disease of the urinary system - zhejiang...
TRANSCRIPT

Pathology Department, Zhejiang University School of Medicine,
Disease of the Urinary System

Disorders of the Kidney
Congenital – Malformations, cysts, dysplasia.
Acquired– Glomerular diseases– Tubulointerstitial diseases– Neoplasms – carcinoma
GlomerularGlomerular DiseasesDiseases((Glomerulonephritis,GNGlomerulonephritis,GN))

GLOMERULONEPHRITISGLOMERULONEPHRITIS
Definition Classification Pathogenesis Histologic Alterations Clinical Manifestations
Primary GNAcute diffuse proliferative glomerulonephritis
Rapidly progressive (crescentic) glomerulonephritis
Membranous glomerulopathyMinimal change diseaseFocal segmental glomerulosclerosisMembranoproliferative glomerulonephritisIgA nephropathyChronic glomerulonephritis
Secondary GNSystemic lupus erythematosusDiabetes mellitusAmyloidosisGoodpasture syndromeMicroscopic polyarteritis/polyangiitisWegener granulomatosisHenoch-Schönlein purpuraBacterial endocarditis
Immune MechanismsImmune MechanismsAntibody-Mediated InjuryCytotoxic AntibodiesCell-mediated Immune InjuryActivation of Alternative Complement Pathway
In Situ Immune Complex Deposition Circulating Immune Complex Deposition
PATHOGENESIS OF GLOMERULAR INJURY
HypercellularityHypercellularity
Basement Membrane Thickening/brokenBasement Membrane Thickening/broken
Hyalinization Hyalinization
Sclerosis Sclerosis
Exudation /necrosisExudation /necrosis
Change of Change of stromastroma
BASIC HISTOLOGIC ALTERATION
HypercellularityHypercellularity
Cellular proliferation of mesangial, endothelial,or epithelial cells
Leukocytic infiltration
Formation of crescents
Basement Membrane ThickeningBasement Membrane Thickening
Thickening of the capillary walls
Deposition of amorphous electron- dense material
Thickening of the basement membrane
proper

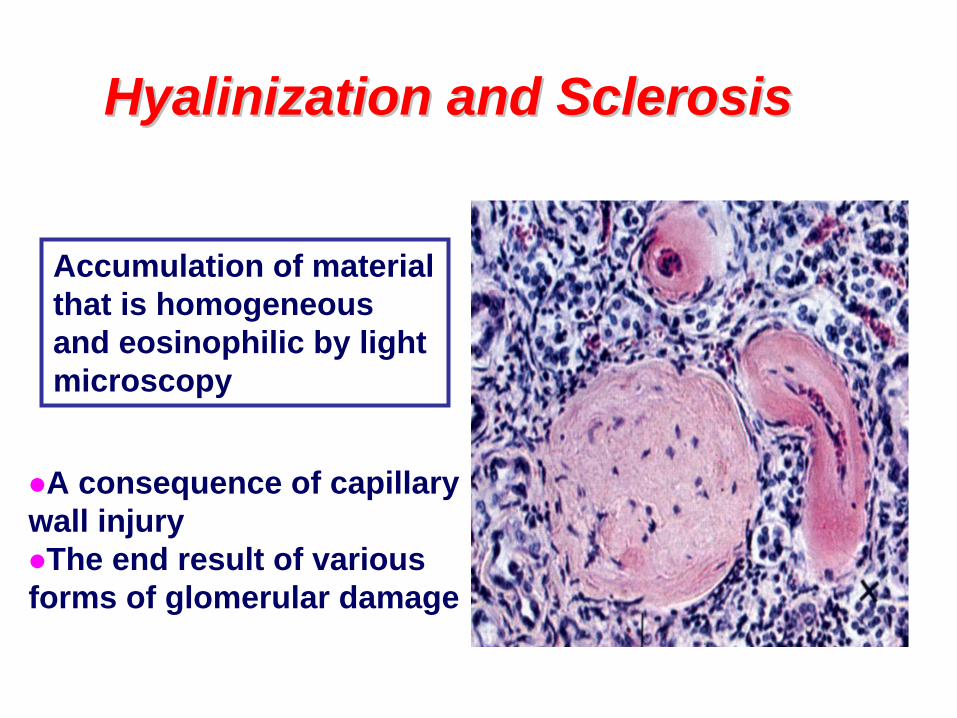
Hyalinization and SclerosisHyalinization and Sclerosis
Accumulation of material that is homogeneous and eosinophilic by light microscopy
A consequence of capillary wall injuryThe end result of various forms of glomerular damage
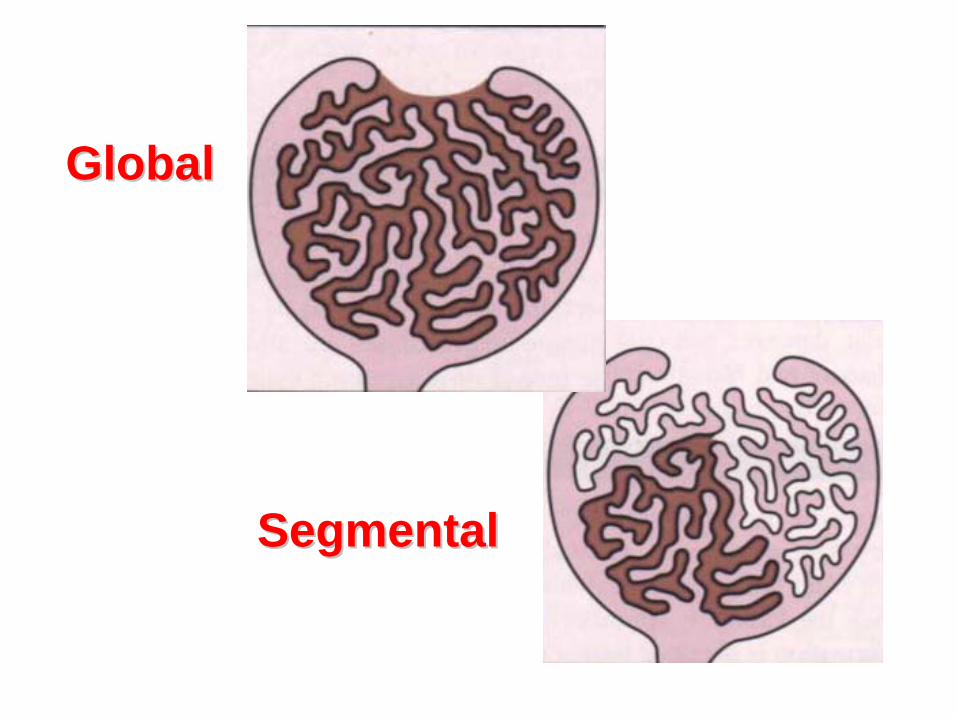
GlobalGlobal
SegmentalSegmental

Pathological DiagnosisPathological Diagnosis
LM (光学显微镜检查)
EM (电子显微镜检查)
IF (免疫荧光显微镜检查)
Clinical Manifestations
Syndromes
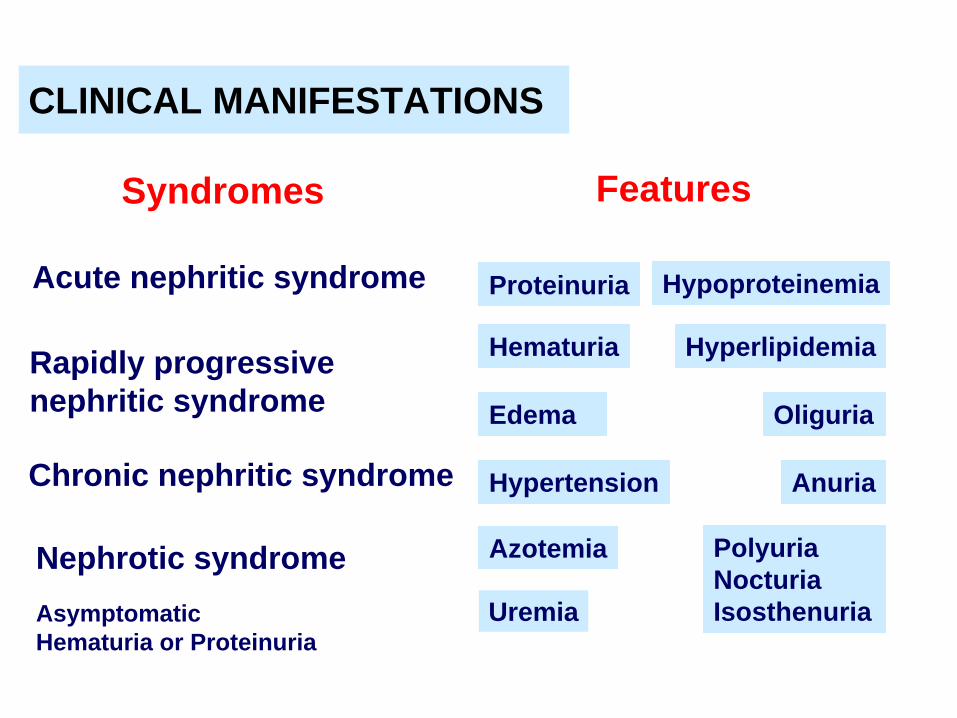
Proteinuria
Hematuria
Edema
Hypertension
Azotemia
Uremia
Features
Hypoproteinemia
Hyperlipidemia
Oliguria
Anuria
PolyuriaNocturiaIsosthenuria
CLINICAL MANIFESTATIONS
Acute nephritic syndrome
Rapidly progressive nephritic syndrome
Chronic nephritic syndrome
Nephrotic syndromeAsymptomatic Hematuria or Proteinuria

MAJOR PRIMARY GN
Acute Postinfectious GN Rapidly Progressive GN Membranous Nephropathy Minimal-change Disease Membranoproliferative GN IgA Nephropathy Chronic GN

Overview
Pathogenesis
Morphology
Treatment and Prognosis
Clinical Features
ACUTE POSTINFECTIOUS GN
Endocapillary Proliferative GN
Acute Diffuse Proliferative GN
Postinfectioous GN
ACUTE POSTINFECTIOUS GN

Appears usually 1-4 weeks after a group A -hemolytic streptococcal pharyngeal or skin infection
Occurs most frequently in children 6-10
years old
Characterized histologically by diffuse
proliferation of glomerular cells with infiltration of leukocytes
ACUTE POSTINFECTIOUS GN

Caused by deposition of immune complexes Ag may be exogenous or endogenous
ACUTE POSTINFECTIOUS GN

Enlarged glomeruli-”diffuse”
Hypercellularity: proliferation of glomerular cells & infiltration by WBC’s
Compression of glomerular capillary lumina
Proliferation of mesangial cells & endothelial cells
ACUTE POSTINFECTIOUS GN
Electron dense deposits – subepithelial “humps”
Granular deposits of IgG, IgM & C3 in the mesangium & along the GBM
ACUTE POSTINFECTIOUS GN

Subepithelial “humps”
EM
Acute Nephritic Syndrome
Mesangial cells Endothelial cells
ACUTE POSTINFECTIOUS GN

Overview
Pathogenesis
Morphology
Treatment and Prognosis
Clinical Features
RAPIDLY PROGRESSIVE GN

Extracapillary Proliferative GN
Crescentic GN
Malignant GN
RAPIDLY PROGRESSIVE GN
Not a specific etiologic form of glomerulonephritis
Characterized clinically by rapid &
progressive loss of renal function with severe oliguria
RAPIDLY PROGRESSIVE GN

Death from renal failure within weeks to months if untreated
Divided into 3 groups based on
immunologic findings
RAPIDLY PROGRESSIVE GN

TYPE I RPGN Idiopathic Goodpasture syndrome
TYPE II RPGN Idiopathic Postinfectious Systemic lupus erythematosus Henoch-Schönlein purpura (IgA) Others
RAPIDLY PROGRESSIVE GN
TYPE III RPGN (pauci-immune) ANCA associated Idiopathic Wegener granulomatosis Microscopic polyarteritis nodosa
RAPIDLY PROGRESSIVE GN
Crescent formation by proliferation of parietal cells,
infiltrates of WBC’s & fibrin deposition in Bowman’s space
EM reveals focal disruptions in
the GBM
RAPIDLY PROGRESSIVE GN
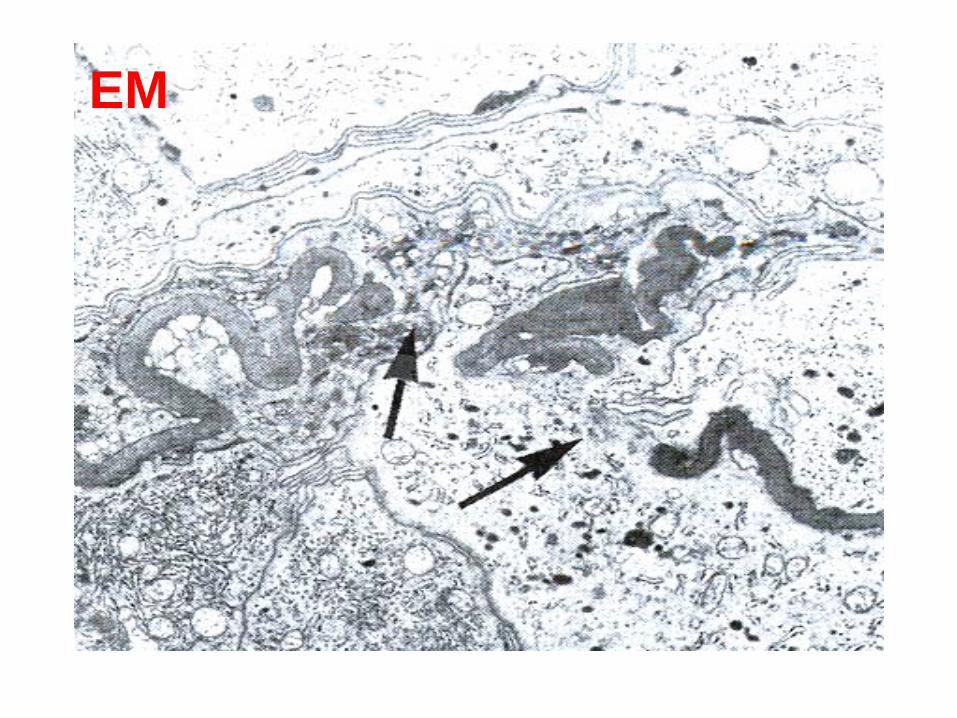
EM

Patients present Rapidly progressive nephritic syndrome with acute nephritic syndrome, occasionally have the nephrotic syndrome
ANCA, anti-GBM & antinuclear Ab’s are
helpful in Dx
RAPIDLY PROGRESSIVE GN
Overview
Pathogenesis
Morphology
Treatment and Prognosis
Clinical Features
MEMBRANOUS NEPHROPATHY

Main cause of nephrotic syndrome in adults Characterized by diffuse thickening of the GBM
& the accumulation of electron-dense, immunoglobulin-containing deposits
MEMBRANOUS NEPHROPATHY
Primary membranous GN is caused by autoantibodies directed against an Ag on the visceral epithelial cells
Secondary membranous GN is caused
by deposition of immune complexes
MEMBRANOUS NEPHROPATHY
Diffuse thickening of glomerular capillary wall EM reveals subepithelial deposits Spikes can be seen by silver stains Granular deposits of Ig’s & complements on IF
GBM becomes progressively thicker and
compresses the capillary lumens
MEMBRANOUS NEPHROPATHY
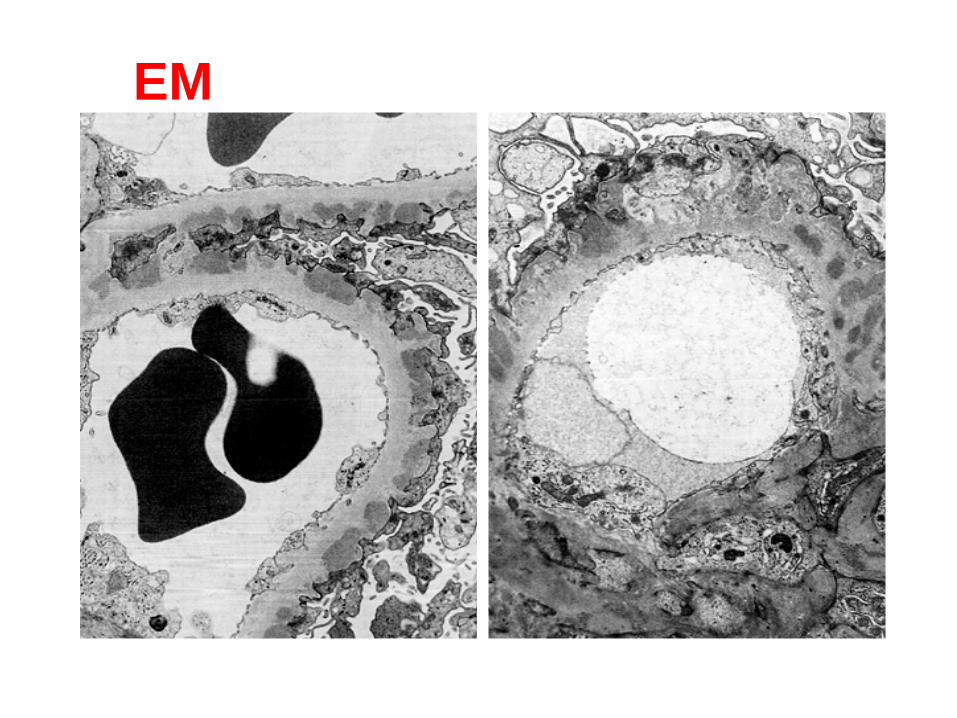
EM
Nephrotic Syndrome
Massive proteinuria
3.5 gm/day
Hypoalbuminemia, plasma albumin levels
< 3 gm/dl Generalized edema Hyperlipidemia & lipiduria
MEMBRANOUS NEPHROPATHY

Nephrotic Syndrome
Derangement in glomerular capillary walls which results in
permeability to plasma
proteins Complications:
infections due to loss of Ig’s &
complement
thrombosis due to loss of anticoagulant
factors
MEMBRANOUS NEPHROPATHY

MAJOR PRIMARY GN
Overview
Pathogenesis
Morphology
Treatment and Prognosis
Clinical Features
MINIMAL-CHANGE DISEASE
Lipoid nephrosis
Minimal Change Glomerulonephritis
MINIMAL-CHANGE DISEASE
Peak incidence 2-6 years of age Main cause of nephrotic syndrome in children
Characterized by diffuse effacement of foot
processes of podocytes
Sometimes follows a respiratory infection or
vaccination
Incidence in patients with Hodgkin disease
MINIMAL-CHANGE DISEASE
Evidence indicates an immune mechanism Immune dysfunction circulating cytokine injures visceral epithelial cells proteinuria
Some cases are caused by mutations in genes that encode slit diaphragm proteins
MINIMAL-CHANGE DISEASE
Glomeruli are normal by LM Proximal tubular cells are often laden with lipid
Epithelial cells exhibit diffuse loss of foot
processes on EM No Ig or complement deposits detected by IF
MINIMAL-CHANGE DISEASE

LM
Nephrotic Syndrome
MINIMAL-CHANGE DISEASE
Overview
Pathogenesis
Morphology
Treatment and Prognosis
Clinical Features
MEMBRANOPROLIFERATIVE GN
Mesangiocapillary Glomerulonephritis
(MPGN)
MEMBRANOPROLIFERATIVE GN
MEMBRANOPROLIFERATIVE GN
Characterized by alterations in the GBM, proliferation of glomerular cells & leukocyte infiltration
Accounts for 10-20% of cases of nephrotic
syndrome in children & young adults
MEMBRANOPROLIFERATIVE GN
Often present with a combined nephritic/nephrotic picture

MEMBRANOPROLIFERATIVE GN
Type I MPGN
Deposition of immune complexes with activation of both classical & alternative complement pathways

MEMBRANOPROLIFERATIVE GN
Type II MPGN
serum C3, factor B & properidin but
normal serum C1 & C4 activation of alternative complement pathway
> 70% of patients have C3 nephritic
factor (C3NeF)
MEMBRANOPROLIFERATIVE GN
Glomeruli are enlarged, hypercellular & lobulated
Glomerular capillary wall has a “double
contour” or “tram-track” appearance caused by duplication of the GBM with mesangial & monocyte interposition
MEMBRANOPROLIFERATIVE GN
Type I MPGN Subendothelial electron-dense deposits
Granular deposits of C3 and often IgG,
C1q & C4

MEMBRANOPROLIFERATIVE GN
Type II MPGN
Lamina densa is extremely electron-dense
(dense-deposit disease)
C3 is present in the GBM & mesangium
(mesangial rings) IgG, C1q & C4 are usually absent

MEMBRANOPROLIFERATIVE GN
10-20% of cases of nephrotic syndrome in children & young adults
A combined nephritic/nephrotic picture

Overview
Pathogenesis
Morphology
Treatment and Prognosis
Clinical Features
IgA NEPHROPATHY
IgA NEPHROPATHY
Berger Disease
Characterized by presence of prominent deposits of IgA in the mesangium Most common type of GN worldwide

IgA NEPHROPATHY
Abnormality of immune regulation
mucosal IgA synthesis in response to
respiratory or GI exposure to environmental antigens
IgA & IgA immune complexes are entrapped in the mesangium activation of alternative complement pathway glomerular injury
IgA NEPHROPATHY
Considerable variation on LM: glomeruli may appear normal, may exhibit mesangioproliferative GN, focal proliferative GN or rarely crescentic GN
IF reveals mesangial deposition of IgA, often
with C3 & properdin, early complement components are absent
IgA NEPHROPATHY
Affects children & young adults Present with hematuria often after a
respiratory infection
Overview
Pathogenesis
Morphology
Treatment and Prognosis
Clinical Features
CHRONIC GN

CHRONIC GN
End-stage Renal Disease Granular Contracted Kidney
Chronic Sclerosing GlomerulonephritisChronic Nephritis
CHRONIC GN
The kidneys are symmetrically small. The outer surface is diffusely granular.
On section, the cortex is thin and there is
increase in peripelvic fat.
Gross

CHRONIC GN
There is hyaline obliteration (hyalinization) of most of the glomeruli.
The glomeruli remaining undergo
compensatory hypertrophy & tubular dilatation Arterial & arteriolar sclerosis Interstitial chronic inflammation and fibrosis
Histological
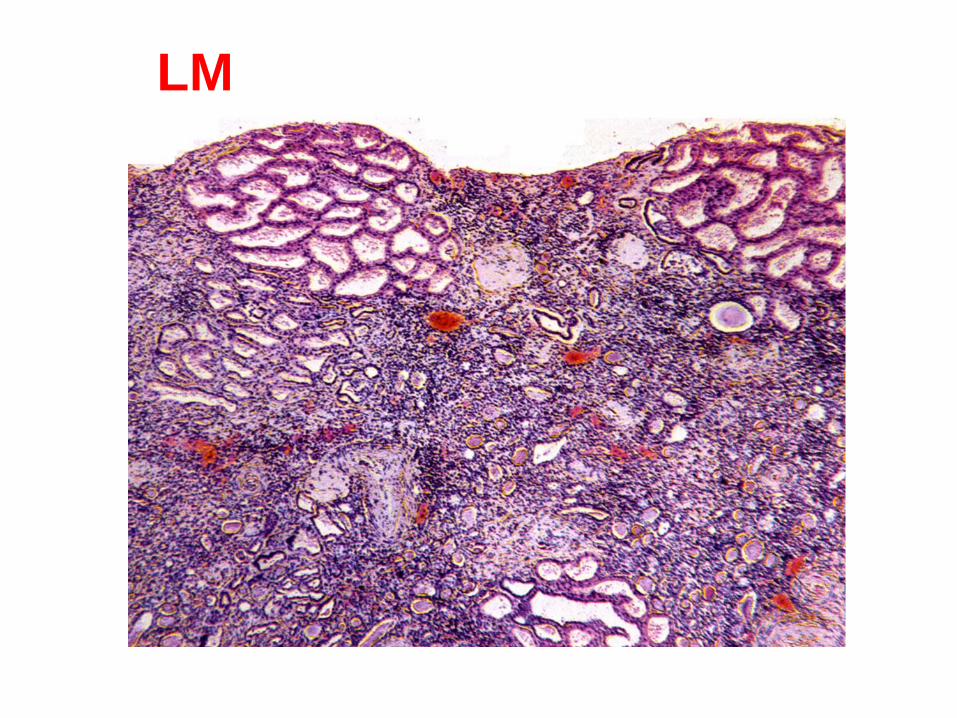
LM

LM
CHRONIC GN
Chronic Renal Failure
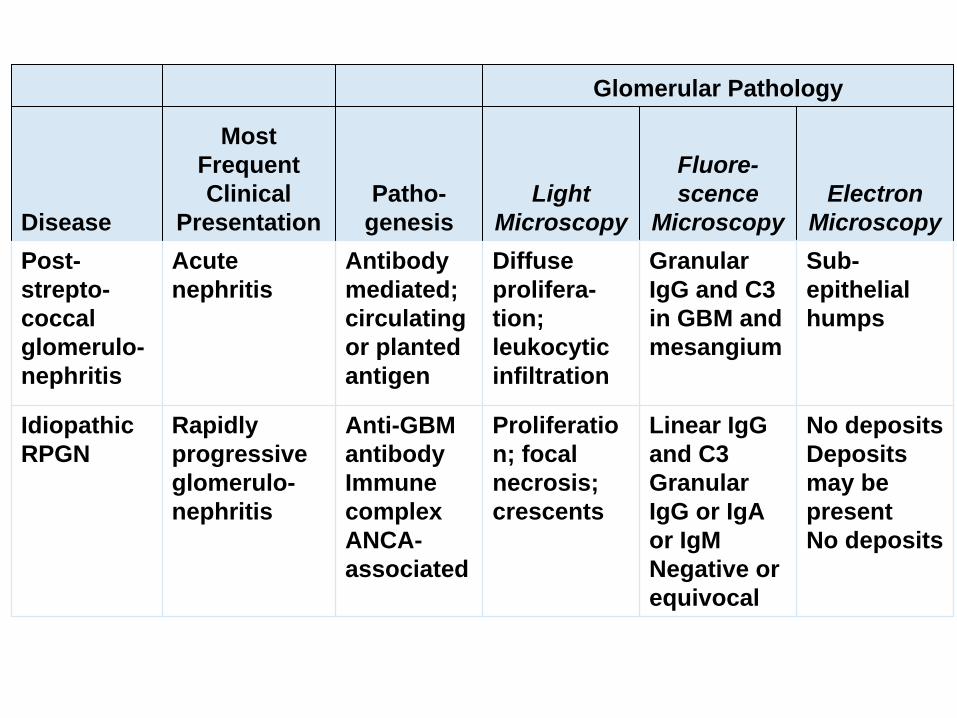
Glomerular Pathology
Disease
Most Frequent Clinical
PresentationPatho-
genesisLight
Microscopy
Fluore- scence
MicroscopyElectron
MicroscopyPost- strepto- coccal glomerulo- nephritis
Acute nephritis
Antibody mediated; circulating or planted antigen
Diffuse prolifera- tion; leukocytic infiltration
Granular IgG and C3 in GBM and mesangium
Sub- epithelial humps
Idiopathic RPGN
Rapidly progressive glomerulo- nephritis
Anti-GBM antibody Immune complex ANCA- associated
Proliferatio n; focal necrosis; crescents
Linear IgG and C3 Granular IgG or IgA or IgM Negative or equivocal
No deposits Deposits may be present No deposits
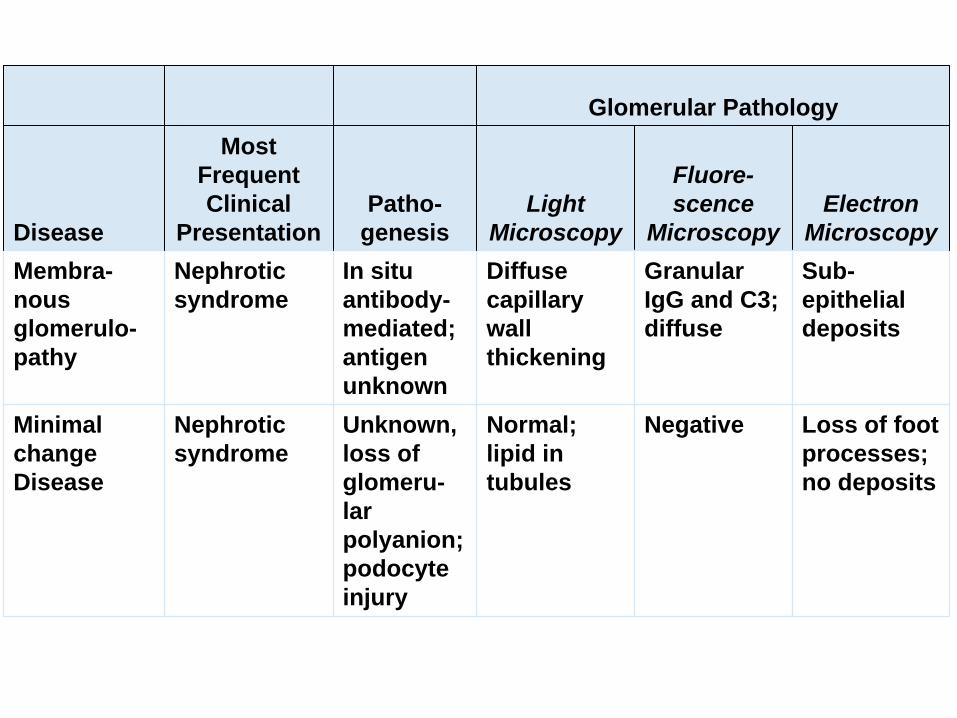
Glomerular Pathology
Disease
Most Frequent Clinical
PresentationPatho-
genesisLight
Microscopy
Fluore- scence
MicroscopyElectron
MicroscopyMembra- nous glomerulo- pathy
Nephrotic syndrome
In situ antibody- mediated; antigen unknown
Diffuse capillary wall thickening
Granular IgG and C3; diffuse
Sub- epithelial deposits
Minimal change Disease
Nephrotic syndrome
Unknown, loss of glomeru- lar polyanion; podocyte injury
Normal; lipid in tubules
Negative Loss of foot processes; no deposits
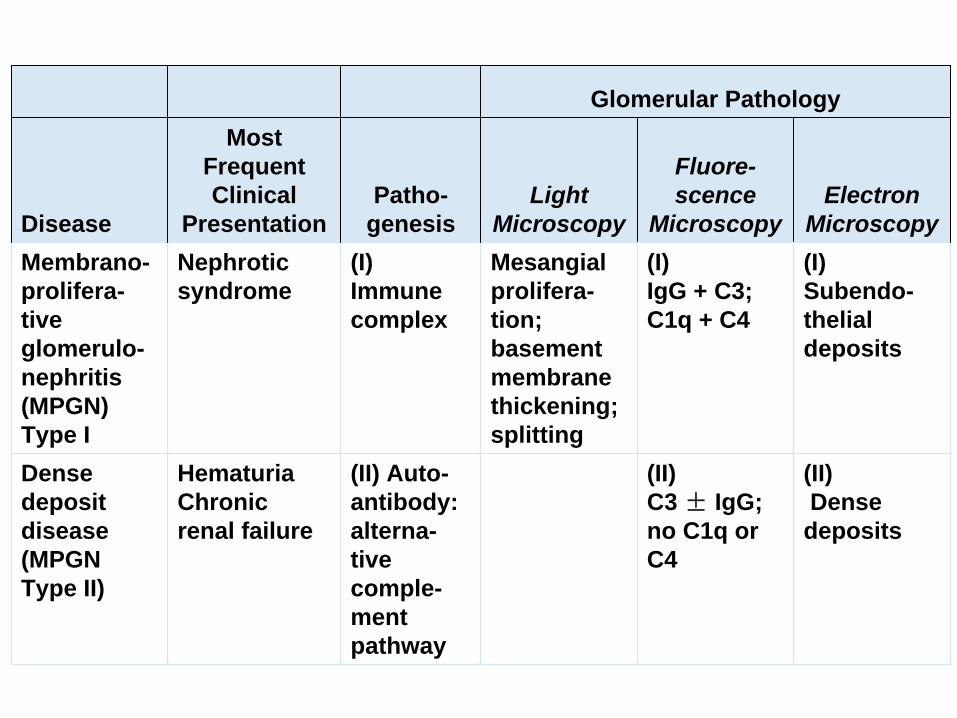
Glomerular Pathology
Disease
Most Frequent Clinical
PresentationPatho-
genesisLight
Microscopy
Fluore- scence
MicroscopyElectron
MicroscopyMembrano- prolifera- tive glomerulo- nephritis (MPGN) Type I
Nephrotic syndrome
(I) Immune complex
Mesangial prolifera- tion; basement membrane thickening; splitting
(I) IgG + C3; C1q + C4
(I) Subendo- thelial deposits
Dense deposit disease (MPGN Type II)
Hematuria Chronic renal failure
(II) Auto- antibody: alterna- tive comple- ment pathway
(II) C3 ± IgG; no C1q or C4
(II)Dense deposits
Glomerular Pathology
Disease
Most Frequent Clinical
PresentationPatho-
genesisLight
Microscopy
Fluore- scence
MicroscopyElectron
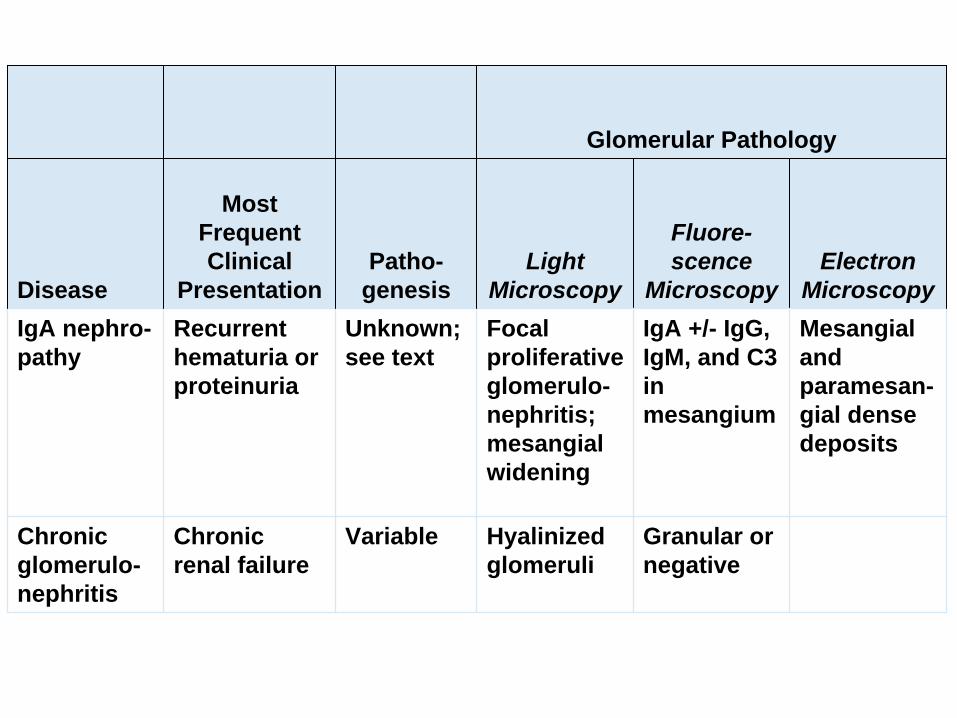
MicroscopyIgA nephro- pathy
Recurrent hematuria or proteinuria
Unknown; see text
Focal proliferative glomerulo- nephritis; mesangial widening
IgA +/- IgG, IgM, and C3 in mesangium
Mesangial and paramesan- gial dense deposits
Chronic glomerulo- nephritis
Chronic renal failure
Variable Hyalinized glomeruli
Granular or negative
TubulointerstitialTubulointerstitial NephritisNephritis
Infections
Toxins
Metabolic Diseases
Physical Factors
Neoplasms
Immunologic Reactions
Vascular Diseases
Miscellaneous
Causes of Tubulointerstitial Nephritis Infections
Toxins
Metabolic Diseases
Physical Factors
Neoplasms
Immunologic Reactions
Vascular Diseases
Miscellaneous

Pyelonephritis
Interstitial diseases induced by drugs

PYELONEPHRITISPYELONEPHRITIS
Definition Etiology & Pathogenesis Two Forms of
Pyelonephritis
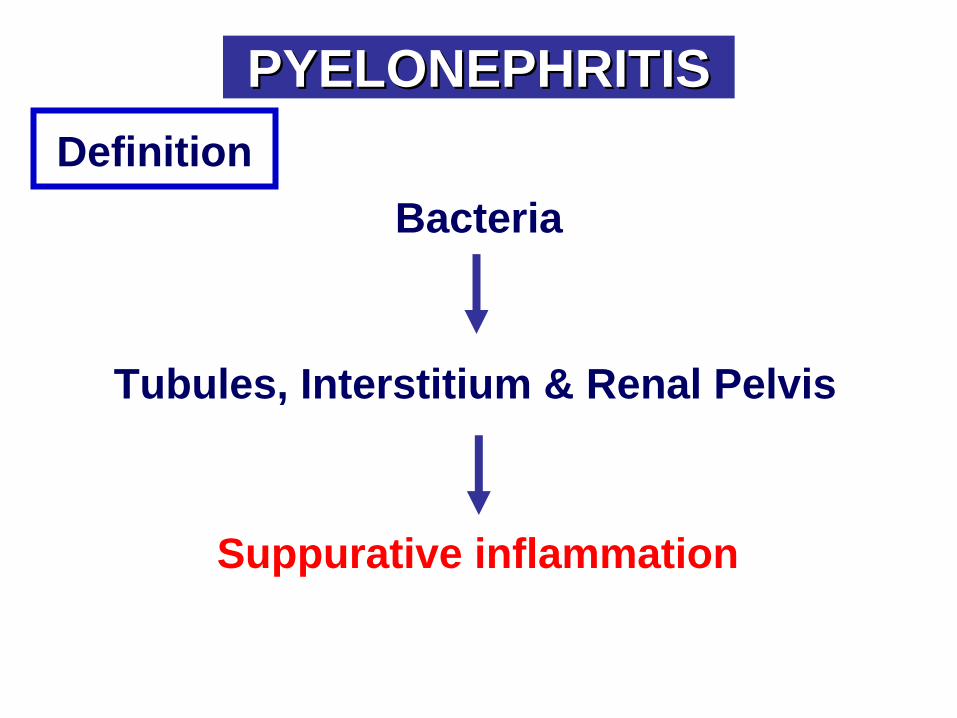
Tubules, Interstitium & Renal Pelvis
Bacteria
Suppurative inflammation
PYELONEPHRITISPYELONEPHRITISDefinition
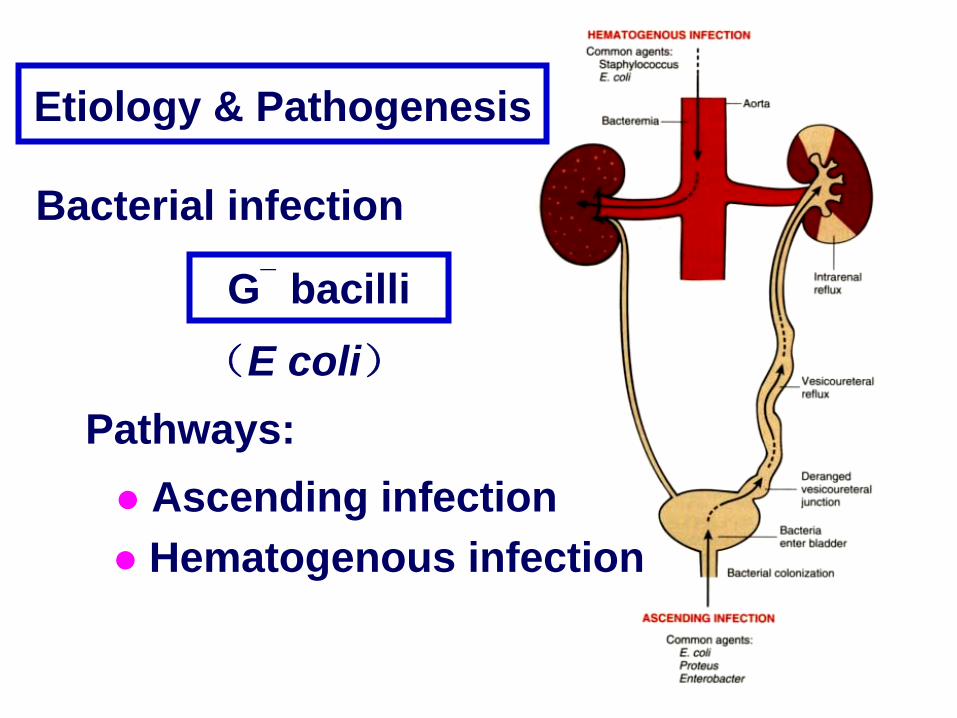
Bacterial infection
G¯ bacilli(E coli)
Etiology & Pathogenesis
Hematogenous infection Ascending infection
Pathways:

Predisposing Factors
Systemic
Local Urinary tract obstruction Urinary tract mucosa injury Vesicoureteral reflux
Etiology & Pathogenesis
Defense mechnisms
ACUTE PYELONEPHRITISACUTE PYELONEPHRITIS
CHRONIC PYELONEPHRITISCHRONIC PYELONEPHRITIS
Two Forms of Pyelonephritis
MorphologyACUTE PYELONEPHRITIS
Patchy interstitial suppurative inflammation Intratubular aggregates of neutrophils Tubular necrosis

LM
Acute pyelonephritis marked by an acute neutrophilic exudate within tubules and the renal substance.
ACUTE PYELONEPHRITIS
Renal papillary necrosis Perinephric abscesses Pyonephrosis

CHRONIC PYELONEPHRITIS

Chronic reflux-associated Chronic obstructive
CHRONIC PYELONEPHRITIS
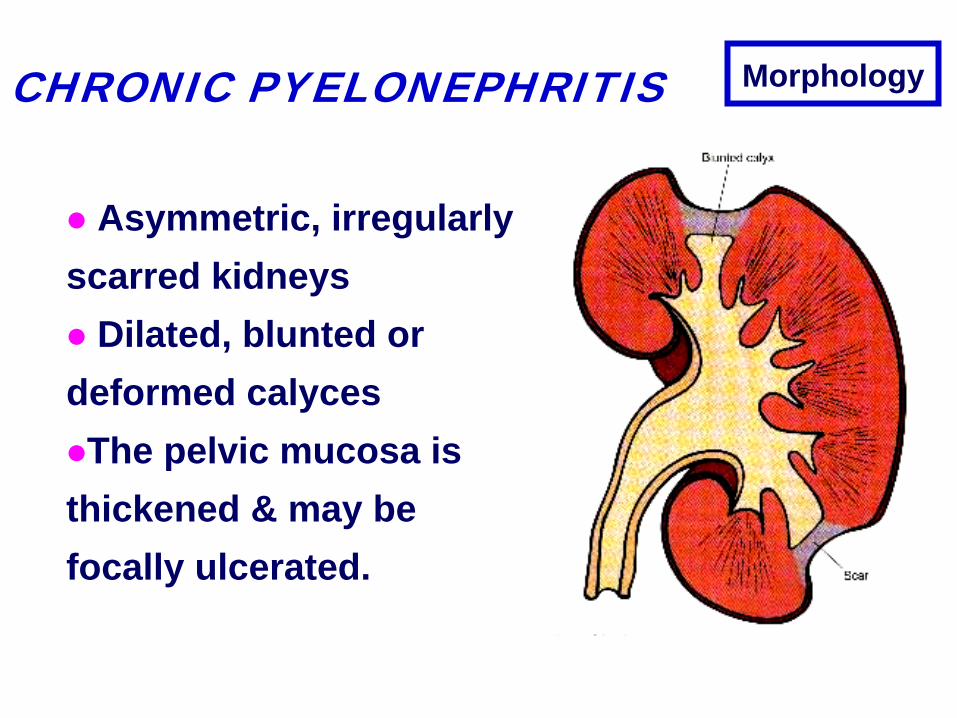
Morphology
Asymmetric, irregularly scarred kidneys
Dilated, blunted or
deformed calycesThe pelvic mucosa is thickened & may be focally ulcerated.
CHRONIC PYELONEPHRITIS
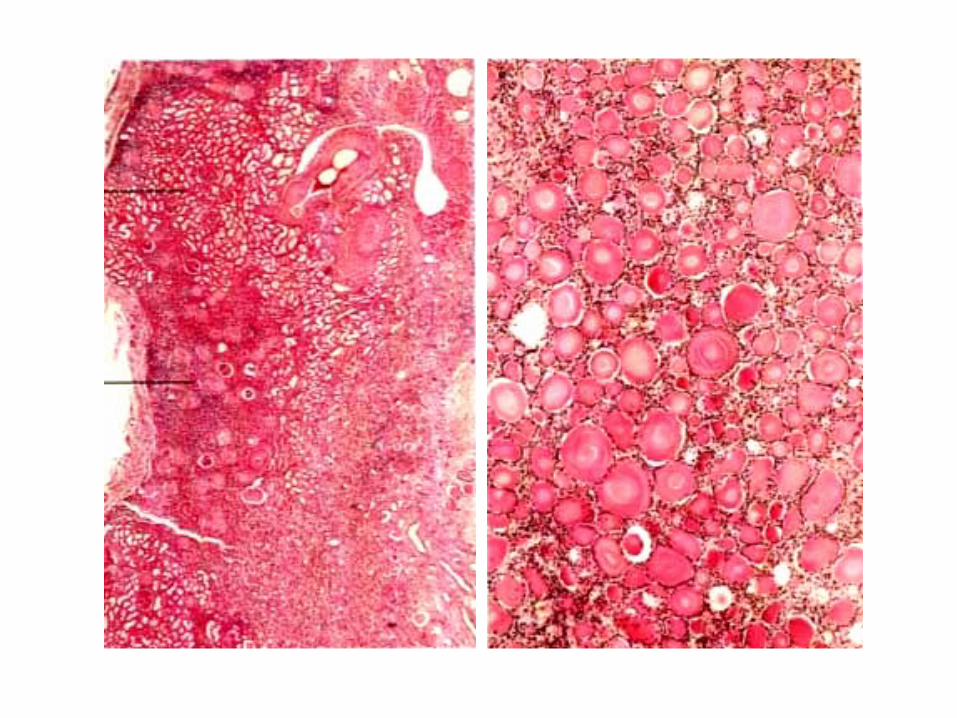
LM The interstitium: Chronic inflammation The tubules:
Atrophy, necrosis & fibrosis Hypertrophy or dilation
May be filled with pink proteinaceous material (colloid
casts, thyroidization).
The calyceal mucosa: Chronic inflammation The glomeruli:periglomerular fibrosis
glomerular fibrosis & hyaline change
Chronic Course
Progression to azotemia and uremia
CHRONIC PYELONEPHRITIS

MALIGNANT TUMORSMALIGNANT TUMORS
Renal Cell Carcinoma
Nephroblastoma
Transitional Cell Carcinoma Of The Bladder

Nephroblastoma

Transitional cell carcinoma of the bladder
