benefits of microvascular decompression on social anxiety … · 2019-06-28 · anxiety symptoms...
TRANSCRIPT

저 시-비 리- 경 지 2.0 한민
는 아래 조건 르는 경 에 한하여 게
l 저 물 복제, 포, 전송, 전시, 공연 송할 수 습니다.
다 과 같 조건 라야 합니다:
l 하는, 저 물 나 포 경 , 저 물에 적 된 허락조건 명확하게 나타내어야 합니다.
l 저 터 허가를 면 러한 조건들 적 되지 않습니다.
저 에 른 리는 내 에 하여 향 지 않습니다.
것 허락규약(Legal Code) 해하 쉽게 약한 것 니다.
Disclaimer
저 시. 하는 원저 를 시하여야 합니다.
비 리. 하는 저 물 리 목적 할 수 없습니다.
경 지. 하는 저 물 개 , 형 또는 가공할 수 없습니다.

Benefits of microvascular decompression
on social anxiety disorder and
health-related quality of life in patients
with hemifacial spasm
Young Goo Kim
Department of Medicine
The Graduate School, Yonsei University
[UCI]I804:11046-000000514575[UCI]I804:11046-000000514575


Benefits of microvascular decompression
on social anxiety disorder and
health-related quality of life in patients
with hemifacial spasm
Directed by Professor Jin Woo Chang
The Master's Thesis submitted to the Department of
Medicine, the Graduate School of Yonsei University
in partial fulfillment of the requirements for the degree
of Master of Medicine
Young Goo Kim
December 2017

This certifies that the Master's Thesis of
Young Goo Kim is approved.
------------------------------------ Thesis Supervisor : Jin Woo Chang
------------------------------------ Thesis Committee Member#1 : Hyun Sang Cho
------------------------------------ Thesis Committee Member#2 : Hyun Ho Jung
The Graduate School
Yonsei University
December 2017

ACKNOWLEDGEMENTS
The authors thank Eun Jeong Kweon, RN, Sang Keum
Park, RN for clinical data collection and patients
assessment.
<TABLE OF CONTENTS>
ABSTRACT ························································ 1
I. INTRODUCTION ··············································· 3
II. MATERIALS AND METHODS ······························ 4
III. RESULTS ····················································· 8
IV. DISCUSSION ················································ 20
1. Social Anxiety Disorder and LSAS ······················ 20
2. Influence of MVD on Psychiatric Aspect ··············· 22
3. Limitation of This Study ·································· 23
V. CONCLUSION ················································ 24
REFERENCES ···················································· 25
ABSTRACT (IN KOREAN) ··································· 27

LIST OF TABLES
Table 1. Sociodemographics and clinical characteristics of
subjects according to LSAS score ································ 10
Table 2. Self-reported psychosocial assessments comparing the
high-LSAS group with the low-LSAS group during 6
months of follow-up ················································ 12
Table 3. Self-reported HRQoL comparing the high-LSAS
group with the low-LSAS group during 6 months of
follow-up ······························································· 14
Table 4. Individual scores of the incomplete resolution patients
············································································ 17
Table 5. Self-reported psychosocial assessments and HRQoL
comparing the incomplete resolution patients with the
complete resolution patients during 6 months of follow-up 18
Table 6. Literature review of hemifacial spasm with social
anxiety disorder ······················································· 21

1
ABSTRACT
Benefits of microvascular decompression on social anxiety disorder and
health-related quality of life in patients with hemifacial spasm
Young Goo Kim
Department of Medicine
The Graduate School, Yonsei University
(Directed by Professor Jin Woo Chang)
BACKGROUND
Hemifacial spasm (HFS), an involuntary movement disorder
characterized by unilateral spasms of the muscles innervated by the facial
nerve, is likely to cause social anxiety disorder due to its significant facial
disfigurement and may have a significant influence on a patient’s
health-related quality of life (HRQoL). The goal of this study was to
investigate the influence of microvascular decompression (MVD) on the
severity of social anxiety symptoms and HRQoL in patients with HFS.
METHODS
Patients who underwent MVD from January to May 2015
were included in this study. Demographic data were collected before
surgery. Clinical data, including the standardized measures of anxiety and
depression (Hospital Anxiety Depression Scale, HADS), social anxiety
(Liebowitz Social Anxiety Scale, LSAS), and the severity of HFS were
assessed before surgery, 6 months after surgery. HRQoL data were
collected before surgery and 6 months after surgery using the Korean
version of the short form 36 (SF-36).
RESULTS

2
Six patients (21.4%) scored 60 or greater on the preoperative
LSAS and were considered to have generalized social anxiety disorder
(high-LSAS group). The duration of symptom was significantly higher in
the high-LSAS group than in the low-LSAS group (7.8 ± 2.2 vs. 4.1 ±
2.6; p = 0.011). The high-LSAS group was more likely to have
psychological comorbidities and had a more impaired quality of life than
the low-LSAS group at preoperative evaluation. Six months after MVD, a
significant improvement, compared to preoperative scores, was observed
for the total LSAS score (p=0.007) and anxiety subscale score of HADS
(p=0.012) in the high-LSAS group. Other significant improvements were
also observed in role-emotional (p=0.039) and mental component
summary (p=0.024) of the SF-36 in the high-LSAS group compared to
the low-LSAS group.
CONCLUSION
This study shows that HFS patients seem to gain benefits
from MVD not only for their facial disfigurement but also for social
anxiety symptoms that may be associated with mental health
improvements in their quality of life.
----------------------------------------------------------------------------------------
Key words: Health-related quality of life, Hemifacial spasm,
Microvascular decompression, Social anxiety disorder, Leibowitz social
anxiety scale.

3
Benefits of microvascular decompression on social anxiety disorder and
health-related quality of life in patients with hemifacial spasm
Young Goo Kim
Department of Medicine
The Graduate School, Yonsei University
(Directed by Professor Jin Woo Chang)
I. INTRODUCTION
Hemifacial spasm (HFS) is characterized by intermittent,
involuntary tonic and clonic contractions of the muscles innervated by the
ipsilateral facial nerve, with the contractions being asymmetrical and
asynchronous. The symptoms typically occur in the orbicularis oculi muscle and
then usually progress in frequency and severity and spread downward to the
ipsilateral facial muscles including the platysma1. The most common cause of
HFS is compression of the facial nerve in its root exit zone by an aberrant
arterial or venous loop2. The disorder occurs in both genders, although it more
frequently affects middle-aged or elderly women, and the condition appears to
be more common in some Asian populations3-6. HFS is not a life threatening
condition; however, patients with chronic facial disfigurement experience
serious visual and verbal disability, social embarrassment, significant distress in
social interaction, and may also develop secondary social anxiety disorders
related to HFS. Previous research revealed that HFS patients have higher scores
on the total Leibowitz Social Anxiety Scale (LSAS), which uses a questionnaire

4
to evaluate the social anxiety disorder, than control groups7.
Social anxiety disorder, also called social phobia, is the most
common anxiety disorder. It usually has an early onset and has serious effects on
social interactions and quality of life8,9. It can be defined as the fear of being
ashamed or humiliated in various social settings, such as speaking in public and
attending with a group of unfamiliar people. It is well-known that social anxiety,
which is quite common as a distinct entity, may also develop secondary to
various disfiguring or disabling physical conditions, such as essential tremor,
spasmodic torticollis, stuttering, acne vulgaris, and strabismus10-15.
Microvascular decompression (MVD) has been described as an
effective and safe procedure in HFS16. Previous studies concerning the effect of
surgical intervention on the health related quality of life (HRQoL) of HFS
patients strongly support this procedure17,18. However, to our knowledge, there
are no data to determine the impact of MVD on social anxiety symptoms using
standardized questionnaires that relate psychological outcomes in HFS patients.
Therefore, the purposes of this study were to assess the influence of MVD on
the level of social anxiety symptoms and HRQoL in patients with HFS. Other
psychiatric comorbidities (i.e., generalized anxiety and depressive mood) were
also evaluated.
II. MATERIALS AND METHODS
In this prospective study with 6 months of follow-up, 30
consecutive patients (10 males and 20 females; mean age: 51.6±9.0 years; age

5
range 34–69 years) who underwent MVD performed by a senior neurosurgeon
(J.W.C.) at Severance Hospital of Yonsei University, were enrolled from January
to October 2015. 28 of the 30 patients completed the 6 months of follow-up for
this study; the other two patients were excluded due to their refusal to respond to
the final questionnaire. Written informed consent was received from all
participants after they obtained information about the study from the
investigator (i.e., full explanation of the nature, purpose, and duration of the
study and the right to withdraw from the study at any time, without affecting the
standard of care received). Patients were included in the study if they provided
informed consent and met no exclusion criteria, which consisted of concomitant
movement disorders, heart failure, and pulmonary, renal, or hepatic
insufficiency or malignancy. Patients were also excluded if they had cognitive
impairments and could not therefore reliably answer the questions included in
the quality of life questionnaire and the self-reported psychosocial assessment.
The study was performed under a protocol approved by the Severance Hospital
Institutional Review Board (4-2014-1090).
Demographic data (i.e., age, gender, duration of symptoms, severity
score of HFS) were collected before surgery. Clinical data, including the LSAS
and Hospital Anxiety Depression Scale (HADS) values, were assessed before
surgery, and at 6 months after surgery. HRQoL data were collected
preoperatively and postoperatively (at 6 months) using the Korean version of the
Short Form 36 (SF-36). The hearing function of all patients was evaluated
6
before the MVD via pure tone audiometry (PTA). After the MVD, potential
adverse effects and any changes in the patient`s neurological state including
hearing function and physical state were assessed at visit by a neurosurgeon via
clinical examination. Postoperative computerized tomography (CT) was
immediately conducted to check the severe complications including intracranial
hemorrhage on all patients.
The severity of HFS in each patient was consecutively determined
based on the Hemifacial Spasm Scale (0=no spasm; 1=mild barely noticeable;
2=mild without, functional impairment; 3=moderate, functional impairment;
4=severe incapacitating) by a single neurosurgeon (Y.G.K.) before surgery, and
at 6 months after surgery. This scale previously has been used to assess HFS or
facial dystonia19.
In this study, social anxiety disorder was assessed via LSAS. The
LSAS is a questionnaire developed by Liebowitz to assess the severity of fear
and avoidance in social interactions (e.g., “going to party”) and performance
situations (e.g., “speaking up at meeting”). It consists of 11 items related to
social interaction and 13 items related to public performance. Fear or anxiety is
rated on a Likert-type scale ranging from 0 (none) to 3 (severe), while avoidance
is rated on a scale ranging from 0 (never) to 3 (usually; 68%–100%). A total
score is calculated by summing all fear and avoidance ratings, and elevated
LSAS scores reflect elevated levels of social anxiety. A self-reported Korean
version of the LSAS was used in this study20. The LSAS has two cut-off scores

7
of 30 and 60 for non-generalized and generalized social anxiety disorder,
respectively, as recently reported by Mennin et al.21. Therefore, in this study,
patients with total LSAS scores of 60 or higher were considered to have
clinically significant symptoms of social anxiety.
Anxiety and depression were assessed using the HADS22. This
14-item scale provides a sub-score for symptoms of anxiety and depression
separately, each scored from 0 to 21, with high scores representing more
psychological symptoms. This scale has demonstrated good psychometric
properties, and is effective in assessing anxiety and depressive symptoms in
patients with different medical diseases and in the general population23. Each
score of 11 or more on either the depression or the anxiety subscales indicates
“probable case” of depression or anxiety, with scores between 8 and 10
indicating a “possible case.”
The SF-36 is a multipurpose, generic health-status questionnaire
that has been applied in studies of more than 130 diseases and conditions24 and
has eight dimensions that can be summated into two components: the physical
component summary and mental component summary. Three dimensions
(physical functioning, role-functioning, bodily pain) correlate most highly with
the physical component summary and contribute most to the scoring of the
physical component summary measure. The mental component correlates most
highly with mental health, role-emotional, and social functioning, which
contributes most to the scoring of the mental component summary measure.

8
Vitality, general health, and social role functionality are noteworthy correlations
with both components24.
Quantitative variables are expressed as mean and standard deviation
(SD), and qualitative variables as frequencies. The Kolmogorov-Smirnov test
was performed to test the normal distribution of the variables. All variables
showed normal distributions except LSAS. Intergroup comparisons were
performed using the Mann-Whitney U test and Student`s t-test for continuous
variables and Fisher`s exact test for dichotomous variables. All data analyses
were performed using SPSS version 20.0 for Windows (SPSS, Chicago, IL, US).
The significance level was set at p<0.05.
III. RESULTS
Of the 30 eligible patients, only 28 (93.3%) completed all follow-up
visits and were thus included in the study. The mean LSAS score was 41.5±26.5
(min-max: 2-125) and the prevalence of clinically significant social anxiety
symptoms in this study was 21.4% (n=6), based on a baseline LSAS cutoff score
of ≥60. The mean LSAS score of high-LSAS group was 77.3±23.8 (min-max:
62-125) and 31.2±16.8 (min-max: 2-57) in low-LSAS group. Age, gender,
disease severity, and education level did not significantly differ between the
high-LSAS and low-LSAS groups. However, the duration of symptoms was
significantly higher in the high-LSAS group than in the low-LSAS group
(7.8±2.2 vs.4.1±2.6, p=0.011). Using HADS cutoff scores to identify “probable”
patients with depression and general anxiety, the rates of comorbidities in the

9
high-LSAS group for depression and general anxiety were 33.3% and 50.0%),
respectively (Table 1).

10
Table 1. Sociodemographics and clinical characteristics of subjects according to LSAS score.
Total (n=28) High LSASa(n=6) Low LSAS(n=22) p-value
Age 52.3±8.8 49.8±6.0 53.0±9.4 0.606d
Gender(female) 18/28(64.3%) 4/6(66.7%) 14/22(63.6%)
Duration of symptoms (years) 4.9±2.9 7.8±2.2 4.1±2.6 0.011d
Severity of symptoms 2.4±0.6 2.3±0.8 2.4±0.5 0.530d
Education(years) 12.9±2.9 11.7±2.6 13.3±2.9 0.141d
Comorbidity disorders
General anxiety(HADS-Ab≥11) 3/28(10.7%) 3/6(50.0%) 0/22(0.0%) 0.060
e
Depression(HADS-Dc≥11) 3/28(10.7%) 2/6(33.3%) 1/22(4.5%) 0.107
Quantitative variables are expressed as mean and standard deviation.
aLiebowitz Social Anxiety Scale
bHospital Anxiety Depression Scale: anxiety subscale
cHospital Anxiety Depression Scale: depression subscale
dStatistical testing was performed using Student`s t-test and the Mann-Whitney U test
eStatistical testing was performed using Fisher`s exact test

11
The mean anxiety subscore of HADS was 11.3±4.1 (min-max:
7-19) in high-LSAS group and 4.5±2.7 (min-max: 0-8) respectively in
low-LSAS group. The mean depression subscore was 9.8±3.5 (min-max: 6-15)
in high-LSAS group and 5.1±2.8 (min-max: 0-13) in low-LSAS group. Three
patients of the high-LSAS group had both generalized anxiety and depression,
two patients had a generalized anxiety, only one patient had a depressive mood.
However, all patients of low-LSAS group had not any psychiatric comorbidities
except one patient with depressive mood (HAD-depression: 13). The results of
the self-reported psychological assessment that compared the high-LSAS group
with the low-LSAS group during 6 months of follow-up are presented in Table 2.
As shown in Table 2, the high-LSAS group had significantly higher scores in all
subscales of HADS and LSAS than the low-LSAS group at baseline evaluation.
The improvements observed after MVD were simultaneous in both groups in
terms of all scores of study scales. However, a comparison of these two groups
in terms of differences observed in their scales at 6 months after MVD indicated
that the improvements of the high-LSAS group in the both assessments were
significantly higher than those of the low-LSAS group except for the HADS
depression subscore.

12
Table 2. Self-reported psychosocial assessments comparing the high-LSAS group with the low-LSAS group during 6 months of follow-up.
Quantitative variables are expressed as mean and standard deviation.
aLiebowitz Social Anxiety Scale
bHospital Anxiety Depression Scale
cDifference in scales: Baseline–6 months after MVD
dHigh-LSAS group vs. Low-LSAS group at Baseline(Statistical testing was performed using the Mann-Whitney U test)
eHigh-LSAS group vs. Low-LSAS group at Difference(Statistical testing was performed using the Mann-Whitney U test)
High LSASa (n=6) Low LSAS (n=22) p-value
d p-value
e
Baseline 6 Months Difference
c
Median[(min)-(max)] Baseline 6 Months
Difference
Median[(min)-(max)]
HADSb
Anxiety
11.3±4.1
4.8±2.3
3.5[(3.00)-(16.00)]
4.5±2.4
3.2±2.7
1.5[(-7.00)-(8.00)]
<0.001
0.012
Depression
LSAS
9.8±3.5
77.3±23.8
5.5±3.0
24.2±21.1
4.0[(-1.00)-(1.00)]
53.0[(13.00)-(106.00)]
5.1±2.8
31.7±16.8
3.2±2.5
18.3±14.2
2.0[(-3.00)-(13.00)]
12.0[(-18.00)-(43.00)]
<0.001
<0.001
0.283
0.007

13
Mean scores from the dimensions of the SF-36, together with
standard deviations, for the two groups during 6 months of follow-up are also
listed in Table 3. The patients in the high-LSAS group showed significantly
greater impairment in the role-physical, vitality, role-emotional, and mental
health dimensions and the mental component summary of the SF-36 at baseline.
After 6 months of follow-up, improvements in HRQoL were observed in both
groups. However, changes in SF-36 scores from baseline to 6 months were
higher in the high-LSAS group than in the low-LSAS group; particularly,
role-emotional and mental component summary were significantly higher (Table
3).

14
Table 3. Self-reported HRQoL comparing the high-LSAS group with the low-LSAS group during 6 months of follow-up.
High LSASa (n=6)
Low LSAS (n=22)
p-valuec
p-valued
Baseline 6 Months Difference
b
Median[(min)-(max)]
Baseline 6 Months
Difference
Median[(min)-(max)]
Physical Functioning
Role-Physical
Bodily Pain
General Health
Vitality
Social Functioning
Role-Emotional
Mental Health
Physical Component
Summary
Mental Component
Summary
48.2±4.1
43.8±9.4
49.9±8.0
38.3±7.1
37.5±8.1
40.5±10.9
36.4±13.5
35.0±6.8
50.4±5.9
32.4±9.4
49.3±7.8
50.0±6.3
54.7±9.0
44.3±8.0
45.8±7.9
50.0±6.6
52.0±4.9
44.8±10.0
50.5±9.4
47.1±9.6
-1.35[(-10.50)-(6.30)]
-7.4[(-14.70)-(4.90)]
-2.35[(-21.50)-(2.30)]
-3.65[(-14.90)-(1.00)]
-6.25[(-28.10)-(3.20)]
-8.15[(-27.30)-(5.50)]
-13.6[(-35.0)-(0.00)]
-8.45[(-22.50)-(0.00)]
2.8[(-12.30)-(5.30)]
-13.1[(-39.0)-(-0.40)]
50.8±5.7
51.5±8.5
51.9±11.5
46.4±10.7
50.2±10.8
48.4±8.7
48.1±11.4
49.2±10.0
51.6±6.3
48.2±9.5
51.4±7.7
53.4±5.0
54.0±10.3
48.2±8.8
50.9±10.5
53.4±5.7
52.8±7.2
52.4±9.5
51.7±7.5
51.9±9.1
0[(-16.80)-(12.60)]
0[(-26.90)-(7.30)]
0[(-32.60)-(17.70)]
-1.15[(-31.90)-(21.50)]
-0.5[(-40.60)-(22.00)]
-0.3[(-21.80)-(10.90)]
0[(-38.90)-(15.50)]
-2.5[(-36.60)-(22..50)]
0[(-16.90)-(11.80)]
-2.95[(-36.00)-(12.40)]
0.157
0.024
0.395
0.059
0.012
0.100
0.033
0.005
0.566
0.003
0.682
0.088
0.259
0.427
0.157
0.643
0.039
0.112
0.427
0.024

15
Quantitative variables are expressed as mean and standard deviation.
aLiebowitz Social Anxiety Scale
b Difference in scales:Baseline–6 months after microvascular decompression
cHigh-LSAS group vs. Low-LSAS group at baseline(Statistical testing was performed using the Mann-Whitney U test)
dHigh-LSAS group vs. Low-LSAS group at difference in scale(Statistical testing was performed using the Mann-Whitney U test)
16
In all 28 patients, symptoms typically started with intermittent
slight twitches in the periorbital muscles. The symptoms then increased in
frequency and severity, and spread downward to other muscles of the face
innervated by the facial nerves. One male patient underwent MVD due to
recurrent spasms. Of these 28 patients, 25 (89.3%) experienced complete
resolution of symptoms, and two patients recognized great improvement yet
continued to experience slight spasms (Grade 1) at 6 months after MVD. Only
one patient complained of remnant spasms (Grade 2) at the last follow-up visit.
Each individual scores of these patients were summarized in Table 4 and
compared with the complete resolution patients, the differences were not
statistically significant (Table 5).
In this present study, minor complications were noted in four of 28
patients (13.3%) after MVD; three patients had transient facial weakness, which
spontaneously resolved within 1 month, and one patient had cerebrospinal fluid
rhinorrhea, which recovered spontaneously after absolute bed rest for 1 week.
Hearing function in all patients was well preserved, and there were no cases of
permanent neurological deficits or intracranial hemorrhage.

17
Table 4. Individual scores of the incomplete resolution patients
Patient No 2.
;Grade 2c
Patient No 13.
;Grade 1
Patient No 27.
;Grade 1
Baseline/
6 months Difference
d
Baseline/
6 Months Difference
Baseline/
6 Months Difference
HADSa
Anxiety
Depression
LSASb
Physical Functioning
Role-Physical
Bodily Pain
General Health
Vitality
Social Functioning
Role-Emotional
Mental Health
Physical Component Summary
Mental Component Summary
11/11
15/14
68/29
52.8/57.0
47.1/56.9
51.1/62.1
43.4/43.0
39.6/42.7
45.9/40.5
40.3/55.9
24.730.3
56.1/60.6
29.7/35.2
0
1
39
-4.2
-9.8
-11.0
0.4
-3.1
5.4
-15.6
-5.6
-4.5
-5.5
0/0
2/0
26/13
57/54.9
56.9/56.9
55.4/62.1
62.5/61.5
61.5/70.8
56.8/56.8
55.9/55.9
58.5/64.1
57.5/57.5
58.0/62.8
0
2
13
2.1
0.0
-6.7
1.0
-9.3
0.0
0.0
-5.6
0.0
-4.8
1/3
0/1
2/0
50.7/50.7
54.4/56.9
51.1/51.1
50.6/30.5
61.5/39.5
45.9/56.8
52.0/55.9
55.6/33.1
51.1/50.5
54.4/42.9
-2
-1
2
0.0
-2.5
0.0
20.1
22.0
-10.9
-3.9
22.5
0.6
11.5

18
aHospital Anxiety Depression Scale
bLiebowitz Social Anxiety Scale
cseverity at 6 months after microvascular decompression
dDifference in scales:Baseline–6 months after MVD
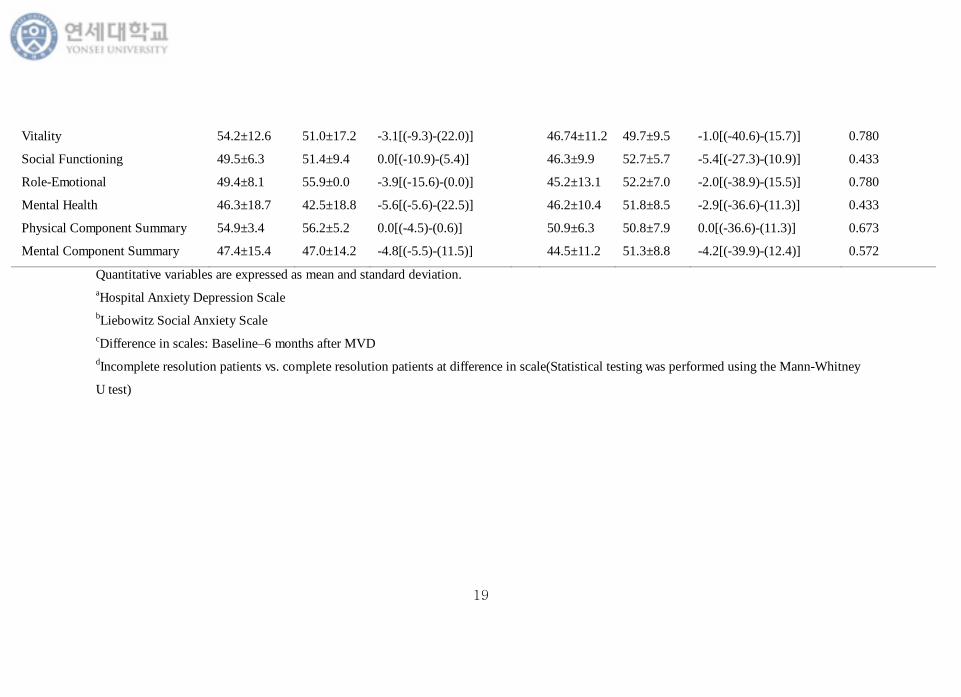
Table 5. Self-reported psychosocial assessments and HRQoL comparing the incomplete resolution patients with the complete resolution patients
during 6 months of follow-up
Incomplete resolution patients(n=3)
Complete resolution patients(n=25)
p-valued
Baseline 6 Months Difference
c
Median[(min)-(max)]
Baseline 6 Months
Difference
Median[(min)-(max)]
HADSa
Anxiety
Depression
LSASb
Physical Functioning
Role-Physical
Bodily Pain
General Health
4.3±5.8
6.0±7.8
32.0±33.4
53.5±3.2
52.8±5.1
52.5±2.5
52.2±9.6
3.7±4.0
3.3±4.9
19.7±23.7
54.2±3.0
56.9±0.0
58.4±6.4
45.0±15.6
0.0[(-2.0)-(3.0)]
2.0[(-1.0)-(6.0)]
13.0[(2.0)-(22.0)]
0.0[(-4.2)-(2.1)]
-2.5[(-9.80)-(0.0)]
-6.7[(-11.0)-(0.0)]
1.0[(0.4)-(20.1)]
6.2±3.7
6.2±2.9
42.6±25.8
49.8±5.6
49.5±9.5
51.3±11.3
43.8±10.3
3.6±2.6
3.7±2.5
19.5±15.1
50.5±7.9
52.2±5.5
53.6±10.2
47.7±8.0
3.0[(-7.0)-(16.0)]
2.0[(-3.0)-(13.0)]
16.0[(-18.0)-(106.0)]
0.0[(-16.8)-(12.6)
0.0[(-26.9)-(7.3)]
0.0[(-32.6)-(17.7)]
-2.4[(-31.9)-(21.5)]
0.280
0.944
0.673
0.999<
0.477
0.314
0.145
19
Vitality
Social Functioning
Role-Emotional
Mental Health
Physical Component Summary
Mental Component Summary
54.2±12.6
49.5±6.3
49.4±8.1
46.3±18.7
54.9±3.4
47.4±15.4
51.0±17.2
51.4±9.4
55.9±0.0
42.5±18.8
56.2±5.2
47.0±14.2
-3.1[(-9.3)-(22.0)]
0.0[(-10.9)-(5.4)]
-3.9[(-15.6)-(0.0)]
-5.6[(-5.6)-(22.5)]
0.0[(-4.5)-(0.6)]
-4.8[(-5.5)-(11.5)]
46.74±11.2
46.3±9.9
45.2±13.1
46.2±10.4
50.9±6.3
44.5±11.2
49.7±9.5
52.7±5.7
52.2±7.0
51.8±8.5
50.8±7.9
51.3±8.8
-1.0[(-40.6)-(15.7)]
-5.4[(-27.3)-(10.9)]
-2.0[(-38.9)-(15.5)]
-2.9[(-36.6)-(11.3)]
0.0[(-36.6)-(11.3)]
-4.2[(-39.9)-(12.4)]
0.780
0.433
0.780
0.433
0.673
0.572
Quantitative variables are expressed as mean and standard deviation.
aHospital Anxiety Depression Scale
bLiebowitz Social Anxiety Scale
cDifference in scales: Baseline–6 months after MVD
dIncomplete resolution patients vs. complete resolution patients at difference in scale(Statistical testing was performed using the Mann-Whitney
U test)

20
IV. DISCUSSION
This study revealed that 21.4% of HFS patients had a tendency for
social anxiety disorder. This result is similar to that of previous studies (Table 6),
which reported similar frequencies among HFS patients by using the modified
DSM-IV criteria (ignoring criterion H, which excluded social anxiety due to a
general medical condition). This rate is higher than that of primary social
anxiety disorder in the general population25 and the frequency of social anxiety
in HFS patients significantly decreased after MVD, this result was supported by
the difference in total scores of LSAS. MVD in these patients also improved
their HRQoL and psychological comorbidities.
1. Social Anxiety Disorder and LSAS
As mentioned above, in this study, social anxiety disorder was
assessed via LSAS. The LSAS is accepted by the International Consensus
Group on Depression and Anxiety as the gold standard for assessment of the
clinical influence of social anxiety disorder in an individual26. The LSAS has
been translated into many languages27-29, and its reliability and validity have
been substantiated. The Korean version of the LSAS also reports high reliability
and verified validity20. Although the LSAS is a screening tool and cannot
replace clinician evaluation, several studies have suggested that it is a useful
instrument for classifying non-anxious controls and patients with social anxiety
disorder30.

21
Table 6. Literature review of hemifacial spasm with social anxiety disorder
N/A: not available
aassessed by the Hemifacial Spasm Scale
bdiagnosed by a psychiatrist
Series (ref. no) Number of
Patients
Age
(mean±SD)
Gender
(male/female)
Duration of
Symptom
Severitya of
Symptom
Frequency of
Social anxiety disorder
Erguvan Tugba
Ozel-Kizil et al.1
20 52±13.9 11/9 111.5±106.8
(months) 2.9±0.64 20%(4/20)
b
Antonio Lucio Teixeira
et al.2
29 60.5±11.7 7/22 9.1±4.9
(years) N/A 24.1%(7/29)
b
Present Study 28 52.2±8.8 10/18 4.9±2.9
(years) 2.4. ±0.6 21.4%(6/28)

22
2. Influence of MVD on Psychiatric Aspect
In this study, the severity of symptoms did not significantly differ
between the high-LSAS and low-LSAS groups (2.3±0.8 vs. 2.4±0.5, p=0.530);
however, the mean duration of symptoms in the high-LSAS group was
significantly longer than that in the low-LSAS group (7.8±2.2 vs. 4.1±2.6,
p=0.011). These results contradict those of a previous study. E.T. Ozel-Kizil et
al. reported in a comparison study that the outpatients with essential tremor
(n=20), cervical dystonia (n=20), HFS (n=20) were treated either with
medication or botulinum toxin injection, in which the severity of social anxiety
as rated via LSAS total scores did not correlated with the severity which
assessed by Hemifacial Spasm Scale (r=0.23, p=0.92) or symptom duration
(r=0.066, p= 0.62)7. This discrepancy may be due to the fact that our patients
were admitted to the hospital for a surgical procedure, MVD, which is not a
first-line therapeutic modality, and patients who underwent MVD did not
usually respond or show side-effects to first-line treatment (i.e., medication or
botulinum toxin injection).Therefore, these patients may have had similar
severities of symptoms. In the light of these facts, the symptom duration of HFS
patients with similar severities may have been affected by the development of
social anxiety.
Preoperative psychosocial assessments indicated that the
high-LSAS group was more likely to experience problems associated with
general anxiety and depressive mood than the low-LSAS group (Table 2). These
23
results are similar to those of previous study that reported significantly higher
Hamilton Anxiety Rating Scale and Hamilton Depression Rating Scale values in
patients with secondary social anxiety disorder in hyperkinesia7.One of the main
findings in this study was the significant reductions in the severity of social
anxiety symptoms and general anxiety after MVD in the high-LSAS group
compared to the low-LSAS group.
Several previous studies has already reported that , MVD provided
significant and prolonged improvement in quality of life for patients with HFS,
as measured using a disease-specific, validated quality-of-life assessment
scale17,18 In this study, the SF-36 was used to specifically measure HRQoL.
Our results show that the role-physical, vitality, role-emotional, and mental
health dimensions and the mental component summary were significantly
impaired in the high-LSAS group compared to the low-LSAS group.
Additionally, the role-emotional dimension and mental component summary
were significantly improved after MVD (Table 3). These findings suggested that
patients with HFS who have social anxiety symptoms are significantly impaired
in aspects of mental health and that MVD also has a positive influence on
HRQoL in these patients via mental health improvement rather than physical
health enhancement.
3. Limitation of This Study
This study had several limitations. The relatively small sample size
of the study participants and the short follow-up period could be considered

24
limitations that restricted the generalization of the results. A longer patient
follow-up period would enable us to observe the long-term effects of MVD;
however, we were able to observe significant improvements even after 6 months.
Consequently, future longitudinal studies on a larger sample size are needed to
understand the clinical characteristics of secondary social anxiety in patients
with HFS and the long-term impact of MVD.
V. CONCLUSION
Our findings suggest that social anxiety symptoms were common
among patients with HFS and that the presence of social anxiety symptoms has
the potential to lower aspects of mental health in HRQoL. HFS patients with
social anxiety symptoms seem to obtain benefits from MVD not only for facial
disfigurement but also for social anxiety levels and HRQoL.

25
REFERENCES
1. Au WL, Tan LCS, Tan AKY. Hemifacial spasm in Singapore: Clinical
characteristics and patients' perceptions. Ann Acad Med Singapore
2004;33:324-8.
2. Jannetta PJ, Abbasy M, Maroon JC, Ramos FM, Albin MS. Etiology and
definitive microsurgical treatment of hemifacial spasm: operative techniques
and results in 47 patients. J Neurosurg 1977;47:321-8.
3. Tan E, Jankovic J. Bilateral hemifacial spasm: a report of five cases and a
literature review. Mov Disord 1999;14:345-9.
4. Felício AC, de Oliveira Godeiro-Junior C, Borges V, de Azevedo Silva SM,
Ferraz HB. Bilateral hemifacial spasm: a series of 10 patients with literature
review. Parkinsonism Relat Disord 2008;14:154-6.
5. Miwa H, Mizuno Y, Kondo T. Familial hemifacial spasm: report of cases and review of literature. J Neurol Sci 2002;193:97-102.
6. Rosso A, Mattos J, Fogel L, Novis S. Bilateral hemifacial spasm. Mov Disord
1994;9:236-7.
7. Ozel‐Kizil ET, Akbostanci MC, Ozguven HD, Atbasoglu EC. Secondary social
anxiety in hyperkinesias. Mov Disord 2008;23:641-5.
8. Kessler R. The impairments caused by social phobia in the general population:
implications for intervention. Acta Psychiatr Scand 2003;108:19-27.
9. Schneier FR. Social anxiety disorder. N Engl J Med 2006;355:1029-36.
10. Bez Y, Yesilova Y, Kaya MC, Sir A. High social phobia frequency and related
disability in patients with acne vulgaris. Eur J Dermatol 2011;21:756-60.
11. Schneier FR, Barnes LF, Albert SM, Louis ED. Characteristics of social phobia
among persons with essential tremor. J Clin Psychiatry 2001;62:367-72.
12. Topcuoglu V, Bez Y, Bicer DS, Dib H, Kuscu MK, Yazgan C, et al. Social
phobia in essential tremor. Turk Psikiyatri Derg 2006;17:93-100.
13. Gundel H, Wolf A, Xidara V, Busch R, Ceballos-Baumann AO. Social phobia
in spasmodic torticollis. J Neurol Neurosurg Psychiatry 2001;71:499-504.
14. Stein MB, Baird A, Walker JR. Social phobia in adults with stuttering. Am J Psychiatry 1996;153:278-80.
15. Bez Y, Coskun E, Erol K, Cingu AK, Eren Z, Topcuoglu V, et al. Adult
strabismus and social phobia: a case-controlled study. J AAPOS
2009;13:249-52.
16. Chung SS, Chang JH, Choi JY, Chang JW, Park YG. Microvascular
decompression for hemifacial spasm: a long-term follow-up of 1,169
consecutive cases. Stereotact Funct Neurosurg 2001;77:190-3.
17. Ray DK, Bahgat D, McCartney S, Burchiel KJ. Surgical outcome and
improvement in quality of life after microvascular decompression for
hemifacial spasms: a case series assessment using a validated disease-specific
scale. Stereotact Funct Neurosurg 2010;88:383-9.
18. Heuser K, Kerty E, Eide P, Cvancarova M, Dietrichs E. Microvascular
decompression for hemifacial spasm: postoperative neurologic follow‐up and
evaluation of life quality. Eur J Neurol 2007;14:335-40.
19. Tan EK, Fook-Chong S, Lum SY, Lim E. Botulinum toxin improves quality of
life in hemifacial spasm: validation of a questionnaire (HFS-30). J Neurol Sci
2004;219:151-5.
20. Kang JH, Lee JA, Oh KS, Lim SW. Validation and clinical efficacy of the
26
Korean Liebowitz Social Anxiety Scale: Clinician Administered. Korean J Clin
Psychol 2013;32:291-312.
21. Mennin DS, Fresco DM, Heimberg RG, Schneier FR, Davies SO, Liebowitz
MR. Screening for social anxiety disorder in the clinical setting: using the
Liebowitz Social Anxiety Scale. J Anxiety Disord 2002;16:661-73.
22. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta
Psychiatr Scand 1983;67:361-70.
23. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital
Anxiety and Depression Scale: an updated literature review. J Psychosom Res 2002;52:69-77.
24. Ware JE, Gandek B. Overview of the SF-36 health survey and the international
quality of life assessment (IQOLA) project. J Clin Epidemiol 1998;51:903-12.
25. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE.
Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the
National Comorbidity Survey Replication. Arch Gen Psychiatry
2005;62:593-602.
26. Ballenger JC, Davidson JR, Lecrubier Y, Nutt DJ, Bobes J, Beidel DC, et al.
Consensus statement on social anxiety disorder from the International
Consensus Group on Depression and Anxiety. J Clin Psychiatry 1998;59 Suppl
17:54-60.
27. Bobes J, Badia X, Luque A, Garcia M, Gonzalez M, Dal-Re R. [Validation of
the Spanish version of the Liebowitz social anxiety scale, social anxiety and
distress scale and Sheehan disability inventory for the evaluation of social
phobia]. Med Clin (Barc) 1999;112:530-8.
28. Yao S, Fanget F, Albuisson E, Bouvard M, Jalenques I, Cottraux J. [Social
anxiety in patients with social phobia: validation of the Liebowitz social anxiety scale: the French version]. Encephale 1998;25:429-35.
29. Asakura S, Inoue S, Sasaki F, Sasaki Y, Kitagawa N, Inoue T, et al. Reliability
and validity of the Japanese version of the Liebowitz Social Anxiety Scale.
Seishin Igaku 2002;44:1077-84.
30. Rytwinski NK, Fresco DM, Heimberg RG, Coles ME, Liebowitz MR, Cissell S,
et al. Screening for social anxiety disorder with the self‐report version of the
Liebowitz Social Anxiety Scale. Depress Anxiety 2009;26:34-8.

27
ABSTRACT (IN KOREAN)
미세혈관 감압술이 반측성 안면 경련 환자의
사회 불안 증상 및 건강 관련 삶의 질에 미치는 이점
<지도교수 장진우>
연세대학교 대학원 의학과
김영구
배경
안면 신경에 지배를 받는 편측 안면 근육의 불수의적인
수축을 특징으로 하는 이상운동 질환인 반측성 안면 경련은
심한 안면의 손상으로 인하여 사회 불안 장애를 유발할 수 있는
가능성이 높으며 이로 인하여 삶의 질에 지대한 영향을 미칠 수
있다. 저자들은 본 연구를 통하여 미세혈관 감압술이 반측성
안면 경련 환자의 사회 불안 증상 정도 및 건강 관련 삶의 질에
미치는 영향을 알아보고자 한다.
방법
본 연구는 2015년 1월부터 5월까지 반측성 안면 경련 의
치료 목적으로 미세혈관 감압술을 시행 받은 환자들을 대상으로
하였으며 인적 사항에 대한 정보는 수술 전에 조사하였으며
표준화된 불안증 및 우울증 (병원 불안-우울 척도), 사회
불안증 (Liebowitz 사회불안 척도) 그리고 반측성 안면 경련의
정도는 수술 전 그리고 수술 후 6개월뒤에 측정하였으며 삶의
질에 대한 정보 역시 short form 36 (SF-36) 한국어 버전을
이용하여 수술 전과 수술 후 6개월 뒤에 측정하였다.
결과
수술 전 시행한 Liebowitz 사회불안 척도에서 60점 이상을

28
받은 6명의 환자 (21.4%)를 범사회 불안장애가 있는 것으로
간주하였으며 이를 high Liebowitz 사회 불안 척도 그룹으로
나머지 환자를 low Liebowitz 사회 불안 척도 그룹으로
분류하였다. 반측성 안면 경련의 증상 기간은 low Liebowitz 사회
불안 척도 그룹에 비하여 high Liebowitz 사회 불안 척도 그룹의
환자들이 통계적으로 유의하게 길었다 (7.8 ± 2.2 vs. 4.1 ± 2.6;
p = 0.011). 수술 전 시행한 검사 상 high Liebowitz 사회 불안
척도 그룹의 환자들이 low Liebowitz 사회 불안 척도 그룹에
비하여 정신과적으로 동반된 질환이 더 많았으며 삶의 질 역시
더 저하되어 있음을 알 수 있었다. 미세혈관 감압술 6개월 뒤
high Liebowitz 사회 불안 척도 그룹에서 수술 전과 비교하였을
때 Liebowitz 사회 불안 척도의 총 점수 (p=0.007) 및 병원
불안-우울 척도의 불안 점수 (p=0.012)가 통계적으로 유의하게
감소하였음을 알 수 있었으며 그 외에도 low Liebowitz 사회
불안 척도 그룹에 비하여 high Liebowitz 사회 불안 척도 그룹의
환자들이 SF-36의 감정 역할 제한 (p=0.039) 그리고 정신 건강
수준 (p=0.024) 항목에서 통계적으로 유의한 개선이
관찰되었다.
결론
본 연구를 통하여 미세혈관 감압술이 반측성 안면 경련
환자의 안면 손상 회복뿐 만 아니라 그들의 삶의 질에 있어서
정신 건강 개선과 관련된 사회불안 증상의 호전에 유익이
있음을 확인 할 수 있었다.
----------------------------------------------------------------------------------------
핵심되는 말 : 건강 관련 삶의 질, 반측성 안면 경련, 미세혈관
감압술, 사회 불안 장애, Liebowitz 사회 불안 척도