casestudy - med.swu.ac.thmed.swu.ac.th/radiology/images/stories/education/case_study/case... ·...
TRANSCRIPT
CASE STUDY
• Case : ผู้ป่วยชายไทยอายุ 64 ปี ภูมิลำเนาสระแก้ว
ไม่ได้ประกอบอาชีพ
• HN : 023588-57 AN : A13075-57
• Underlying disease : Hypertension , old
cerebrovascular accident (10years PTA)
• Chief complaint : กลืนลำบาก 4 months PTA
PRESENT ILLNESS
• 4 months PTA ผู้ป่วยกลืนแล้วเจ็บบริเวณในคอ
กลืนของแข็งแล้วติด บางครั้งกลืนไม่ได้จนมีอาการอาเจียน กลืนของเหลวได้ ไม่มีไข้ ไม่มีเบื่ออาหาร ไปคลินิคได้ยาแก้อักเสบมากินอาการไม่ดีขึ้น คลินิคแนะนำให้ไปตรวจเพิ่มเติมที่รพ.สมิติเวช ได้ทำ Barium swallowing
(22/10/57)
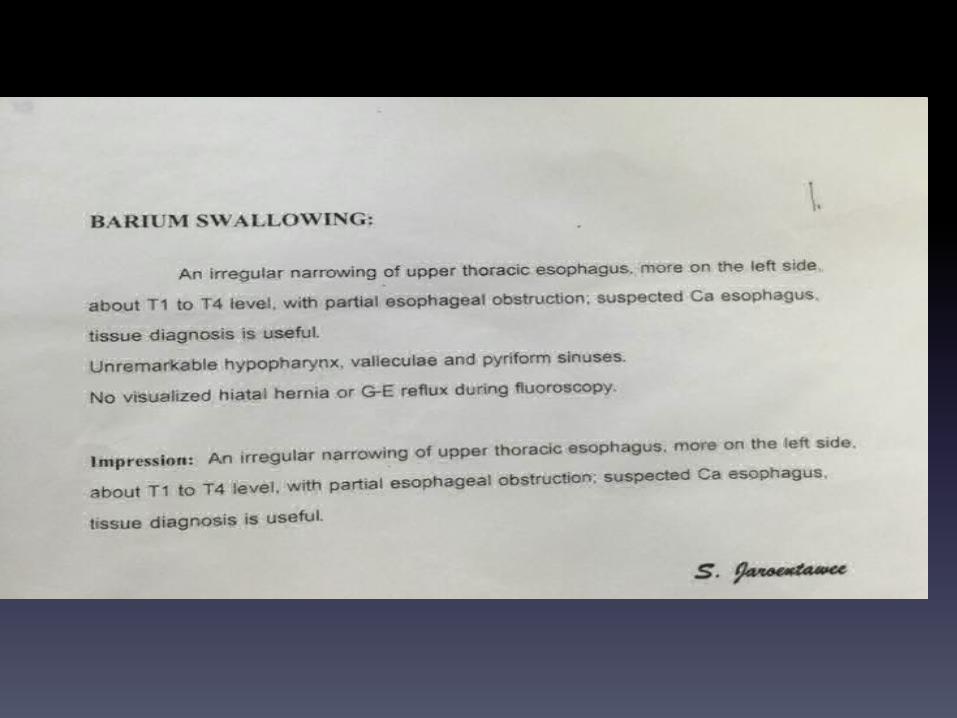
• พบ irregular narrowing of upper thoracic
esophagus, more on right side about T1 to T4
level with partial esophageal obstruction,
suspected CA esophagus
-2 weeks PTA ผู้ป่วยได้ไปตรวจเพิ่มเติม
ได้ Biopsy และ CT scan ที่รพ.สระแก้ว (ยังไม่ทราบผลชิ้นเนื้อ) หลังทำ Biopsy กินอาหารไม่ได้เลยทั้งของแข็งและของเหลว กินน้ำได้ทีละน้อยๆ ถ้ากินมากจะอาเจียนออกมาหมด
ระหว่างนั้น admit ที่รพ.สระแก้ว ได้ IV fluid
ตลอด ผู้ป่วยไม่สะดวกรักษาที่รพ.สระแก้ว จึง
refer มาที่รพ.ศูนย์การแพทย์ (มีน้ำหนักลดจาก
70kg เหลือ 56 kg ใน 4 เดือน)
PAST HISTORY
- Hypertension ไม่ได้รับยาสม่ำเสมอ ไม่มีเวียนศีรษะ ไม่มีตาพร่า ไม่มีใจสั่น ตอนนี้ไม่ได้ทานยา
- Old CVA 10 years PTA มีแขนขาซ้ายอ่อนแรง ตอนนี้พอขยับได้ ช่วยเหลือตัวเองได้
- No current medicine
- No food/drug allergy
- Smoking 60 pack years หยุดมา 2 สัปดาห์
- Alcohol drinking เบียร์ 2-3 ขวดต่อวัน 30 ปี
หยุดมา ครึ่งปี
- ไม่มีประวัติการผ่าตัดหรืออุบัติเหตุร้ายแรง
FAMILY HISTORY
- บิดา,มารดา เป็น Hypertension
-‐ No history of CA in the family
Physical examination
• Vital sign : BT 36, PR 62 bpm, RR 20/min, BP
145/66 mmHg
• GA : a Thai male, good conciousness, not pale,
no jaundice
• HEENT : not pale conjunctiva, anicteric sclera,
pharynx and tonsil aren’t injected, no mass
was seen in oral cavity
• Lymph node : left supraclavicular lymph node
1.5 cm, not tender movable
Physical examination
• CVS : normal S1S2, no murmur
• RS : normal breath sound, no adventitious sound
• Abdomen : flat shaped, normoactive bowel sound,
soft, not tender, liver and spleen can’t be palpated
• Extremities : no edema, capillary refill < 2 sec
Neurological exam Mental status : E4M6V5
Cranial nerve test :WNL
Motor power :
Deep tendon reflex : 2+ all

Problem lists 1. progressive dysphagia , odynophagia and
weight loss 4 months PTA
2. Malnultrition 2 wks PTA
3. Left supraclavicular lymph node enlarges 1.5
cm
4. Underlying disease : Old CVA, HTN
Differential diagnosis
• 1.Esophageal cancer
• 2.Achalasia
• 3.Peptic stricture
• 4.Scleroderma
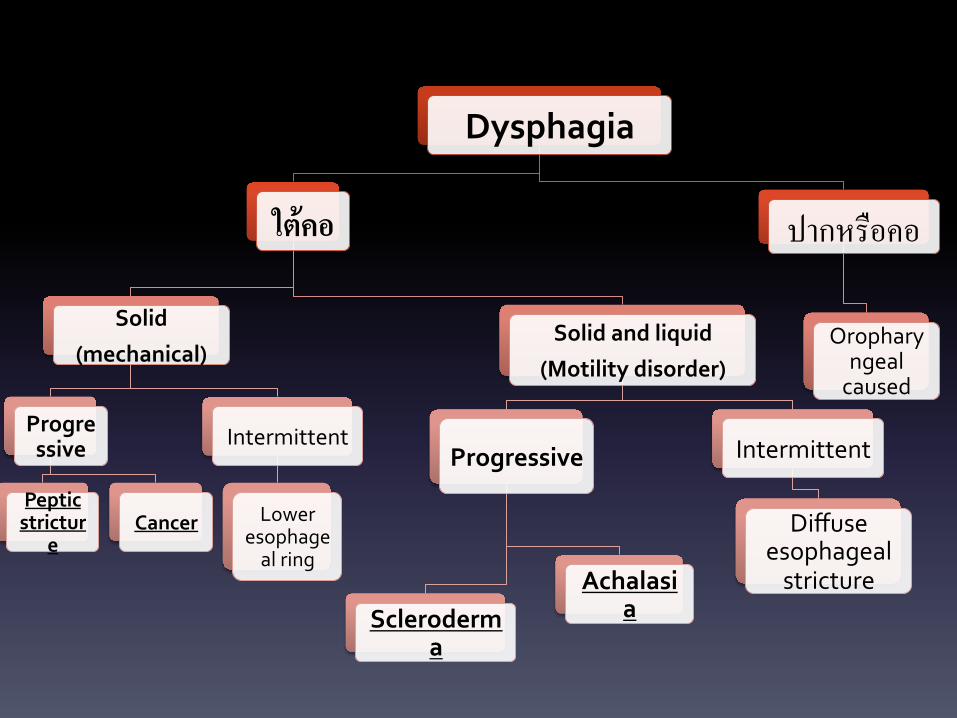
Dysphagia
ใต้คอ&
Solid
(mechanical)
Progressive
Peptic strictur
e Cancer
Intermittent
Lower esophageal ring
Solid and liquid
(Motility disorder)
Progressive
Scleroderma
Achalasia
Intermittent
Diffuse esophageal stricture
ปากหรือคอ)
Oropharyngeal caused
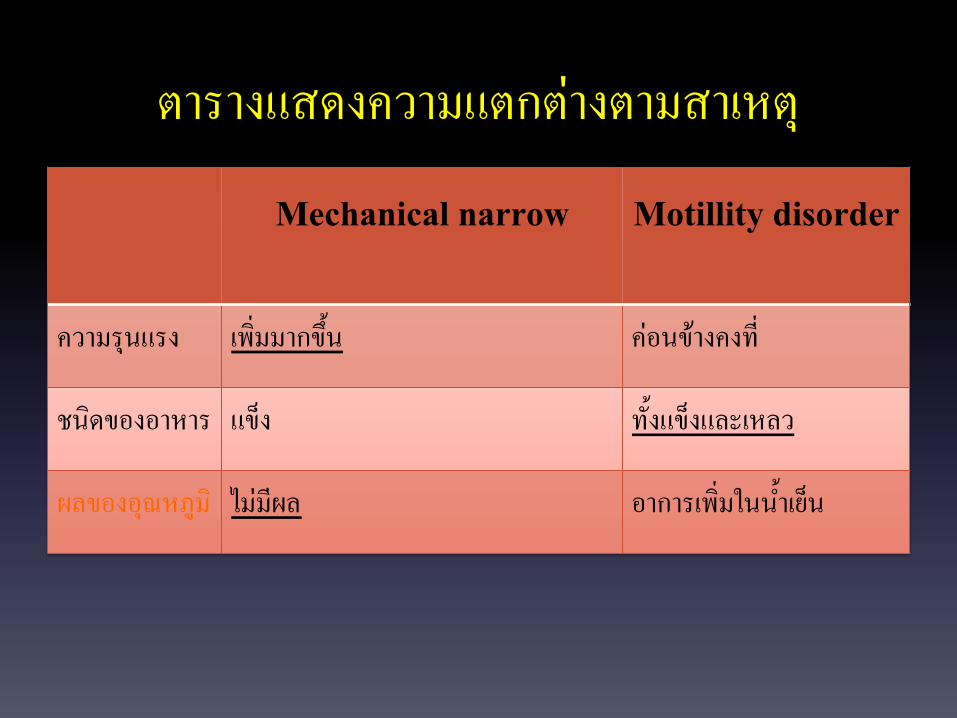
ตารางแสดงความแตกต่างตามสาเหตุ)
Mechanical narrow &
&
Motillity disorder&
&ความรุนแรง) เพิ่มมากข้ึน) ค่อนข้างคงที่)
ชนิดของอาหาร) แข็ง) ทั้งแข็งและเหลว)
ผลของอุณหภูมิ) ไม่มีผล) อาการเพิ่มในน้ำเย็น)
Carcinoma of Esophagus • อาหารแข็งจะกลืนลำบากกว่าอาหารเหลว เเบบ Progressive โดยมักเริ่มจากกลืน
ของแข็งลำบากก่อนจึงตามด้วยของเหลว)
• มีน้ำหนักลดผิดปกติ , เบื่ออาหาร)
• ตรวจคลำได้ก้อนที่บริเวณต้นคอ)
• ตรวจพบ Mulnutrition, Supraclavicular lymphnode
enlargement )
• ผู้ป่วยมีประวัติ Smoking, Alcohol)
Laboratory
• Barium swallow ---- เพื่อหาสาเหตุ, ตำแหน่งของรอยตีบ, มี
ความยาวเท่าไหร่,ตีบมากน้อยเท่าไหร,่ เพื่อเป็นแนวทางการส่องกล้อง
“mucosal destruction irregular surface, stricture”
• Esophagoscopy and biopsy --- เพื่อหาว่าเป็นมะเร็งชนิด
ใด??

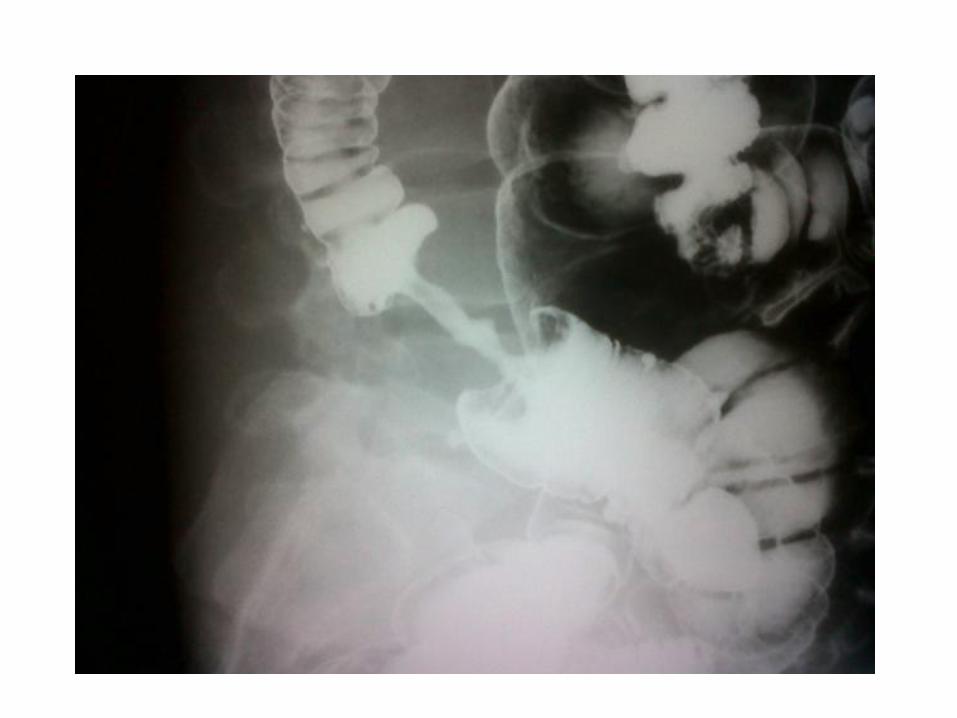
Apple Core Lesion

Achalasia • motility disorder characterized by failure of lower
esophageal sphincter (LES) relaxation as well as loss of peristalsis in the distal esophagus )
• มี clinical triad คือ dysphagia, regurgitation, weight loss)
• ไม่มีอาการ regurgitation )
• ไม่สามารถอธิบายเรื่องก้อนที่พบ)
• มักพบในเพศหญิงมากกว่า , ในช่วงอายุ 30-50 ปี)
Laboratory
• Barium swallowing --- dilate esophagus บริเวณ esophagogastric
junction จะพบ bird beak deformities )
• Manometry -- non peritalsis, incomplete relaxation ของ LES )
• Esophagogastroscopy -- เห็น esophagus มีขนาดใหญ่ พบรอยคอดบริเวณ
EG junction แต่ esophageal mucosal ปกติ และสามารถส่องกล้องบริเวณ
ท่ออาหารได้ง่าย)
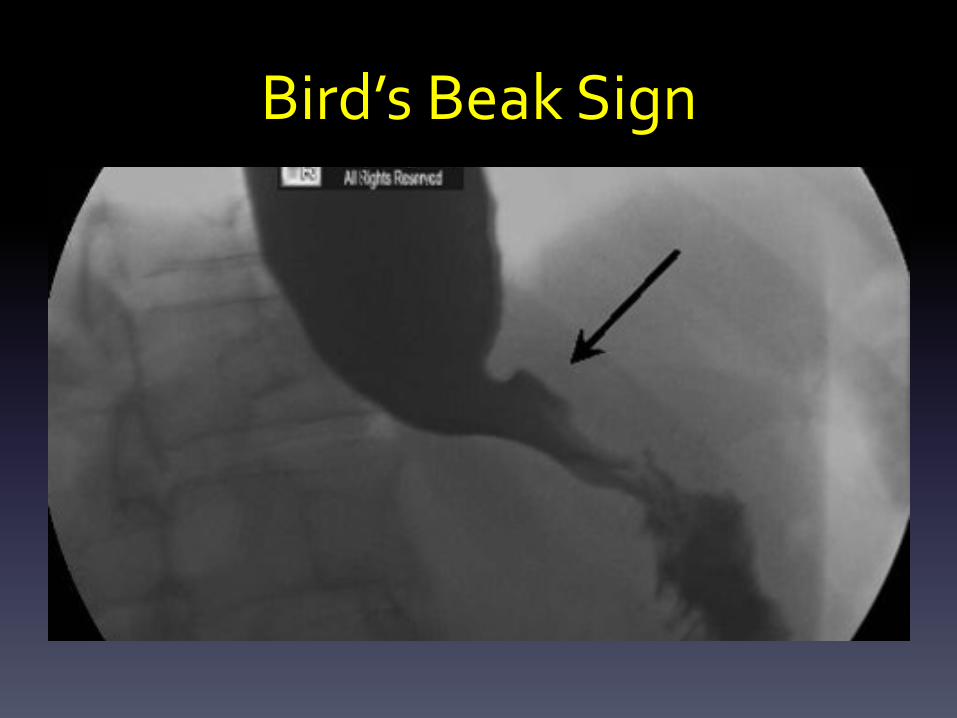
Bird’s Beak Sign
Peptic stricture )
• Progressive dysphagia
• ผู้ป่วยไม่มีประวัติแสบหน้าอก ( Heart burn) หลังรับประทาน
อาหาร)
• อธิบายลักษณะก้อนที่พบบริเวณที่คอไม่ได้
Laboratory
• Barrium swallowing จะพบรอยตีบที่ lower
esophagus แต่อาจจะแยกจาก esophageal cancer ไม่ได้
การตรวจ esophagoscopy และ biospy จะดีที่สุด
Scleroderma
• Progressive Dysphagia)
• ไม่พบผิวหนังแข็งซ่ึงเป็น major criteria
• มักพบในเพศหญิงมากกว่า)
• อธิบายลักษณะก้อนที่พบไม่ได้
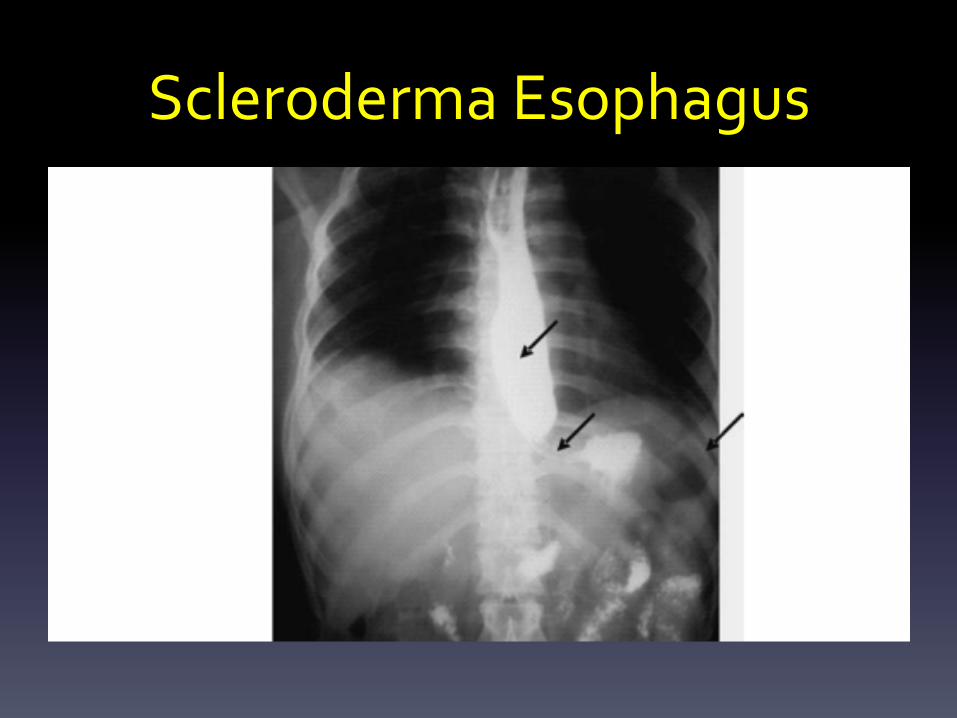
Scleroderma Esophagus
Provisional diagnosis
• ESOPHAGEAL CANCER
Lab investigation
• CBC Hb 15 g/dL Hct 42.7 % Red cell count 50.7 x10^6/mm3MCV 84.2 fL MCH 29.6 pg RDW 13.2 %
• White cell count 5.89 x10^3/mm3 Neutrophil 63.8% Lymphocyte 23.1% Monocyte 8.3 % Eosinophil 4.6 % Basophil 0.2 % Platelet smear adequate Red cell morphology :normocytosis normochromic
• PT 11.50 sec INR 0.98 PTT 27.80 sec
• Mg 2.33 mg/dL Ca (total) 9.60 mg/dL BUN 11.3 mg/dL Cr 0.73 mg/dL
• 5 พฤศจิกายน 2557
Na 134 mmol/L K 5.13 mmol/L
Cl 96.4 mmol/L HCO3- 24.2 mmol/L
Anion gap 18.59
• Liver function test
Total protein 8.26 g/dL
Albumin 4.25 g/dL Globulin 3.3 g/dL
Bilirubin (total) 1.08 g/dL (high)
Bilirubin (direct) 0.23 mg/dL (high)
AST 33 U/L ALT 32 U/L ALP 56U/L

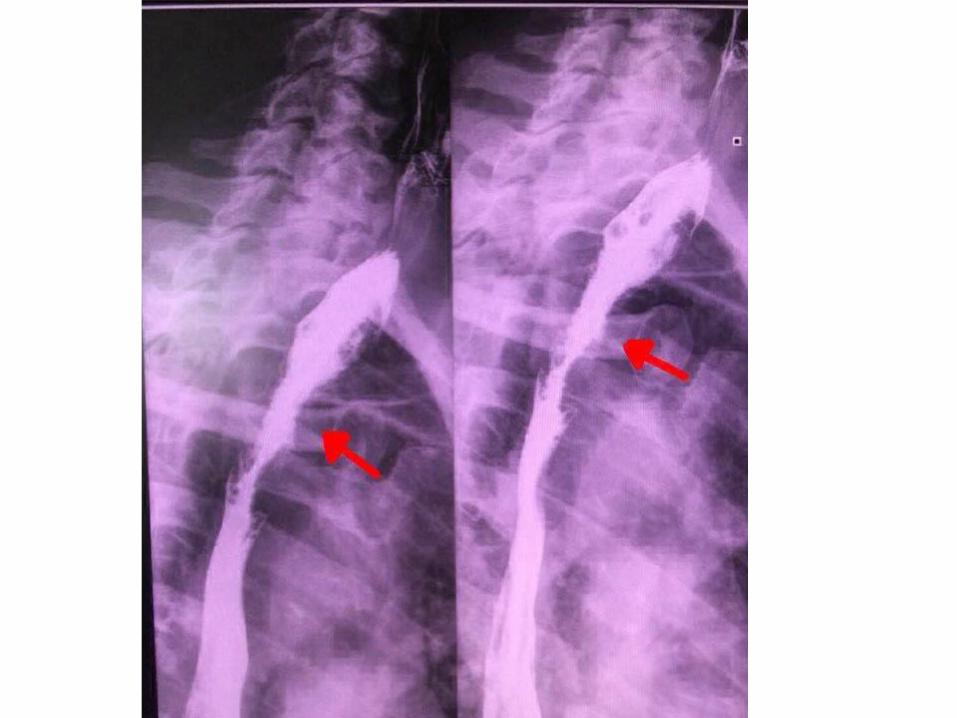
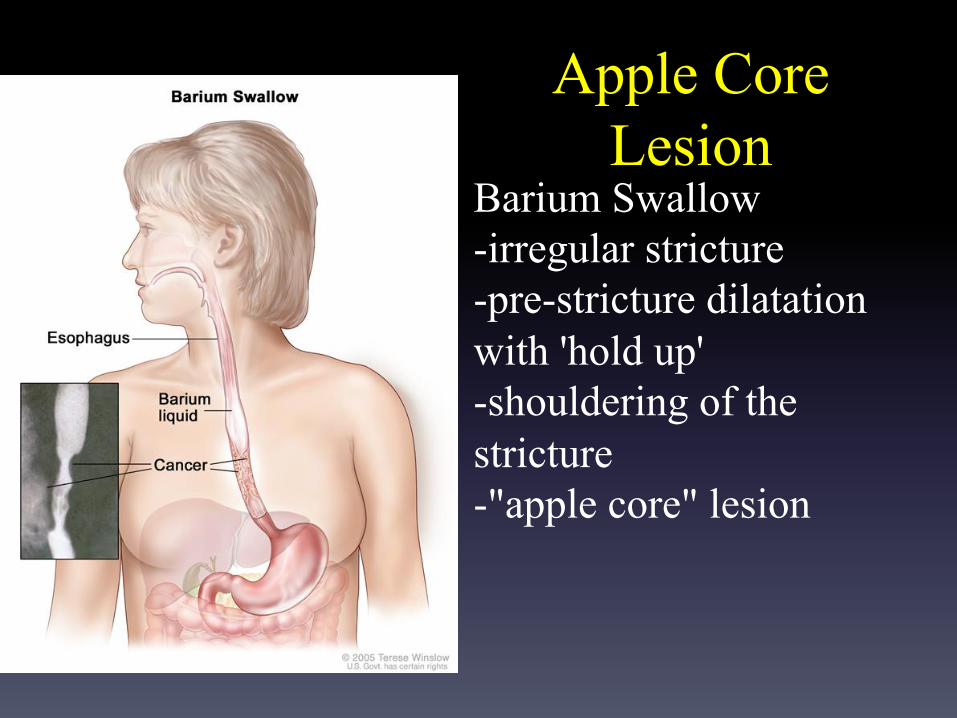
Apple Core Lesion
Barium Swallow -irregular stricture -pre-stricture dilatation with 'hold up' -shouldering of the stricture -"apple core" lesion
Other apple core sign
• COLON
also known as a napkin ring sign (bowel), is
most frequently associated with constriction
of the lumen of the colon by a stenosing
annular colorectal carcinoma .
Other apple core sign
• FEMUR
- describe the circumferential erosion of the
femoral neck seen in synovial chrondomatosis

Conclusion • History Taking >> กลืนเจ็บ,กลืนลำบาก, น้ำหนักลด,เหล้า,บุหรี่ • Physical Examination >> supraclavicular lymphadenopathy 1.5 cm • Investigation >> barrium swallowing-apple core • Epidermiology >> M:F = 3:1 age 55-65 yrs
“ESOPHAGEAL CANCER”
TREATMENT
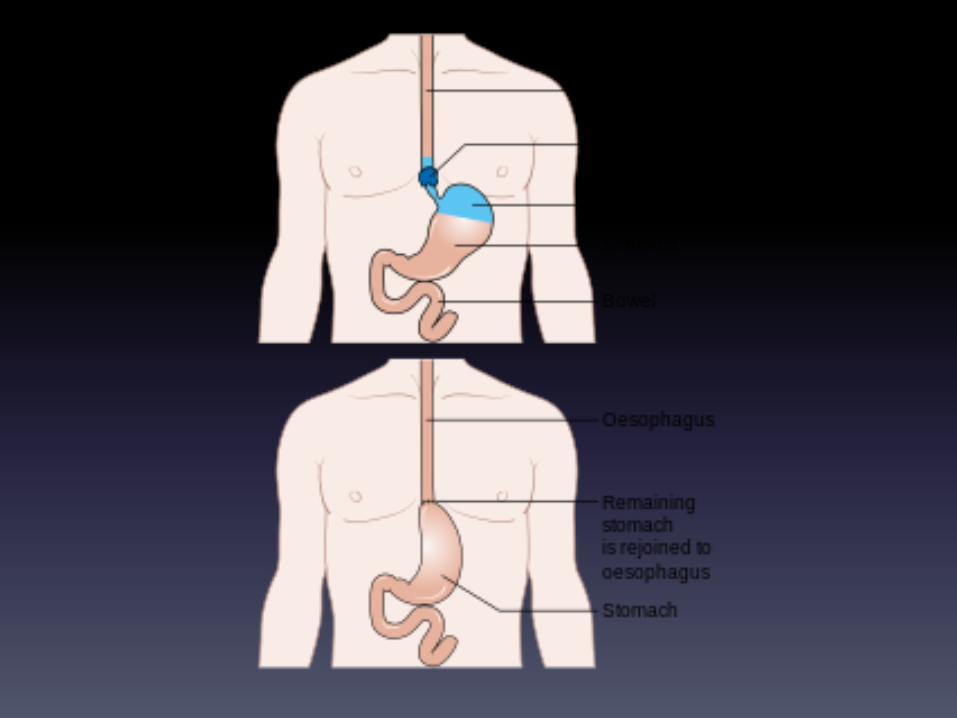
• Esophagectomy
การผ่าตัดหลอดอาหารบางส่วนออก และเชื่อมต่อส่วนของหลอดอาหารที่เหลือเข้ากับกระเพาะอาหาร ผู้ป่วยจะยังคงกลืนอาหารได้ตามปกติ หลอดพลาสติกหรือบางส่วนของลำไส้เล็กอาจถูกใช้เพื่อมาเชื่อมต่อ ต่อมน้ำเหลืองบริเวณใกล้เคียงหลอดอาหารจะถูกตัดออกมาตรวจเพื่อหาการกระจายของเซลล์มะเร็ง ถ้าหลอดอาหารตีบเนื่องจากเนื้องอก อาจมีการใส่หลอดโลหะ (stent) เพื่อขยายหลอดอาหารด้วย
MORE KNOWLEDGE
• first and the most common symptom is
usually dysphagia , which is often experienced first
with solid foods and later with softer foods and liquids.
• Esophageal cancer is the eighth most frequently
diagnosed cancer worldwide,and because of its poor
prognosis it is the sixth most common cause of cancer-
related death
Esophageal cancer has main 2 subtype
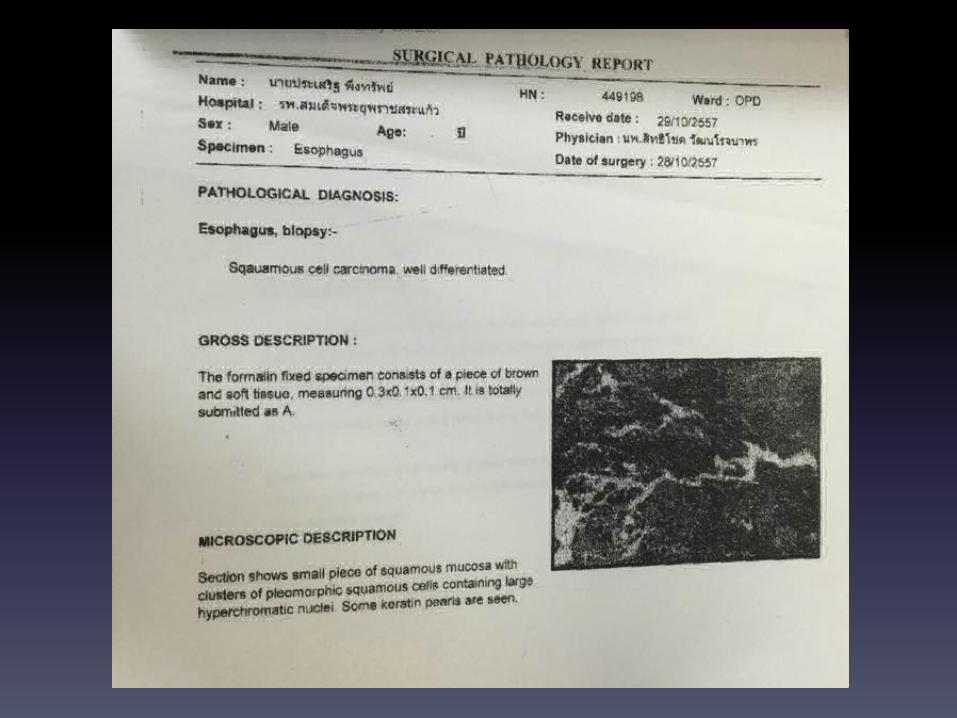
• 1.Squamous cell carcinoma
- more common in the developing world
- arises from the skin cells line the esophagus.
- most common causes of the squamous-cell
type are: tobacco, alcohol, very hot drinks, and
a poor diet.
• 2.Adenocarcinoma
-more common in the developed world
- arises from glandular cells present in the lower third of
the esophagus
- The most common causes of the adenocarcinoma type
are smoking tobacco, obesity , and acid refulx.

• diets high in cruciferous (cabbage, broccoli, cauliflower, Brussels sprouts) and green and
yellow vegetables and fruits are associated with
a decreased risk of esophageal cancer.“
• Dietary fiber is thought to be protective, especially against esophageal adenocarcinoma.
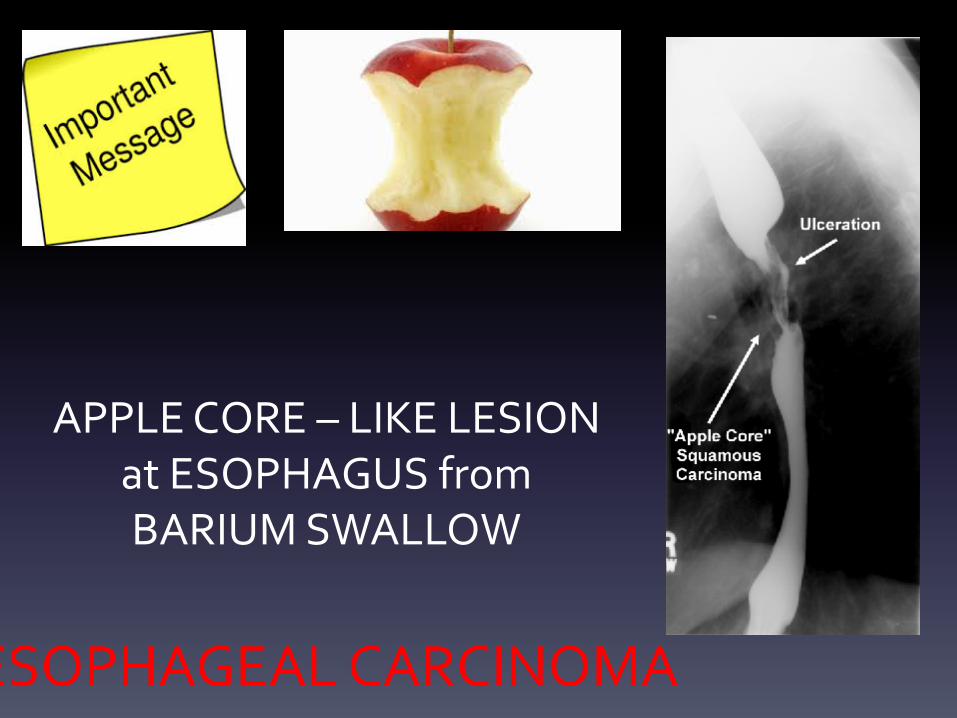
APPLE CORE – LIKE LESION at ESOPHAGUS from BARIUM SWALLOW
ESOPHAGEAL CARCINOMA