adenokarzinom des Ösophagus und magens filechristian meyer zum büschenfelde klinikum rechts der...
TRANSCRIPT

Christian Meyer zum Büschenfelde
Klinikum rechts der Isar der Technischen Universität München
III. Medizinische Klinik und Poliklinik
Schwerpunkt: Hämatologie / Internistische Onkologie
Adenokarzinom des Ösophagus und
Magens
Neoadjuvant
Adjuvant
Palliativ
Second line
Therapiekonzepte
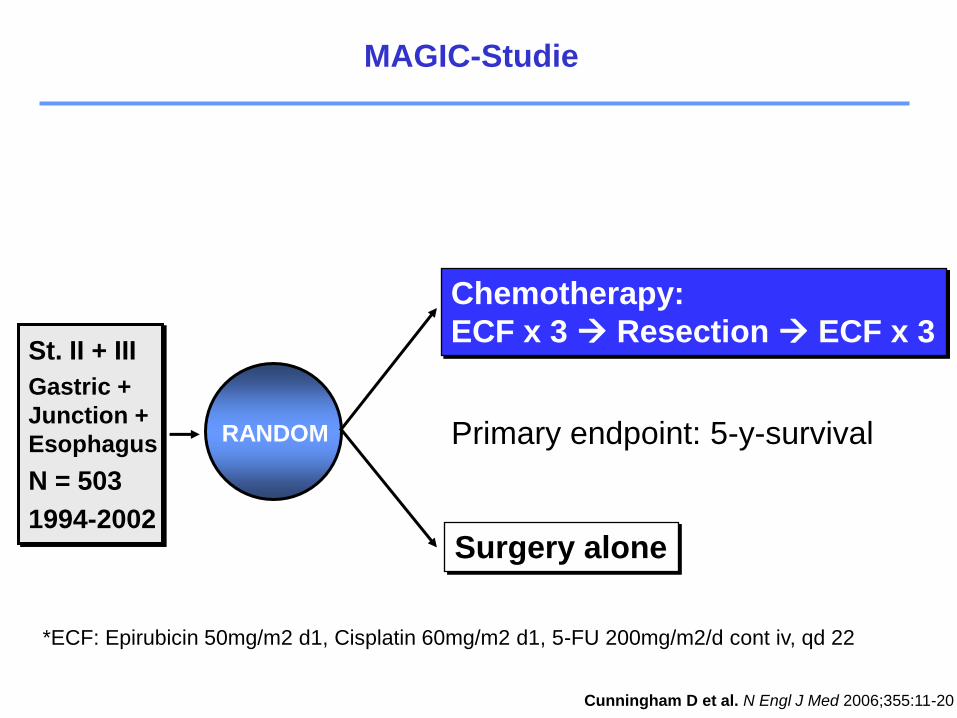
MAGIC-Studie
St. II + III
Gastric +
Junction +
Esophagus
N = 503
1994-2002
RANDOM
Chemotherapy:
ECF x 3 Resection ECF x 3
Surgery alone
Primary endpoint: 5-y-survival
*ECF: Epirubicin 50mg/m2 d1, Cisplatin 60mg/m2 d1, 5-FU 200mg/m2/d cont iv, qd 22
Cunningham D et al. N Engl J Med 2006;355:11-20
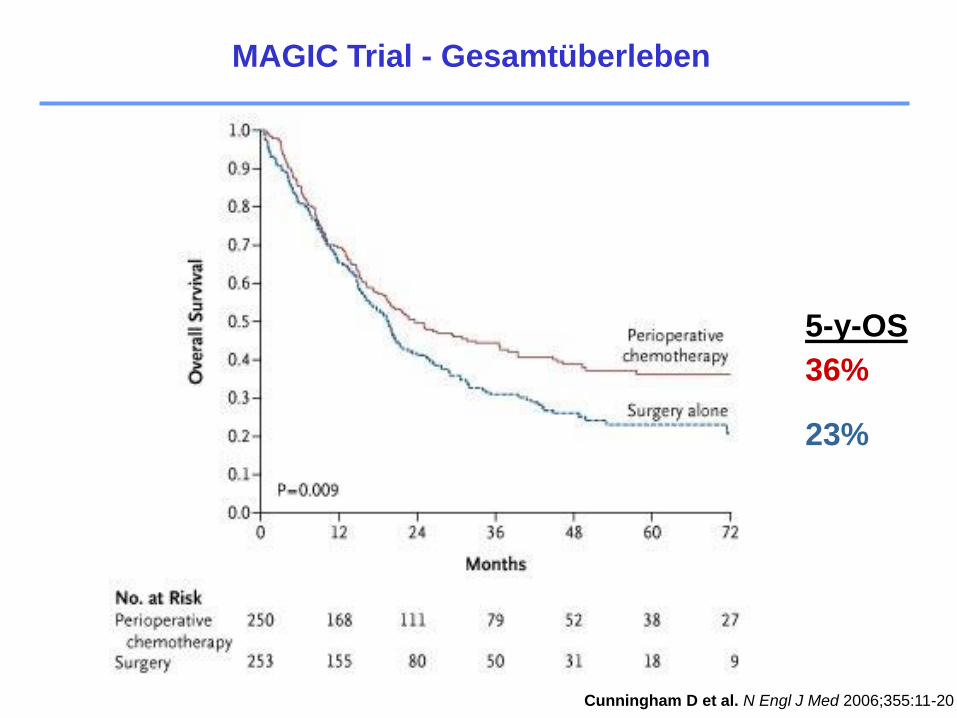
MAGIC Trial - Gesamtüberleben
Cunningham D et al. N Engl J Med 2006;355:11-20
23%
5-y-OS
36%
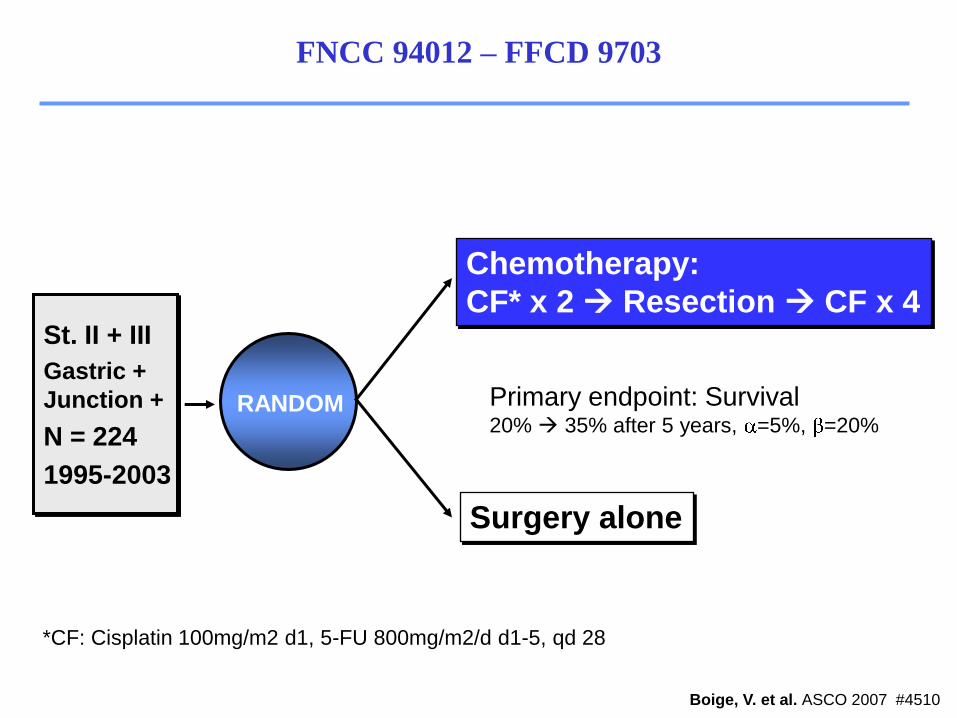
St. II + III
Gastric +
Junction +
N = 224
1995-2003
RANDOM
Chemotherapy:
CF* x 2 Resection CF x 4
Surgery alone
*CF: Cisplatin 100mg/m2 d1, 5-FU 800mg/m2/d d1-5, qd 28
Primary endpoint: Survival20% 35% after 5 years, =5%, =20%
Boige, V. et al. ASCO 2007 #4510
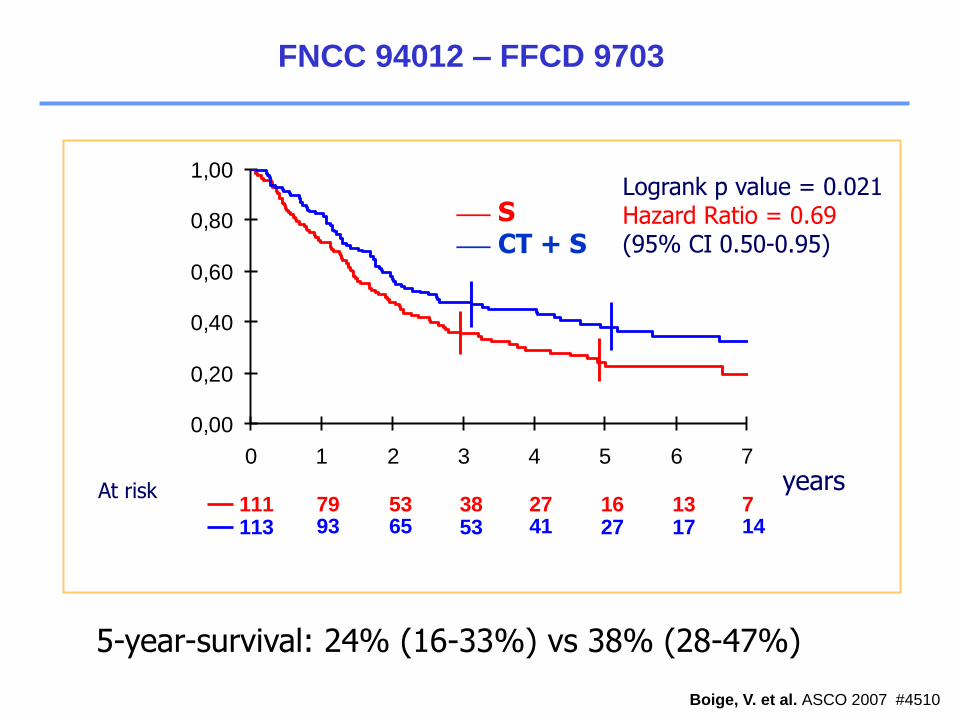
FNCC 94012 – FFCD 9703
FNCC 94012 – FFCD 9703
Boige, V. et al. ASCO 2007 #4510
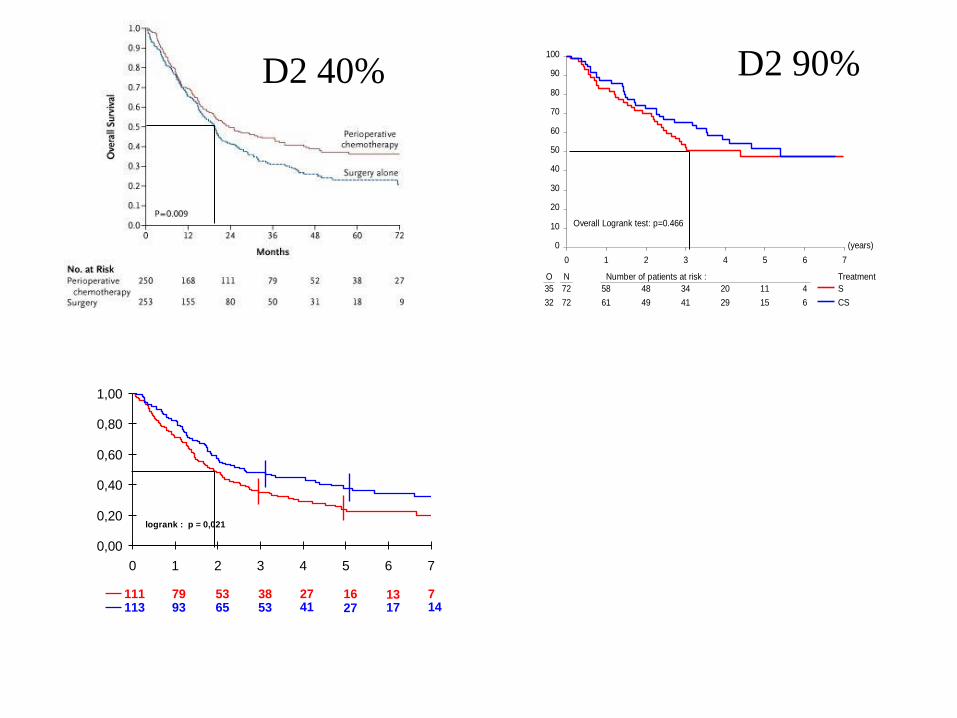
713162738537911114172741536593113
0,00
0,20
0,40
0,60
0,80
1,00
0 1 2 3 4 5 6 7
A risque
logrank : p = 0,021
___ S___ CT + S
yearsAt risk
5-year-survival: 24% (16-33%) vs 38% (28-47%)
Logrank p value = 0.021Hazard Ratio = 0.69(95% CI 0.50-0.95)
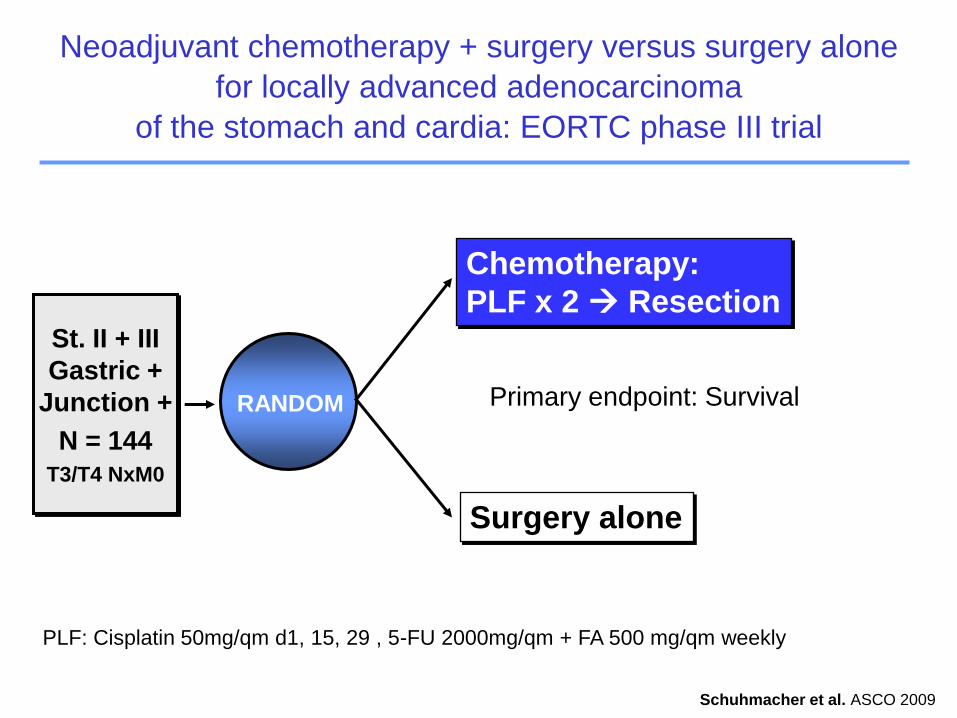
St. II + III
Gastric +
Junction +
N = 144
T3/T4 NxM0
RANDOM
Chemotherapy:
PLF x 2 Resection
Surgery alone
PLF: Cisplatin 50mg/qm d1, 15, 29 , 5-FU 2000mg/qm + FA 500 mg/qm weekly
Primary endpoint: Survival
Schuhmacher et al. ASCO 2009
Neoadjuvant chemotherapy + surgery versus surgery alone
for locally advanced adenocarcinoma
of the stomach and cardia: EORTC phase III trial
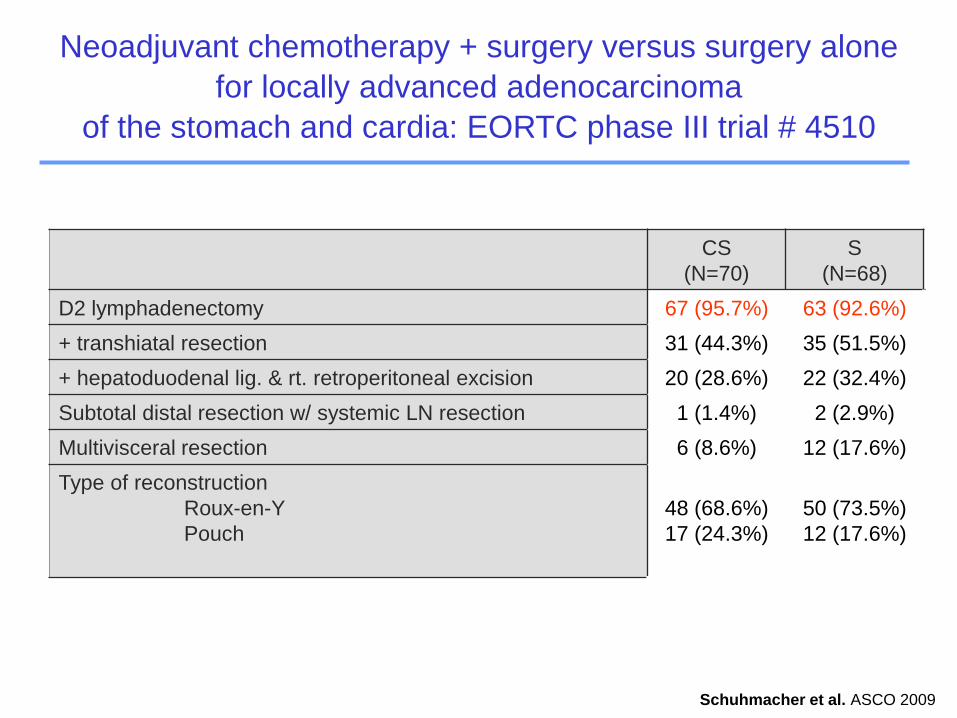
CS
(N=70)
S
(N=68)
D2 lymphadenectomy 67 (95.7%) 63 (92.6%)
+ transhiatal resection 31 (44.3%) 35 (51.5%)
+ hepatoduodenal lig. & rt. retroperitoneal excision 20 (28.6%) 22 (32.4%)
Subtotal distal resection w/ systemic LN resection 1 (1.4%) 2 (2.9%)
Multivisceral resection 6 (8.6%) 12 (17.6%)
Type of reconstruction
Roux-en-Y
Pouch
48 (68.6%)
17 (24.3%)
50 (73.5%)
12 (17.6%)
Schuhmacher, ASCO 2009; Abstract 4510
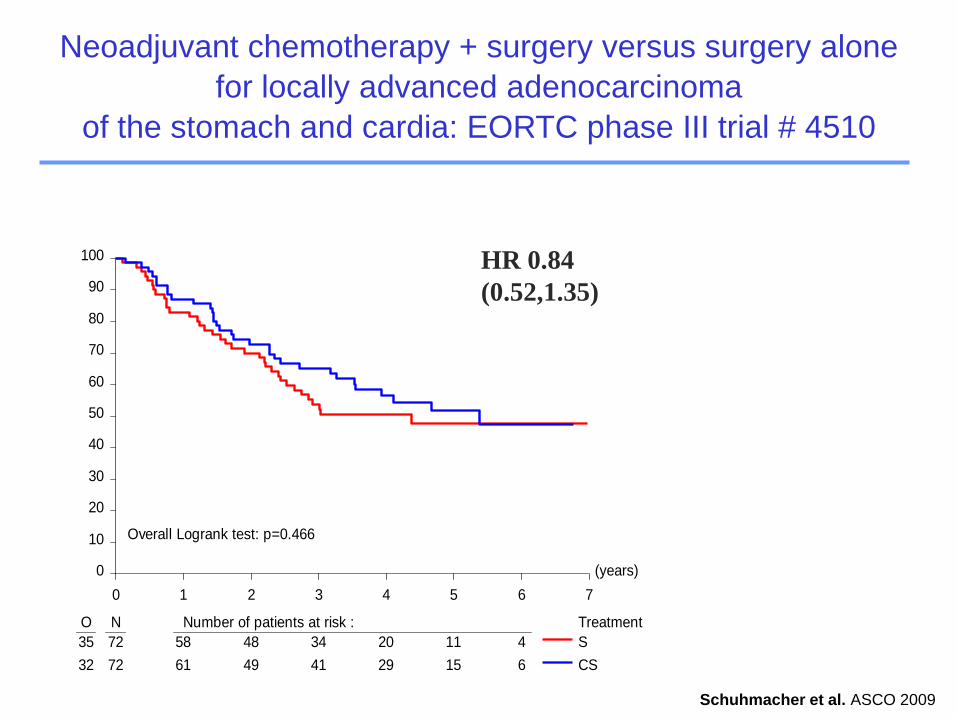
Neoadjuvant chemotherapy + surgery versus surgery alone
for locally advanced adenocarcinoma
of the stomach and cardia: EORTC phase III trial # 4510
Schuhmacher et al. ASCO 2009
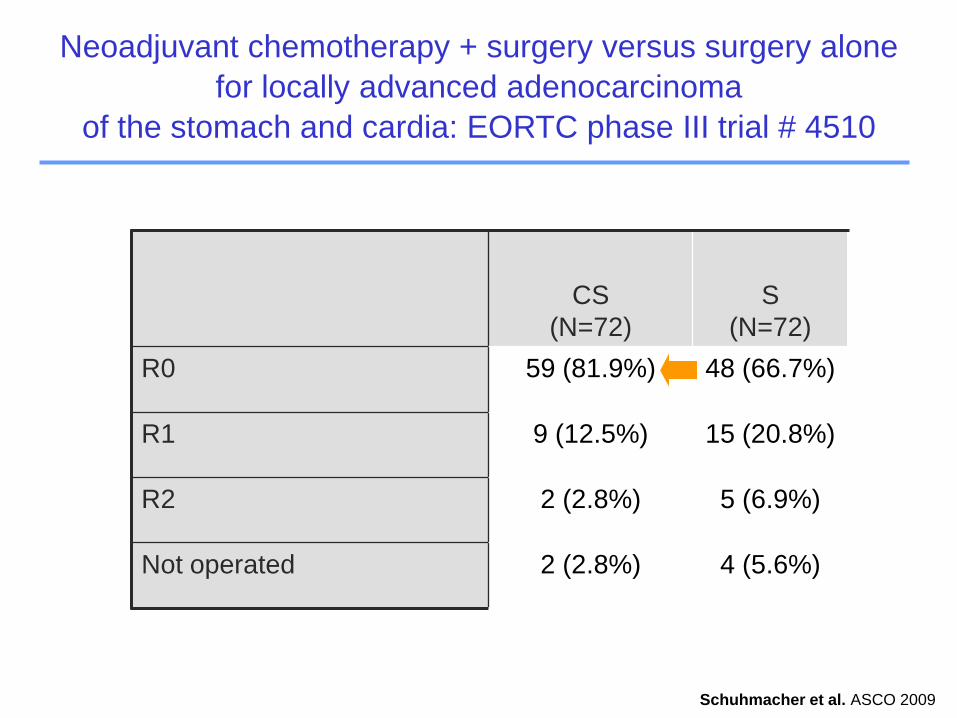
CS
(N=72)
S
(N=72)
R0 59 (81.9%) 48 (66.7%)
R1 9 (12.5%) 15 (20.8%)
R2 2 (2.8%) 5 (6.9%)
Not operated 2 (2.8%) 4 (5.6%)
Neoadjuvant chemotherapy + surgery versus surgery alone
for locally advanced adenocarcinoma
of the stomach and cardia: EORTC phase III trial # 4510
Schuhmacher et al. ASCO 2009
(years)
0 1 2 3 4 5 6 7
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment
35 72 58 48 34 20 11 4
32 72 61 49 41 29 15 6
S
CS
Overall Logrank test: p=0.466
Neoadjuvant chemotherapy + surgery versus surgery alone
for locally advanced adenocarcinoma
of the stomach and cardia: EORTC phase III trial # 4510
HR 0.84
(0.52,1.35)
Schuhmacher et al. ASCO 2009
(years)
0 1 2 3 4 5 6 7
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment
35 72 58 48 34 20 11 4
32 72 61 49 41 29 15 6
S
CS
Overall Logrank test: p=0.466
713162738537911114172741536593113
0,00
0,20
0,40
0,60
0,80
1,00
0 1 2 3 4 5 6 7
A risque
logrank : p = 0,021
D2 40% D2 90%
Intensivierte Therapie
Verbesserte Selektion
Therapiekonzepte
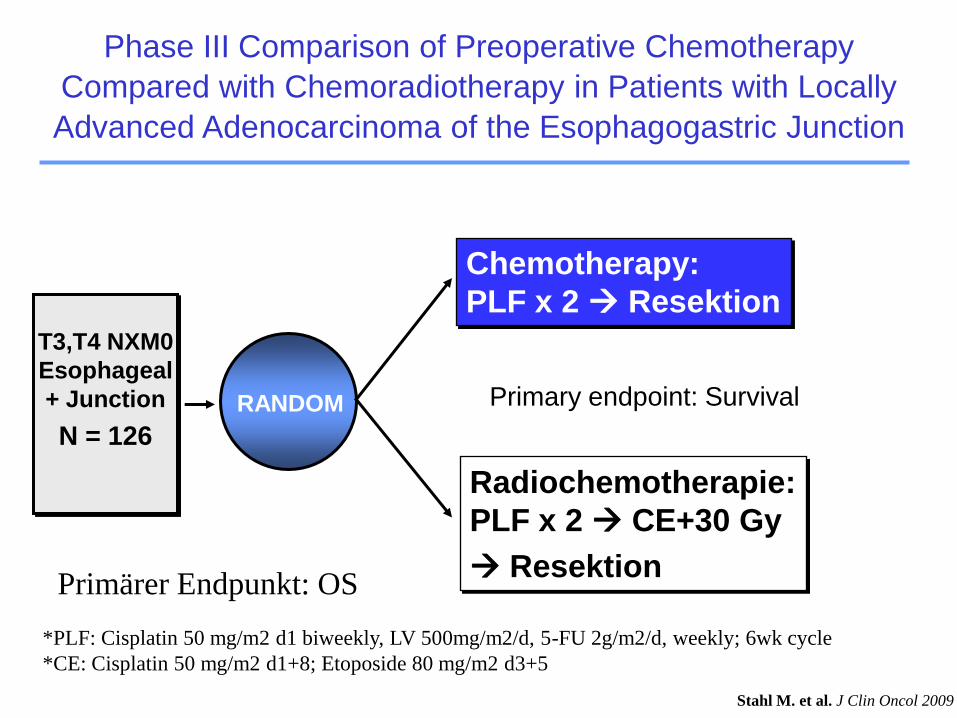
T3,T4 NXM0
Esophageal
+ Junction
N = 126
RANDOM
Chemotherapy:
PLF x 2 Resektion
Radiochemotherapie:
PLF x 2 CE+30 Gy
Resektion
Primary endpoint: Survival
Phase III Comparison of Preoperative Chemotherapy
Compared with Chemoradiotherapy in Patients with Locally
Advanced Adenocarcinoma of the Esophagogastric Junction
Stahl M. et al. J Clin Oncol 2009
Primärer Endpunkt: OS
*PLF: Cisplatin 50 mg/m2 d1 biweekly, LV 500mg/m2/d, 5-FU 2g/m2/d, weekly; 6wk cycle
*CE: Cisplatin 50 mg/m2 d1+8; Etoposide 80 mg/m2 d3+5
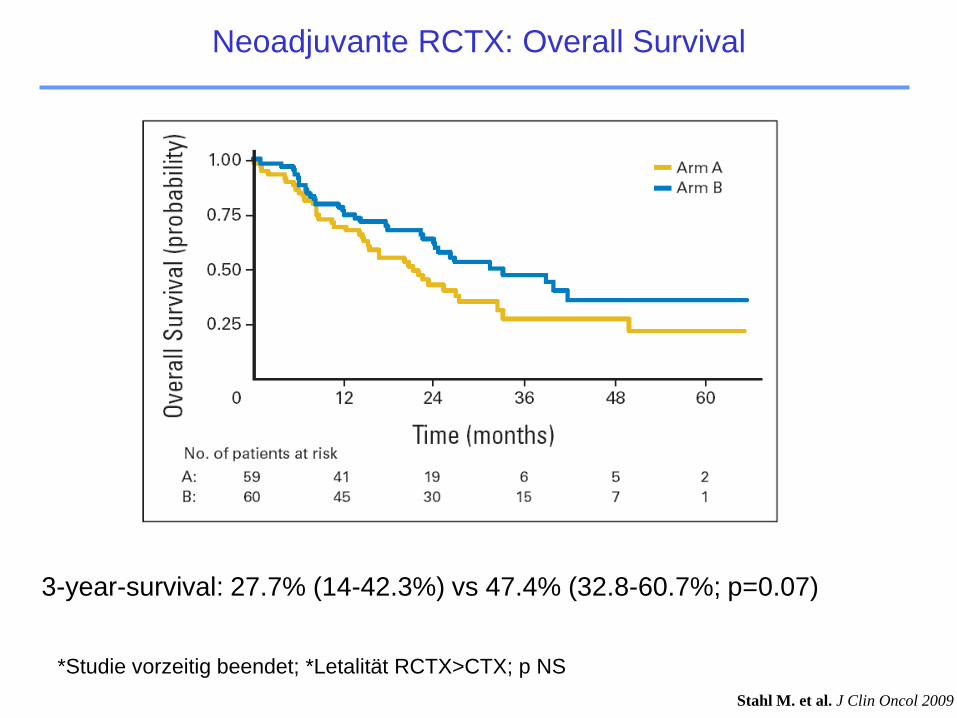
*Studie vorzeitig beendet; *Letalität RCTX>CTX; p NS
3-year-survival: 27.7% (14-42.3%) vs 47.4% (32.8-60.7%; p=0.07)
Stahl M. et al. J Clin Oncol 2009
Neoadjuvante RCTX: Overall Survival
Intensivierte Therapie
Verbesserte Selektion
Therapiekonzepte
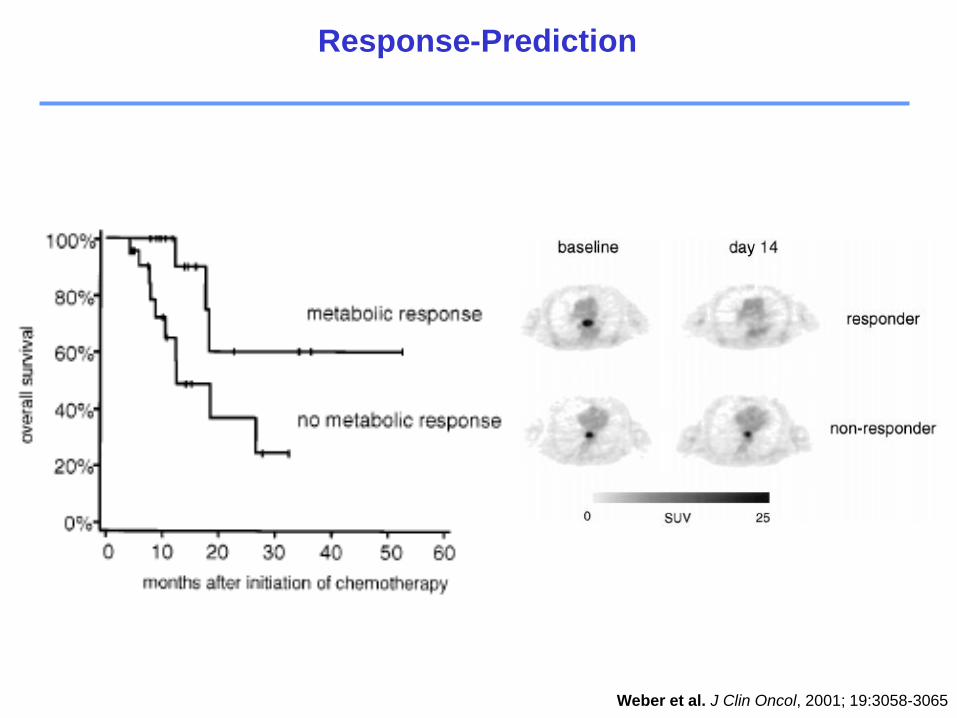
Weber et al. J Clin Oncol, 2001; 19:3058-3065
Response-Prediction
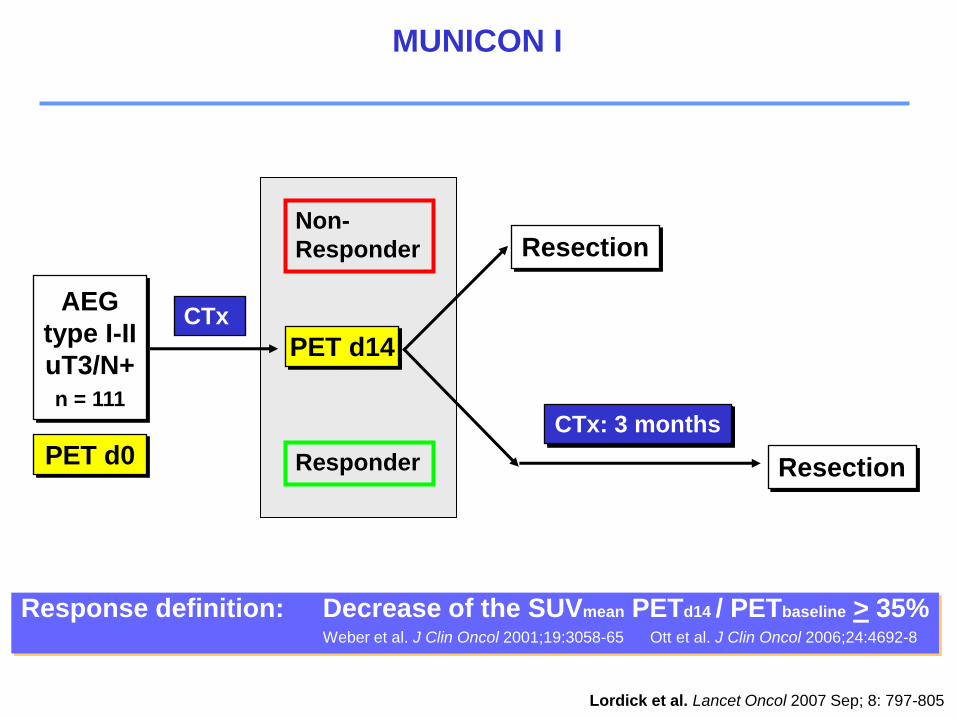
AEG
type I-II
uT3/N+
n = 111
CTx
Resection
Resection
Non-
Responder
Responder
CTx: 3 months
PET d0
PET d14
Response definition: Decrease of the SUVmean PETd14 / PETbaseline > 35%Weber et al. J Clin Oncol 2001;19:3058-65 Ott et al. J Clin Oncol 2006;24:4692-8
Lordick et al. Lancet Oncol 2007 Sep; 8: 797-805
MUNICON I
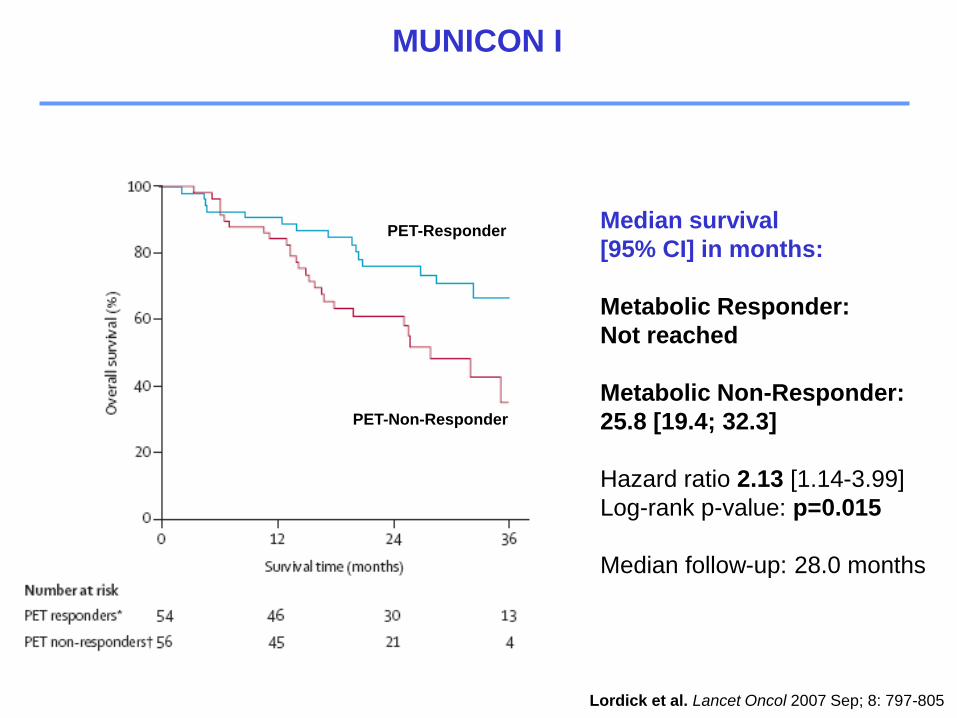
Lordick et al. Lancet Oncol 2007 Sep; 8: 797-805
Median survival
[95% CI] in months:
Metabolic Responder:
Not reached
Metabolic Non-Responder:
25.8 [19.4; 32.3]
Hazard ratio 2.13 [1.14-3.99]
Log-rank p-value: p=0.015
Median follow-up: 28.0 months
PET-Non-Responder
PET-Responder
MUNICON I
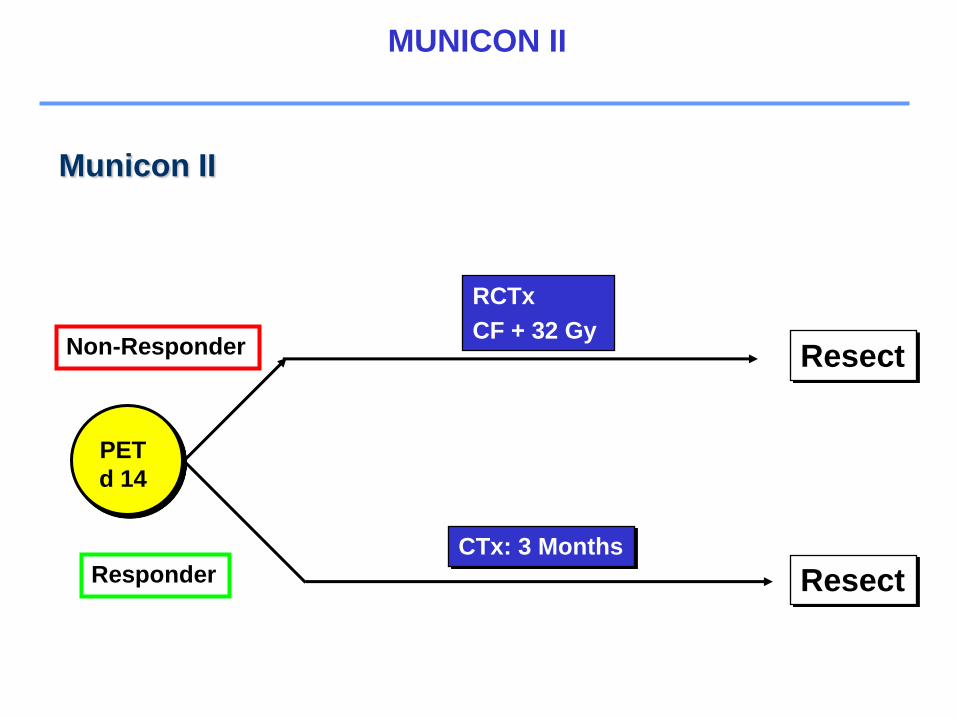
Municon II
PET
d 14
Resect
Non-Responder
ResponderCTx: 3 Months
Resect
RCTx
CF + 32 Gy
MUNICON II
Neoadjuvant
Adjuvant
Palliativ
Second line
Therapiekonzepte
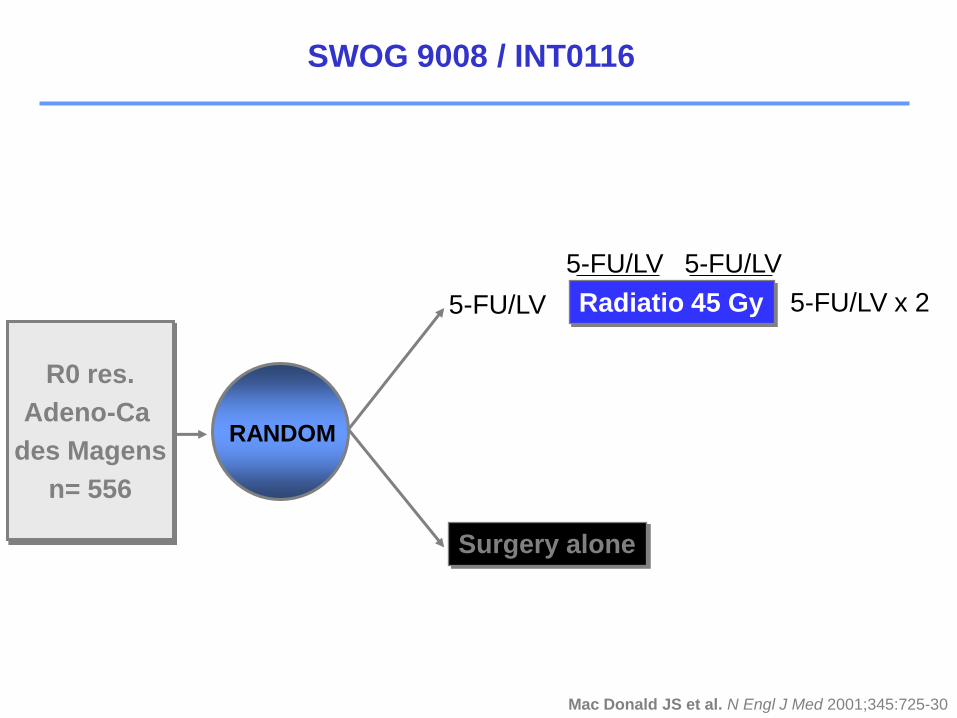
SWOG 9008 / INT0116
R0 res.
Adeno-Ca
des Magens
n= 556
RANDOM
Radiatio 45 Gy
Surgery alone
5-FU/LV 5-FU/LV x 2
5-FU/LV5-FU/LV
Mac Donald JS et al. N Engl J Med 2001;345:725-30
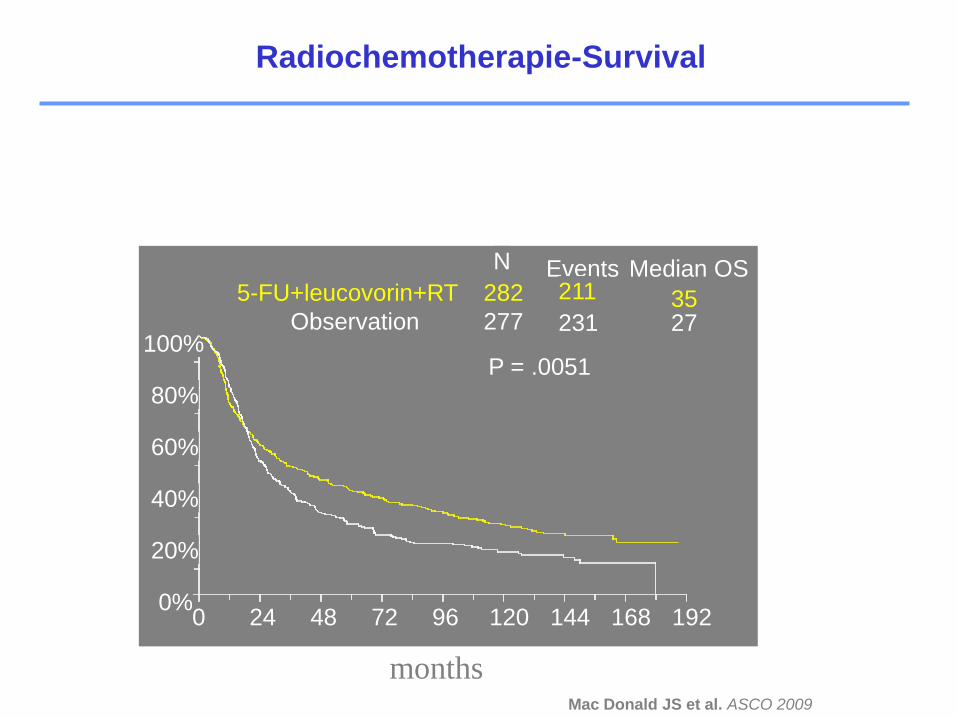
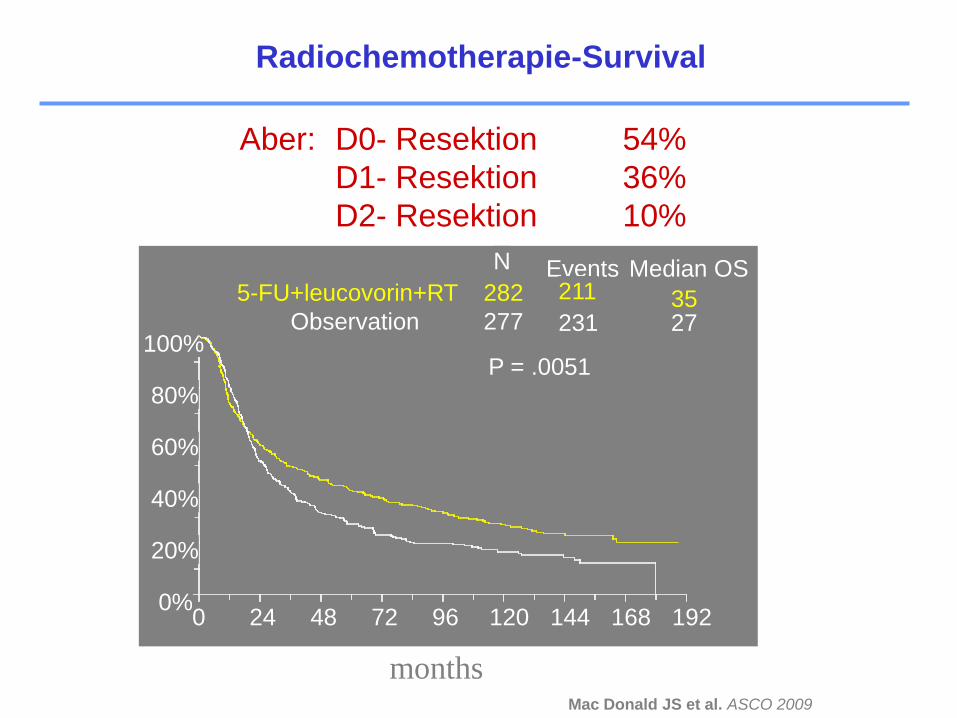
Mac Donald JS et al. ASCO 2009
Radiochemotherapie-Survival
0%
20%
40%
60%
80%
100%
0 24 48 72 96 120 144 168 192
5-FU+leucovorin+RT
Observation
N
282
277
Events211
231
Median OS
3527
P = .0051
months
Mac Donald JS et al. ASCO 2009
Radiochemotherapie-Survival
0%
20%
40%
60%
80%
100%
0 24 48 72 96 120 144 168 192
5-FU+leucovorin+RT
Observation
N
282
277
Events211
231
Median OS
3527
P = .0051
months
Aber: D0- Resektion 54%
D1- Resektion 36%
D2- Resektion 10%
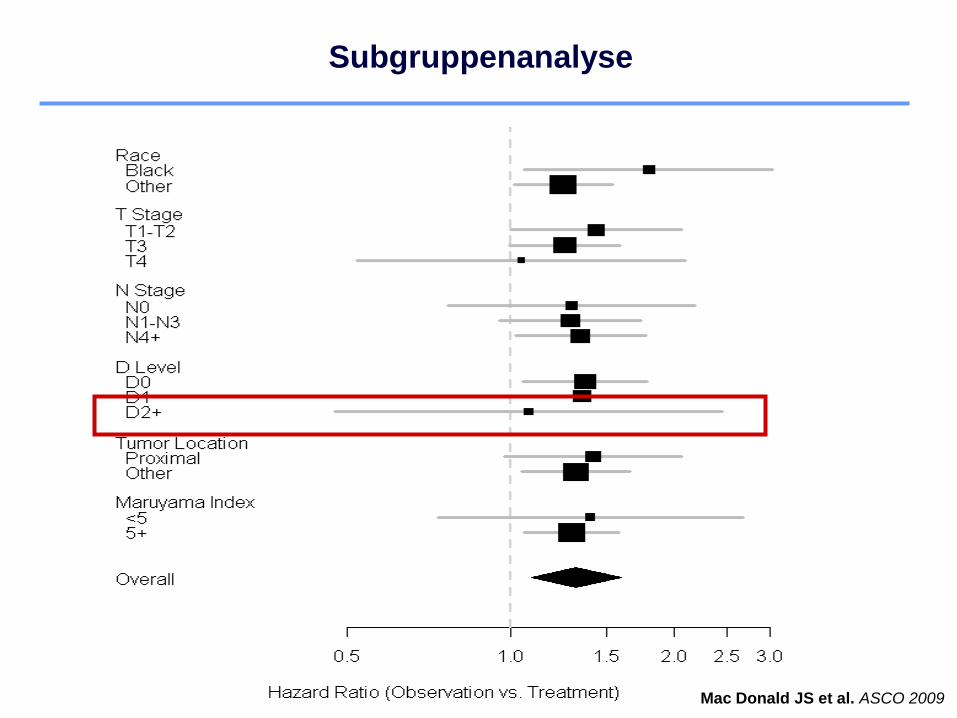
Subgruppenanalyse
Mac Donald JS et al. ASCO 2009
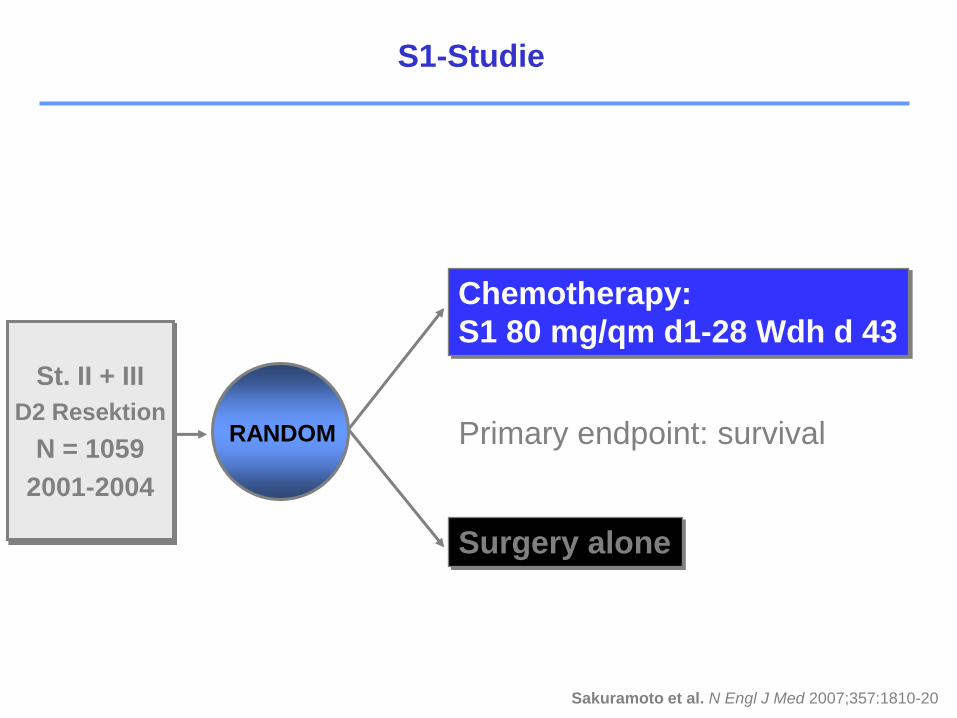
S1-Studie
St. II + III
D2 Resektion
N = 1059
2001-2004
RANDOM
Chemotherapy:
S1 80 mg/qm d1-28 Wdh d 43
Surgery alone
Primary endpoint: survival
Sakuramoto et al. N Engl J Med 2007;357:1810-20
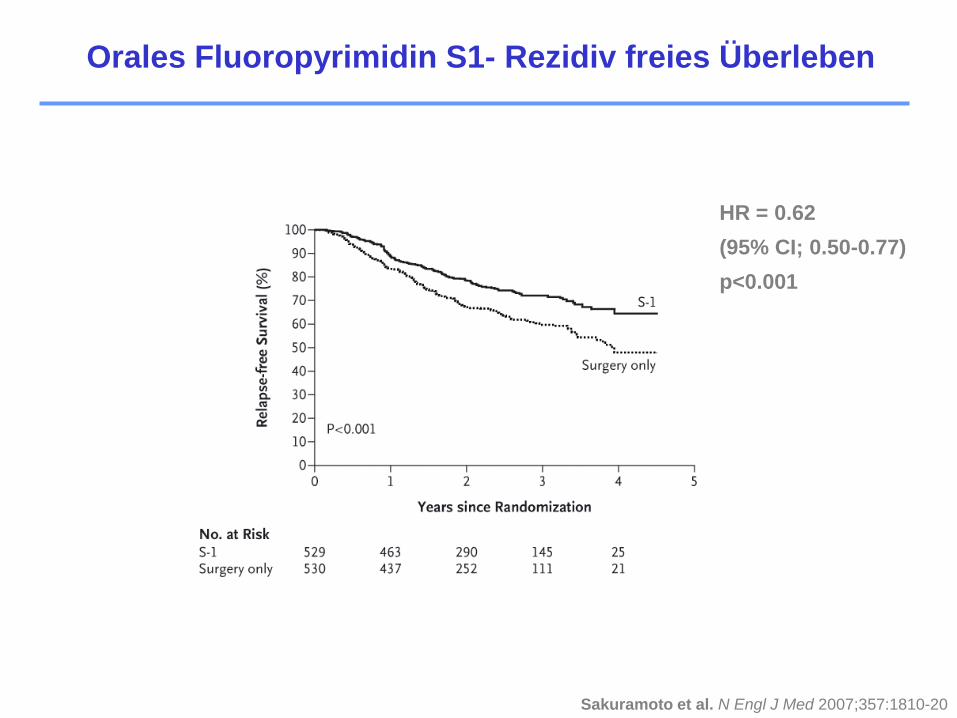
HR = 0.62
(95% CI; 0.50-0.77)
p<0.001
Sakuramoto et al. N Engl J Med 2007;357:1810-20
Orales Fluoropyrimidin S1- Rezidiv freies Überleben
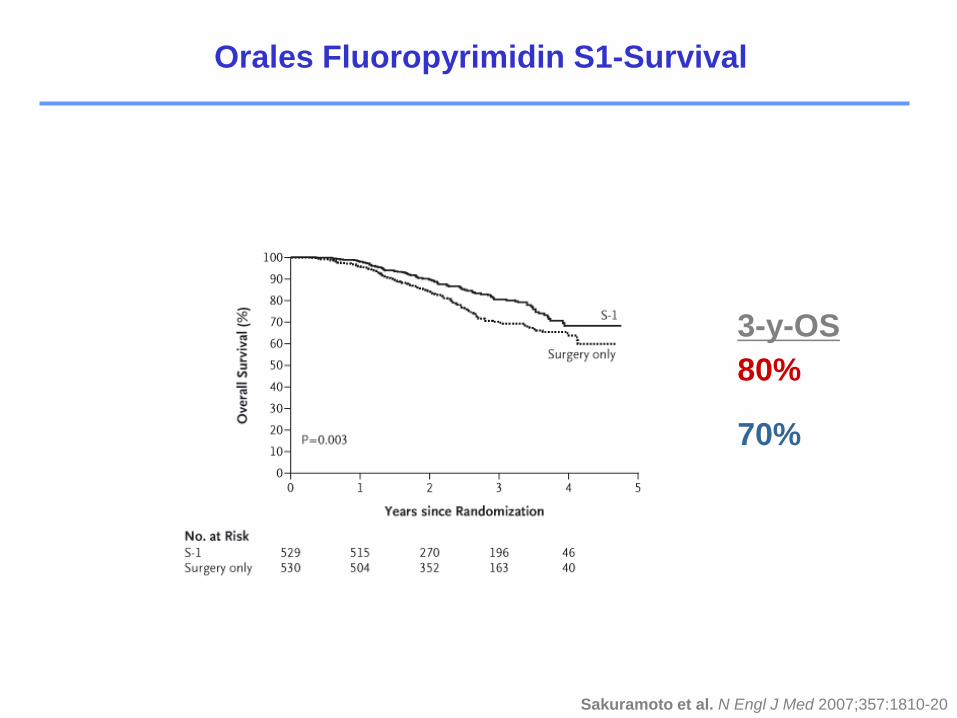
70%
3-y-OS
80%
Sakuramoto et al. N Engl J Med 2007;357:1810-20
Orales Fluoropyrimidin S1-Survival
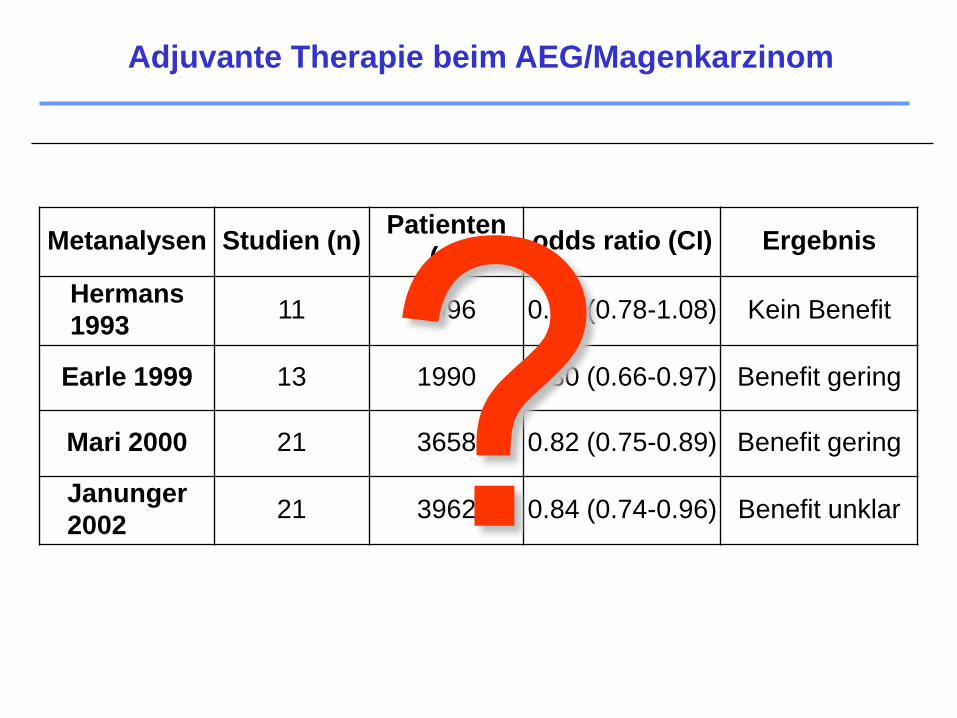
Metanalysen Studien (n)Patienten
(n)odds ratio (CI) Ergebnis
Hermans
199311 2096 0.88 (0.78-1.08) Kein Benefit
Earle 1999 13 1990 0.80 (0.66-0.97) Benefit gering
Mari 2000 21 3658 0.82 (0.75-0.89) Benefit gering
Janunger
200221 3962 0.84 (0.74-0.96) Benefit unklar
Adjuvante Therapie beim AEG/Magenkarzinom
Neoadjuvant
Adjuvant
Palliativ
Second line
Therapiekonzepte
Gibt es eine Standardchemotherapie für
metastasierte Stadien?
Metastasiertes Magenkarzinom
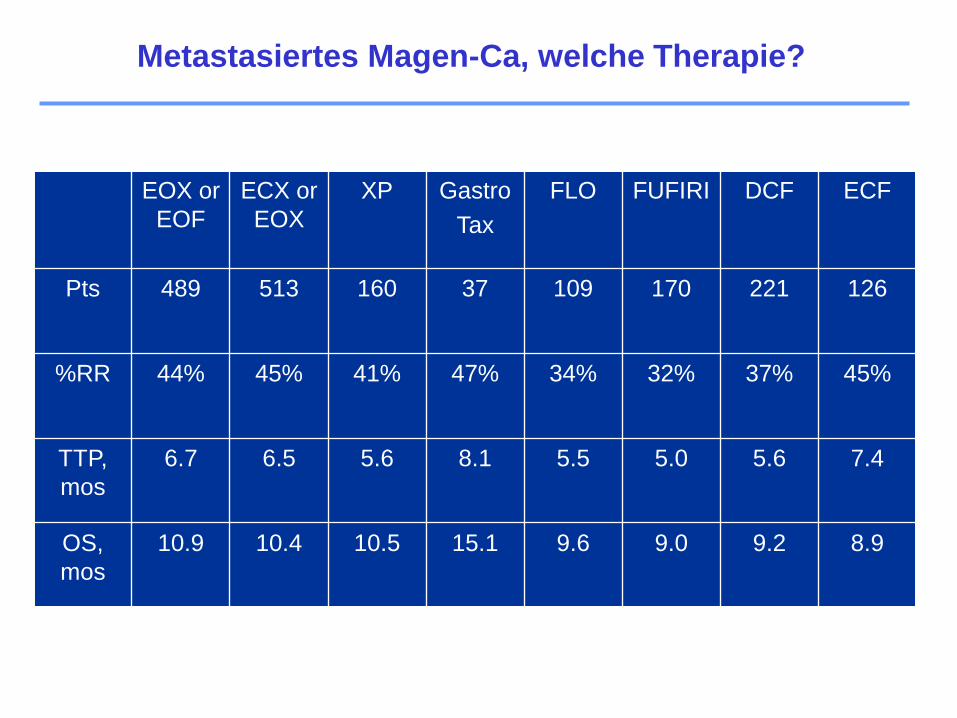
EOX or
EOF
ECX or
EOX
XP Gastro
Tax
FLO FUFIRI DCF ECF
Pts 489 513 160 37 109 170 221 126
%RR 44% 45% 41% 47% 34% 32% 37% 45%
TTP,
mos
6.7 6.5 5.6 8.1 5.5 5.0 5.6 7.4
OS,
mos
10.9 10.4 10.5 15.1 9.6 9.0 9.2 8.9
Metastasiertes Magen-Ca, welche Therapie?
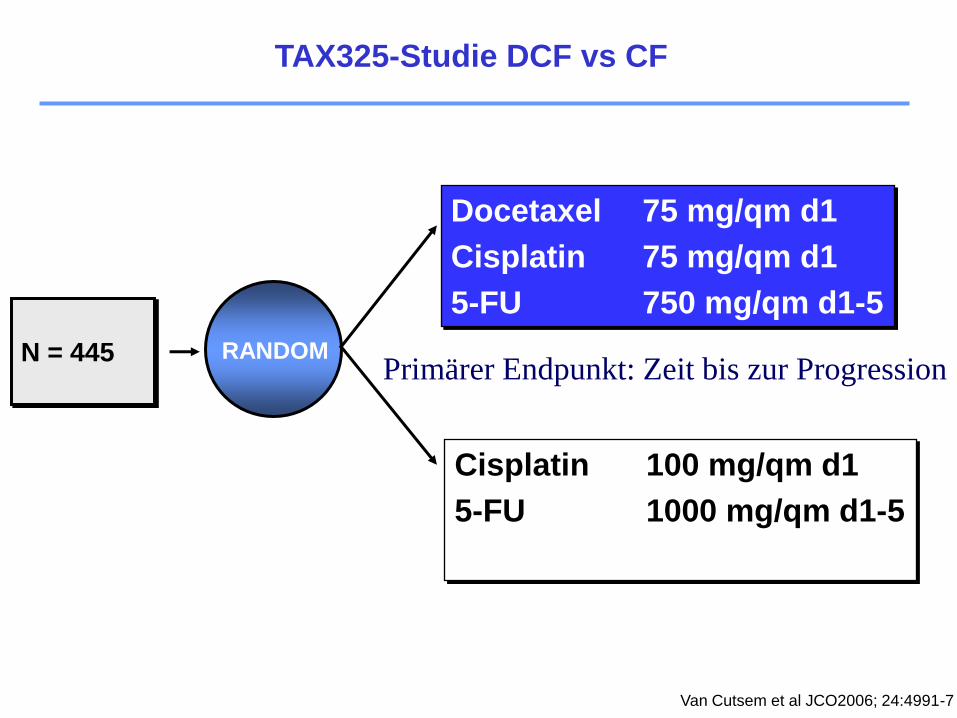
TAX325-Studie DCF vs CF
N = 445 RANDOM
Docetaxel 75 mg/qm d1
Cisplatin 75 mg/qm d1
5-FU 750 mg/qm d1-5
Cisplatin 100 mg/qm d1
5-FU 1000 mg/qm d1-5
Van Cutsem et al JCO2006; 24:4991-7
Primärer Endpunkt: Zeit bis zur Progression
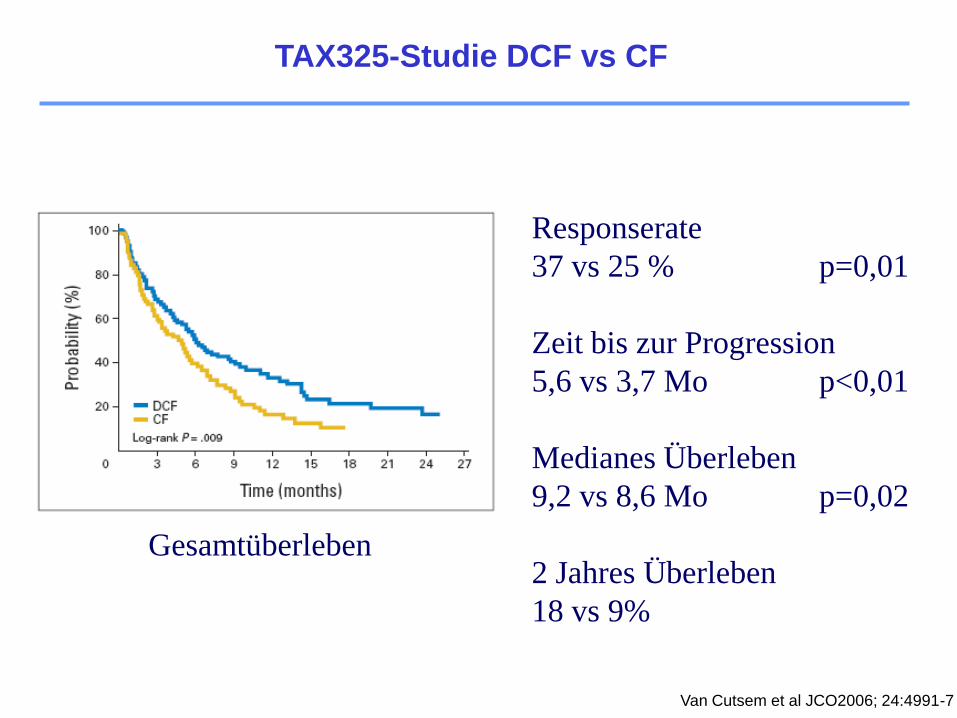
TAX325-Studie DCF vs CF
Van Cutsem et al JCO2006; 24:4991-7
Responserate
37 vs 25 % p=0,01
Zeit bis zur Progression
5,6 vs 3,7 Mo p<0,01
Medianes Überleben
9,2 vs 8,6 Mo p=0,02
2 Jahres Überleben
18 vs 9%
Gesamtüberleben
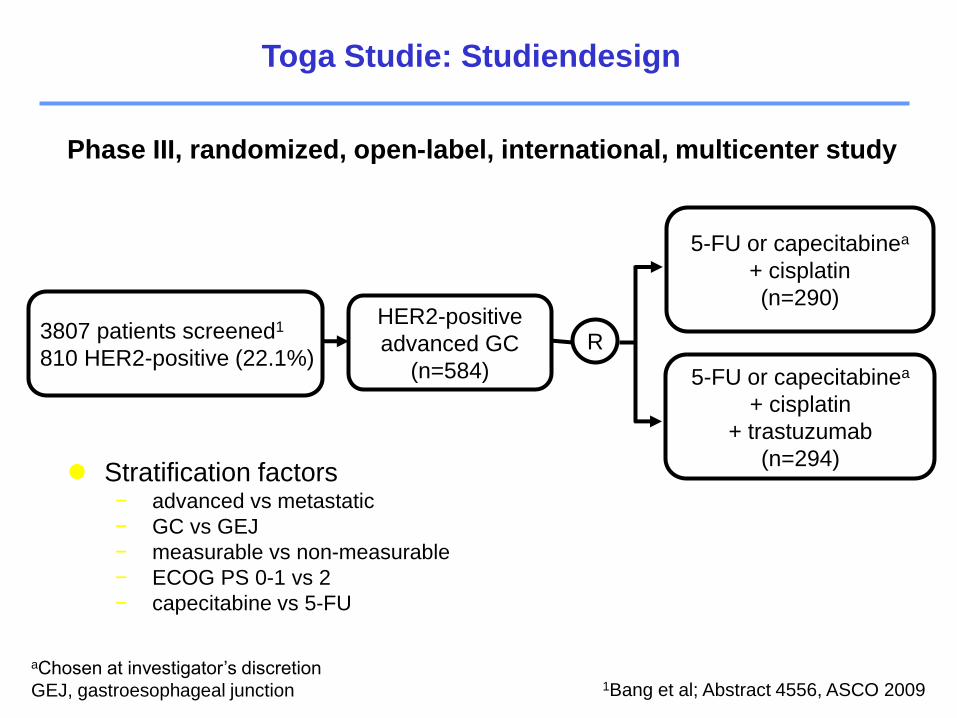
HER2-positive
advanced GC
(n=584)
5-FU or capecitabinea
+ cisplatin
(n=290)
R
aChosen at investigator’s discretion
GEJ, gastroesophageal junction
5-FU or capecitabinea
+ cisplatin
+ trastuzumab
(n=294) Stratification factors
− advanced vs metastatic
− GC vs GEJ
− measurable vs non-measurable
− ECOG PS 0-1 vs 2
− capecitabine vs 5-FU
Phase III, randomized, open-label, international, multicenter study
1Bang et al; Abstract 4556, ASCO 2009
3807 patients screened1
810 HER2-positive (22.1%)
Toga Studie: Studiendesign
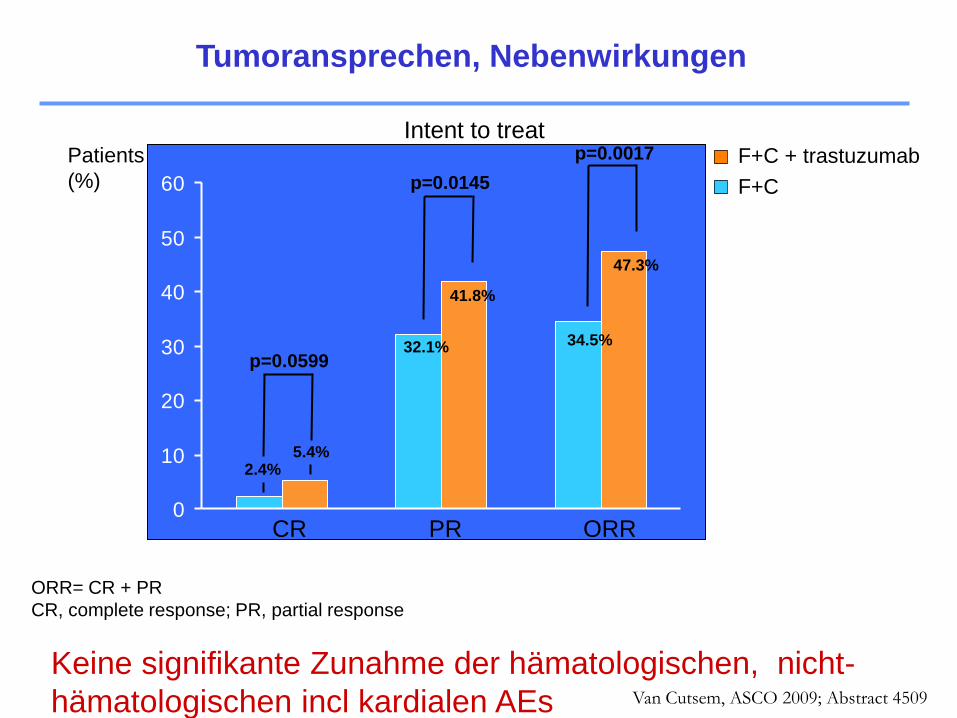
0
10
20
30
40
50
60
2.4%5.4%
32.1%
41.8%
34.5%
47.3%
Intent to treat
ORR= CR + PR
CR, complete response; PR, partial response
p=0.0599
p=0.0145
F+C + trastuzumab
F+C
p=0.0017Patients
(%)
CR PR ORR
Tumoransprechen, Nebenwirkungen
Keine signifikante Zunahme der hämatologischen, nicht-
hämatologischen incl kardialen AEs Van Cutsem, ASCO 2009; Abstract 4509
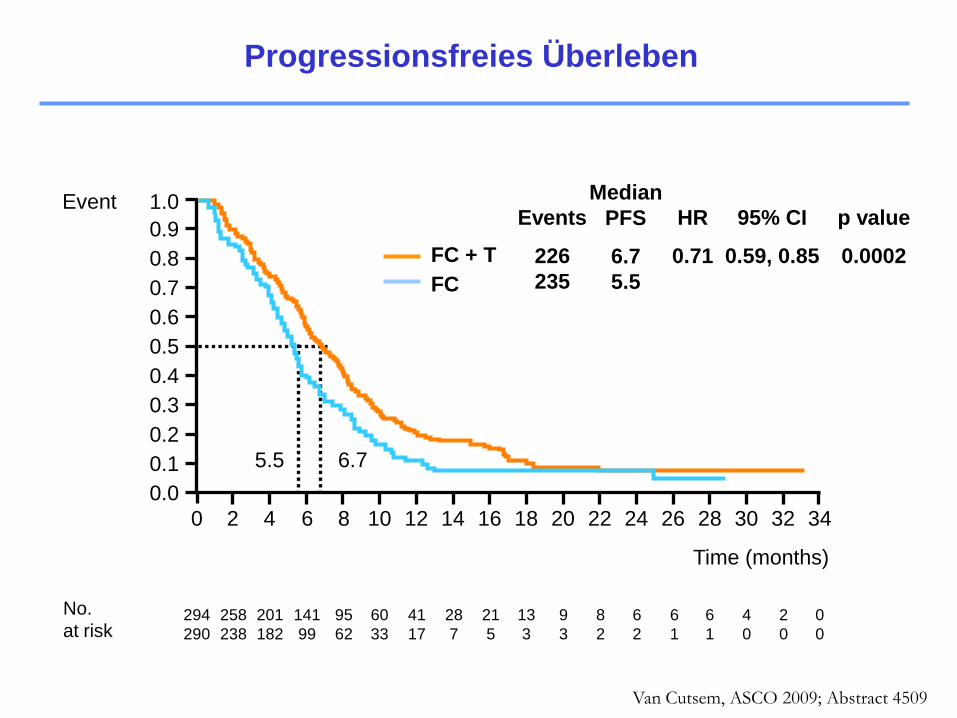
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Event
294
290
258
238
201
182
141
99
95
62
60
33
41
17
28
7
21
5
13
3
9
3
8
2
6
2
6
1
6
1
4
0
2
0
0
0
5.5 6.7
No.
at risk
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Time (months)
FC + T
FC
Events
226
235
HR
0.71
95% CI
0.59, 0.85
p value
0.0002
Median
PFS
6.7
5.5
Progressionsfreies Überleben
Van Cutsem, ASCO 2009; Abstract 4509
Time (months)
294
290
277
266
246
223
209
185
173
143
147
117
113
90
90
64
71
47
56
32
43
24
30
16
21
14
13
7
12
6
6
5
4
0
1
0
0
0
No.
at risk
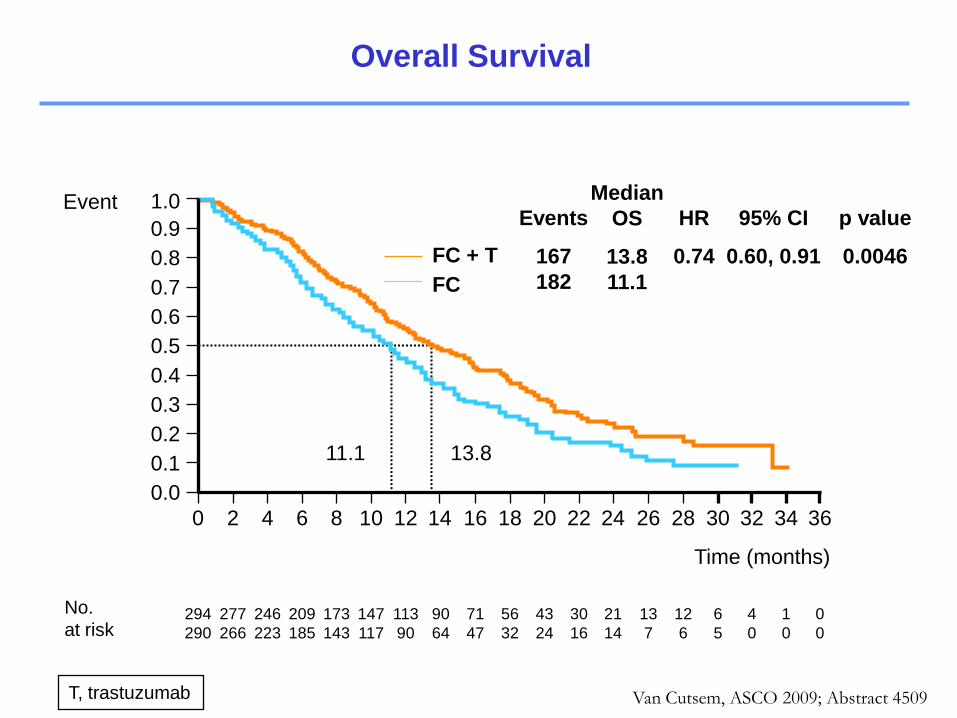
11.1 13.8
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Event
FC + T
FC
Events
167
182
HR
0.74
95% CI
0.60, 0.91
p value
0.0046
Median
OS
13.8
11.1
T, trastuzumab
Overall Survival
Van Cutsem, ASCO 2009; Abstract 4509

Subgroup Median OS
(months)
All 11.1 13.8vs
Pre-planned analysis
IHC0/FISH+
IHC1+/FISH+
IHC2+/FISH+
IHC3+/FISH+
IHC3+/FISH-
7.2
10.2
10.8
12.3
17.7
10.6
8.7
12.3
17.9
17.5
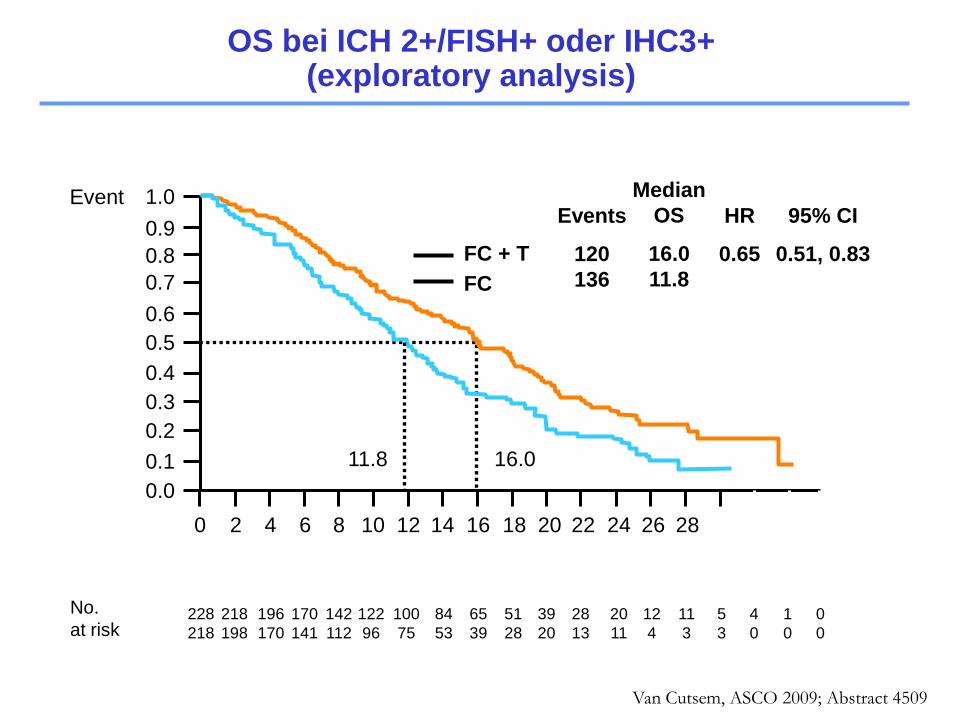
Exploratory analysis
IHC0 or 1+/FISH+
IHC2+/FISH+ or IHC3+
8.7
11.8
10.0
16.0
vs
vs
0.2 0.4 0.6 1 2 3 4 5
vs
vs
vs
vs
vs
0.92
1.24
0.75
0.58
0.83
0.48, 1.76
0.70, 2.20
0.51, 1.11
0.41, 0.81
0.20, 3.38
Hazard
ratio
95% CI
0.74 0.60, 0.91
1.07
0.65
0.70, 1.62
0.51, 0.83
Risk ratioFavors T Favors no T
584
61
70
159
256
15
131
446
N
OS in Abhängigkeit des HER2 Status
Van Cutsem, ASCO 2009; Abstract 4509
11
3
1.0
0.8
0.6
0.4
0.2
0.0
363432302826242220181614121086420
Time (months)
11.8 16.0
FC + T
FC
Events
120
136
HR
0.65
95% CI
0.51, 0.83
Median
OS
16.0
11.8
Event
0.1
0.3
0.5
0.7
0.9
218
198
4
0
5
3
12
4
20
11
228
218
196
170
170
141
142
112
122
96
100
75
84
53
65
39
51
28
1
0
0
0
No.
at risk39
20
28
13
OS bei ICH 2+/FISH+ oder IHC3+(exploratory analysis)
Van Cutsem, ASCO 2009; Abstract 4509
Neoadjuvant
Adjuvant
Palliativ
Second line
Therapiekonzepte
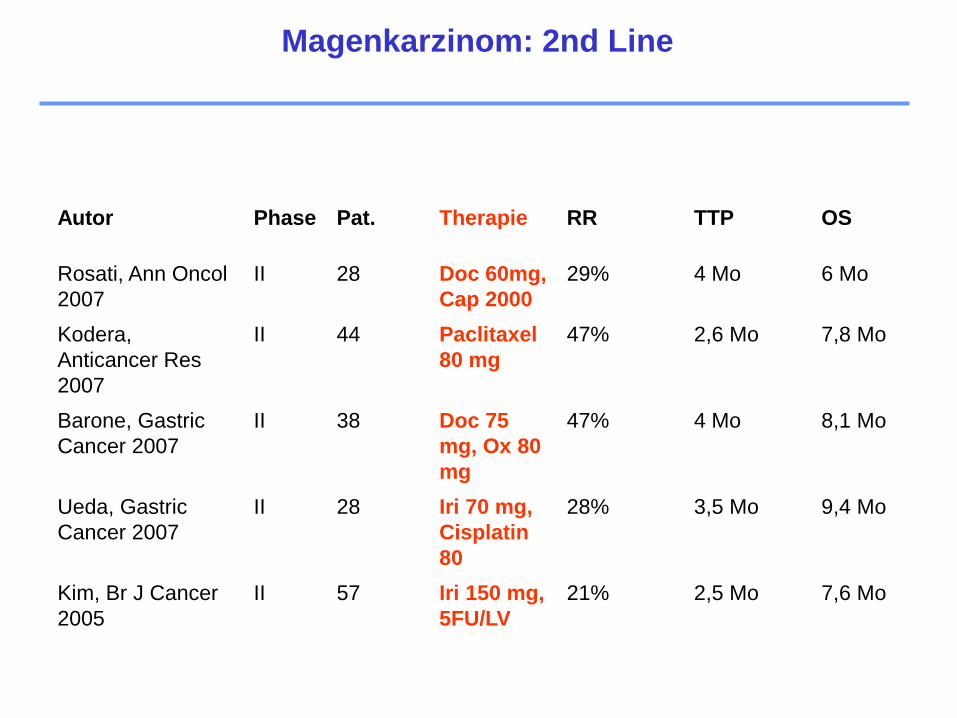
Autor Phase Pat. Therapie RR TTP OS
Rosati, Ann Oncol
2007
II 28 Doc 60mg,
Cap 2000
29% 4 Mo 6 Mo
Kodera,
Anticancer Res
2007
II 44 Paclitaxel
80 mg
47% 2,6 Mo 7,8 Mo
Barone, Gastric
Cancer 2007
II 38 Doc 75
mg, Ox 80
mg
47% 4 Mo 8,1 Mo
Ueda, Gastric
Cancer 2007
II 28 Iri 70 mg,
Cisplatin
80
28% 3,5 Mo 9,4 Mo
Kim, Br J Cancer
2005
II 57 Iri 150 mg,
5FU/LV
21% 2,5 Mo 7,6 Mo
Magenkarzinom: 2nd Line
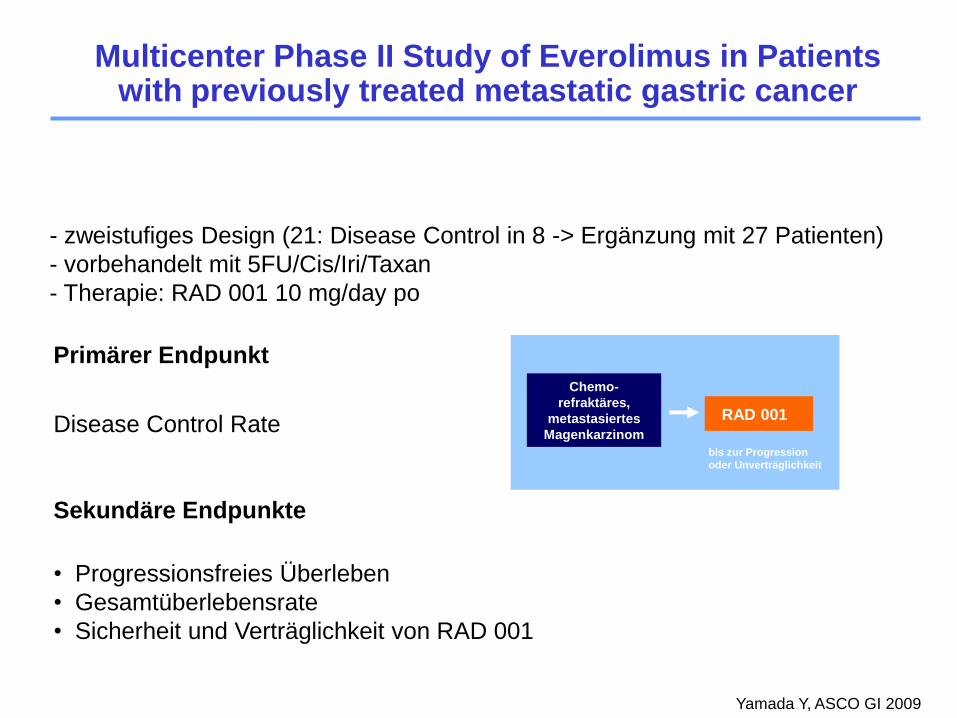
Studiendesign
- zweistufiges Design (21: Disease Control in 8 -> Ergänzung mit 27 Patienten)
- vorbehandelt mit 5FU/Cis/Iri/Taxan
- Therapie: RAD 001 10 mg/day po
Primärer Endpunkt
Disease Control Rate
Sekundäre Endpunkte
• Progressionsfreies Überleben
• Gesamtüberlebensrate
• Sicherheit und Verträglichkeit von RAD 001
RAD 001
Chemo-
refraktäres,
metastasiertes
Magenkarzinom
bis zur Progression
oder Unverträglichkeit
Yamada Y, ASCO GI 2009
Multicenter Phase II Study of Everolimus in Patients with previously treated metastatic gastric cancer
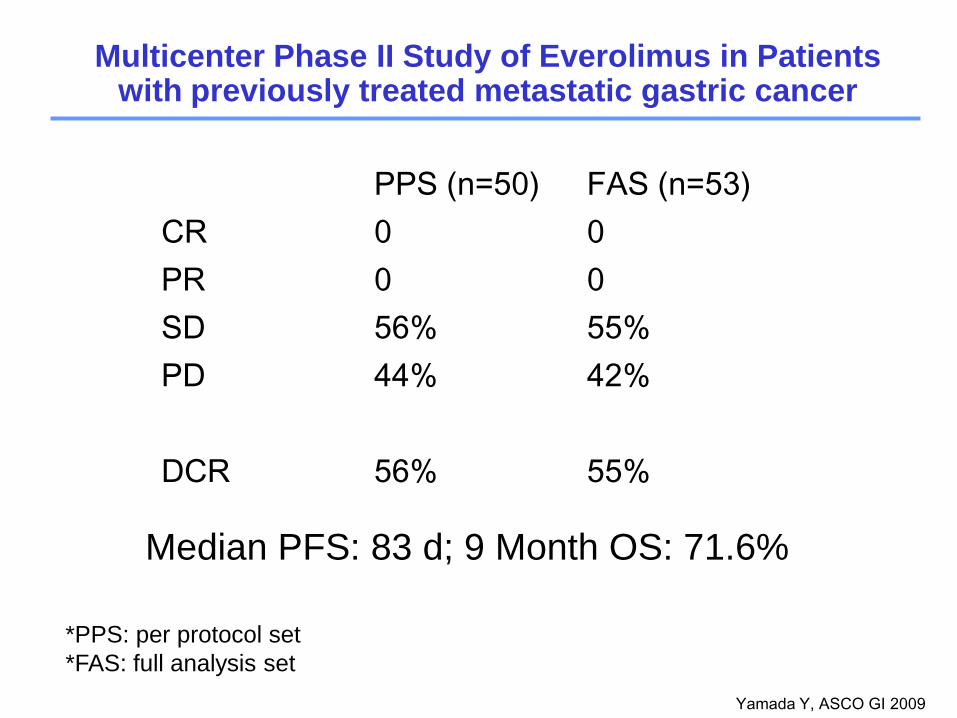
Yamada Y, ASCO GI 2009
PPS (n=50) FAS (n=53)
CR 0 0
PR 0 0
SD 56% 55%
PD 44% 42%
DCR 56% 55%
*PPS: per protocol set
*FAS: full analysis set
Median PFS: 83 d; 9 Month OS: 71.6%
Multicenter Phase II Study of Everolimus in Patients with previously treated metastatic gastric cancer
FAZIT
Perioperative Therapie ist Standard beim lokal fortgeschrittenem
Magenkarzinom
Lk Metastasierung und Chirurg wesentliche prognostische Faktoren
Erfolg der adjuvanten Therapie abhängig vom Ausmaß der OP (?)
5FU=Cap, Cis=Ox, -> Standards in der palliativen Therapie
Targeted Therapy – HER2 Testung -> Kombination mit Herceptin
Second line Therapie: Innovative Konzepte in Entwicklung
Therapie des Magenkarzinoms

Danke für Ihre Aufmerksamkeit
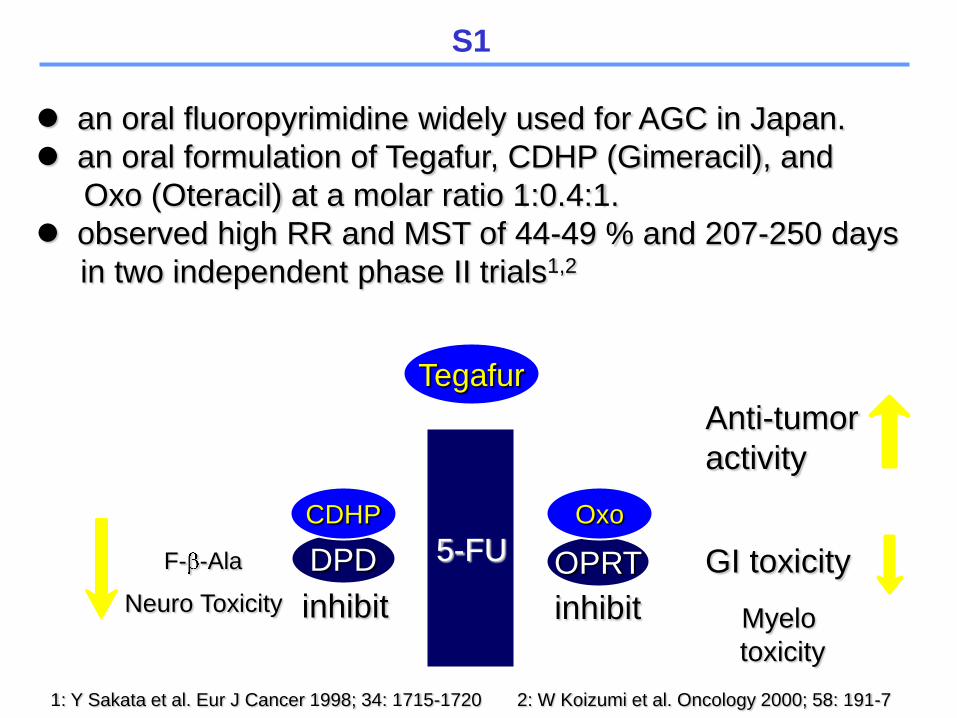
F- -Ala
Neuro Toxicity
GI toxicity
Myelo
toxicity
5-FU
Anti-tumor
activity
an oral fluoropyrimidine widely used for AGC in Japan.
an oral formulation of Tegafur, CDHP (Gimeracil), and
Oxo (Oteracil) at a molar ratio 1:0.4:1.
observed high RR and MST of 44-49 % and 207-250 days
in two independent phase II trials1,2
1: Y Sakata et al. Eur J Cancer 1998; 34: 1715-1720 2: W Koizumi et al. Oncology 2000; 58: 191-7
DPD
Tegafur
CDHP
OPRT
Oxo
inhibit inhibit
S1
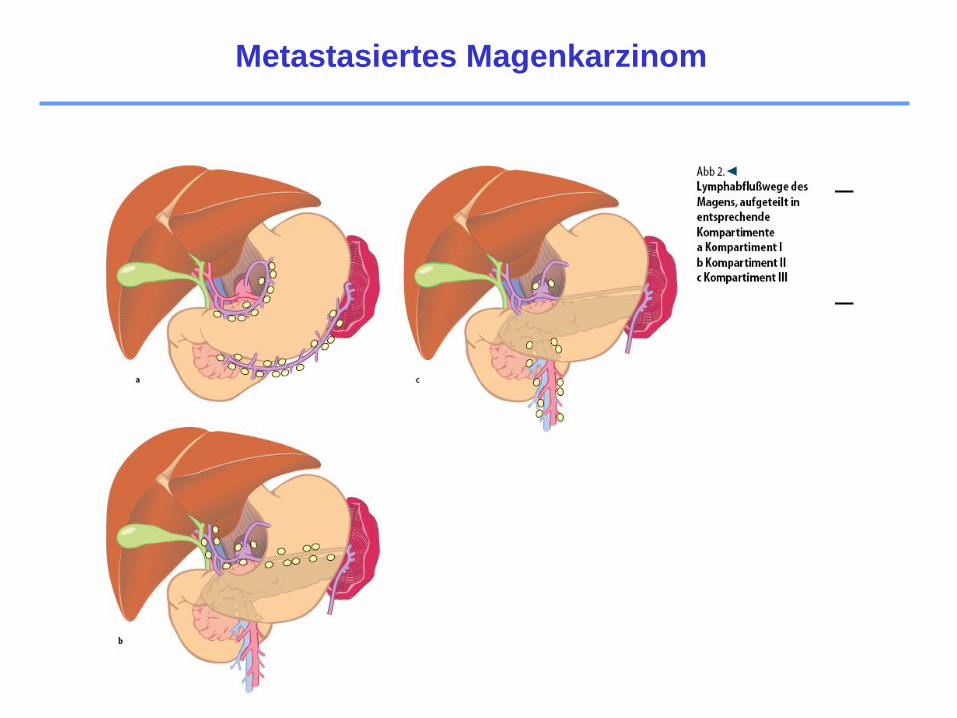
Metastasiertes Magenkarzinom