canal stenosis
DESCRIPTION
semoga bermanfaat!TRANSCRIPT

Canal Stenosis

Extension – occurs when standing
Flexion – Occurs when sitting or bending forward
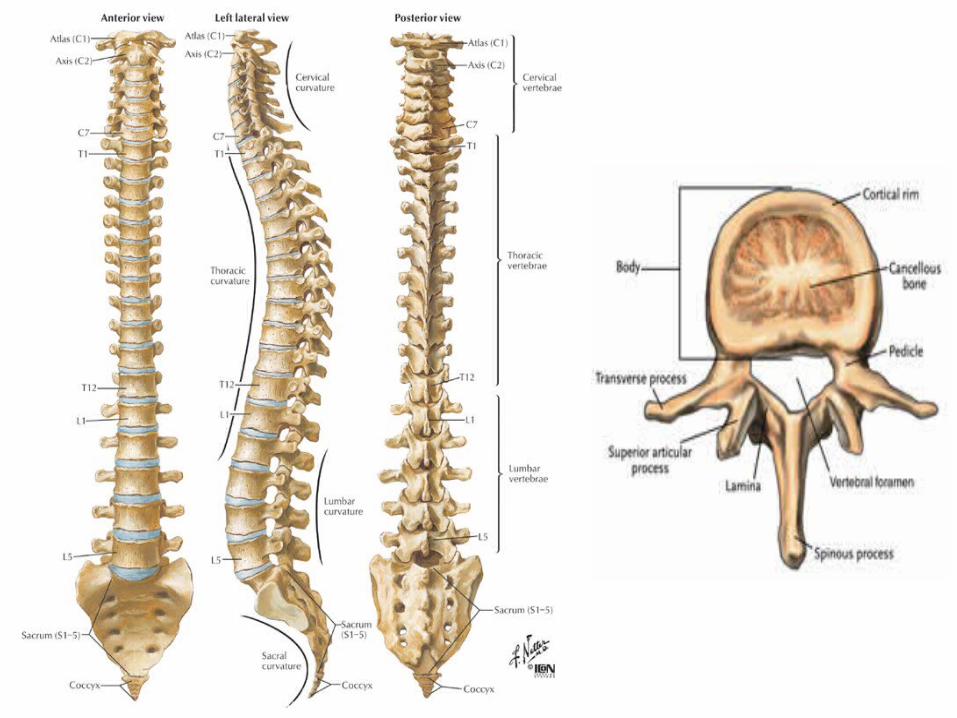
Anatomy of the SpineUnderstanding your spine: Helpful Terms

CANAL SHAPE
• Round• Triangular• Trefoiled
(15%)• Trefoiled &
asymmetric

STENOSIS
• Narrowing of the spinal canal or neuroforamina
• causing a symptomatic compression of the neural element.
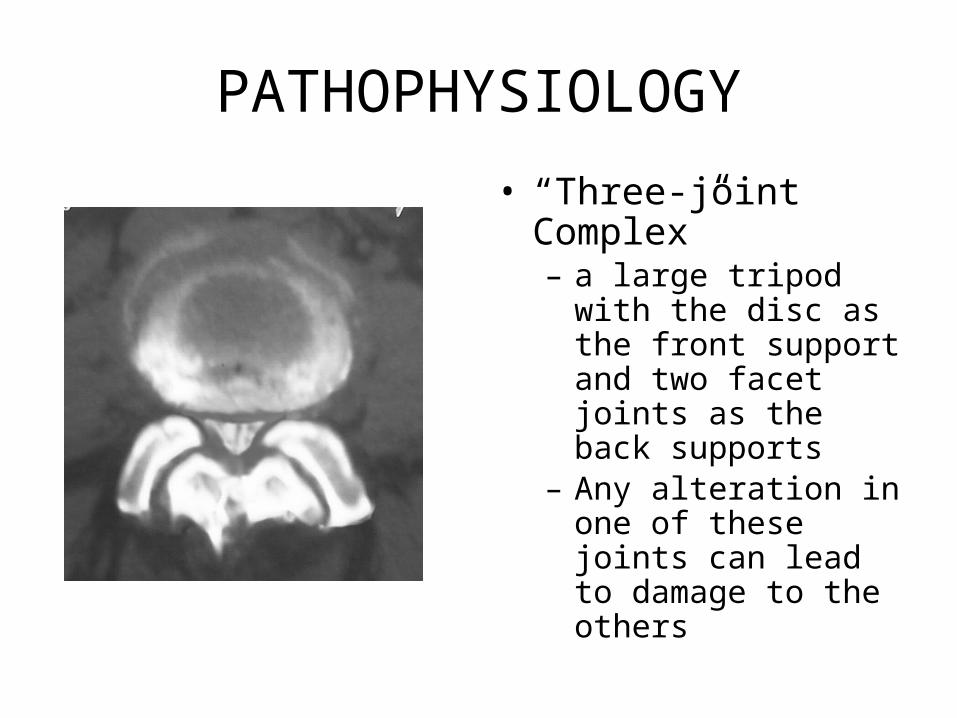
PATHOPHYSIOLOGY
• “Three-joint Complex”– a large tripod with the
disc as the front support and two facet joints as the back supports
– Any alteration in one of these joints can lead to damage to the others

• Vertebrae provide support for your head and body
• Discs act as “shock absorbers”• Vertebra protects spinal cord• Nerves have space and are not
pinched
• As we age, ligaments and bone can thicken
• Narrowing is called “stenosis”• Narrowing impinges on nerves in
spinal canal and nerve roots exiting to the legs
• Result - pain & numbness in back and legs
Nerve Root
Spinal Canal
Vertebra
“Trapped” Nerve Root
Bone (Facet Joint)
Ligament Flavum
Healthy Stenotic
Intervertebral Disc

STENOSIS
PREVALENCE
• Most common indication for spinal surgery in patients over 60 y.o.
• 400,000 Americans are estimated to have spinal stenosis
SYMPTOMS
• Neurogenic claudication• Radicular pain• Weakness• Sensory abnormalities• Back pain
PHYSICAL FINDINGSPhysical Finding Literature
Review
• Limited lumbar extension 66-100%• Muscle weakness 18-52%• Sensory deficit 32-58%
• Katz JN, et al: Diagnosis of lumbar spinal stenosis. Rheum. Dis. Clin. North Am. 20:471-483, 1994

NEUROGENIC CLAUDICATION
• Cardinal symptom of lumbar stenosis• Progressive pain and/or paresthesia in the
back, buttock, thigh and calves brought on by walking or standing, and relieved by sitting or lying down with hip flexion
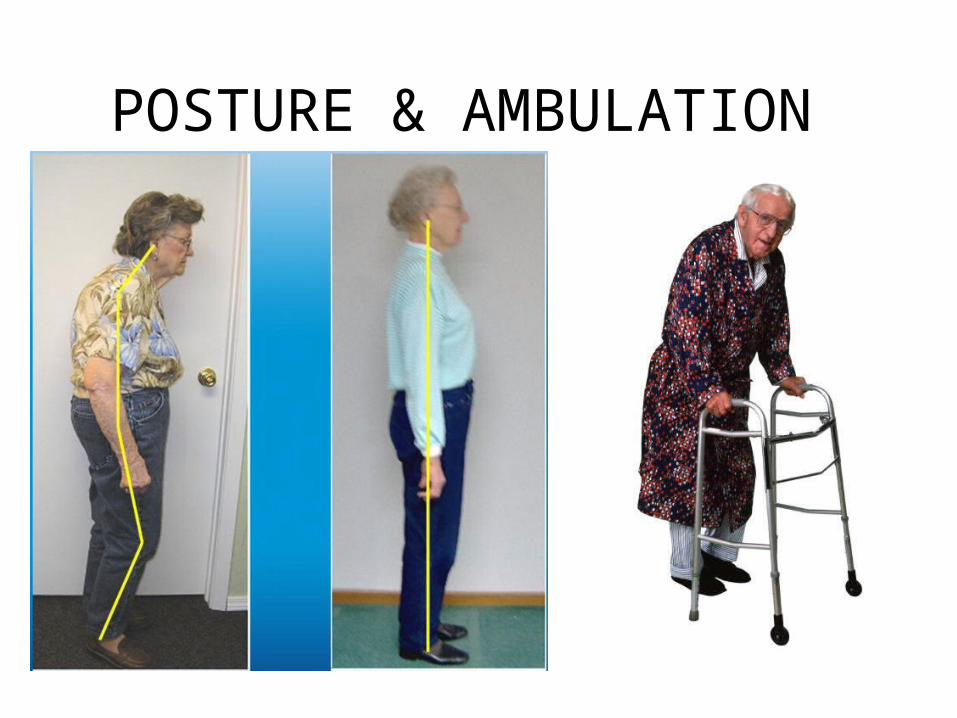
POSTURE & AMBULATION
DIFFERENTIAL DIAGNOSIS
• Vascular claudication• Osteoarthritis of hip or knee• Lumbar disc protrusion• Intraspinal tumor• Unrecognized neurologic disease• Peripheral neuropathy

NONOPERATIVE TREATMENT
• Rest• Analgesic• Oral steroid• Physical therapy• Bracing• Spinal injection

REST
• Short term activity modification for acute pain
• Long term activity modification is not recommended
Lack of activity may lead to: • Obesity• General physical deterioration• Depression/other psychological problems• Worsening of co-morbidities
Treatment of Degenerative Lumbar Spinal Stenosis, Agency for Health and Quality 2004
Disease Burden of LSS

ANALGESIC
• NSAIDS• Tylenol• Narcotics• Neurontin

Oral Steroid
• Effective for acute pain• Short duration therapy• ? Chronic or repeat tapering dose

PHYSICAL THERAPY
• Avoid extension exercises acutely
• William Flexion Exercises
• Water aerobics• Strengthening of weak
muscle groups

SPINAL INJECTIONS
• Epidural steroid• Transforaminal root block• Facet joint injection

EPIDURAL STEROID
• Commonly prescribed• 50% short-term efficacy• Not as selective• May not require
fluroscope
SPINAL INJECTION
• Most effective for acute pain• May not be indicated in cases of acute
denervation or progressive motor loss
OPERATIVE TREATMENT
• Decompression of neural element
• Stabilization of unstable segment

“LAMINECTOMY”

DECOMPRESSION OF LATERAL RECESS
• Undercutting the ventral aspect of the facet joints and the associated ligamentum flavum.
• Medial facetectomy if necessary
• The traversing nerve root underneath the facet joint must be visualized

FUSION
• Sagittal instability• Scoliosis• Iatrogenic pars defect• Greater than 50%
facet joint resection

INSTRUMENTATION
References
• Jung U. Yoo, M.D. Spinal Stenosis. Department of Orthopedics and Rehabiliatation: Oregon Health and Science University.
• Hazem Eltahawy. Lumbar Spinal Stenosis:Symptoms and Treatment. University Neuologic Surgeons