early detection mods 16 พค.58
TRANSCRIPT

EARLY DETECTION OF MULTIPLE ORGAN
DYSFUNCTION SYNDROME
ผศ.ดร.กรองได อุณหสตู
Multi organ dysfunction syndrome
Multi organ dysfunction syndrome (MODS) as the dysfunction of at least 2 organ systems from an inflammatory insult.
ผศ.ดร.กรองได อุณหสูต
Injury stress reaction SIRS/CARS MODS MOF
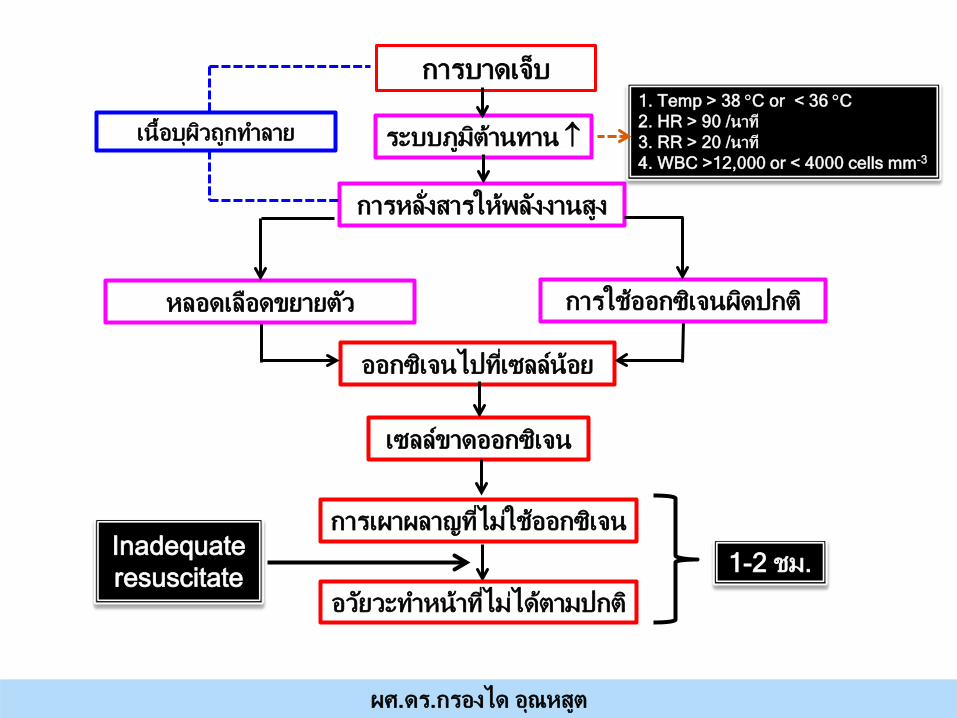
การบาดเจ็บ
เน้ือบุผวิถูกทาํลาย
ออกซเิจนไปทีเ่ซลล์น้อย
เซลล์ขาดออกซเิจน
การเผาผลาญทีไ่มใ่ชอ้อกซเิจน
ระบบภูมติา้นทาน ↑
การหล ั่งสารใหพ้ลงังานสูง
หลอดเลือดขยายตวั การใชอ้อกซเิจนผดิปกต ิ
อวยัวะทาํหน้าทีไ่มไ่ดต้ามปกต ิ
1. Temp > 38 °C or < 36 °C 2. HR > 90 /นาที 3. RR > 20 /นาที 4. WBC >12,000 or < 4000 cells mm-3
ผศ.ดร.กรองได อุณหสูต
1-2 ชม. Inadequate resuscitate
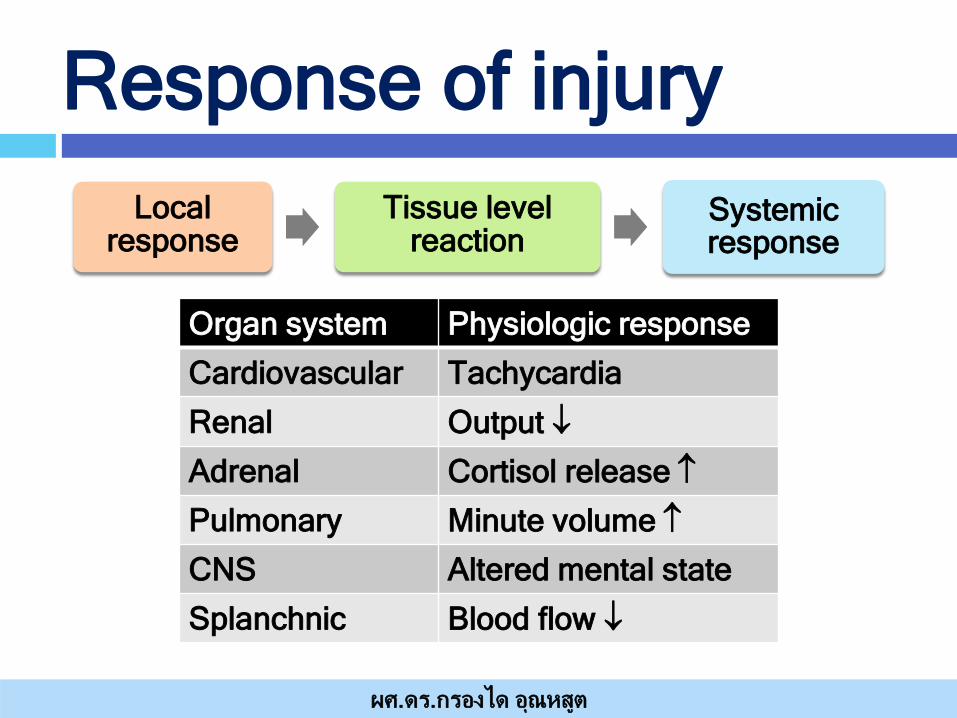
Response of injury Local
response Tissue level
reaction Systemic response
ผศ.ดร.กรองได อุณหสูต
Organ system Physiologic response
Cardiovascular Tachycardia
Renal Output ↓
Adrenal Cortisol release ↑
Pulmonary Minute volume ↑
CNS Altered mental state
Splanchnic Blood flow ↓

Injury
ACTH
กระตุน้การสรา้ง
cortisol
เผาผลาญ คาร์โบไฮเดรท โปรตีน ไขมนั
และโปแตสเซียม
โอกาสเกดิ การตดิเช้ือสงู
Renin
angiotensin I และangiotensin
II
หล ั่ง Aldosterone
และ vasopressin
ACTH
Catecholamine (epinephrine,
norepinephrine)
Vasopressin (ADH)
Osmo - regulation
เกดิการดูดน้ํากลบั
Vasoactive เกดิ
vasoconstriction
Metabolic เกดิ hepatic glycogeno -
lysis และ gluconeo- genesis
Insulin ไมเ่พิม่ขึน้
ลดลงสูปกตภิายใน 5 วัน
อัตรารอดชวีติ ↓
การดดูกลบัของโซเดยีม โปตัสเซยีม
สูงขึ้นทนัทใีน 24-48 ชม.
• เพิ่มการผลติกลโูคสเขาสูกระแสเลือด ลดการนาํกลโูคสเขาสูเซลล • กระตุนการเปลีย่นแปลงกรดอะมิโนเปนน้าํตาลกลโูคส สลายไขมนัเปนกรดไขมนั
กลูคากอน ยับยัง้การสราง
ผศ.ดร.กรองได อุณหสูต

SIRS
Systemic Immune Response Syndrome Temp > 38 °C or < 36 °C HR > 90 /นาท ีRR > 20 /นาท ีWBC >12,000 or < 4000 cells mm-3
ผศ.ดร.กรองได อุณหสูต
1 = absence 2 = mild 3 = moderate 4 = severe

Prediction of MODS
No singular standard to identify MODS No laboratory test has yet proven
diagnosis
ผศ.ดร.กรองได อุณหสูต
Physiologic scoring systems determine a severity score
and predict outcome

Organ indicator none minimal mild moderate severe
Respiratory PaO2/FiO2 ratio
> 300 226-300 151-225 76-150 ≤ 75
Renal Serum creatinine (umol/L)
≤ 100 101-200 201-350 351-500 > 500
Hepatic Serum birirubin (umol/L)
≤ 20 21-60 61-120 121-240 > 240
Cardiovascular CVP/MAP < 10.0 10.1-15.0 15.1-20.0 20.1-30.0 > 30.0
Hematologic Platelet count (mm3)
> 120,000 81,000-120,000
51,000-80,000
21,000-50,000
≤ 20,000
Neurologic GCS 15 13-14 10-12 7-9 ≤ 6
Multiple Organ Dysfunction Score Marshall,J.C
ผศ.ดร.กรองได อุณหสูต

Score point 1 2 3 4
Respiration PaO2FiO2 <400 <300 <200 with respiratory
support
<100 with respiratory
support
Cardiovascular Hypotension
MAP <70 Dopamine ≤5 or
dobutamine in any dose
Dopamine >5 or epinephrine
≤0.1 or norepinephrine
≤0.1
Dopamine >15 or epinephrine
>0.1 or norepinephrine
>0.1
Liver Birilubin(mg/dl)
1.2-1.9 2.0-5.9 6.0-11.9 >12.0
Renal Creatinine (mg/dl) or urine output (ml/d)
1.2-1.9 2.0-3.4 3.5-4.9 or <500 1n 24 hr
>5.0 or <200 in 24 hr
Coagulation Platelet x 103/mm3
>150 <100 <50 <25
CNS (GCS) 13-14 10-12 6-9 <6
Logistic Organ Dysfunction Score Le Gall et al
ผศ.ดร.กรองได อุณหสูต

Dysfunction 0 1 2 3
Pulmonary PaO2/FiO2 >208 208-165 165-83 <83
Renal Creatinine (umol/l)
>159 160-210 211-420 >420
Hepatic Total Birilubin (umol/l)
<34 34-68 69-137 >137
Cardiac Inotropes
No inotropes Only one inotrope at a small dose
Any inotrope at moderate dose
or >1 agent, all at small
dose
Any inotrope at large dose
or >2 agents, at moderate
dose
Denver Post injury Multiple organ Failure Score (Moore)
• ISS >15, survived longer 48 hr, ≥ 16 years of age
ผศ.ดร.กรองได อุณหสูต
SOFA score 0 1 2 3 4
Respiration PaO2FiO2 or SaO2/FiO2 mmHg
>400 <400 221-301
<300 142-220
<200 67-141
<100 <67
Coagulation >150 <150 <100 <50 <20
Liver Birilubin(mg/dl)
<1.2 1.2-1.9 2.0-5.9 6.0-11.9 >12.0
Cardiovascular Hypotension
No hypotension
MAP <70 Dopamine ≤5 or any
Dopamine >5 or
notepinephrine ≤0.1
Dopamine >15 or
norepinephrine >0.1
CNS (GCS) 15 13-14 10-12 6-9 <6
Renal Creatinine (mg/dl) or urine output (ml/d)
<1.2 1.2-1.9 2.0-3.4 3.5-4.9 or <5.00
>5.0 or <200
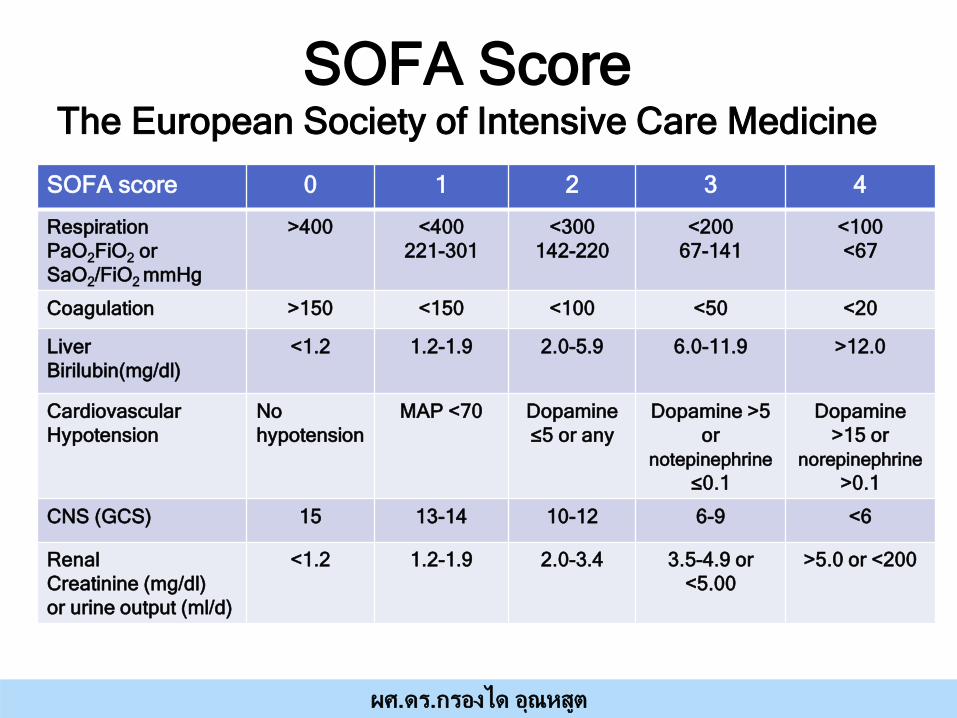
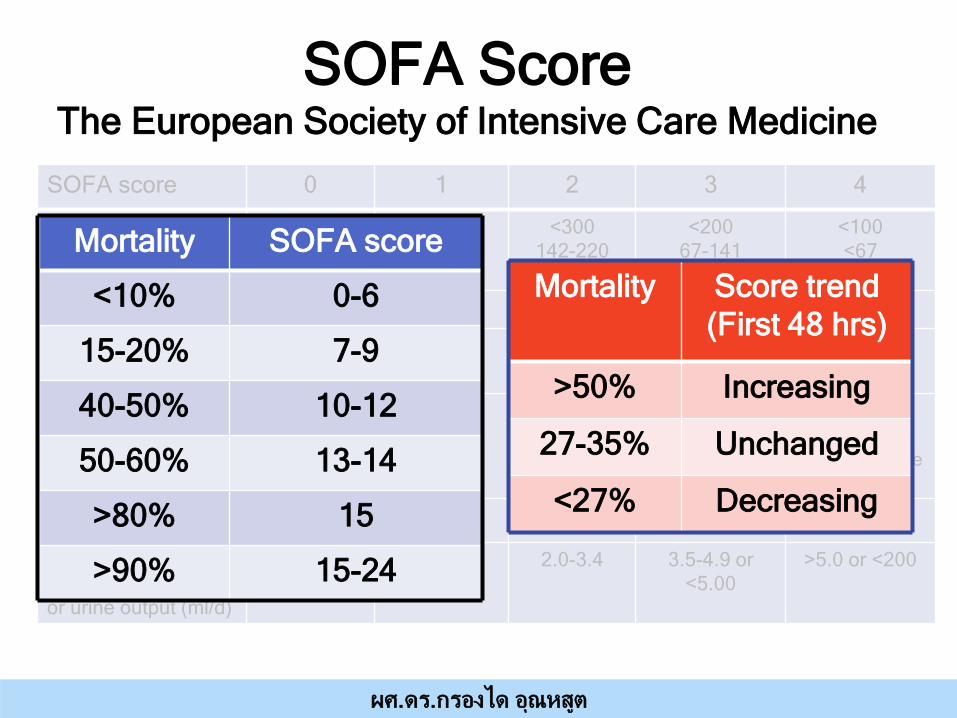
SOFA Score The European Society of Intensive Care Medicine
ผศ.ดร.กรองได อุณหสูต
SOFA score 0 1 2 3 4
Respiration PaO2FiO2 or SaO2/FiO2 mmHg
>400 <400 221-301
<300 142-220
<200 67-141
<100 <67
Coagulation >150 <150 <100 <50 <20
Liver Birilubin(mg/dl)
<1.2 1.2-1.9 2.0-5.9 6.0-11.9 >12.0
Cardiovascular Hypotension
No hypotension
MAP <70 Dopamine ≤5 or any
Dopamine >5 or
notepinephrine ≤0.1
Dopamine >15 or
norepinephrine >0.1
CNS (GCS) 15 13-14 10-12 6-9 <6
Renal Creatinine (mg/dl) or urine output (ml/d)
<1.2 1.2-1.9 2.0-3.4 3.5-4.9 or <5.00
>5.0 or <200
SOFA Score The European Society of Intensive Care Medicine
Mortality SOFA score
<10% 0-6
15-20% 7-9
40-50% 10-12
50-60% 13-14
>80% 15
>90% 15-24
Mortality Score trend (First 48 hrs)
>50% Increasing
27-35% Unchanged
<27% Decreasing
ผศ.ดร.กรองได อุณหสูต
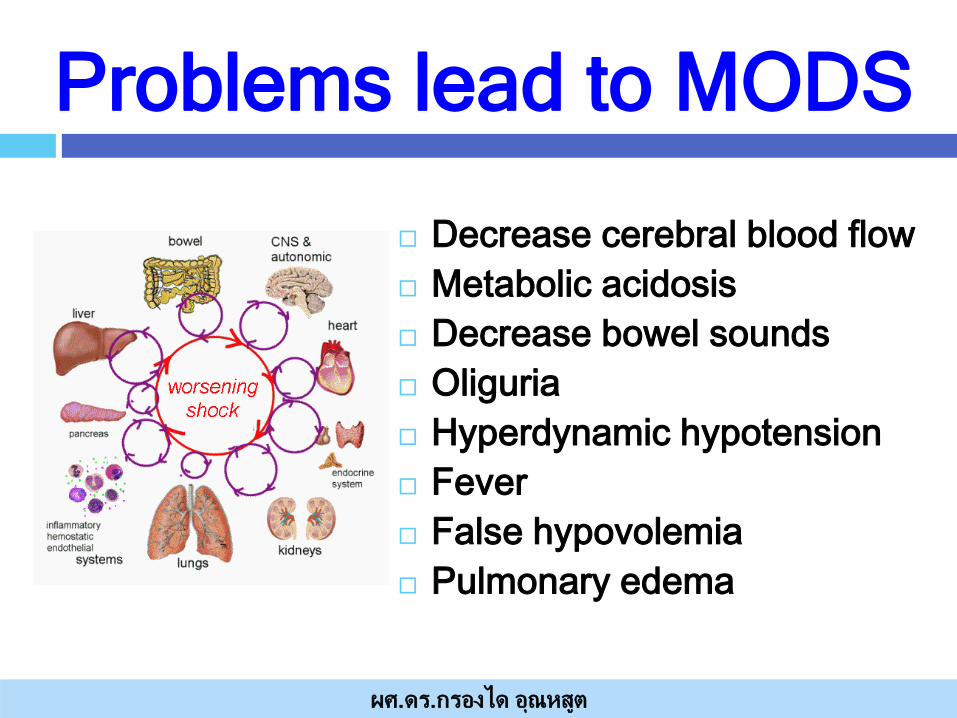
Problems lead to MODS
Decrease cerebral blood flow Metabolic acidosis Decrease bowel sounds Oliguria Hyperdynamic hypotension Fever False hypovolemia Pulmonary edema
ผศ.ดร.กรองได อุณหสูต
Hypoperfusion or hypotension variables;
Tissue perfusion variables; Hyperlactatemia (>2 mmol/L) Hemodynamic variables: Arterial hypotension (SBP <90 mm Hg,
MAP <70, or SBP decrease >40 mm Hg)
ผศ.ดร.กรองได อุณหสูต

Classification of MODS
Immediate Type (1° type) Dysfunction is happened simultaneously
in 2 or more organs due to primary disease. Delayed type (2° type) Dysfunction happened in a organ, other
organs sequentially happened dysfunction or failure.
Accumulation type: Dysfunction leaded by chronic disease.
ผศ.ดร.กรองได อุณหสูต
ผศ.ดร.กรองได อุณหสูต
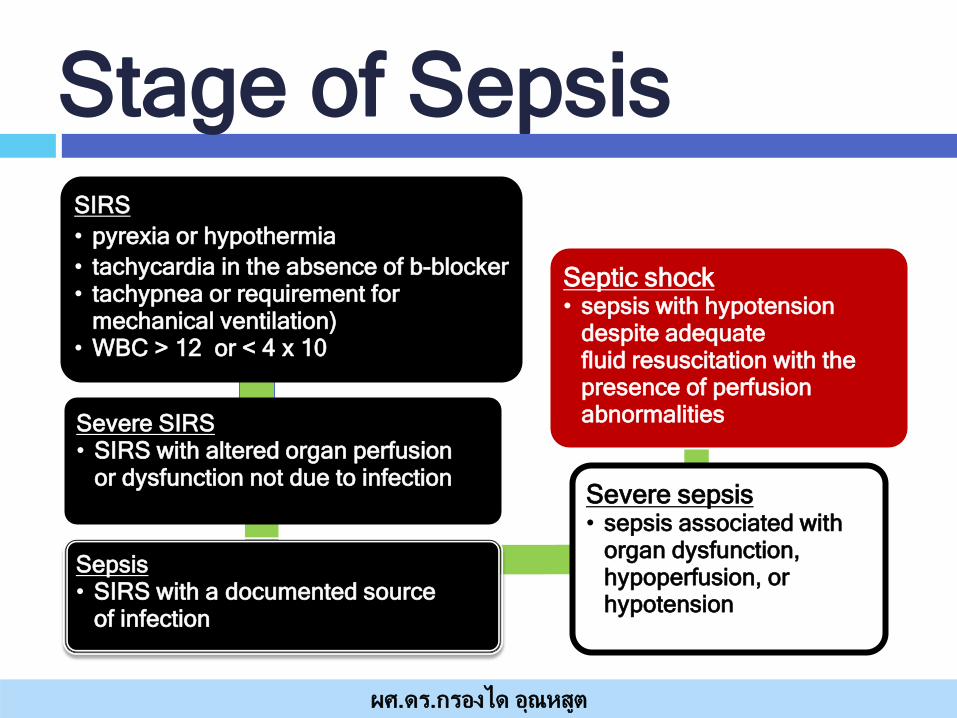
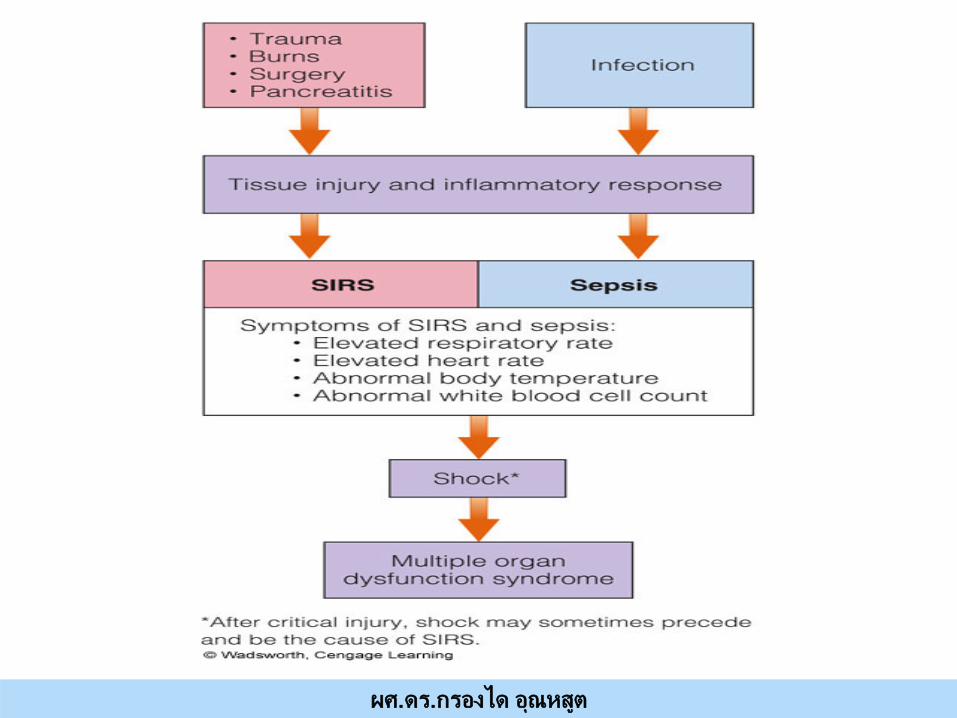
Stage of Sepsis SIRS
• pyrexia or hypothermia
• tachycardia in the absence of b-blocker • tachypnea or requirement for
mechanical ventilation) • WBC > 12 or < 4 x 10
Severe SIRS • SIRS with altered organ perfusion
or dysfunction not due to infection
Sepsis • SIRS with a documented source
of infection
Severe sepsis • sepsis associated with
organ dysfunction, hypoperfusion, or hypotension
Septic shock • sepsis with hypotension
despite adequate fluid resuscitation with the presence of perfusion abnormalities
ผศ.ดร.กรองได อุณหสูต

Respiratory failure is common in the first 72 hrs after the original insult
Hepatic failure (5-7days)
Gastrointestinal bleeding (10-15 days)
Renal failure (11-17 days)
2-3 days: SIRS develops 7-10 days: hypermetabolic state develops 14-21 days: unstable stage
ผศ.ดร.กรองได อุณหสูต
If MODS is not reversed by day 21, the client will die
Death occurs between day 21-28, after injury
Patient Care
Temperature control Metabolic support Anemia & coagulopathy Renal dysfunction Nutritional support
ผศ.ดร.กรองได อุณหสูต
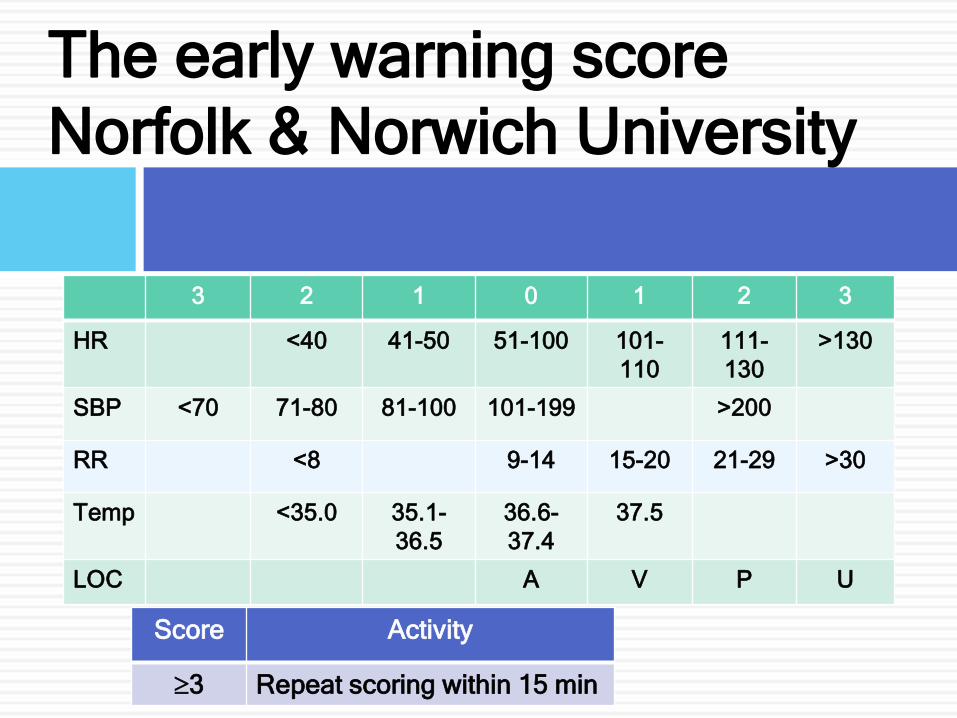
The early warning score Norfolk & Norwich University
3 2 1 0 1 2 3
HR <40 41-50 51-100 101-110
111-130
>130
SBP <70 71-80 81-100 101-199 >200
RR <8 9-14 15-20 21-29 >30
Temp <35.0 35.1-36.5
36.6-37.4
37.5
LOC A V P U
Score Activity
≥3 Repeat scoring within 15 min

MEWS 3 2 1 0 1 2 3
RR <8 9-14 15-20 21-29 >30
HR <40 40-50 51-100 101-110
111-129
>129
SBP <70 71-80 81-100 101-199 >200
LOC U P V A Confuse
Temp (°C) <35.0 35.1-36
36.1-38 38.1-38.5
>38.6
Hourly Urine for 2 hours
>10 cc/hr
>30 cc/hr
>45 cc/hr
Score Activity
1-2 Observe q 2 hr
3 Observe q 1 hr
>4 Observe q 30 mins

“Early treatment with antibiotic and fluid resuscitation has been found
to be strongly related to increased survival, which makes severe sepsis a condition which is important to identify and treat
as early as possible.”
ผศ.ดร.กรองได อุณหสูต