 파 검사에 EF 40%, Hypokinesia in LAD territory 찰 었다.
• 현재 사용하고 약 CCB, Diuretics, Theophylline, steroid inhaler 등 었다.
– Q1> 환 에 베타차단제 추가 사용하여야 하 가?
Beta blockers in HF
• b recepotors
1) b1 : heart (increase in contractility, heart rate),kidney
2) b2 : lung (bronchodilatation), vessel (vasodilatation)
• Interrelation of RAA system and SNS
• Hypotheses for beneficial effect of beta blocker
1) norepinephrine-myocardial toxicity theory
2) downregulation of beta receptor theory
3) tachycardia-dependent cardiomyopathy
theory

SNS/RAS Activation Leads Directly to Impaired Cardiac Function
Adapted from Packer M. Prog Cardiovasc Dis. 1998;39(suppl I):39–52.
CNS sympathetic outflow
b1-receptors
Cardiac sympathetic activity
b2-receptors
a1-receptors
Activationof RAS
VasoconstrictionSodium retention
Myocyte hypertrophy, dilation,ischemia, arrhythmias, death
Disease progression
Sympathetic activity tokidneys + blood vessels
Beta-Blockers: All the Same?
• Potency and duration of action
• Cardioselectivity (Beta-1 selectivity)
• Intrinsic sympathomimetic activity
• Lipid solubility

Not all beta-blockers are equal !!
29
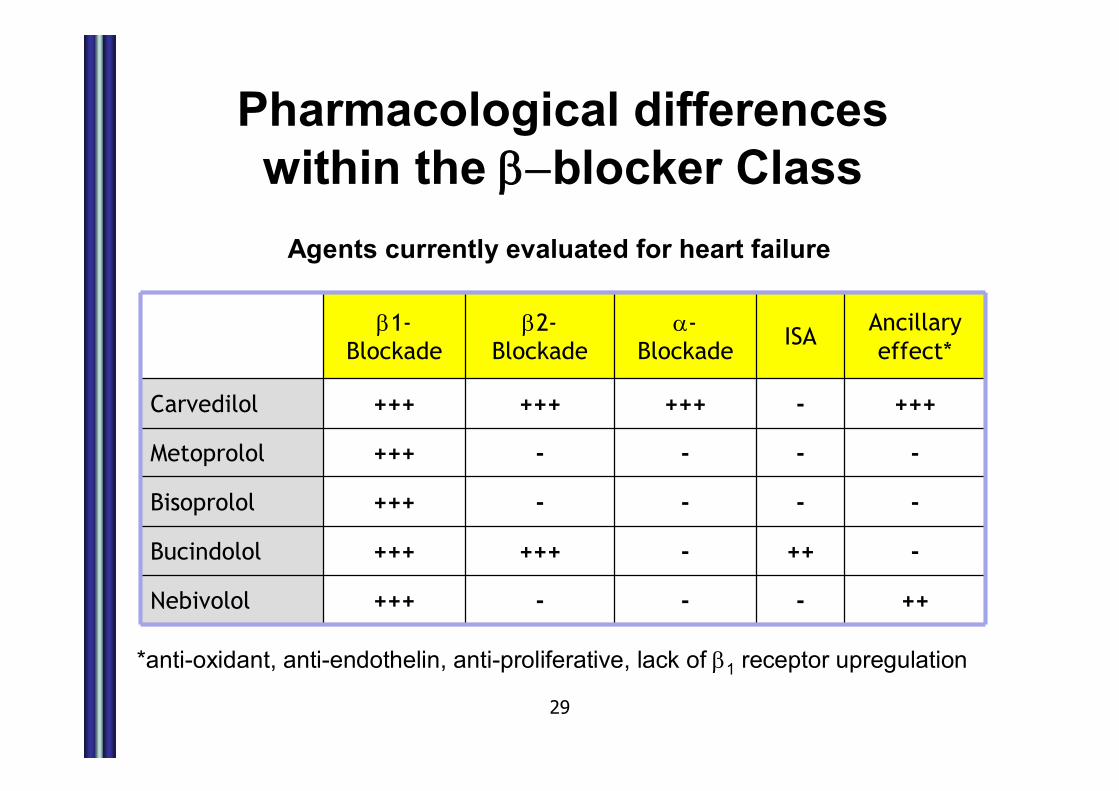
Pharmacological differences within the b-blocker Class
*anti-oxidant, anti-endothelin, anti-proliferative, lack of b1 receptor upregulation
b1-Blockade
b2-Blockade
a-Blockade
ISAAncillary effect*
Carvedilol +++ +++ +++ - +++
Metoprolol +++ - - - -
Bisoprolol +++ - - - -
Bucindolol +++ +++ - ++ -
Nebivolol +++ - - - ++
Agents currently evaluated for heart failure

례 5. 90세남자환자
• 심계항진 로 주 로 내원하 다. 고혈압과 당뇨병 로투약 환 로 20 측 상지 마비
병력 었다.
• 심 도 검사에 심방 동 견 찰 었고 심초파 검사에 심방 확 상 견 없었다.
– Q1> 환 에 항 고 료가 필 한가?
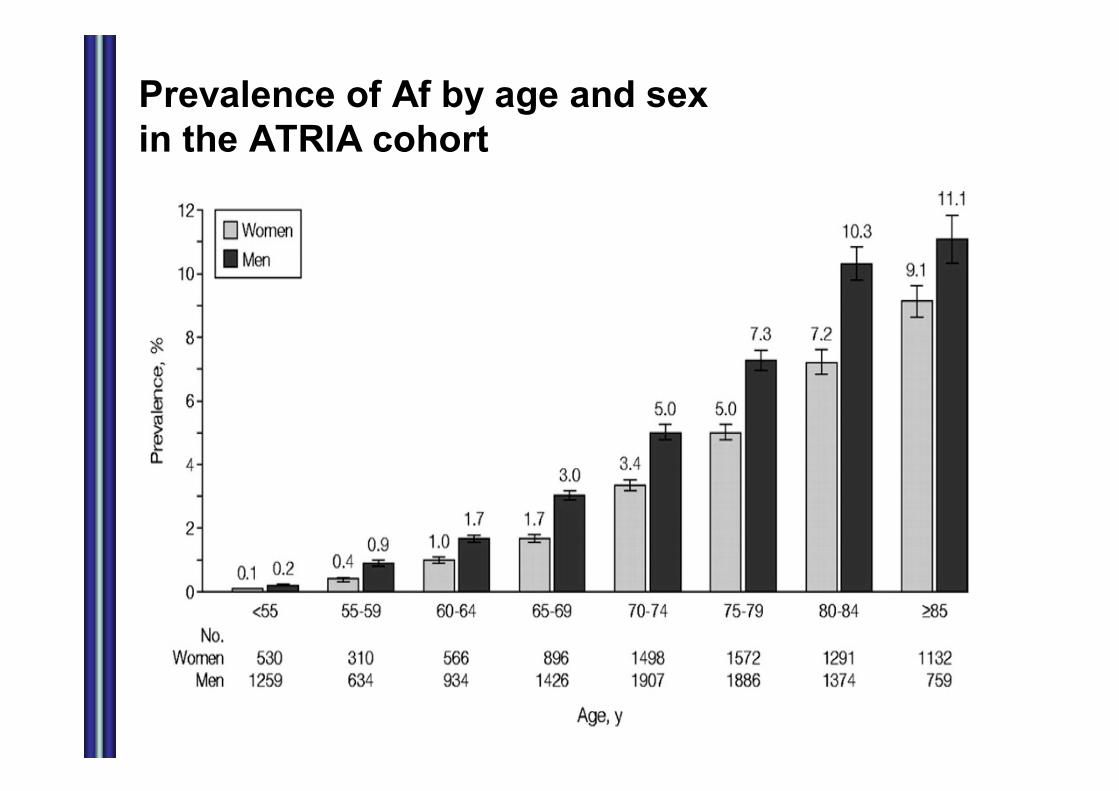
Prevalence of Af by age and sex in the ATRIA cohort

심방 동 치료
• Stroke prevention• Heart rate control• Rhythm control
• Risk stratification schemes can help guide the anticoagulation decision, although warfarin’s benefits generally outweigh its risks
• Rate and rhythm control result in similar outcomes; rate control is usually the initial therapy for elderly patients.


CHADS2 scores
• Congestive heart failure
• Hypertension
• Age 75
• Diabetes mellitus
• prior Stroke or transient ischemic attack

CHADS2 scores & Stroke risk

Warfarin vs aspirin for stroke prevention in elderly patients with Af
Mant et al, Lancet 2007; BAFTA Study
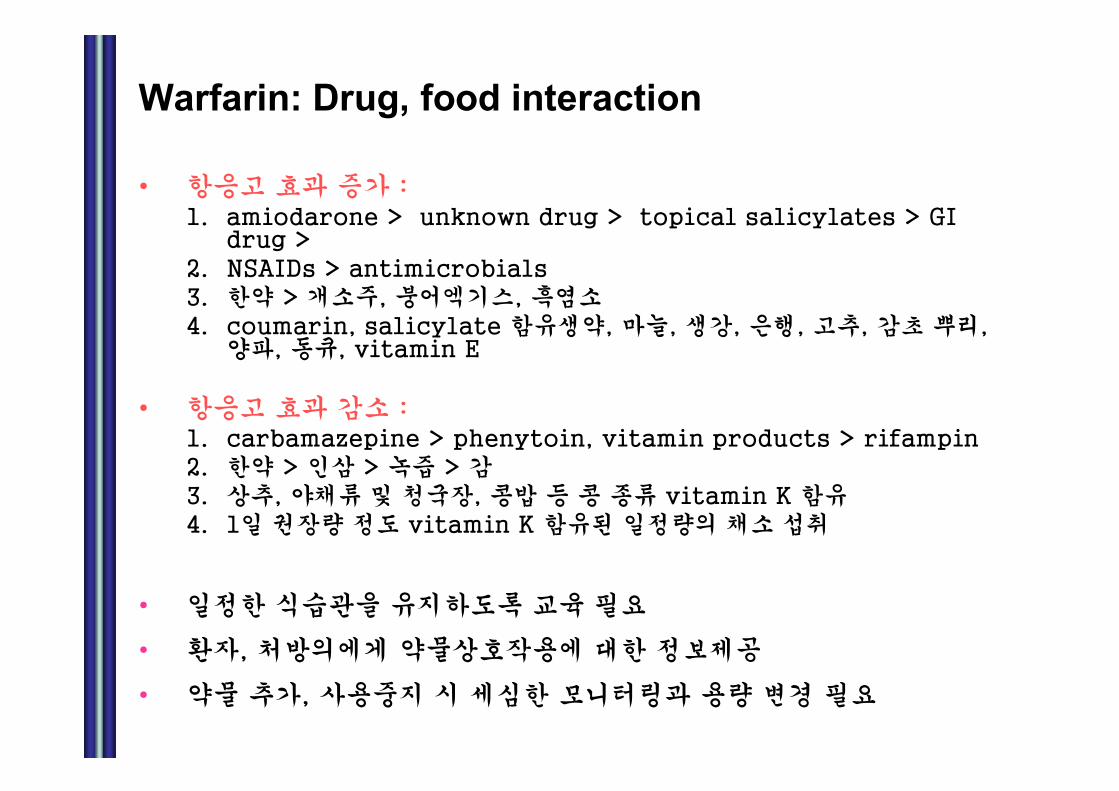
Warfarin: Drug, food interaction
• 항응고 효과 가 :1. amiodarone > unknown drug > topical salicylates > GI
drug > 2. NSAIDs > antimicrobials 3. 한약 > 개 주, 어엑기스, 흑염4. coumarin, salicylate 함유생약, 마늘, 생강, 은행, 고추, 감초 뿌리,
양파, 동큐, vitamin E
• 항응고 효과 감 : 1. carbamazepine > phenytoin, vitamin products > rifampin2. 한약 > 인삼 > 녹 > 감3. 상추, 야채류 및 청 장, 콩밥 등 콩 종류 vitamin K 함유4. 1일 장량 정도 vitamin K 함유 일정량의 채 취
• 일정한 식습 을 유 하도록 육 필
• 환자, 처방의에게 약물상호작 에 대한 정보제공
• 약물 추가, 사 시 심한 모니터링과 량 변경 필

례 6. 78 여 환
• 고혈압 3 째 슘 항제 thiazide 뇨제혈압조절 78 여 환 가 내원하 다. 2회정한 평균 혈압 160/90 mmHg 었 2달 전처방 받 혈압약 많 남았다고 한다.
• 최근 골 절염 악화 진통제 복용하 경우가 많았 혈압약 었다고 하나 복용하 약많아 확실하지 않다고 한다.
– Q1> 환 에 충 한 혈압 조절 원 생각되것 ?
– Q2> 혈압약 량 또 추가 고 해야 하 가?
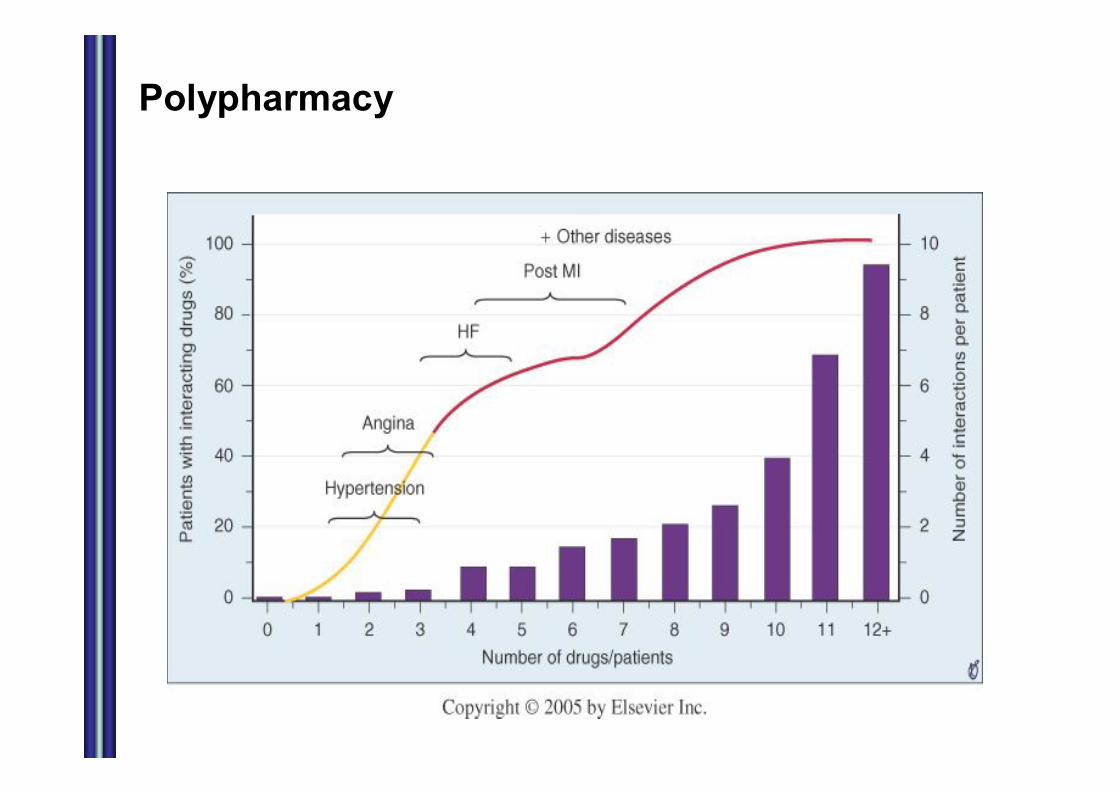
Polypharmacy

Drug therapy in elderly
노인성 환
약물 사의변화
노화
다약제복(Polypharmacy)
약물상호작
Adverse DrugReaction
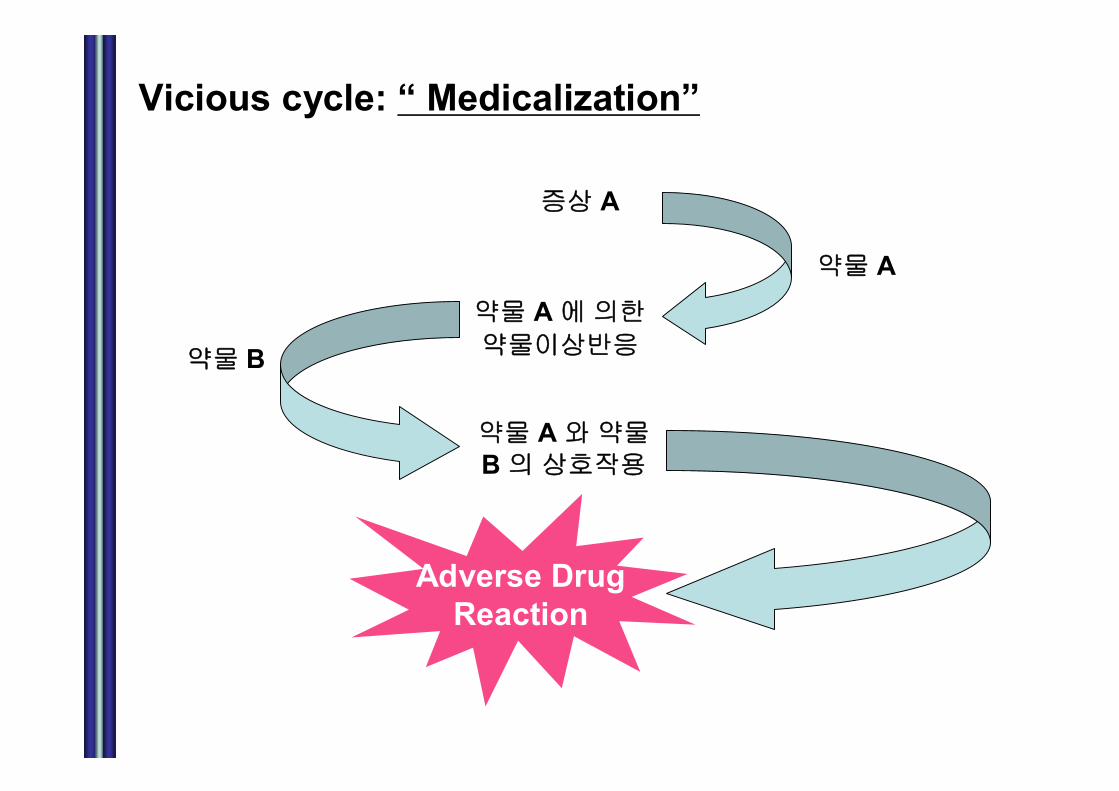
Vicious cycle: “ Medicalization”
상 A
약물 A
약물 A 에의한
약물이상반응약물 B
약물 A 약물B 의상호작
Adverse DrugReaction

What are the problems with medications?
Polypharmacy
Taking medications prescribed for someone else
Forgetting Alterations in schedules and
dosages
Inappropriate discontinuation
Taking medications not currently prescribed
Overuse

Impaired Organ Function
Altered OrganResponse
Decreased HomeostaticRegulation
Altered DrugConcentrations
Adverse DrugReaction
Multiple DiseaseStates
Multiple DrugAdministration
AlteredCompliance

약물처방 반 원칙 (1)
• 비처 약 (일 의약품), 한약을 포함한 환자의 모든 복용 약 을 악한다. (환자가 외래 시 모든 복용 약
을 가 도록 한다.)
• 드시 필요한 경우에만 약 을 사용한다. 증상이 미미하거나 특이 이 없어 확한 진단을 할 없거나, 약 치료로 인한 이득이 의심스러운 경우에는 약 처 을 한다. 해당 증상이 없어진 경우에는 즉시 약을 끊는다.
• 처 하는 약에 한 약리학 특 , 잠재 해 응과독 을 악하고 있어야 한다. 약 과 능 지표를 충분히 모니터링 한다.

약물처방 반 원칙 (2)
• 소량부터 시작하고, 천천히 증량한다(“Start low & go slow”) 그러나 충분히 치료한다(Treat adequately).
• 응도를 높일 있도록 노 한다. 복용 법을 단 화하고 주 로 약 복용이 로 이루어지는지 평가해야 한다.
• 신약 사용 시에는 특히 주의한다. 노인에 신약에 한평가가 충분히 이루어지지 않아 risk/benefit ratio를알 없는 경우가 많다.
• 약 치 료 이 외 의 법 을 고 한 다 (non-drug alternatives).
Cardiovascular Regimen Characteristics Affect Adherence
• Complexity/pill burden
– Single Anti-HT pill versus two Anti-HT pills
• Dose frequency
• Side effects
• Lifestyle fit/ therapy initiation
Take Home Message !!
• Altered pharmacokinetics & pharmacodynamics
• Multiple diseases & Multiple medications
• Inadequate knowledge of drug administration
• Cognitive impairment
Risk of Drug-drug interaction & adverse drug reaction
n Have patient bring in all medications
n Ask about other providers
n Eliminate questionable medications
n Simplify regimens
n For new medications, start low and go slow, but get there!